
Real-Life Effectiveness and Safety of Guselkumab in Patients with Psoriasis Who Have an Inadequate Response to Ustekinumab: A 3-Year Multicenter Study

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
Statistical Analysis
3. Results
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rendon, A.; Schäkel, K. Psoriasis Pathogenesis and Treatment. Int. J. Mol. Sci. 2019, 20, 1475. [Google Scholar] [CrossRef] [PubMed]
- Raharja, A.; Mahil, S.K.; Barker, J.N. Psoriasis: A brief overview. Clin. Med. 2021, 21, 170–173. [Google Scholar] [CrossRef] [PubMed]
- Korman, N.J. Management of psoriasis as a systemic disease: What is the evidence? Br. J. Dermatol. 2020, 182, 840–848. [Google Scholar] [CrossRef] [PubMed]
- Augustin, M.; Radtke, M.A. Quality of life in psoriasis patients. Expert. Rev. Pharmacoecon. Outcomes Res. 2014, 14, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Nast, A.; Smith, C.; Spuls, P.; Valle, G.A.; Bata-Csörgö, Z.; Boonen, H.; De Jong, E.; Garcia-Doval, I.; Gisondi, P.; Kaur-Knudsen, D.; et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis vulgaris—Part 1: Treatment and monitoring recommendations. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 2461–2498. [Google Scholar] [CrossRef] [PubMed]
- Nast, A.; Smith, C.; Spuls, P.; Valle, G.A.; Bata-Csörgö, Z.; Boonen, H.; De Jong, E.; Garcia-Doval, I.; Gisondi, P.; Kaur-Knudsen, D.; et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis vulgaris—Part 2: Specific clinical and comorbid situations. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 281–317. [Google Scholar] [CrossRef] [PubMed]
- Kamata, M.; Tada, Y. Efficacy and Safety of Biologics for Psoriasis and Psoriatic Arthritis and Their Impact on Comorbidities: A Literature Review. Int. J. Mol. Sci. 2020, 21, 1690. [Google Scholar] [CrossRef] [PubMed]
- Camela, E.; Potestio, L.; Fabbrocini, G.; Pallotta, S.; Megna, M. The holistic approach to psoriasis patients with comorbidities: The role of investigational drugs. Expert. Opin. Investig. Drugs. 2023, 32, 537–552. [Google Scholar] [CrossRef]
- Camela, E.; Potestio, L.; Fabbrocini, G.; Ruggiero, A.; Megna, M. New frontiers in personalized medicine in psoriasis. Expert. Opin. Biol. Ther. 2022, 22, 1431–1433. [Google Scholar] [CrossRef]
- Megna, M.; Balato, A.; Raimondo, A.; Balato, N. Guselkumab for the treatment of psoriasis. Expert. Opin. Biol. Ther. 2018, 18, 459–468. [Google Scholar] [CrossRef]
