
Robot-Assisted Radical Prostatectomy Performed with the Novel Hugo™ RAS System: A Systematic Review and Pooled Analysis of Surgical, Oncological, and Functional Outcomes

 , , ,
, , ,  ,
,  , , , ,
, , , ,  , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Material and Methods
2.1. Search Strategy
2.2. Study Selection and Eligibility Criteria
2.3. Data Extraction and Outcome Measures
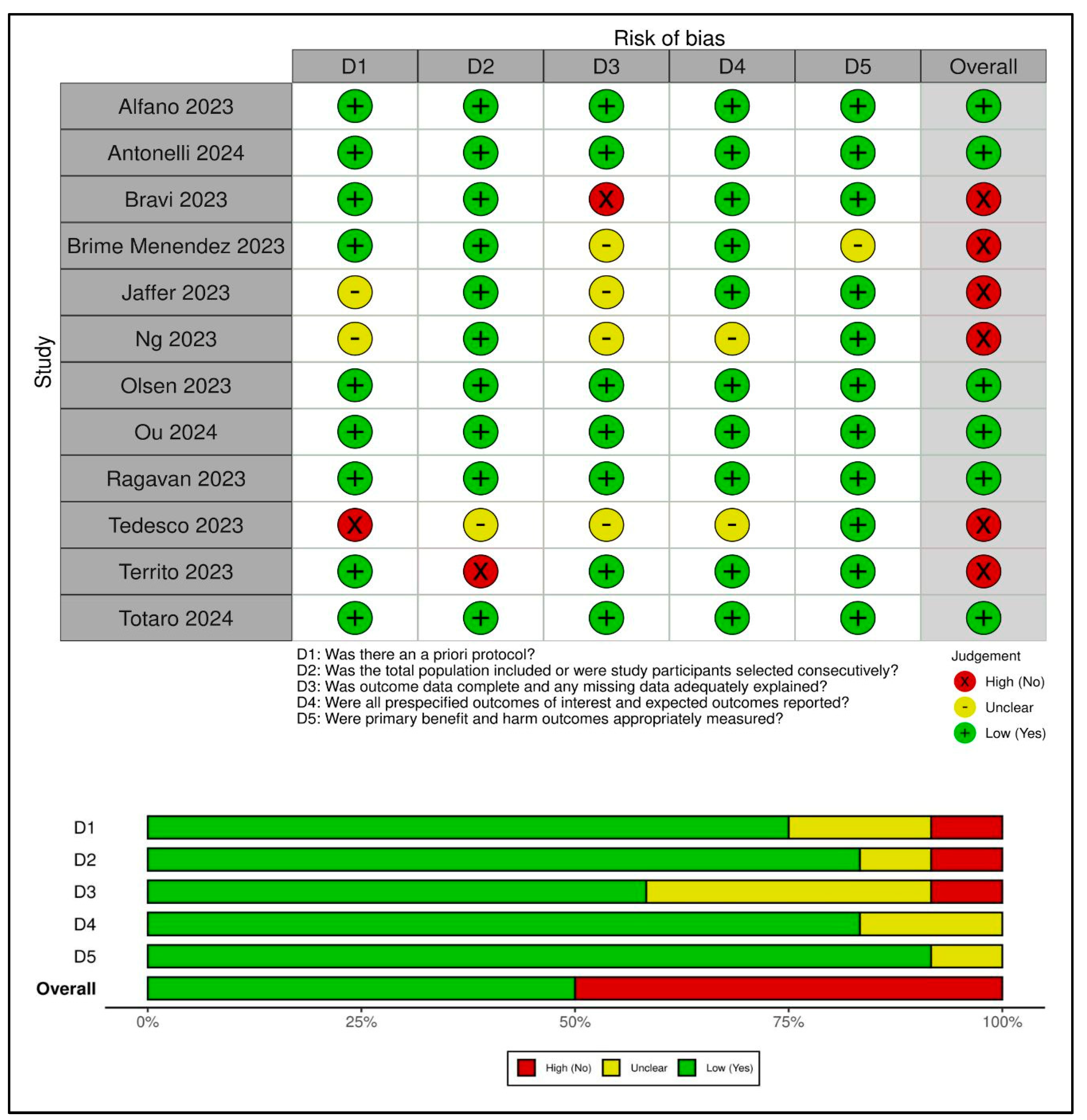
2.4. Study Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Selection and Characteristics
3.2. Risk of Bias
3.3. Baseline Patient Characteristics
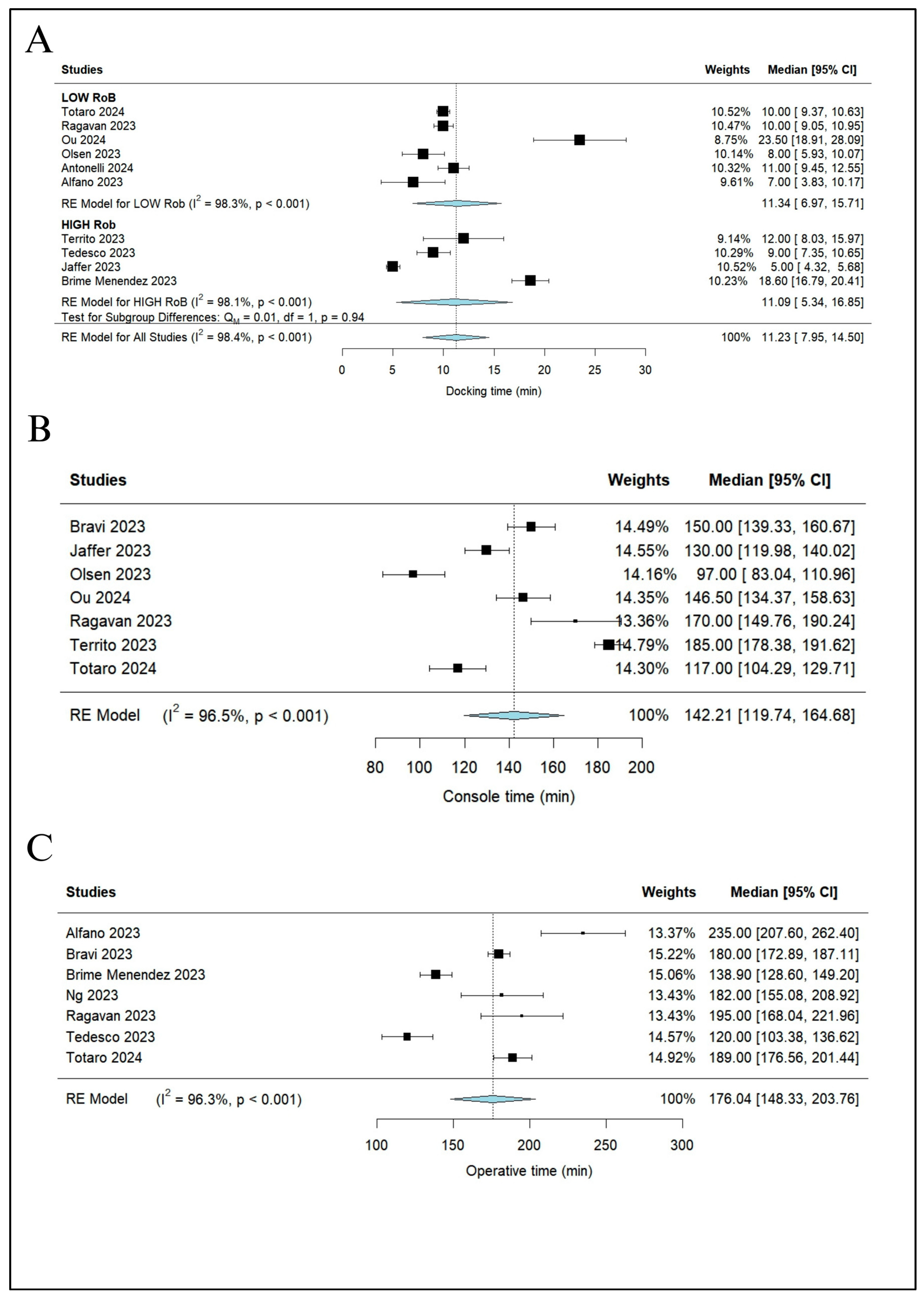
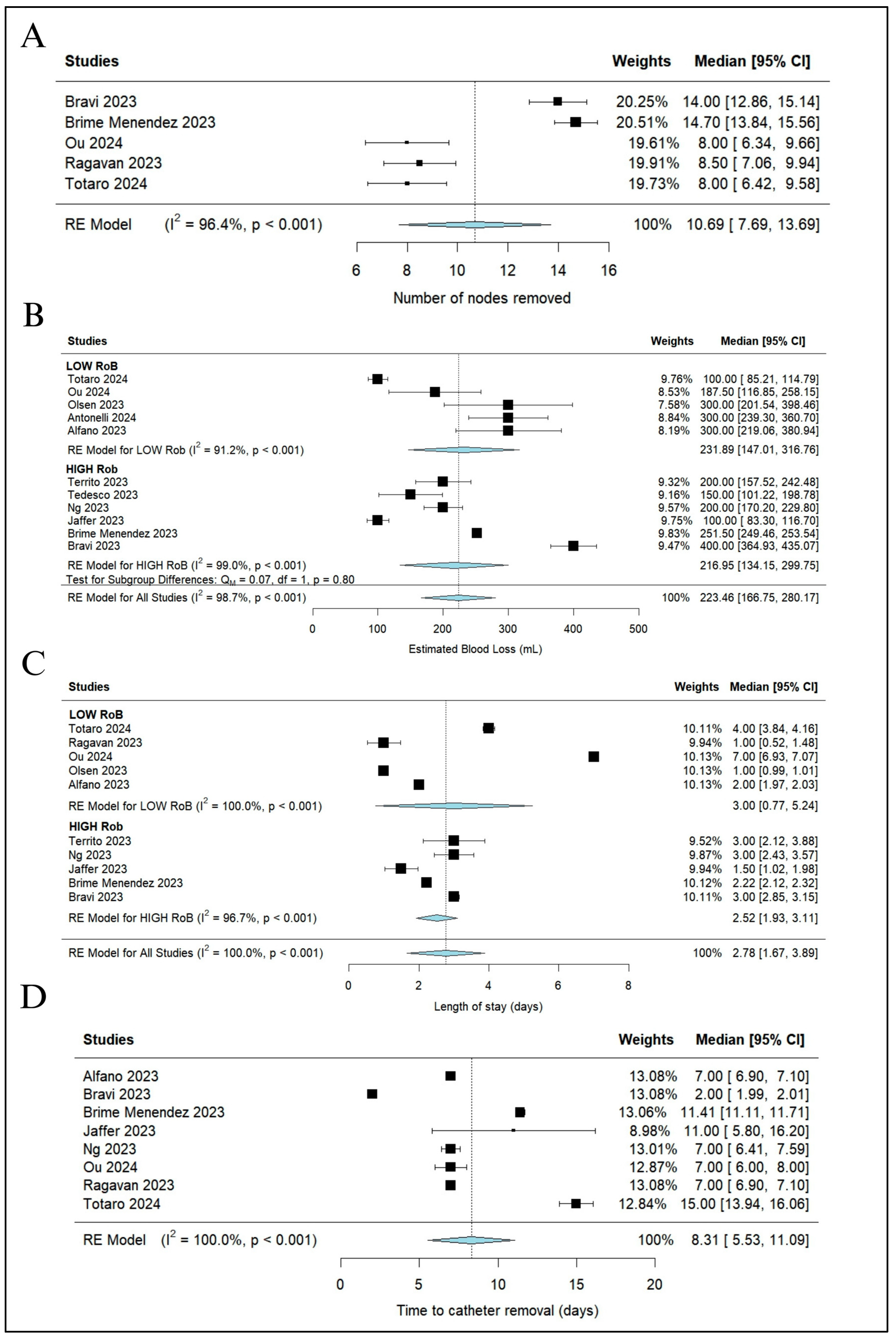
3.4. Surgical Outcomes
3.5. Oncological Outcomes
3.6. Functional Outcomes
3.7. Sensitivity Analysis
4. Discussion
4.1. Main Findings and Interpretation of the Results
4.2. Limitations
4.3. Implications for Practice and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Wang, J.; Hu, K.; Wang, Y.; Wu, Y.; Bao, E.; Wang, J.; Tan, C.; Tang, T. Robot-assisted versus open radical prostatectomy: A systematic review and meta-analysis of prospective studies. J. Robot. Surg. 2023, 17, 2617–2631. [Google Scholar] [CrossRef]
