
Continual Monitoring of Respiratory Disorders to Enhance Therapy via Real-Time Lung Sound Imaging in Telemedicine


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Literature Review
3. Monitoring System for Remote Assessment
3.1. Hardware Design
3.1.1. Microphone Array
3.1.2. Microcontroller and BLE
3.1.3. Data Acquisition System Design
3.2. Software Design
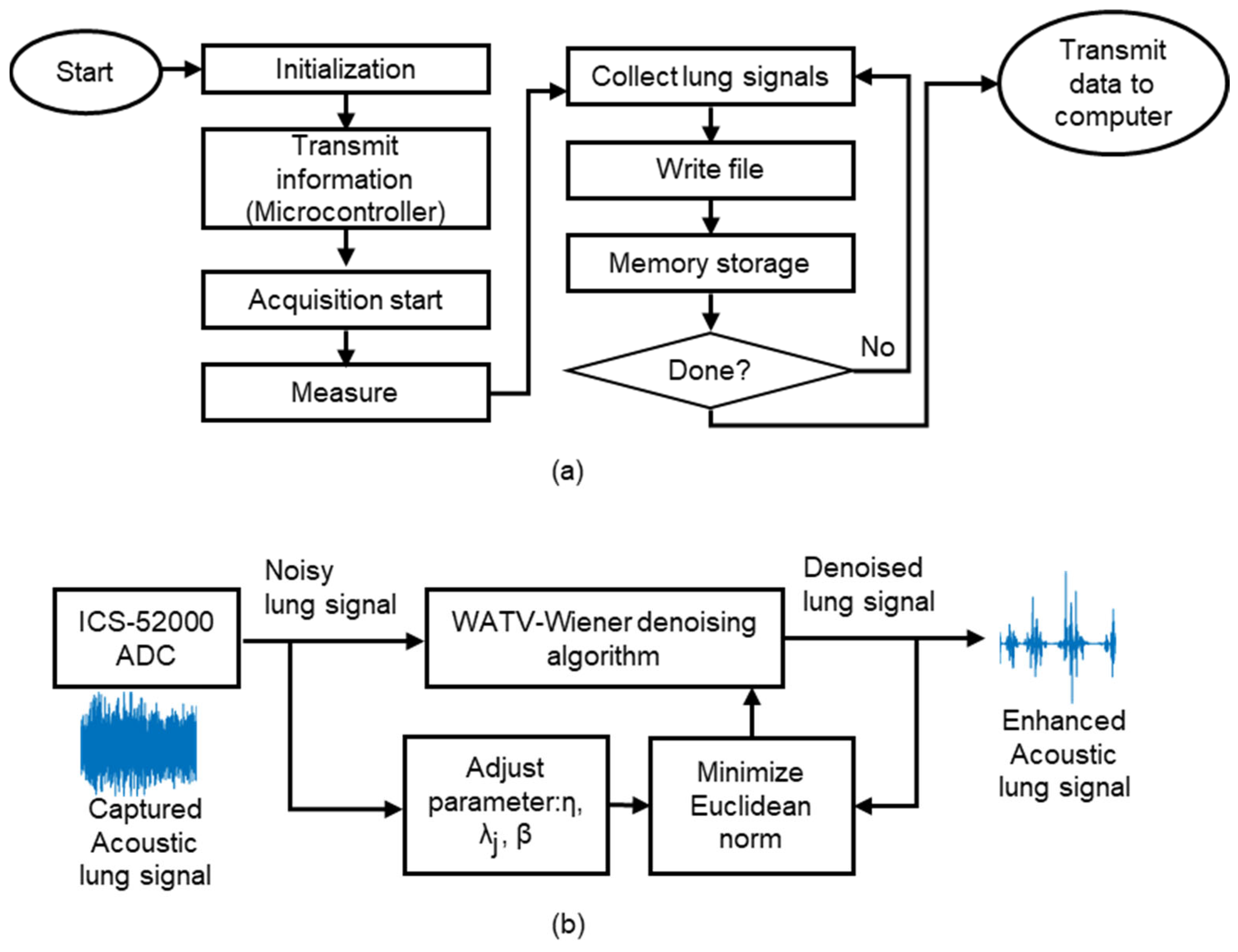
3.2.1. Data Acquisition Software Design
3.2.2. Signal Processing Denoising Module
| Algorithm 1. WATV-Wiener denoising algorithm [38] |
| Input: Noisy data (y); Number of vanishing moment (km); Regularization parameter (); TV parts (); Step size (); Number of wavelet scale (); Number of iterations (); Threshold function (); Wavelet transform (W); Wavelet coefficient (ωc) Output: 1: Initialization: ; 2: Identifying an estimated wavelet coefficient by iteratively minimizing with respect to ωc and with variable splitting and augmented Lagrangian approach. 3: ; 4: Iteration till convergence between and . 5: For = 1: 6: 7: Finding the wavelet coefficient for all with the input from , , , , 8: 9: 10: Total variation denoising () requires data input from , length of the data in put () and TV parts 11: 12: 13: 14: end For 15: Denoised wavelet coefficient (), where the signal 16: Empirical Wiener filter design for smoothing: 17: 18: Smooth denoised output: |
3.2.3. Image Processing
4. System Evaluation and Comparative Analysis
4.1. Acoustic Signals Acquisition and Setup
4.1.1. Acoustic Signals Acquisition
- Recordings collected from the posterior chest were chosen as the region of interest.
