
Unveiling Timetable for Physical Therapy after Single-Level Lumbar Surgery for Degenerative Disc Disease: Insights from a Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Review Design
2.2. Search Strategy
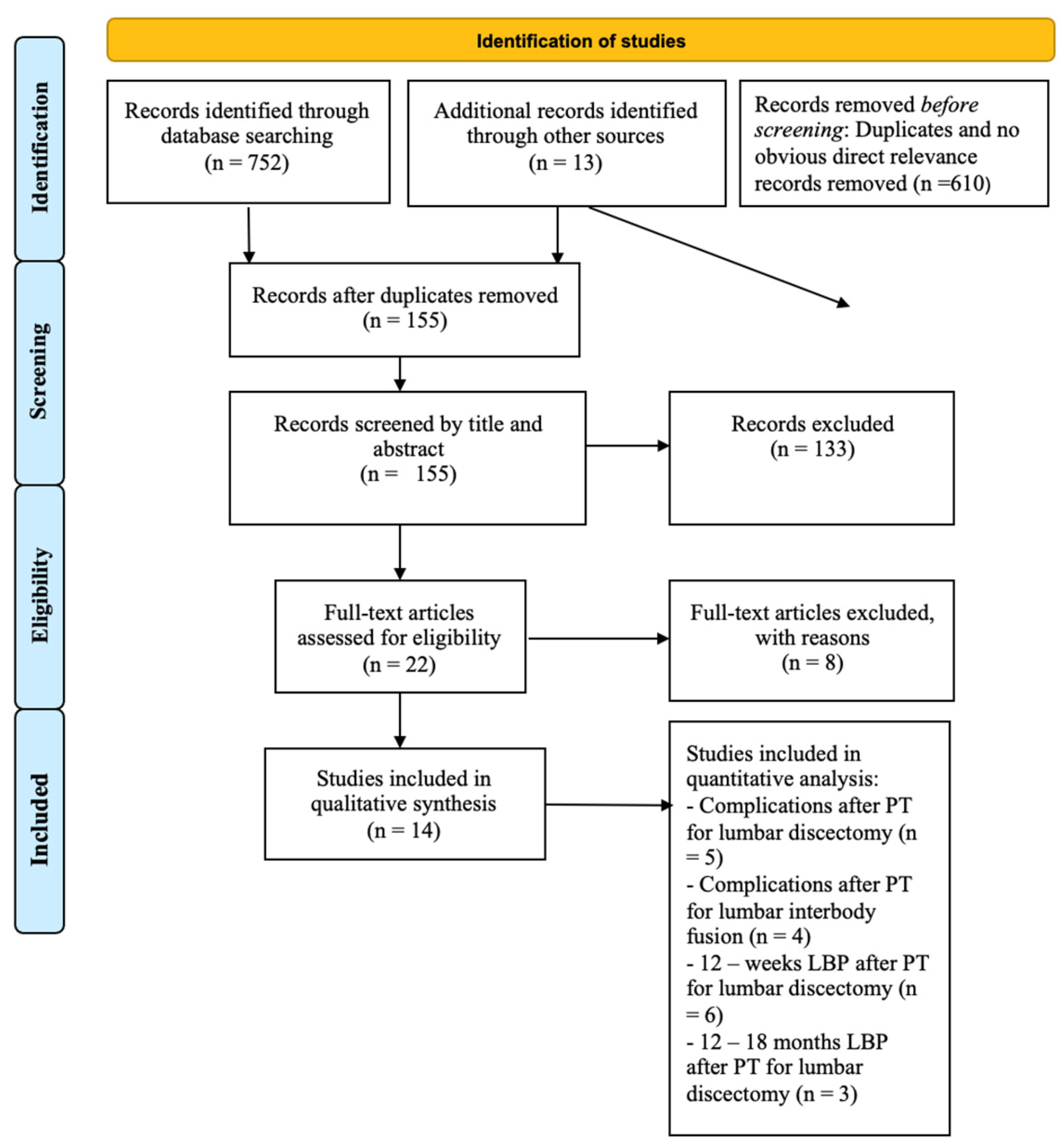
2.3. Study Selection
2.4. Data Extraction
2.5. Methodological Quality Assessment of Included Studies
2.6. Statistical Analysis
3. Results
3.1. Included Studies and Population
3.2. Risk of Bias Assessment
3.3. Timing of Physical Therapy
3.4. Outcomes Evaluated
4. Discussion
4.1. Limitations of the Study
4.2. Conclusions of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fehlings, M.G.; Tetreault, L.; Nater, A.; Choma, T.; Harrop, J.; Mroz, T.; Santaguida, C.; Smith, J.S. The Aging of the Global Population: The Changing Epidemiology of Disease and Spinal Disorders. Neurosurgery 2015, 77, S1–S5. [Google Scholar] [CrossRef] [PubMed]
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Męczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) Approach to Healthy Ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Kotwal, S.; Pumberger, M.; Hughes, A.; Girardi, F. Degenerative Scoliosis: A Review. HSS J. 2011, 7, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.N.; Zimmerman, Z.E.; Mass, H.; Makhni, M.C. Diagnosis and Management of Lumbar Spinal Stenosis: A Review. Jama 2022, 327, 1688–1699. [Google Scholar] [CrossRef] [PubMed]
- Aebi, M. The Adult Scoliosis. Eur. Spine J. 2005, 14, 925–948. [Google Scholar] [CrossRef]
- Ostelo, R.W.; De Vet, H.C.; Waddell, G.; Kerckhoffs, M.R.; Leffers, P.; Van Tulder, M. Rehabilitation Following First-Time Lumbar Disc Surgery. Spine 2003, 28, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Snowdon, M.; Peiris, C.L. Physiotherapy Commenced Within the First Four Weeks Post-Spinal Surgery Is Safe and Effective: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2016, 97, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Millisdotter, M.; Strömqvist, B. Early Neuromuscular Customized Training after Surgery for Lumbar Disc Herniation: A Prospective Controlled Study. Eur. Spine J. 2007, 16, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Oestergaard, L.G.; Nielsen, C.V.; Bünger, C.E.; Sogaard, R.; Fruensgaard, S.; Helmig, P.; Christensen, F.B. The Effect of Early Initiation of Rehabilitation after Lumbar Spinal Fusion: A Randomized Clinical Study. Spine 2012, 37, 1803–1809. [Google Scholar] [CrossRef]
- Zaed, I.; Bossi, B.; Ganau, M.; Tinterri, B.; Giordano, M.; Chibbaro, S. Current State of Benefits of Enhanced Recovery After Surgery (ERAS) in Spinal Surgeries: A Systematic Review of the Literature. Neurochirurgie 2022, 68, 61–68. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalgh, T.; Heneghan, C.; Liberati, A.; Hodgkinson, M. The Oxford 2011 Levels of Evidence. Oxford Centre Evidence-Based Medicine. Available online: http://www.cebm.net/index.aspx?o=5653 (accessed on 3 March 2024).
- Sideri, S.; Papageorgiou, S.N.; Eliades, T. Registration in the International Prospective Register of Systematic Reviews (PROSPERO) of Systematic Review Protocols Was Associated with Increased Review Quality. J. Clin. Epidemiol. 2018, 100, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Crocker, T.F.; Lam, N.; Jordão, M.; Brundle, C.; Prescott, M.; Forster, A.; Ensor, J.; Gladman, J.; Clegg, A. Risk-of-Bias Assessment Using Cochrane’s Revised Tool for Randomized Trials (RoB 2) Was Useful but Challenging and Resource-Intensive: Observations from a Systematic Review. J. Clin. Epidemiol. 2023, 161, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Kjellby-Wendt, G.; Styf, J. Early Active Training after Lumbar Discectomy: A Prospective, Randomized, and Controlled Study. Spine 1998, 23, 2345–2351. [Google Scholar] [CrossRef] [PubMed]