- Carbonara, U.; Srinath, M.; Crocerossa, F.; Ferro, M.; Cantiello, F.; Lucarelli, G.; Porpiglia, F.; Battaglia, M.; Ditonno, P.; Autorino, R. Robot-assisted radical prostatectomy versus standard laparoscopic radical prostatectomy: An evidence-based analysis of comparative outcomes. World J. Urol. 2021, 39, 3721–3732. [Google Scholar] [CrossRef] [PubMed]
- Alfano, C.G.; Moschovas, M.C.; Montagne, V.; Soto, I.; Porter, J.; Patel, V.; Ureña, R.; Bodden, E. Implementation and outcomes of Hugo(TM) RAS System in robotic-assisted radical prostatectomy. Int. Braz. J. Urol. 2023, 49, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Prata, F.; Ragusa, A.; Tempesta, C.; Iannuzzi, A.; Tedesco, F.; Cacciatore, L.; Raso, G.; Civitella, A.; Tuzzolo, P.; Callè, P.; et al. State of the Art in Robotic Surgery with Hugo RAS System: Feasibility, Safety and Clinical Applications. J. Pers. Med. 2023, 13, 1233. [Google Scholar] [CrossRef] [PubMed]
- Sheetz, K.H.; Claflin, J.; Dimick, J.B. Trends in the Adoption of Robotic Surgery for Common Surgical Procedures. JAMA Netw. Open 2020, 3, e1918911. [Google Scholar] [CrossRef] [PubMed]
- Knoll, T.; Omar, M.I.; Maclennan, S.; Hernández, V.; Canfield, S.; Yuan, Y.; Bruins, M.; Marconi, L.; Van Poppel, H.; N’Dow, J.; et al. EAU Guidelines Office Senior Associates Group Authorship. Key Steps in Conducting Systematic Reviews for Underpinning Clinical Practice Guidelines: Methodology of the European Association of Urology. Eur. Urol. 2018, 73, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int. J. Evid. Based Healthc. 2015, 13, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Centre for reviews and dissemination. Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Health Care. Available online: https://www.equator-network.org/reporting-guidelines/systematic-reviews-crds-guidance-for-undertaking-reviews-in-health-care/ (accessed on 12 November 2023).
