
No Detectable Differences in microRNA Plasma Levels between Diabetic Hypertensive Patients with and without Incident Subclinical Atrial Fibrillation

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Device Implantation and AF Definitions
2.3. RNA Extraction
2.4. Reverse Transcription-Quantitative Polymerase Chain Reaction (RT-qPCR)
2.5. Normalization
2.6. Data Acquisition and Statistical Analyses
3. Results
3.1. Characteristics of the Study Population
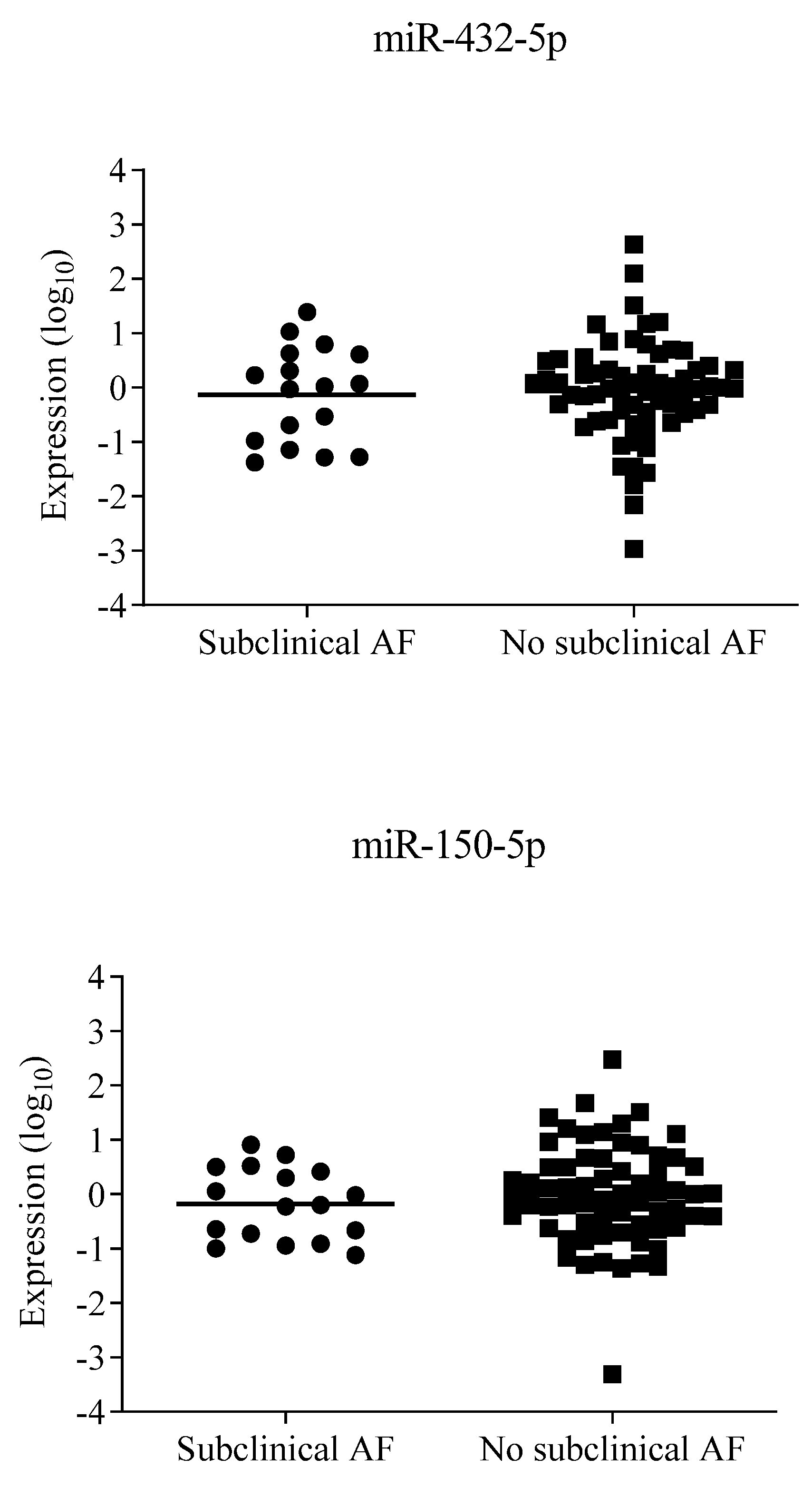
3.2. MicroRNA Findings
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wolf, P.A.; Abbott, R.D.; Kannel, W.B. Atrial fibrillation as an independent risk factor for stroke: The Framingham Study. Stroke 1991, 22, 983–988. [Google Scholar] [CrossRef]
- Stewart, S.; Hart, C.L.; Hole, D.J.; McMurray, J.J. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am. J. Med. 2002, 113, 359–364. [Google Scholar] [CrossRef]
- Freedman, B.; Camm, J.; Calkins, H.; Healey, J.S.; Rosenqvist, M.; Wang, J.; Albert, C.M.; Anderson, C.S.; Antoniou, S.; Benjamin, E.J.; et al. Screening for Atrial Fibrillation: A Report of the AF-SCREEN International Collaboration. Circulation 2017, 135, 1851–1867. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Camm, A.J.; Goette, A.; Brandes, A.; Eckardt, L.; Elvan, A.; Fetsch, T.; van Gelder, I.C.; Haase, D.; Haegeli, L.M.; et al. Early Rhythm-Control Therapy in Patients with Atrial Fibrillation. N. Engl. J. Med. 2020, 383, 1305–1316. [Google Scholar] [CrossRef] [PubMed]
- Andrade, J.G.; Deyell, M.W.; Macle, L.; Wells, G.A.; Bennett, M.; Essebag, V.; Champagne, J.; Roux, J.-F.; Yung, D.; Skanes, A.; et al. Progression of Atrial Fibrillation after Cryoablation or Drug Therapy. N. Engl. J. Med. 2023, 388, 105–116. [Google Scholar] [CrossRef]
- Solheim, E.; Off, M.K.; Hoff, P.I.; De Bortoli, A.; Schuster, P.; Ohm, O.-J.; Chen, J. N-terminal pro-B-type natriuretic peptide level at long-term follow-up after atrial fibrillation ablation: A marker of reverse atrial remodelling and successful ablation. J. Interv. Card. Electrophysiol. 2012, 34, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Cao, H.; Su, L.; Ling, Z.; Liu, Z.; Lan, X.; Xu, Y.; Chen, W.; Yin, Y. NT-proBNP, but not ANP and C-reactive protein, is predictive of paroxysmal atrial fibrillation in patients undergoing pulmonary vein isolation. J. Interv. Card. Electrophysiol. 2012, 33, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Kara, K.; Geisel, M.H.; Möhlenkamp, S.; Lehmann, N.; Kälsch, H.; Bauer, M.; Neumann, T.; Dragano, N.; Moebus, S.; Jöckel, K.-H.; et al. B-type natriuretic peptide for incident atrial fibrillation—The Heinz Nixdorf Recall Study. J. Cardiol. 2015, 65, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Latini, R.; Masson, S.; Pirelli, S.; Barlera, S.; Pulitano, G.; Carbonieri, E.; Gulizia, M.; Vago, T.; Favero, C.; Zdunek, D.; et al. Circulating cardiovascular biomarkers in recurrent atrial fibrillation: Data from the GISSI-Atrial Fibrillation Trial. J. Intern. Med. 2011, 269, 160–171. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, L. B-type natriuretic peptide levels in patients with paroxysmal lone atrial fibrillation. Heart Vessel. 2006, 21, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Hussein, A.A.; Bartz, T.M.; Gottdiener, J.S.; Sotoodehnia, N.; Heckbert, S.R.; Lloyd-Jones, D.; Kizer, J.R.; Christenson, R.; Wazni, O.; Defilippi, C. Serial measures of cardiac troponin T levels by a highly sensitive assay and incident atrial fibrillation in a prospective cohort of ambulatory older adults. Heart Rhythm 2015, 12, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Filion, K.B.; Agarwal, S.K.; Ballantyne, C.M.; Eberg, M.; Hoogeveen, R.C.; Huxley, R.R.; Loehr, L.R.; Nambi, V.; Soliman, E.Z.; Alonso, A. High-sensitivity cardiac troponin T and the risk of incident atrial fibrillation: The Atherosclerosis Risk in Communities (ARIC) study. Am. Heart J. 2015, 169, 31–38.e3. [Google Scholar] [CrossRef] [PubMed]
- Wachter, R.; Lahno, R.; Haase, B.; Weber-Krüger, M.; Seegers, J.; Edelmann, F.; Wohlfahrt, J.; Gelbrich, G.; Görlitz, A.; Kermer, P.; et al. Natriuretic Peptides for the Detection of Paroxysmal Atrial Fibrillation in Patients with Cerebral Ischemia—The Find-AF Study. PLoS ONE 2012, 7, e34351. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Yang, B.; Nattel, S. MicroRNAs and atrial fibrillation: Mechanisms and translational potential. Nat. Rev. Cardiol. 2015, 12, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Gilad, S.; Meiri, E.; Yogev, Y.; Benjamin, S.; Lebanony, D.; Yerushalmi, N.; Benjamin, H.; Kushnir, M.; Cholakh, H.; Melamed, N.; et al. Serum MicroRNAs Are Promising Novel Biomarkers. PLoS ONE 2008, 3, e3148. [Google Scholar] [CrossRef] [PubMed]
- Bartel, D.P. MicroRNAs: Genomics, biogenesis, mechanism, and function. Cell 2004, 116, 281–297. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Hannon, G.J. MicroRNAs: Small RNAs with a big role in gene regulation. Nat. Rev. Genet. 2004, 5, 522–531. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Zhang, C. MicroRNAs in Vascular Disease. J. Cardiovasc. Pharmacol. 2011, 57, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Bhaskaran, M.; Mohan, M. MicroRNAs: History, biogenesis, and their evolving role in animal development and disease. Vet. Pathol. 2014, 51, 759–774. [Google Scholar] [CrossRef] [PubMed]
- Soifer, H.S.; Rossi, J.J.; Sætrom, P. MicroRNAs in Disease and Potential Therapeutic Applications. Mol. Ther. 2007, 15, 2070–2079. [Google Scholar] [CrossRef] [PubMed]
- Filipowicz, W.; Bhattacharyya, S.N.; Sonenberg, N. Mechanisms of post-transcriptional regulation by microRNAs: Are the answers in sight? Nat. Rev. Genet. 2008, 9, 102–114. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, J.; Hayder, H.; Zayed, Y.; Peng, C. Overview of MicroRNA Biogenesis, Mechanisms of Actions, and Circulation. Front. Endocrinol. 2018, 9, 402. [Google Scholar] [CrossRef] [PubMed]