- Samples were separated into healthy and unhealthy groups based on annotated labels.
- Unhealthy sounds lacking clinician labels for crackles/wheezing were excluded. Similarly, healthy sounds with annotated anomalies were omitted.
4.1.2. Acoustic Imaging Generation
4.2. Signal Acquisition and Identification of Nidi Performance Index
4.2.1. Signal Acquisition Performance Index
4.2.2. Acoustic Imaging Performance Index
5. Results and Discussion
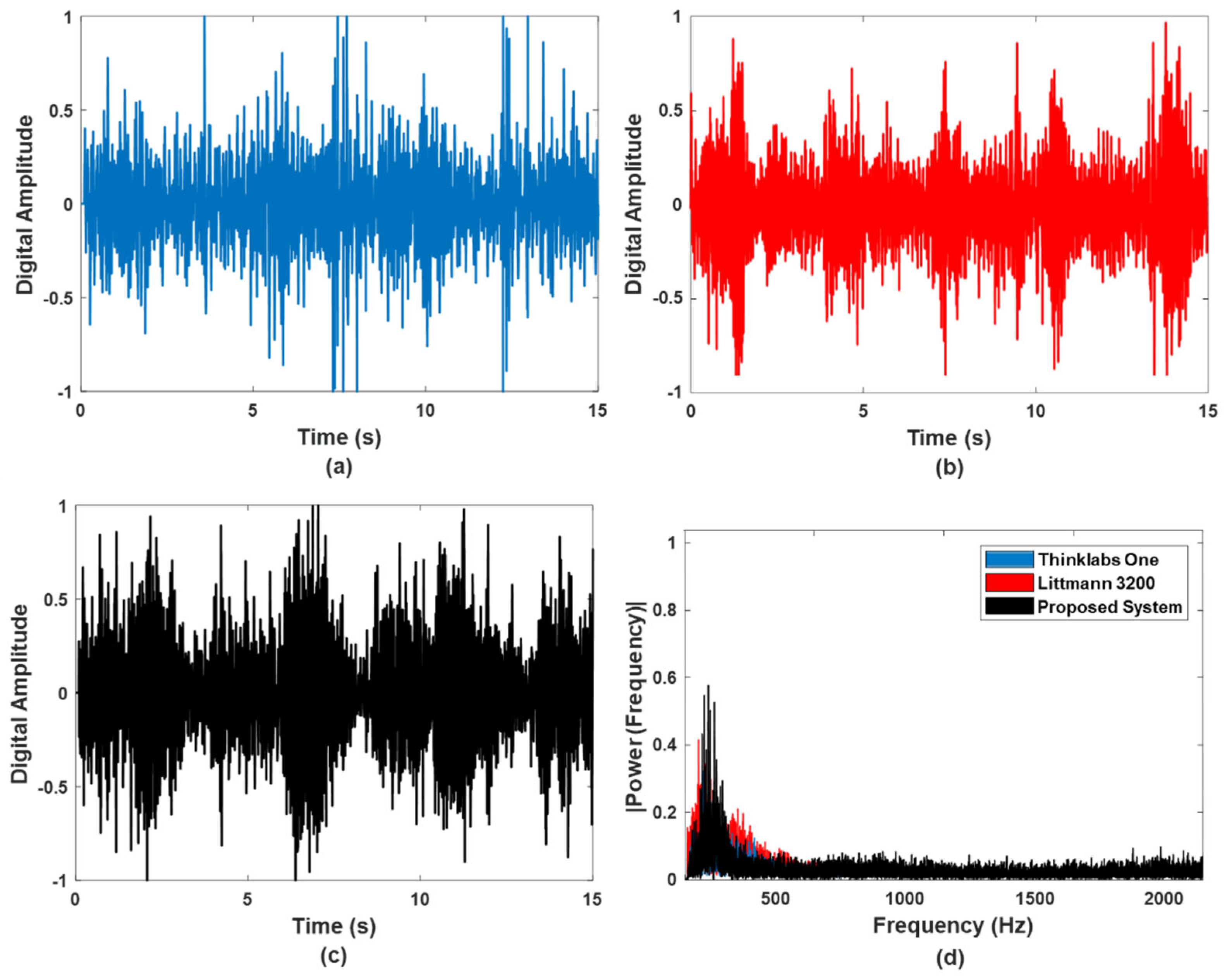
5.1. Signal Accuracy and Noise Robustness
5.2. Acoustic Imaging
5.3. General Discussion and Limitations
6. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, D.Y.; Ghoshal, A.G.; Muttalif, A.R.B.A.; Lin, H.-C.; Thanaviratananich, S.; Bagga, S.; Faruqi, R.; Sajjan, S.; Brnabic, A.J.; Dehle, F.C.; et al. Quality of life and economic burden of respiratory disease in Asia-Pacific burden of respiratory diseases study. Value Heal. Reg. Issues 2016, 9, 72–77. [Google Scholar] [CrossRef]
- Bahadori, K.; Doyle-Waters, M.M.; Marra, C.; Lynd, L.; Alasaly, K.; Swiston, J.; FitzGerald, J.M. Economic burden of asthma: A systematic review. BMC Pulm. Med. 2009, 9, 24. [Google Scholar] [CrossRef] [PubMed]
- McIlwaine, M.; Bradley, J.; Elborn, J.S.; Moran, F. Personalising airway clearance in chronic lung disease. Eur. Respir. Rev. 2017, 26, 160086. [Google Scholar] [CrossRef]