- Sacco, E.; Marino, F.; Gandi, C.; Bientinesi, R.; Totaro, A.; Moretto, S.; Gavi, F.; Campetella, M.; Racioppi, M. Transalbugineal Artificial Urinary Sphincter: A Refined Implantation Technique to Improve Surgical Outcomes. J. Clin. Med. 2023, 12, 3021. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Syn. Meth 2020, 12, 55–61. [Google Scholar] [CrossRef]
- McGrath, S.; Sohn, H.; Steele, R.; Benedetti, A. Meta-analysis of the difference of medians. Biom. J. 2020, 62, 69–98. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Xu, C. Arcsine-based transformations for meta-analysis of proportions: Pros, cons, and alternatives. Health Sci. Rep. 2020, 3, e178. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Viechtbauer, W. Bias and efficiency of meta-analytic variance estimators in the random-effects model. J. Educ. Behav. Stat. 2005, 30, 261–293. [Google Scholar] [CrossRef]
- Assel, M.; Sjoberg, D.; Elders, A.; Wang, X.; Huo, D.; Botchway, A.; Delfino, K.; Fan, Y.; Zhao, Z.; Koyama, T.; et al. Guidelines for reporting of statistics for clinical research in urology. BJU Int. 2019, 123, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Tobías, A. Assessing the influence of a single study in the meta-anyalysis estimate. Stata Tech. Bull. 1999, 47, 15–17. [Google Scholar]
- Brime Menendez, R.; García Rojo, E.; Feltes Ochoa, J.A.; Justo Quintas, J.; Hevia Palacios, V.; Lista Mateos, F.; Crespo Martinez, L.; Belkahia, G.; Romero Otero, J. PE029—Preliminary comparative study between the Hugo-RAS system and the daVinci system for the performance of robotic radical prostatectomy. Eur. Urol. Op. Sci. 2023, 55, S69. [Google Scholar] [CrossRef]
- Tedesco, F.; Prata, F.; Ragusa, A.; Civitella, A.; Cacciatore, L.; Pira, M.; Iannuzzi, A.; Tuzzolo, P.; Raso, G.; D’Addurno, G. Safety and feasibility of three arms settings robot-assisted radical prostatectomy using the Hugo RAS system. Eur. Urol. Op. Sci. 2023, 55, S216. [Google Scholar] [CrossRef]
- Ng, C.F.; (Chinese University of Hong Kong, Hong Kong); Yee, C.H.; (Chinese University of Hong Kong, Hong Kong); Lai, F.; (Chinese University of Hong Kong, Hong Kong); Leung, S.; (Chinese University of Hong Kong, Hong Kong); Teoh, J.; (Chinese University of Hong Kong, Hong Kong); Chiu, P.; (Chinese University of Hong Kong, Hong Kong). Hugoc RAS Robotic Radical Prostatectomy—The Initial Experience and Learning Curve. 2023. Unpublished work.