- Blauvelt, A.; Papp, K.A.; Griffiths, C.E.; Randazzo, B.; Wasfi, Y.; Shen, Y.-K.; Li, S.; Kimball, A.B. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the continuous treatment of patients with moderate to severe psoriasis: Results from the phase III, double-blinded, placebo- and active comparator-controlled VOYAGE 1 trial. J. Am. Acad. Dermatol. 2017, 76, 405–417. [Google Scholar] [PubMed]
- Reich, K.; Armstrong, A.W.; Foley, P.; Song, M.; Wasfi, Y.; Randazzo, B.; Li, S.; Shen, Y.-K.; Gordon, K.B. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the treatment of patients with moderate to severe psoriasis with randomized withdrawal and retreatment: Results from the phase III, double-blind, placebo- and active comparator-controlled VOYAGE 2 trial. J. Am. Acad. Dermatol. 2017, 76, 418–431. [Google Scholar] [PubMed]
- Langley, R.; Tsai, T.; Flavin, S.; Song, M.; Randazzo, B.; Wasfi, Y.; Jiang, J.; Li, S.; Puig, L. Efficacy and safety of guselkumab in patients with psoriasis who have an inadequate response to ustekinumab: Results of the randomized, double-blind, phase III NAVIGATE trial. Br. J. Dermatol. 2018, 178, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Reich, K.; Armstrong, A.W.; Langley, R.G.; Flavin, S.; Randazzo, B.; Li, S.; Hsu, M.-C.; Branigan, P.; Blauvelt, A. Guselkumab versus secukinumab for the treatment of moderate-to-severe psoriasis (ECLIPSE): Results from a phase 3, randomised controlled trial. Lancet 2019, 394, 831–839. [Google Scholar] [CrossRef] [PubMed]
- Cinelli, E.; Fabbrocini, G.; Megna, M. Real-world experience versus clinical trials: Pros and cons in psoriasis therapy evaluation. Int. J. Dermatol. 2022, 61, e107–e108. [Google Scholar] [CrossRef] [PubMed]
- Reid, C.; Griffiths, C.E.M. Psoriasis and Treatment: Past, Present and Future Aspects. Acta Derm. Venereol. 2020, 100, adv00032. [Google Scholar] [CrossRef] [PubMed]
- Klisic, A.; Bakic, M.; Karanikolic, V. Comparative Analysis of Redox Homeostasis Biomarkers in Patients with Psoriasis and Atopic Dermatitis. Antioxidants 2023, 12, 1875. [Google Scholar] [CrossRef]
- Tokuyama, M.; Mabuchi, T. New Treatment Addressing the Pathogenesis of Psoriasis. Int. J. Mol. Sci. 2020, 21, 7488. [Google Scholar] [CrossRef] [PubMed]
- Reich, K.; Bianchi, L.; Khemis, A.; Maul, J.-T.; Tsianakas, A.; Schempp, C.M.; Petersen, K.; Noergaard, M.M.; Puig, L. Brodalumab Versus Guselkumab in Patients with Moderate-to-Severe Psoriasis with an Inadequate Response to Ustekinumab: A Randomized, Multicenter, Double-Blind Phase 4 Trial (COBRA). Dermatol. Ther. 2024, 14, 453–468. [Google Scholar] [CrossRef]