- Franssen, F.M.; Alter, P.; Bar, N.; Benedikter, B.J.; Iurato, S.; Maier, D.; Maxheim, M.; Roessler, F.K.; Spruit, M.A.; Vogelmeier, C.F.; et al. Personalized medicine for patients with COPD: Where are we? Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 1465–1484. [Google Scholar] [CrossRef] [PubMed]
- Ohashi, C.; Akiguchi, S.; Ohira, M. Development of a remote health monitoring system to prevent frailty in elderly home-care patients with COPD. Sensors 2022, 22, 2670. [Google Scholar] [CrossRef] [PubMed]
- Janjua, S.; Carter, D.; Threapleton, C.J.; Prigmore, S.; Disler, R.T. Telehealth interventions: Remote monitoring and consultations for people with chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2021, 7, CD013196. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.; Huynh, E.; Royston, T.J.; Kornblith, A.; Roy, S. Acoustic methods for pulmonary diagnosis. IEEE Rev. Biomed. Eng. 2018, 12, 221–239. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-S.; Li, M.; Lou, Y.; Abbasi, Q.H.; Imran, M.A. Acoustic lung imaging utilized in continual assessment of patients with obstructed airway: A systematic review. Sensors 2023, 23, 6222. [Google Scholar] [CrossRef] [PubMed]
- Ward, J.J.; Wattier, B.A. Technology for enhancing chest auscultation in clinical simulation. Respir. Care 2011, 56, 834–845. [Google Scholar] [CrossRef]
- 3M Littmann Electronic Stethoscope Model 3200. Available online: https://multimedia.3m.com/mws/media/594115O/3m-littmann-electronic-stethoscope-model-3200-user-manual.pdf (accessed on 23 November 2023).
- ThinklabsOne. Available online: https://www.thinklabs.com/ (accessed on 23 November 2023).