- Santulli, G.; Iaccarino, G.; De Luca, N.; Trimarco, B.; Condorelli, G. Atrial fibrillation and microRNAs. Front. Physiol. 2014, 5, 15. [Google Scholar] [CrossRef] [PubMed]
- Ravelli, F.; Masè, M. MicroRNAs: New contributors to mechano-electric coupling and atrial fibrillation. Prog. Biophys. Mol. Biol. 2021, 159, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Adam, O.; Löhfelm, B.; Thum, T.; Gupta, S.K.; Puhl, S.-L.; Schäfers, H.-J.; Böhm, M.; Laufs, U. Role of miR-21 in the pathogenesis of atrial fibrosis. Basic Res. Cardiol. 2012, 107, 278. [Google Scholar] [CrossRef] [PubMed]
- Dawson, K.; Wakili, R.; Ördög, B.; Clauss, S.; Chen, Y.; Iwasaki, Y.; Voigt, N.; Qi, X.Y.; Sinner, M.F.; Dobrev, D.; et al. MicroRNA29: A mechanistic contributor and potential biomarker in atrial fibrillation. Circulation 2013, 127, 1466–1475. [Google Scholar] [CrossRef] [PubMed]
- McManus, D.D.; Tanriverdi, K.; Lin, H.; Esa, N.; Kinno, M.; Mandapati, D.; Tam, S.; Okike, O.N.; Ellinor, P.T.; Keaney, J.F., Jr.; et al. Plasma microRNAs are associated with atrial fibrillation and change after catheter ablation (the miRhythm study). Heart Rhythm 2015, 12, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Zhou, C.; Liu, Y.; Wang, S.; Ye, P.; Miao, X.; Xia, J. The Expression Levels of Plasma micoRNAs in Atrial Fibrillation Patients. PLoS ONE 2012, 7, e44906. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Zhang, Y.; Wang, N.; Pan, Z.; Gao, X.; Zhang, F.; Zhang, Y.; Shan, H.; Luo, X.; Bai, Y.; et al. MicroRNA-328 Contributes to Adverse Electrical Remodeling in Atrial Fibrillation. Circulation 2010, 122, 2378–2387. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Zhong, S.; Rao, F.; Xue, Y.; Qi, Z.; Wu, S. Catheter ablation restores decreased plasma miR-409-3p and miR-432 in atrial fibrillation patients. Europace 2016, 18, 92–99. [Google Scholar] [CrossRef] [PubMed]
- McManus, D.D.; Lin, H.; Tanriverdi, K.; Quercio, M.; Yin, X.; Larson, M.G.; Ellinor, P.T.; Levy, D.; Freedman, J.E.; Benjamin, E.J. Relations between circulating microRNAs and atrial fibrillation: Data from the Framingham Offspring Study. Heart Rhythm 2014, 11, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Vaze, A.; Tran, K.-V.; Tanriverdi, K.; Sardana, M.; Lessard, D.; Donahue, J.K.; Barton, B.; Aurigemma, G.; Lubitz, S.A.; Lin, H.; et al. Relations between plasma microRNAs, echocardiographic markers of atrial remodeling, and atrial fibrillation: Data from the Framingham Offspring study. PLoS ONE 2020, 15, e0236960. [Google Scholar] [CrossRef] [PubMed]
- Geurts, S.; Mens, M.M.J.; Bos, M.M.; Ikram, M.A.; Ghanbari, M.; Kavousi, M. Circulatory MicroRNAs in Plasma and Atrial Fibrillation in the General Population: The Rotterdam Study. Genes 2022, 13, 11. [Google Scholar] [CrossRef] [PubMed]