- Berenguer-Ruiz, S.; Rivera, R.; Herranz, P.; De la Cueva, P.; Hospital, M.; Ruiz-Genao, D.; Roustan, G.; Daudén, E.; Llamas-Velasco, M. Ustekinumab to guselkumab transitions: A series of 54 patients emulating the navigate trial in real life. Dermatol. Ther. 2022, 35, e15757. [Google Scholar] [CrossRef]
- Fougerousse, A.-C.; Ghislain, P.-D.; Reguiai, Z.; Maccari, F.; Parier, J.; Auvray, D.B.; Chaby, G.; Pallure, V.; Schmutz, J.-L.; Clément, C.; et al. Effectiveness and short-term (16-week) tolerance of guselkumab for psoriasis under real-life conditions: A retrospective multicenter study. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e644–e646. [Google Scholar] [CrossRef] [PubMed]
- Gargiulo, L.; Ibba, L.; Malagoli, P.; Angileri, R.G.; Bardazzi, F.; Bernardini, N.; Burlando, M.; Carrera, C.G.; Chiricozzi, A.; Dapavo, P.; et al. Real-life effectiveness and safety of guselkumab in patients with psoriasis who have an inadequate response to ustekinumab: A 104-week multicenter retrospective study—IL PSO (ITALIAN LANDSCAPE PSORIASIS). J. Eur. Acad. Dermatol. Venereol. 2023, 37, 1017–1027. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, A.; Fabbrocini, G.; Cinelli, E.; Megna, M. Efficacy and safety of guselkumab in psoriasis patients who failed ustekinumab and/or anti-interleukin-17 treatment: A real-life 52-week retrospective study. Dermatol. Ther. 2021, 34, e14673. [Google Scholar] [CrossRef] [PubMed]
- Megna, M.; Potestio, L.; Ruggiero, A.; Camela, E.; Fabbrocini, G. Guselkumab is efficacious and safe in psoriasis patients who failed anti-IL17: A 52-week real-life study. J. DermatologTreat. 2022, 33, 2560–2564. [Google Scholar] [CrossRef] [PubMed]
- Megna, M.; Tommasino, N.; Potestio, L.; Battista, T.; Ruggiero, A.; Noto, M.; Fabbrocini, G.; Genco, L. Real-world practice indirect comparison between guselkumab, risankizumab, and tildrakizumab: Results from an Italian 28-week retrospective study. J. Dermatolog Treat. 2022, 33, 2813–2820. [Google Scholar] [CrossRef]
- Ruiz-Villaverde, R.; Rodriguez-Fernandez-Freire, L.; Armario-Hita, J.C.; Pérez-Gil, A.; Chinchay, F.V.; Galán-Gutiérrez, M. Guselkumab as a switching strategy after anti-TNFα, anti-IL17, or anti-IL12/23 therapies in moderate-to-severe psoriasis. Dermatol. Ther. 2022, 35, e15760. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Number of patients | 112 | |||||
| Sex: | ||||||
| Male | 70 (62.6%) | |||||
| Female | 42 (37.5%) | |||||
| Mean age(years) | 54.8 ± 11.7 | |||||
| Mean duration of psoriasis(years) | 20.2 ± 10.4 | |||||
| Psoriatic Arthritis | 53 (47.3%) | |||||
| Difficult-to-treat areas involvement | ||||||
| Scalp | 76 (67.9%) | |||||
| Palms or soles | 38 (33.9%) | |||||
| Genital | 42 (37.5%) | |||||