- Lee, C.S.; Lou, Y.; Li, M.; Abbasi, Q.H.; Imran, M.A. Locating nidi for high-frequency chest wall oscillation smart therapy via acoustic imaging of lung airways as a spatial network. IEEE Access 2023, 11, 109408–109421. [Google Scholar] [CrossRef]
- Lee, C.S.; Li, M.; Lou, Y.; Dahiya, R. Modeling and simulation of pulmonary acoustic signal and imaging for lung function assessment. In Proceedings of the 2023 IEEE International Conference on Consumer Electronics (ICCE), Las Vegas, NV, USA, 6–8 January 2023; pp. 1–6. [Google Scholar]
- Lee, C.S.; Li, M.; Lou, Y.; Dahiya, R. The Effect of sensor array design on acoustic imaging for enhancing HFCWO therapy. In Proceedings of the 2023 20th International Multi-Conference on Systems, Signals & Devices (SSD), Mahdia, Tunisia, 20–23 February 2023; pp. 887–892. [Google Scholar]
- Szem, J.W.; Hydo, L.J.; Fischer, E.; Kapur, S.; Klemperer, J.; Barie, P.S. High-risk intrahospital transport of critically ill patients: Safety and outcome of the necessary “road trip”. Crit. Care Med. 1995, 23, 1660–1666. [Google Scholar] [CrossRef] [PubMed]
- Beckmann, U.; Gillies, D.M.; Berenholtz, S.M.; Wu, A.W.; Pronovost, P. Incidents relating to the intra-hospital transfer of critically ill patients. Intensiv. Care Med. 2004, 30, 1579–1585. [Google Scholar] [CrossRef] [PubMed]
- De Alwis, C.; Pham, Q.-V.; Liyanage, M. 6G for healthcare. In 6G Frontiers: Towards Future Wireless Systems; Wiley-IEEE Press: Hoboken, NJ, USA, 2023; pp. 189–196. [Google Scholar]
- William, M.; Sharif, S.; Ejaz, W. Enabling communication and networking technologies for 6G in healthcare sector. In Proceedings of the 2023 Second International Conference on Smart Technologies for Smart Nation (SmartTechCon), Singapore, 18–19 August 2023; pp. 699–704. [Google Scholar]
- McLane, I.; Emmanouilidou, D.; West, J.E.; Elhilali, M. Design and comparative performance of a robust lung auscultation system for noisy clinical settings. IEEE J. Biomed. Heal Inform. 2021, 25, 2583–2594. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.S.; Li, M.; Lou, Y.; Dahiya, R. Design of a robust lung sound acquisition system for reliable acoustic lung imaging. In Proceedings of the 2023 IEEE International Ultrasonics Symposium (IUS), Montreal, QC, Canada, 3–8 September 2023; pp. 1–4. [Google Scholar]
- Liu, H.; Barekatain, M.; Roy, A.; Liu, S.; Cao, Y.; Tang, Y.; Shkel, A.; Kim, E.S. MEMS piezoelectric resonant microphone array for lung sound classification. J. Micromech. Microeng. 2023, 33, 044003. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Moghimi, M.J.; Jeong, Y.; Gupta, D.; Inan, O.T.; Ayazi, F. Precision wearable accelerometer contact microphones for longitudinal monitoring of mechano-acoustic cardiopulmonary signals. npj Digit. Med. 2020, 3, 19. [Google Scholar] [CrossRef]
- Duanmu, Z.; Kong, C.; Guo, Y.; Zhang, X.; Liu, H.; Zhao, C.; Gong, X.; Cai, C.; Ho, C.; Wan, C. Design and implementation of an acoustic-vibration capacitive MEMS microphone. AIP Adv. 2022, 12, 065309. [Google Scholar] [CrossRef]
- Shah, M.A.; Shah, I.A.; Lee, D.-G.; Hur, S. Design approaches of MEMS microphones for enhanced performance. J. Sens. 2019, 2019, 9294528. [Google Scholar] [CrossRef]
- Zawawi, S.A.; Hamzah, A.A.; Majlis, B.Y.; Mohd-Yasin, F. A review of MEMS capacitive microphones. Micromachines 2020, 11, 484. [Google Scholar] [CrossRef]
- Charleston-Villalobos, S.; Cortés-Rubiano, S.; González-Camerena, R.; Chi-Lem, G.; Aljama-Corrales, T. Respiratory acoustic thoracic imaging (RATHI): Assessing deterministic interpolation techniques. Med. Biol. Eng. Comput. 2004, 42, 618–626. [Google Scholar] [CrossRef]
- Charleston-Villalobos, S.; Gonzalez-Camarena, R.; Chi-Lem, G.; Aljama-Corrales, T. Acoustic thoracic images for transmitted glottal sounds. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; pp. 3481–3484. [Google Scholar]