- Jaffer, A.; Chia, D.; Ritualo, J.; Lee, N.; Vendivil, R.; Dasgupta, P.; Challacombe, B. PE095—HUGO RAS—UK’s first experience of integrating a new robotic platform into an existing high volume cancer centre. Eur. Urol. Op. Sci. 2023, 55, S149–S150. [Google Scholar] [CrossRef]
- Totaro, A.; Scarciglia, E.; Marino, F.; Campetella, M.; Gandi, C.; Ragonese, M.; Bientinesi, R.; Palermo, G.; Bizzarri, F.P.; Cretì, A.; et al. Robot Assisted Radical Prostatectomy Performed with the Novel Surgical Robotic Platform HUGOTM RAS: Monocentric First Series of 132 Cases Reporting Surgical, and Early Functional and Oncological Outcomes at a Tertiary Referral Robotic Center. Cancers 2024, 16, 1602. [Google Scholar] [CrossRef]
- Bravi, C.A.; Balestrazzi, E.; De Loof, M.; Rebuffo, S.; Piramide, F.; Mottaran, A.; Paciotti, M.; Sorce, G.; Nocera, L.; Sarchi, L.; et al. Robot-assisted Radical Prostatectomy Performed with Different Robotic Platforms: First Comparative Evidence between Da Vinci and HUGO Robot-assisted Surgery Robots. Eur. Urol. Focus. 2023, 10, 107–114. [Google Scholar] [CrossRef]
- Olsen, R.G.; Karas, V.; Bjerrum, F.; Konge, L.; Stroomberg, H.V.; Dagnæs-Hansen, J.A.; Røder, A. Skills transfer from the DaVinci® system to the Hugo™ RAS system. Int. Urol. Nephrol. 2024, 56, 389–397. [Google Scholar] [CrossRef]
- Ragavan, N.; Bharathkumar, S.; Chirravur, P.; Sankaran, S. Robot-Assisted Laparoscopic Radical Prostatectomy Utilizing Hugo RAS Platform: Initial Experience. J. Endourol. 2023, 37, 147–150. [Google Scholar] [CrossRef]
- Ou, H.C.; Marian, L.; Li, C.C.; Juan, Y.S.; Tung, M.C.; Shih, H.J.; Chang, C.P.; Chen, J.T.; Yang, C.H.; Ou, Y.C. Robot-Assisted Radical Prostatectomy by the Hugo Robotic-Assisted Surgery (RAS) System and the da Vinci System: A Comparison between the Two Platforms. Cancers 2024, 19, 1207. [Google Scholar] [CrossRef]
- Territo, A.; Uleri, A.; Gallioli, A.; Gaya, J.M.; Verri, P.; Basile, G.; Farré, A.; Bravo, A.; Tedde, A.; Faba, Ó.R.; et al. Robot-assisted oncologic pelvic surgery with Hugo™ robot-assisted surgery system: A single-center experience. Asian J. Urol. 2023, 10, 461–466. [Google Scholar] [CrossRef]
- Antonelli, A.; Veccia, A.; Malandra, S.; Rizzetto, R.; De Marco, V.; Baielli, A.; Franceschini, A.; Fumanelli, F.; Montanaro, F.; Palumbo, I. Intraoperative Performance of DaVinci Versus Hugo RAS During Radical Prostatectomy: Focus on Timing, Malfunctioning, Complications, and User Satisfaction in 100 Consecutive Cases (the COMPAR-P trial). Eur. Urol. Open Sci. 2024, 63, 104–112. [Google Scholar] [CrossRef]
- Bravi, C.A.; Paciotti, M.; Balestrazzi, E.; Piro, A.; Piramide, F.; Peraire, M.; Sarchi, L.; Mottaran, A.; Nocera, L.; De Backer, P.; et al. Outcomes of Robot-assisted Radical Prostatectomy with the Hugo RAS Surgical System: Initial Experience at a High-volume Robotic Center. Eur. Urol. Focus. 2023, 9, 642–644. [Google Scholar] [CrossRef]
- Totaro, A.; Campetella, M.; Bientinesi, R.; Gandi, C.; Palermo, G.; Russo, A.; Aceto, P.; Bassi, P.; Sacco, E. The new surgical robotic platform HUGOTM RAS: System description and docking settings for robot-assisted radical prostatectomy. Urologia 2022, 89, 603–609. [Google Scholar] [CrossRef]
- Ragavan, N.; Bharathkumar, S.; Chirravur, P.; Sankaran, S.; Mottrie, A. Evaluation of Hugo RAS System in Major Urologic Surgery: Our Initial Experience. J. Endourol. 2022, 36, 1029–1035. [Google Scholar] [CrossRef]