- Benito, B.; García-Elías, A.; Ois, Á.; Tajes, M.; Vallès, E.; Ble, M.; Bisbe, L.Y.; Giralt-Steinhauer, E.; Rodríguez-Campello, A.; Capdevila, M.C.; et al. Plasma levels of miRNA-1-3p are associated with subclinical atrial fibrillation in patients with cryptogenic stroke. Rev. Esp. Cardiol. Engl. Ed. 2022, 75, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Philippsen, T.J.; Christensen, L.S.; Hansen, M.G.; Dahl, J.S.; Brandes, A. Detection of Subclinical Atrial Fibrillation in High-Risk Patients Using an Insertable Cardiac Monitor. JACC Clin. Electrophysiol. 2017, 3, 1557–1564. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Pokushalov, E.; Urban, L.; Taborsky, M.; Kuck, K.-H.; Lebedev, D.; Rieger, G.; Pürerfellner, H. Performance of a New Leadless Implantable Cardiac Monitor in Detecting and Quantifying Atrial Fibrillation Results of the XPECT Trial. Circ. Arrhythmia Electrophysiol. 2010, 3, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc. Natl. Acad. Sci. USA 2008, 105, 10513–10518. [Google Scholar] [CrossRef]
- Kroh, E.M.; Parkin, R.K.; Mitchell, P.S.; Tewari, M. Analysis of circulating microRNA biomarkers in plasma and serum using quantitative reverse transcription-PCR (qRT-PCR). Methods 2010, 50, 298–301. [Google Scholar] [CrossRef] [PubMed]
- Hellemans, J.; Mortier, G.; De Paepe, A.; Speleman, F.; Vandesompele, J. qBase relative quantification framework and software for management and automated analysis of real-time quantitative PCR data. Genome Biol. 2007, 8, R19. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Wu, N.; Zhang, Z.; Zhong, L.; Li, G.; Li, Y. Non-coding RNA and arrhythmias: Expression, function, and molecular mechanism. Europace 2023, 25, 1296–1308. [Google Scholar] [CrossRef] [PubMed]
- Nattel, S.; Harada, M. Atrial remodeling and atrial fibrillation: Recent advances and translational perspectives. J. Am. Coll. Cardiol. 2014, 63, 2335–2345. [Google Scholar] [CrossRef] [PubMed]
- Creemers, E.E.; Tijsen, A.J.; Pinto, Y.M. Circulating microRNAs: Novel biomarkers and extracellular communicators in cardiovascular disease? Circ. Res. 2012, 110, 483–495. [Google Scholar] [CrossRef] [PubMed]
- Reyes-García, A.M.d.L.; Zapata-Martínez, L.; Águila, S.; Lozano, M.L.; Martínez, C.; González-Conejero, R. microRNAs as biomarkers of risk of major adverse cardiovascular events in atrial fibrillation. Front. Cardiovasc. Med. 2023, 10, 1135127. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, C.C.; Kroh, E.; Wood, B.; Arroyo, J.D.; Dougherty, K.J.; Miyaji, M.M.; Tait, J.F.; Tewari, M. Blood Cell Origin of Circulating MicroRNAs: A Cautionary Note for Cancer Biomarker Studies. Cancer Prev. Res. 2012, 5, 492–497. [Google Scholar] [CrossRef] [PubMed]
- Mussbacher, M.; Krammer, T.L.; Heber, S.; Schrottmaier, W.C.; Zeibig, S.; Holthoff, H.-P.; Pereyra, D.; Starlinger, P.; Hackl, M.; Assinger, A. Impact of Anticoagulation and Sample Processing on the Quantification of Human Blood-Derived microRNA Signatures. Cells 2020, 9, 1915. [Google Scholar] [CrossRef] [PubMed]
- Kok, M.G.M.; de Ronde, M.W.J.; Moerland, P.D.; Ruijter, J.M.; Creemers, E.E.; Pinto-Sietsma, S.J. Small sample sizes in high-throughput miRNA screens: A common pitfall for the identification of miRNA biomarkers. Biomol. Detect. Quantif. 2018, 15, 1–5. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Included Patients (n = 82) | Subclinical AF (n = 17) | No Subclinical AF (n = 65) | p-Value | |