- Oestergaard, L.G.; Nielsen, C.V.; Bünger, C.E.; Svidt, K.; Christensen, F.B. The Effect of Timing of Rehabilitation on Physical Performance after Lumbar Spinal Fusion: A Randomized Clinical Study. Eur. Spine J. 2013, 22, 1884–1890. [Google Scholar] [CrossRef] [PubMed]
- Oestergaard, L.G.; Christensen, F.B.; Nielsen, C.V.; Bünger, C.E.; Fruensgaard, S.; Sogaard, R. Early versus Late Initiation of Rehabilitation after Lumbar Spinal Fusion: Economic Evaluation alongside a Randomized Controlled Trial. Spine 2013, 38, 1979–1985. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Zhang, S.J.; Wang, X.J. Postoperative Functional Exercise for Patients Who Underwent Percutaneous Transforaminal Endoscopic Discectomy for Lumbar Disc Herniation. Eur. Rev. Med. Pharmacol. Sci. 2021, 22, 15–22. [Google Scholar] [CrossRef]
- Kernc, D.; Strojnik, V.; Vengust, R. Early Initiation of a Strength Training Based Rehabilitation after Lumbar Spine Fusion Improves Core Muscle Strength: A Randomized Controlled Trial. J. Orthop. Surg. Res. 2018, 13, 151. [Google Scholar] [CrossRef] [PubMed]
- Kjellby-Wendt, G.; Styf, J.; Carlsson, S.G. Early Active Rehabilitation after Surgery for Lumbar Disc Herniation: A Prospective, Randomized Study of Psychometric Assessment in 50 Patients. Acta Orthop. Scand. 2001, 72, 518–524. [Google Scholar] [CrossRef]
- Erdogmus, C.B.; Resch, K.L.; Sabitzer, R.; Müller, H.; Nuhr, M.; Schöggl, A.; Posch, M.; Osterode, W.; Ungersböck, K.; Ebenbichler, G.R. Physiotherapy-Based Rehabilitation Following Disc Herniation Operation: Results of a Randomized Clinical Trial. Spine 2007, 32, 2041–2049. [Google Scholar] [CrossRef]
- Ju, S.; Park, G.; Kim, E. Effects of an Exercise Treatment Program on Lumbar Extensor Muscle Strength and Pain of Rehabilitation Patients Recovering from Lumbar Disc Herniation Surgery. J. Phys. Ther. Sci. 2012, 24, 515–518. [Google Scholar] [CrossRef]
- Newsome, R.J.; May, S.; Chiverton, N.; Cole, A.A. A Prospective, Randomised Trial of Immediate Exercise Following Lumbar Microdiscectomy: A Preliminary Study. Physiotherapy 2009, 95, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Abbott, A.D.; Tyni-Lenné, R.; Hedlund, R. Early Rehabilitation Targeting Cognition, Behavior, and Motor Function after Lumbar Fusion: A Randomized Controlled Trial. Spine 2010, 35, 848–857. [Google Scholar] [CrossRef] [PubMed]
- Ogutluler Ozkara, G.; Ozgen, M.; Ozkara, E.; Armagan, O.; Arslantas, A.; Atasoy, M.A. Effectiveness of Physical Therapy and Rehabilitation Programs Starting Immediately after Lumbar Disc Surgery. Turk. Neurosurg. 2015, 25, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Oosterhuis, T.; Ostelo, R.W.; van Dongen, J.M.; Peul, W.C.; de Boer, M.R.; Bosmans, J.E.; Vleggeert-Lankamp, C.L.; Arts, M.P.; van Tulder, M.W. Early Rehabilitation after Lumbar Disc Surgery Is Not Effective or Cost-Effective Compared to No Referral: A Randomised Trial and Economic Evaluation. J. Physiother. 2017, 63, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Christensen, F.B.; Laurberg, I.; Bünger, C.E. Importance of the Back-Café Concept to Rehabilitation after Lumbar Spinal Fusion: A Randomized Clinical Study with a 2-Year Follow-Up. Spine 2003, 28, 2561–2569. [Google Scholar] [CrossRef]
- Kahanovitz, N.; Viola, K.; Muculloch, J. Limited Surgical Discectomy and Microdiscectomy: A Clinical Comparison. Spine 1989, 14, 79–81. [Google Scholar] [CrossRef]
- Salame, K.; Lidar, Z. Minimally Invasive Approach to Far Lateral Lumbar Disc Herniation: Technique and Clinical Results. Acta Neurochir. 2010, 152, 663–668. [Google Scholar] [CrossRef]