- Ou, Y.C.; Ou, H.C.; Juan, Y.S.; Ragavan, N.; Mottrie, A.; Weng, W.C.; Huang, L.H.; Lin, Y.S.; Hsu, C.Y.; Yang, H.; et al. Robot-assisted radical prostatectomy using hugo RAS system: The pioneer experience in Taiwan and Northeast Asia. Int. J. Med. Robot. 2024, 20, e2577. [Google Scholar] [CrossRef]
- Veccia, A.; Malandra, S.; Montanaro, F.; Pettenuzzo, G.; DE Marco, V.; Antonelli, A. Mirrored port placement for robotic radical prostatectomy with the Hugo RAS™ System: Initial experience. Minerva Urol. Nephrol. 2024, 25. [Google Scholar] [CrossRef]
- Biyani, C.S.; Pecanka, J.; Rouprêt, M.; Jensen, J.B.; Mitropoulos, D. Intraoperative adverse incident classification (EAUiaiC) by the European Association of Urology Ad Hoc Complications Guidelines Panel. Eur. Urol. 2020, 77, 601–610. [Google Scholar] [CrossRef]
- Novara, G.; Ficarra, V.; Rosen, R.C.; Artibani, W.; Costello, A.; Eastham, J.A.; Graefen, M.; Guazzoni, G.; Shariat, S.F.; Stolzenburg, J.U.; et al. Systematic review and meta-analysis of perioperative outcomes and complications after robot-assisted radical prostatectomy. Eur. Urol. 2012, 62, 431–452. [Google Scholar] [CrossRef]
- Bertolo, R.; Garisto, J.; Bove, P.; Mottrie, A.; Rocco, B.; EAU Robotic Urology Section (ERUS) Working Group on Science. Perioperative Outcomes Between Single-Port and “Multi-Port” Robotic Assisted Radical Prostatecomy: Where do we stand? Urology 2021, 155, 138–143. [Google Scholar] [CrossRef]
- Tewari, A.; Rao, S.; Martinez-Salamanca, J.I.; Leung, R.; Ramanathan, R.; Mandhani, A.; Vaughan, E.D.; Menon, M.; Horninger, W.; Tu, J.; et al. Cancer control and the preservation of neurovascular tissue: How to meet competing goals during robotic radical prostatectomy. BJU Int. 2008, 101, 1013–1018. [Google Scholar] [CrossRef]
- Novara, G.; Ficarra, V.; Mocellin, S.; Ahlering, T.E.; Carroll, P.R.; Graefen, M.; Guazzoni, G.; Menon, M.; Patel, V.R.; Shariat, S.F.; et al. Systematic review and meta-analysis of studies reporting oncologic outcome after robot-assisted radical prostatectomy. Eur. Urol. 2012, 62, 382–404. [Google Scholar] [CrossRef]
- Coelho, R.F.; Rocco, B.; Patel, M.B.; Orvieto, M.A.; Chauhan, S.; Ficarra, V.; Melegari, S.; Palmer, K.J.; Patel, V.R. Retropubic, laparoscopic, and robot-assisted radical prostatectomy: A critical review of outcomes reported by high-volume centers. J. Endourol. 2010, 24, 2003–2015. [Google Scholar] [CrossRef]
- Gandi, C.; Totaro, A.; Bientinesi, R.; Marino, F.; Pierconti, F.; Martini, M.; Russo, A.; Racioppi, M.; Bassi, P.; Sacco, E. A multi-surgeon learning curve analysis of overall and site-specific positive surgical margins after RARP and implications for training. J. Robot. Surg. 2022, 16, 1451–1461. [Google Scholar] [CrossRef]
- Ngu, J.C.; Lin, C.C.; Sia, C.J.; Teo, N.Z. A narrative review of the Medtronic Hugo RAS and technical comparison with the Intuitive da Vinci robotic surgical system. J. Robot. Surg. 2024, 18, 99. [Google Scholar] [CrossRef]
- Atife, M.; Okondo, E.; Jaffer, A.; Noel, J.; Dasgupta, P.; Challacombe, B. Intuitive’s da Vinci vs Medtronic’s Hugo: Real life observations from a robot naïve perspective. J. Robot. Surg. 2024, 18, 4. [Google Scholar] [CrossRef]
- Available online: https://www.medtronic.com/covidien/en-gb/robotic-assisted-surgery/hugo-ras-system/products-and-system.html (accessed on 10 April 2024).