|---|---|---|---|---|
| Clinical parameters and medications | ||||
| Age (years) | 71 ± 4 | 73 ± 5 | 71 ± 4 | 0.11 |
| Men | 52 (63) | 12 (71) | 40 (62) | 0.49 |
| BMI (kg/m2) | 31 ± 5 | 30 ± 5 | 31 ± 5 | 0.55 |
| CHA2DS2-VASc score | 4 (3–4) | 4 (3–4) | 4 (3–4) | 0.44 |
| Cholesterol-lowering drugs | 72 (88) | 15 (88) | 57 (88) | 1.00 |
| Insulin treatment | 61 (74) | 14 (82) | 47 (72) | 0.54 |
| Oral antidiabetics | 61 (74) | 12 (71) | 49 (75) | 0.69 |
| Beta-blockers | 32 (39) | 7 (41) | 25 (38) | 0.84 |
| Diuretics | 68 (83) | 13 (76) | 55 (85) | 0.47 |
| Calcium channel blockers | 57 (70) | 10 (59) | 47 (72) | 0.28 |
| ACE-I/ARB | 79 (96) | 16 (94) | 63 (97) | 0.51 |
| No. of antihypertensive drugs | 4 (0.9) | 4 (0.9) | 4 (0.9) | 0.81 |
| Laboratory and echocardiographic parameters | ||||
| HbA1c (mmol/mol) | 60 ± 11 | 62 ± 11 | 60 ± 12 | 0.37 |
| Creatinine (µmol/L) | 88 (71–117) | 99 (91–109) | 85 (71–117) | 0.03 |
| LVEF (%) | 60 ± 7 | 61 ± 9 | 60 ± 7 | 0.58 |
| LA diameter (mm) | 36 ± 5 | 37 ± 5 | 35 ± 4 | 0.10 |
| LA volume index (mL/m2) | 30 ± 7 | 28 ± 7 | 30 ± 7 | 0.36 |
| LA maximum volume biplane (mL) | 60 ± 15 | 58 ± 16 | 60 ± 15 | 0.59 |
| LA minimum volume biplane (mL) | 22 ± 8 | 22 ± 7 | 23 ± 8 | 0.60 |
| LA emptying fraction (%) | 63 ± 8 | 63 ± 5 | 63 ± 8 | 0.76 |
| MicroRNA | Assay Number | Reference | Subclinical AF (n = 17) | No Subclinical AF (n = 65) | p-Value |
|---|---|---|---|---|---|
| miR-328-3p | 543 | [31] | −0.106 ± 0.754 | −0.031 ± 0.501 | 0.76 |
| miR-29b-3p | 413 | [26] | −0.016 ± 0.398 | 0.031 ± 0.818 | 0.85 |
| miR-21-5p | 397 | [27] | −0.085 ± 0.561 | 0.033 ± 0.488 | 0.63 |
| miR-432-5p | 1026 | [30] | −0.131 ± 0.287 | −0.056 ± 0.347 | 0.76 |
| miR-150-5p | 473 | [27] | −0.176 ± 0.218 | −0.005 ± 0.377 | 0.47 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feddersen, S.; Philippsen, T.J.; Hansen, M.S.; Christensen, L.S.; Nybo, M.; Brandes, A. No Detectable Differences in microRNA Plasma Levels between Diabetic Hypertensive Patients with and without Incident Subclinical Atrial Fibrillation. J. Clin. Med. 2024, 13, 2554. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092554
Feddersen S, Philippsen TJ, Hansen MS, Christensen LS, Nybo M, Brandes A. No Detectable Differences in microRNA Plasma Levels between Diabetic Hypertensive Patients with and without Incident Subclinical Atrial Fibrillation. Journal of Clinical Medicine. 2024; 13(9):2554. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092554
Chicago/Turabian StyleFeddersen, Søren, Tine J. Philippsen, Michael S. Hansen, Lene S. Christensen, Mads Nybo, and Axel Brandes. 2024. "No Detectable Differences in microRNA Plasma Levels between Diabetic Hypertensive Patients with and without Incident Subclinical Atrial Fibrillation" Journal of Clinical Medicine 13, no. 9: 2554. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092554