| Fingernails | 41 (36.6%) | |||||
| Comorbidities: | ||||||
| Hypertension | 41 (36.7%) | |||||
| Dyslipidemia | 34 (30.4%) | |||||
| Obesity | 27 (24.1%) | |||||
| Diabetes | 20 (17.9%) | |||||
| Cardiopathy | 10 (8.9%) | |||||
| Thyropathy | 7 (6.3%) | |||||
| Previous systemic treatments (conventional and small molecules): | ||||||
| Methotrexate | 50 (44.6%) | |||||
| Cyclosporine | 69 (61.6%) | |||||
| Nb-UVB Phototherapy | 37 (33.0%) | |||||
| P-UVA | 3 (2.7%) | |||||
| Acitretin | 25 (22.3%) | |||||
| Apremilast | 3 (2.7%) | |||||
| Naïve | 13 (11.6%) | |||||
| Previous biologic treatments: | ||||||
| Anti-TNFα | ||||||
| Adalimumab | 32 (28.6%) | |||||
| Etanercept | 27 (24.1%) | |||||
| Infliximab | 2 (1.8%) | |||||
| Golimumab | 1 (0.9%) | |||||
| Anti-IL12/23 | 112 (100%) | |||||
| Anti-IL17 | ||||||
| Secukinumab | 4 (3.6%) | |||||
| BASELINE | WEEK 16 | WEEK 36 | WEEK 52 | WEEK 104 | WEEK 156 | |
| Mean PASI | 10.1 ± 5.1 | 1.2 ± 1.9 | 1.1 ± 2.0 | 1.1 ± 2.0 | 0.7 ± 1.5 | 0.9 ± 2.2 |
| MeanDLQI | 16.4 ± 6.5 | 1.2 ± 2.7 | 1.7 ± 3.2 | 1.0 ± 2.1 | 0.2 ± 0.5 | 0 |
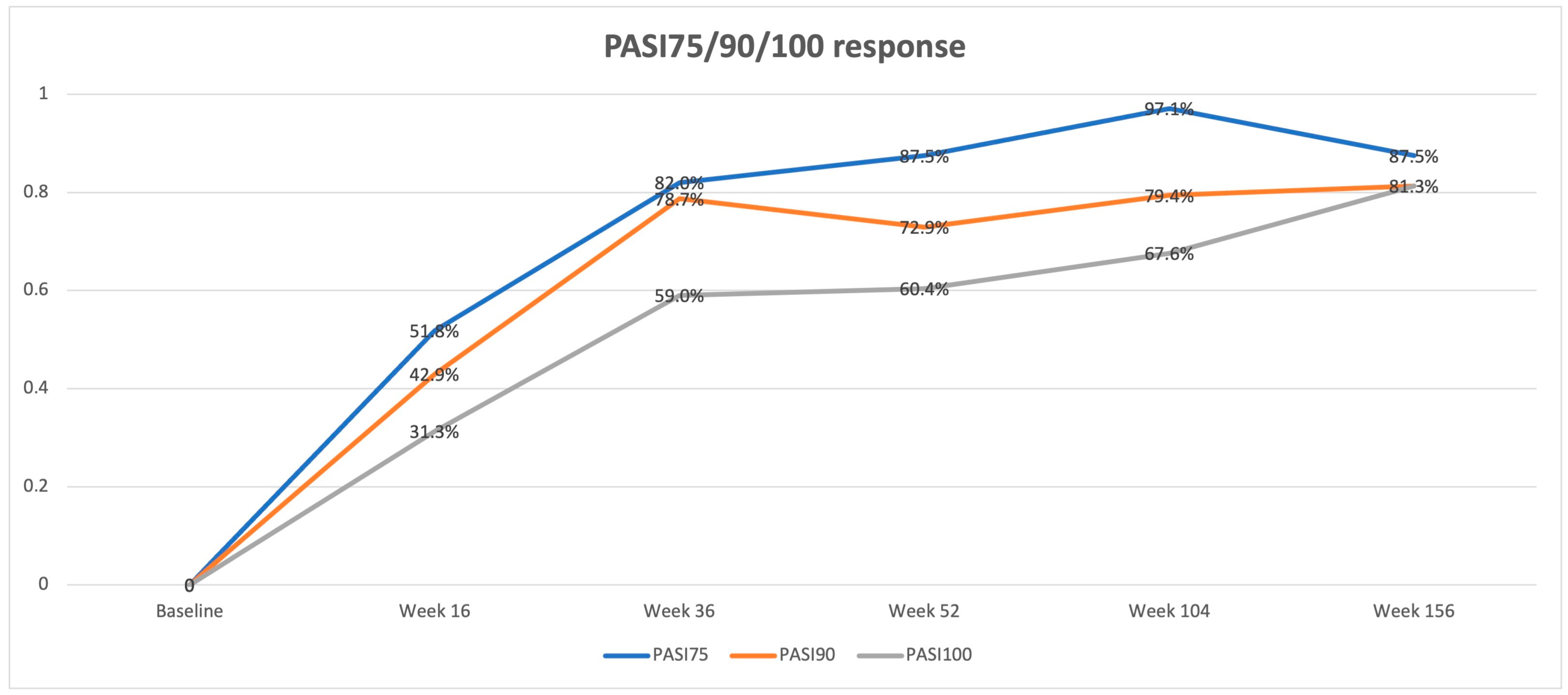
| PASI75 | / | 51.8% | 82.0% | 87.5% | 97.1% | 87.5% |
| PASI90 | / | 42.9% | 78.7% | 72.9% | 79.4% | 81.3% |
| PASI100 | / | 31.3% | 59.0% | 60.4% | 67.6% | 81.3% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Megna, M.; Balato, A.; Caccavale, S.; Cacciapuoti, S.; Calabrese, G.; Di Brizzi, E.V.; Di Costanzo, L.; Manzo, R.; Marino, V.; Puca, R.V.; et al. Real-Life Effectiveness and Safety of Guselkumab in Patients with Psoriasis Who Have an Inadequate Response to Ustekinumab: A 3-Year Multicenter Study. J. Clin. Med. 2024, 13, 2552. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092552
Megna M, Balato A, Caccavale S, Cacciapuoti S, Calabrese G, Di Brizzi EV, Di Costanzo L, Manzo R, Marino V, Puca RV, et al. Real-Life Effectiveness and Safety of Guselkumab in Patients with Psoriasis Who Have an Inadequate Response to Ustekinumab: A 3-Year Multicenter Study. Journal of Clinical Medicine. 2024; 13(9):2552. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092552
Chicago/Turabian StyleMegna, Matteo, Anna Balato, Stefano Caccavale, Sara Cacciapuoti, Giulia Calabrese, Eugenia Veronica Di Brizzi, Luisa Di Costanzo, Raffaella Manzo, Vincenzo Marino, Rosa Valentina Puca, and et al. 2024. "Real-Life Effectiveness and Safety of Guselkumab in Patients with Psoriasis Who Have an Inadequate Response to Ustekinumab: A 3-Year Multicenter Study" Journal of Clinical Medicine 13, no. 9: 2552. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092552