- Available online: https://www.intuitive.com/en-gb/products-and-services/da-vinci (accessed on 10 April 2024).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Country | Type of Study | Number of Patients N | Age (Years) Median (Q1–Q3) | BMI (kg/m2) Median (Q1–Q3) | Preoperative PSA Level (ng/mL) Median (Q1–Q3) | Prostate Volume (cc) Median (Q1–Q3) | Clinical T Stage Unpalpable (cT1) N (%) | Clinical T Stage Palpable (cT2–T4) N (%) | ISUP 1–2 at Biopsy N (%) | ISUP 3–5 at Biopsy N (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Alfano et al., 2023 [3] | Panama | R | 15 | 62 (59–67) | 24.9 (23–28) | 7.3 (4.8–8.1) | 52 (41–56) | 8 (53) | 7 (47) | 13 (87) | 2 (13) |
| Antonelli et al. 2024 [28] | Italy | P | 50 | 65.9 ± 5.9 mean ± SD | 25.4 (24.5–27.8) | 7.7 (5.9–11) | 40 (29–50) (on 44 patients) | NR | NR | 27 (54) | 23 (46) |
| Bravi et al., 2023 [23] | Belgium | R | 164 | 65 (60–70) | 26 (24–29) | 8 (5.7–11.1) | 42 (33–58) | 109 (66) | 55 (34) | 111 (67) | 53 (33) |
| Brime Menendez et al., 2023 [18] | Spain | P (RCT) | 75 | 65.8 ± 8.1 mean ± SD | 26.2 ± 4 mean ± SD | 6.4 ± 1.9 mean ± SD | 41.7 ± 16.3 mean ± SD | 51 (68) | 24 (32) | 49 (65.4) | 26 (34.6) |
| Jaffer et al., 2023 [21] | England | R | 20 | 61 (50–72) median (range min-max) | 25.7 (22.1–34) median (range min-max) | 7.9 (3.8–43) median (range min-max) | NR | NR | NR | NR | NR |
| Ng et al., 2023 [20] | Hong Kong | R | 10 | 68 (67–71) | NR | 9.4 (7.4–12.3) | 43 (34–45) | NR | NR | NR | NR |
| Olsen et al., 2023 [24] | Denmark | R | 19 | 66 (63–73) | 25.5 (23.7–27.5) | NR | 47 (30–75) | 10 (52.6) | 9 (47.4) | NR | NR |
| Ou et al., 2024 [26] | Taiwan | R | 30 | 66.5 (10) median (IQR) | 25.79 (4.26) median (IQR) | 8.81 (7.66) median (IQR) | 40 (16.5) median (IQR) | 0 (0) | 30 (100) | 23 (76.6) | 7 (23.3) |
| Ragavan et al., 2023 [25] | India | P | 17 | 68 (66–72) | 24.6 (22.6–26.6) | 12.4 (8.8–27) | NR | 0 (0) | 17 (100) | NR | NR |
| Tedesco et al., 2023 [19] | Italy | R | 30 | NR | NR | NR | NR | NR | NR | NR | NR |
| Territo et al., 2023 [27] | Spain | R | 17 | 64 (59–69) | 27 (24–27) | 6.4 (5.1–9.4) | 35 (30–56) | 10 (58.8) | 7 (41.2) | NR | NR |
| Totaro et al., 2024 [22] | Italy | P | 132 | 66.5 (62–71.5) | 26 (24.4–28) | 8 (5.5–11.3) | 46 (33–62) | 105 (79.6) | 27 (20.4) | 91 (68.9) | 41 (31.1) |
| Author, Year | Docking Time (Min) Median (Q1-Q3) | Console Time (min) Median (Q1–Q3) | Operative Time (min) Median (Q1–Q3) | EBL (mL) Median (Q1–Q3) | Nerve-Sparing Surgery (n; %) | Lymphadenectomy (n; %) | Number of Lymph Nodes Removed Median (Q1–Q3) | LOS (Days) Median (Q1–Q3) | Catheter Removal (Days) Median (Q1–Q3) |
|---|---|---|---|---|---|---|---|---|---|
| Alfano et al., 2023 [3] | 7 (15) median (max) | NR | 235 (213–271) | 300 (100–310) | NR | 5 (33) | NR | 2 (2–2) | 7 (7–7) |
| Antonelli et al. 2024 [28] | 11 (8–14) | NR | NR | 300 (150–400) | NR | NR | NR | NR | NR |
| Bravi et al., 2023 [23] | NR | 150 (110–175 on 112 patients) | 180 (150–200) | 400 (250–500) | 147 (90) | 41 (25) | 14 (10–18) | 3 (3–4) | 2 (2–2) |
| Brime Menendez et al., 2023 [18] | 18.6 ± 8 mean ± SD | NR | 138.9 ± 45.5 mean ± SD | 251.5 ± 9 mean ± SD | 61 (81.3) | 22 (29.3) | 14.7 ± 3.8 mean ± SD | 2.22 ± 0.42 mean ± SD | 11.41 ± 1.34 mean ± SD |
| Jaffer et al., 2023 [21] | 5 (4–8) median (range min-max) | 130 (90–150) median (Range min-max) | NR | 100 (50–500) median (range min-max) | NR | NR | NR | 1.5 (1–4) median (range min-max) | 11 (10–43) median (range min-max) |
| Ng et al., 2023 [20] | NR | NR | 182 (171–217) | 200 (200–500) | NR | NR | NR | 3 (2–3) | 7 (7–8) |
| Olsen et al., 2023 [24] | 8 (6–11) | 97 (87–120) | NR | 300 (150–400) | 11 (57.9) | 10 (52.6) | NR | 1 (1–1) | NR |