- Pourtaheri, S.; Issa, K.; Lord, E.; Ajiboye, R.; Drysch, A.; Hwang, K.; Faloon, M.; Sinha, K.; Emami, A. Paraspinal Muscle Atrophy After Lumbar Spine Surgery. Orthopedics 2016, 39, e209–e214. [Google Scholar] [CrossRef]
- Arja, H.; Tiina, K.; Ulla, T.; Jari, Y. Trunk Muscle Strength in Flexion, Extension, and Axial Rotation in Patients Managed with Lumbar Disc Herniation Surgery and in Healthy Control Subjects. Spine 2003, 28, 1068–1073. [Google Scholar] [CrossRef]
- Choi, J.H.; Jang, J.S.; Yoo, K.S.; Shin, J.M.; Jang, I.T. Functional Limitations Due to Stiffness after Long-Level Spinal Instrumented Fusion Surgery to Correct Lumbar Degenerative Flat Back. Spine 2018, 43, 1044–1051. [Google Scholar] [CrossRef] [PubMed]
- Rushton, A.; Heneghan, N.R.; Calvert, M.; Heap, A.; White, L.; Goodwin, P.C. Physiotherapy Post Lumbar Discectomy: Prospective Feasibility and Pilot Randomised Controlled Trial. PLoS ONE 2015, 10, e0142013. [Google Scholar] [CrossRef] [PubMed]
- Oosterhuis, T.; Costa, L.O.P.; Maher, C.G.; de Vet, H.C.W.; van Tulder, M.W.; Ostelo, R.W.J.G. Rehabilitation after Lumbar Disc Surgery. Cochrane Database Syst. Rev. 2014, 2014, CD003007. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors (Year) | Study Design (Level of Evidence) | Number of Patients (M:F) | Mean Age (±or Range or SD) (Years) | Surgery | Timing of PT | Intervention | Control | Outcomes | Complications |
|---|---|---|---|---|---|---|---|---|---|
| Kjellby-Wendt et al. (1998) [14] | Randomized controlled trial (I) | - Early active training program (EAT): 26 (18:8) - Control group: 26 (20:6) | - EAT group: 41 years (range, 24–68 years) - Control group: 39 years (range, 21–66 years) | Lumbar microdiscectomy | Postoperative day 1 in both groups, but control group had a less active program | Education, lumbar braces, stretching, muscular strengthening exercises | Patients in the control group were treated with a less active training program after lumbar discectomy (17 min shorter the first 6 weeks and 21 min shorter the last 6 weeks) | Patients rehabilitated according to the EAT program had significantly less intense pain and more range of motion in the lumbar spine at 12 weeks after surgery. One year after surgery, there was no significant difference between groups in duration of sick leave and treatment satisfaction, even though the patients in the early therapy group were more satisfied compared to the controls (88% vs. 67%) | - ETA: 1 reoperation, 1 spondylolisthesis - Control: 1 reoperation, 1 reoperation at the same level of the lumbar spine |
| Kjellby-Wendt et al. (2001) [15] | Prospective randomized study (II) | - Early treatment group (EAT): 26 (18:8) - Control: 24 (18:6) | - Treatment: 41 (24–68) - Control: 37 (26–66) | Lumbar microdiscectomy | Postoperative day 1 in both groups, but control group had a less active program | Exercises to restore mobility of the trunk, reduce local edema, and stretch legs. Patients were encouraged to swim or jog | Traditional, less active training program | Both groups improved pain severity and state of anxiety. The multidimensional pain inventory improved more in the EAT group | NS |