- Kompis, M.; Pasterkamp, H.; Wodicka, G.R. Acoustic imaging of the human chest. Chest 2001, 120, 1309–1321. [Google Scholar] [CrossRef] [PubMed]
- Lev, S.; Glickman, Y.A.; Kagan, I.; Shapiro, M.; Moreh-Rahav, O.; Dahan, D.; Cohen, J.; Grinev, M.; Singer, P. Computerized lung acoustic monitoring can help to differentiate between various chest radiographic densities in critically ill patients. Respiration 2010, 80, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Manwar, R.; Zafar, M.; Xu, Q. Signal and image processing in biomedical photoacoustic imaging: A review. Optics 2020, 2, 1–24. [Google Scholar] [CrossRef]
- Dellinger, R.P.; Parrillo, J.E.; Kushnir, A.; Rossi, M.; Kushnir, I. Dynamic Visualization of lung sounds with a vibration response device: A case series. Respiration 2007, 75, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Shi, C.; Boehme, S.; Bentley, A.H.; Hartmann, E.K.; Klein, K.U.; Bodenstein, M.; Baumgardner, J.E.; David, M.; Ullrich, R.; Markstaller, K. Assessment of regional ventilation distribution: Comparison of vibration response imaging (VRI) with electrical impedance tomography (EIT). PLoS ONE 2014, 9, e86638. [Google Scholar] [CrossRef] [PubMed]
- Yigla, M.; Gat, M.; Meyer, J.-J.; Friedman, P.J.; Maher, T.M.; Madison, J.M. Vibration response imaging technology in healthy subjects. Am. J. Roentgenol. 2008, 191, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.S.; Li, M.; Lou, Y.; Abbasi, Q.H.; Imran, M. An acoustic system of sound acquisition and image generation for frequent and reliable lung function assessment. IEEE Sens. J. 2023, 24, 3731–3747. [Google Scholar] [CrossRef]
- C. TDK Group. ICS-52000. Available online: https://invensense.tdk.com/products/ics-52000/ (accessed on 23 November 2023).
- Gregtomasch. Bluetooth Low Energy (BLE) Connectivity for Teensy 3.X Boards. Available online: https://github.com/gregtomasch/Tlera_nRF52_MCU_Add_On_Board/tree/master/ble_app_uart_c_Add_on (accessed on 22 November 2023).
- NORDIC. Versatile Bluetooth 5.4 SoC supporting Bluetooth Low Energy, Bluetooth Mesh and NFC. Available online: https://infocenter.nordicsemi.com/index.jsp (accessed on 22 November 2023).
- Lee, C.S.; Li, M.; Lou, Y.; Dahiya, R. Restoration of lung sound signals using a hybrid wavelet-based approach. IEEE Sens. J. 2022, 22, 19700–19712. [Google Scholar] [CrossRef]
- Ding, Y.; Selesnick, I.W. Artifact-free wavelet denoising: Non-convex sparse regularization, convex optimization. IEEE Signal Process. Lett. 2015, 22, 1364–1368. [Google Scholar] [CrossRef]
- Meng, F.; Wang, Y.; Shi, Y.; Zhao, H. A kind of integrated serial algorithms for noise reduction and characteristics expanding in respiratory sound. Int. J. Biol. Sci. 2019, 15, 1921–1932. [Google Scholar] [CrossRef] [PubMed]
- Ulukaya, S.; Serbes, G.; Kahya, Y.P. Performance comparison of wavelet based denoising methods on discontinuous adventitious lung sounds. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju Island, Republic of Korea, 11–15 July 2017; pp. 2928–2931. [Google Scholar]
- Rocha, B.M.; Filos, D.; Mendes, L.; Serbes, G.; Ulukaya, S.; Kahya, Y.P.; Jakovljevic, N.; Turukalo, T.L.; Vogiatzis, I.M.; Perantoni, E.; et al. An open access database for the evaluation of respiratory sound classification algorithms. Physiol. Meas. 2019, 40, 035001. [Google Scholar] [CrossRef] [PubMed]
- Kraman, S.S. Transmission of lung sounds through light clothing. Respiration 2007, 75, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Wen, H.; Di Francesco, L.; Ayazi, F. Detection of pathological mechano-acoustic signatures using precision accelerometer contact microphones in patients with pulmonary disorders. Sci. Rep. 2021, 11, 13427. [Google Scholar] [CrossRef] [PubMed]
- Frequency Response Graph (Bose S1 Pro System). Available online: https://www.rtings.com/speaker/0-8/graph#6982/4559 (accessed on 22 November 2023).