| Ou et al., 2024 [26] | 23.5 (22–30.5) (on 12 patients) | 146.5 (36.5) median (IQR) | NR | 187.5 (242.5) median (IQR) | NR | NR | 8 (5) median (IQR) | 7 (0) median (IQR) | 7 (3) median (IQR) |
| Ragavan et al., 2023 [25] | 10 (5–10) median (range min–max) | 170 (160–205) | 195 (180–240) | NR | 0 (0) | 17 (100) | 8.5 (6.75–10) | 1 (1–2) | 7 (7–7) |
| Tedesco et al., 2023 [19] | 9 (7–12) | NR | 120 (100–150) | 150 (100–250) | NR | NR | NR | NR | NR |
| Territo et al., 2023 [27] | 12 (7–16) | 185 (177–192) | NR | 200 (150–250) | NR | NR | NR | 3 (2–4) | NR |
| Totaro et al., 2024 [22] | 10 (8–12) | 117 (96–175) | 189 (146–227) | 100 (50–150) | 33 (25.2) | 25 (18.9) | 8 (4.5–15) | 4 (4–5) | 15 (14–20.5) |
| Author, Year | Positive Surgical Margins N (%) | Postoperative PSA Levels at 1 Month (ng/mL) Median (Q1–Q3) | Postoperative PSA at 3 Months (ng/mL) Median (Q1–Q3) | Undetectable PSA at 1 Month N (%) | Undetectable PSA at 3 Months N (%) | Social Continence Rate at 1 Month N (%) | Social Continence at 3 Months N (%) | Postoperative Complications (Clavien–Dindo ≥ 2) N (%) | Postoperative Erections N (%) (Follow-Up) |
|---|---|---|---|---|---|---|---|---|---|
| Alfano et al., 2023 [3] | 5 (33) | 0 (0–0) | NR | 15 (100) | NR | 9 (61) | NR | 1 (6.7) | NR |
| Antonelli et al., 2024 [28] | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Bravi et al., 2023 [23,29] | 20 (12) | NR | NR | 60 (88%) | NR | 108 (66) | 133 (81) | 10 (6) | NR |
| Brime Menendez et al., 2023 [18] | 15 (20) | 0.34 (0.83) median (IQR) | 0.07 (0.21) median (IQR) | NR | NR | NR | 66 (88) | 1 (1.3) | NR |
| Jaffer et al., 2023 [21] | 0 (0) | NR | NR | NR | NR | NR | NR | 6 (30) | NR |
| Ng et al., 2023 [20] | NR | NR | NR | NR | NR | NR | 8 (80) | 1 (10) | NR |
| Olsen et al., 2023 [24] | 7 (36.8) | NR | 0 (0–0.45) | NR | NR | NR | 11 (57.9) | 2 (10.5) | 5 (26.3) (3 months) |
| Ou et al., 2024 [26] | 6 (20) | NR | NR | NR | NR | 8 (26.7) | 23 (76.6) | 0 (0) | 22 (73.3) (3 months) |
| Ragavan et al., 2023 [25] | 4 (23.5) | NR | 0.07 Median | NR | NR | NR | 17 (100) | 0 (0) | 0 (0) (3 months) |
| Tedesco et al., 2023 [19] | NR | NR | NR | NR | NR | NR | NR | 0 (0) | NR |
| Territo et al., 2023 [27] | 5 (29.4) | NR | 0.009 (0.006–0.045) | NR | NR | NR | NR | 3 (17.7) | NR |
| Totaro et al., 2024 [22] | 37 (28) | NR | NR | NR | 125 (94.6%) | NR | 100 (75.7%) | 3 (4) | 25 (31) (6 months) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marino, F.; Moretto, S.; Rossi, F.; Gandi, C.; Gavi, F.; Bientinesi, R.; Campetella, M.; Russo, P.; Bizzarri, F.P.; Scarciglia, E.; et al. Robot-Assisted Radical Prostatectomy Performed with the Novel Hugo™ RAS System: A Systematic Review and Pooled Analysis of Surgical, Oncological, and Functional Outcomes. J. Clin. Med. 2024, 13, 2551. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092551
Marino F, Moretto S, Rossi F, Gandi C, Gavi F, Bientinesi R, Campetella M, Russo P, Bizzarri FP, Scarciglia E, et al. Robot-Assisted Radical Prostatectomy Performed with the Novel Hugo™ RAS System: A Systematic Review and Pooled Analysis of Surgical, Oncological, and Functional Outcomes. Journal of Clinical Medicine. 2024; 13(9):2551. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092551
Chicago/Turabian StyleMarino, Filippo, Stefano Moretto, Francesco Rossi, Carlo Gandi, Filippo Gavi, Riccardo Bientinesi, Marco Campetella, Pierluigi Russo, Francesco Pio Bizzarri, Eros Scarciglia, and et al. 2024. "Robot-Assisted Radical Prostatectomy Performed with the Novel Hugo™ RAS System: A Systematic Review and Pooled Analysis of Surgical, Oncological, and Functional Outcomes" Journal of Clinical Medicine 13, no. 9: 2551. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092551