| Erdogmus et al. (2007) [16] | Randomized control trial (I) | - No therapy: 40 (25:15) - Sham therapy: 40 (21:19) - Physical therapy: 40 (21:19) | - No therapy: 41.8 ± 10.4 - Sham therapy: 42.3 ± 9.8 - Physical therapy: 39.8 ± 10.5 | Standard laminectomy and either discectomy or microdiscectomy procedure | Within the first postoperative week in both groups, but control group had sham therapy or no therapy at all until after the first 3 months | Education, stretching, endurance exercises | - No therapies for the first 3 postoperative months. - Sham therapy: only massages for 30 min | After 12 weeks, low back pain was significantly less in physical therapy group than in untreated group. After 1.5 years, there were no significant outcome differences, including secondary outcomes (return to work, patient satisfaction, and activity of daily living) | - No therapy: 2 re-herniations - Sham therapy: 2 re-herniations - Physical therapy: 1 re-herniation |
| Millisdotter et al. (2007) [8] | Prospective controlled trial, not randomized—Level II | - Total: 56 (36:20) - Early Training (ET): 25 (19:6) - Control: 31 (17:14) | - Total: 38 - ETG: 37 - CG: 31 | Open microscopic lumbar disc discectomy | - Early training group (ETG): 2 weeks after surgery - Control group (CG—traditional training): after 6 weeks | Education, neuromuscular closed-chain exercises | Control group (CG—traditional training): stabilization exercises mainly using different types of stationary gym equipment and focused on coordination and mobility | Early neuromuscular customized training had a superior effect on disability (RMQ and DRI), with a significant difference compared to traditional training at follow-up 12 months after surgery. No differences in terms of pain (VAS) between groups | - Early training: 2 revision surgeries - Control: 1 revision surgery |
| Newsome et al. (2009) [17] | Prospective randomized control trial (I) | - Intervention group: 15 (7:8) - Control: 15 (11:4) | - Intervention group: 38 (27–43.3) - Control: 37 (30.5–45) | Lumbar microdiscectomy | - Intervention group: postoperative hour 2 - Control: postoperative day 1 | Passive hip and knee flexion toward the chest. Mobilization out of bed and education | Started on postoperative day 1, similar care but no knee and hip flexion | Significantly reduced time to independent mobility and return to work (median 6 vs. 8 weeks in the intervention group compared with the control group). At 15 h after surgery, independent mobility was attained in 80 and 40% of the intervention and control groups, respectively. There were no significant differences in disability and pain scores at 4 weeks and 3 months | - Intervention: 1 recurrence of symptoms - Control: 1 recurrence of symptoms |
| Abbott et al. (2010) [18] | Randomized control trial (I) | - Total: 107 (41:66) - Control: 54 (23:31) - Physical therapy: 53 (18:35) | - Control: 50.3 ± 10 - Physical therapy: 51.0 ± 10.9 | Lumbar fusion surgery | Starting from postop week 3 in both groups, but controls had a less active program | Education, motor relearning exercises, cognitive behavioral relearning exercises | Patients in the control group received education on walking, daily living exercises, and activity restrictions | Physical therapy improved functional disability, self-efficacy, outcome expectancy, and fear of movement/(re)injury significantly more than control group at the respective follow-up occasions. Similar results occurred for pain coping, but group differences were non-significant at 2 to 3 years of follow-up | - Control: 2 removals of instrumentation, 1 adjacent-level degeneration, 2 pseudoarthroses - Physical therapy: 5 removals of instrumentation, 2 adjacent-level degenerations, 5 pseudoarthroses |