- Darbyshire, J.L.; Müller-Trapet, M.; Cheer, J.; Fazi, F.M.; Young, J.D. Mapping sources of noise in an intensive care unit. Anaesthesia 2019, 74, 1018–1025. [Google Scholar] [CrossRef] [PubMed]
- British Broadcasting. Corporation. (BBC). Sound Effects. Available online: https://sound-effects.bbcrewind.co.uk/search?q=Intensive%20care%20unit (accessed on 22 November 2023).
- The Audio Filter in Your One. Available online: http://thinklabsone.com/downloads/Stethoscope_Filters.pdf (accessed on 22 November 2023).
- Salehin, S.A.; Abhayapala, T.D. Lung sound localization using array of acoustic sensors. In Proceedings of the 2008 2nd International Conference on Signal Processing and Communication Systems (ICSPCS 2008), Gold Coast, Australia, 15–17 December 2008; pp. 1–5. [Google Scholar]
- Messner, E.; Hagmüller, M.; Swatek, P.; Pernkopf, F. A Robust multichannel lung sound recording device. In Proceedings of the 9th International Conference on Biomedical Electronics and Devices, Rome, Italy, 21 February 2016; pp. 34–39. [Google Scholar]
- Skalicky, D.; Koucky, V.; Hadraba, D.; Viteznik, M.; Dub, M.; Lopot, F. Detection of respiratory phases in a breath sound and their subsequent utilization in a diagnosis. Appl. Sci. 2021, 11, 6535. [Google Scholar] [CrossRef]
- Bing, D.; Jian, K.; Long-Feng, S.; Wei, T.; Hong-Wen, Z. Vibration response imaging: A novel noninvasive tool for evaluating the initial therapeutic effect of noninvasive positive pressure ventilation in patients with acute exacerbation of chronic obstructive pulmonary disease. Respir. Res. 2012, 13, 65. [Google Scholar] [CrossRef] [PubMed]
- Bradley, D.; Roth, G. Adaptive thresholding using the integral image. J. Graph. Tools 2007, 12, 13–21. [Google Scholar] [CrossRef]
- Dellinger, R.P.; Jean, S.; Cinel, I.; Tay, C.; Rajanala, S.; Glickman, Y.A.; Parrillo, J.E. Regional distribution of acoustic-based lung vibration as a function of mechanical ventilation mode. Crit. Care 2007, 11, R26. [Google Scholar] [CrossRef] [PubMed]












Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muhammad, M.; Li, M.; Lou, Y.; Lee, C.-S. Continual Monitoring of Respiratory Disorders to Enhance Therapy via Real-Time Lung Sound Imaging in Telemedicine. Electronics 2024, 13, 1669. https://0-doi-org.brum.beds.ac.uk/10.3390/electronics13091669
Muhammad M, Li M, Lou Y, Lee C-S. Continual Monitoring of Respiratory Disorders to Enhance Therapy via Real-Time Lung Sound Imaging in Telemedicine. Electronics. 2024; 13(9):1669. https://0-doi-org.brum.beds.ac.uk/10.3390/electronics13091669
Chicago/Turabian StyleMuhammad, Murdifi, Minghui Li, Yaolong Lou, and Chang-Sheng Lee. 2024. "Continual Monitoring of Respiratory Disorders to Enhance Therapy via Real-Time Lung Sound Imaging in Telemedicine" Electronics 13, no. 9: 1669. https://0-doi-org.brum.beds.ac.uk/10.3390/electronics13091669