| Oestergaard et al. (2012) [9] | Randomized control trial (II) | - Total: 82 (38:44) - Intervention: 41 (21:20) - Control: 41 (17:24) | - 6 weeks: 52 ± 8.5 - 12 weeks: 51.3 ± 9.9 | Lumbar spine fusion for degenerative disc disease | - Intervention: starting at postop week 6 - Control: postop week 12 | Education, muscle strengthening, exercises focusing on trunk and large muscle groups | The same physical therapy protocol, but started at 12 weeks | According to the Oswestry Disability Index, at 1-year follow-up, the 6-week group had significantly lower median reduction compared to the 12-week group. The Dallas Pain Questionnaire showed the same tendency overall, and daily activities were significantly reduced in favor of the 12-week group. For back pain, the 6-week group had a median reduction similar to the 12-week group. The results at 6 months of follow-up were similar. No difference was found in return to work 1 year post-surgery | - 6 weeks: 3 revision surgeries, 2 removals of instrumentation - 12 weeks: 5 revision surgeries, 2 removals of instrumentation |
| Ju et al. (2012) [19] | Randomized control trial (II) | - Exercise therapy group (ETG): 7 - Control: 7 | - ETG: 45.2 ± 3.96 - CONG: 46.2 ± 5.3 | Lumbar disc discectomy | - Exercise Therapy Group: postoperative week 2 - Control: no physical therapy | Lumbar extension program, resistance exercises | The control group did not participate in any exercise rehabilitation programs | ETG showed significant improvements in all items that measured lumbar extensor muscle strength and pain after the intervention, but the control group did not exhibit any significant improvements | NS |
| Oestergaard et al. (2013) [20] | Randomized control trial (I) | - Total: 82 (38:44) - 6 weeks: 41 (21:20) - 12 weeks: 41 (17:24) | - 6 weeks: 52 ± 8.5 - 12 weeks: 51.3 ± 9.9 | Lumbar spine fusion for degenerative disc disease | - Intervention: starting at postop week 6 - Control: postop week 12 | Education, muscle strengthening, exercises focusing on trunk and large muscle groups | The same physical therapy protocol, but started at 12 weeks | No statistically significant difference was found in walking distance or fitness over time. In both groups, the patients achieved an overall increase in walking distance but no improvement in fitness | - 6 weeks: 3 revision surgeries, 2 removals of instrumentation - 12 weeks: 5 revision surgeries, 2 removals of instrumentation |
| Oestergaard et al. (2013) [21] | Randomized control trial (I) | - Total: 82 (38:44) - 6 weeks: 41 (21:20) - 12 weeks: 41 (17:24) | - 6 weeks: 52 ± 8.5 - 12 weeks: 51.3 ± 9.9 | Lumbar spine fusion for degenerative disc disease | - Intervention: starting at postop week 6 - Control: postop week 12 | Education, muscle strengthening, exercises focusing on trunk and large muscle groups | The same physical therapy protocol, but started at 12 weeks | The 6w group had significantly poorer outcome in relation to functional disability than the 12w group. The same tendency was found for QALY, although this difference was not statistically significant | - 6 weeks: 2 readmissions before rehabilitation - 12 weeks: 1 readmission before rehabilitation |
| Ozkara et al. (2015) [22] | Prospective randomized control study (II) | - Treatment group: 15 (6:9) - Control: 15 (7:8) | - Treatment group: 48.5 ± 11.9 - Control: 44.1 ± 8.8 | Lumbar disc discectomy | Postoperative day 1 in both groups, but control group did not perform any exercises but only education | Education, exercises for pelvic tilt, abdominal and isometric quadriceps strengthening. Back exercises, leg raises, and hip flexions were added after the sixth week | Only instructions regarding lying, standing, sitting, and walking | When the groups were compared at week 12, a statistically significant difference was found in the VAS, Oswestry Low Back Pain Disability Questionnaire, and physical functioning of the SF-36, including body pain and social functioning subparameters. There was no significant difference in terms of return to work and patient satisfaction | NS |
| Oosterhuis et al. (2017) [23] | Multicenter, randomized, controlled trial (I) | - Experimental group: 92 (38:54) - Control: 77 (20:57) | - Exp: 47 (12) - Con: 47 (12) | Lumbar disc discectomy | - Experimental group: starting the first week after discharge - Control: only education after discharge | Education, daily activity training, gradually increasing intensity of exercises | Participants assigned to the control group were not referred for rehabilitation after discharge from the hospital | No clinically relevant or statistically significant overall mean differences between rehabilitation and control for any outcome adjusted for baseline characteristics (global perceived recovery, functional status, leg pain, back pain, physical health, and mental health) | - Exp: 1 nerve root injury, 2 dural tears - Control: 1 nerve root injury, 2 dural tears, 1 increase in sensimotor deficit |
| Kernc et al. (2018) [24] | Randomized controlled trial (I) | - Control group: 14 (5:9) - Training group: 13 (9:4) | - Control group: 60.3 ± 8.1 - Training group: 61.1 ± 8 | One-level instrumented trans-foraminal interbody fusion | - Training group: starting 3 weeks after the surgery - Control group: started 3 months postoperatively | Isometric exercises focused on trunk extension, flexion, and lateral flexion muscles. Leg adduction and hip extension | - Control group: no exercises or physical therapy prior to 3 months postoperatively | Both groups improved their walking speed after 3 months, although improvement in the training group was significantly greater than that in the control group. The training group significantly improved in all isometric trunk muscle measurements | - Training group: 0 - Control group: 2 hardware loosenings |
| Zhang et al. (2021) [25] | Randomized controlled trial (I) | - Total: 92 (48:44) - Intervention group: 46 - Control group: 46 | 57.4 ± 6.1 (20–68) | Percutaneous trans-foraminal endoscopic discectomy | - Intervention group: started at postoperative day 1 - Control group: no exercises were performed | Education, daily activity training, extension and flexion exercises of lower limbs, back muscle exercises | Control group performed routine functional exercises after their operations (not mentioned when) | Scores for residual lumbocrural pain, straight leg raising, muscle strength, sensory (skin), nerve reflex, and lumbar function of patients in the intervention group were significantly better than those of the control group | NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruffilli, A.; Manzetti, M.; Cargeli, A.; Viroli, G.; Ialuna, M.; Traversari, M.; Vita, F.; Giannini, I.S.; Faldini, C. Unveiling Timetable for Physical Therapy after Single-Level Lumbar Surgery for Degenerative Disc Disease: Insights from a Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 2553. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092553
Ruffilli A, Manzetti M, Cargeli A, Viroli G, Ialuna M, Traversari M, Vita F, Giannini IS, Faldini C. Unveiling Timetable for Physical Therapy after Single-Level Lumbar Surgery for Degenerative Disc Disease: Insights from a Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(9):2553. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092553
Chicago/Turabian StyleRuffilli, Alberto, Marco Manzetti, Alessandro Cargeli, Giovanni Viroli, Marco Ialuna, Matteo Traversari, Fabio Vita, Isabella Sofia Giannini, and Cesare Faldini. 2024. "Unveiling Timetable for Physical Therapy after Single-Level Lumbar Surgery for Degenerative Disc Disease: Insights from a Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 9: 2553. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092553