

Numerical Analysis of the Plantar Pressure Points during the Stance Phases for the Design of a 3D-Printable Patient-Specific Insole
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Biomodel Construction
2.2. Gait Experimental Baropodometric Testing
2.3. Finite Element Analyses Simulating the Stance Phases of the Gait Cycle
2.3.1. First Case Study
2.3.2. Second Case Study
3. Results
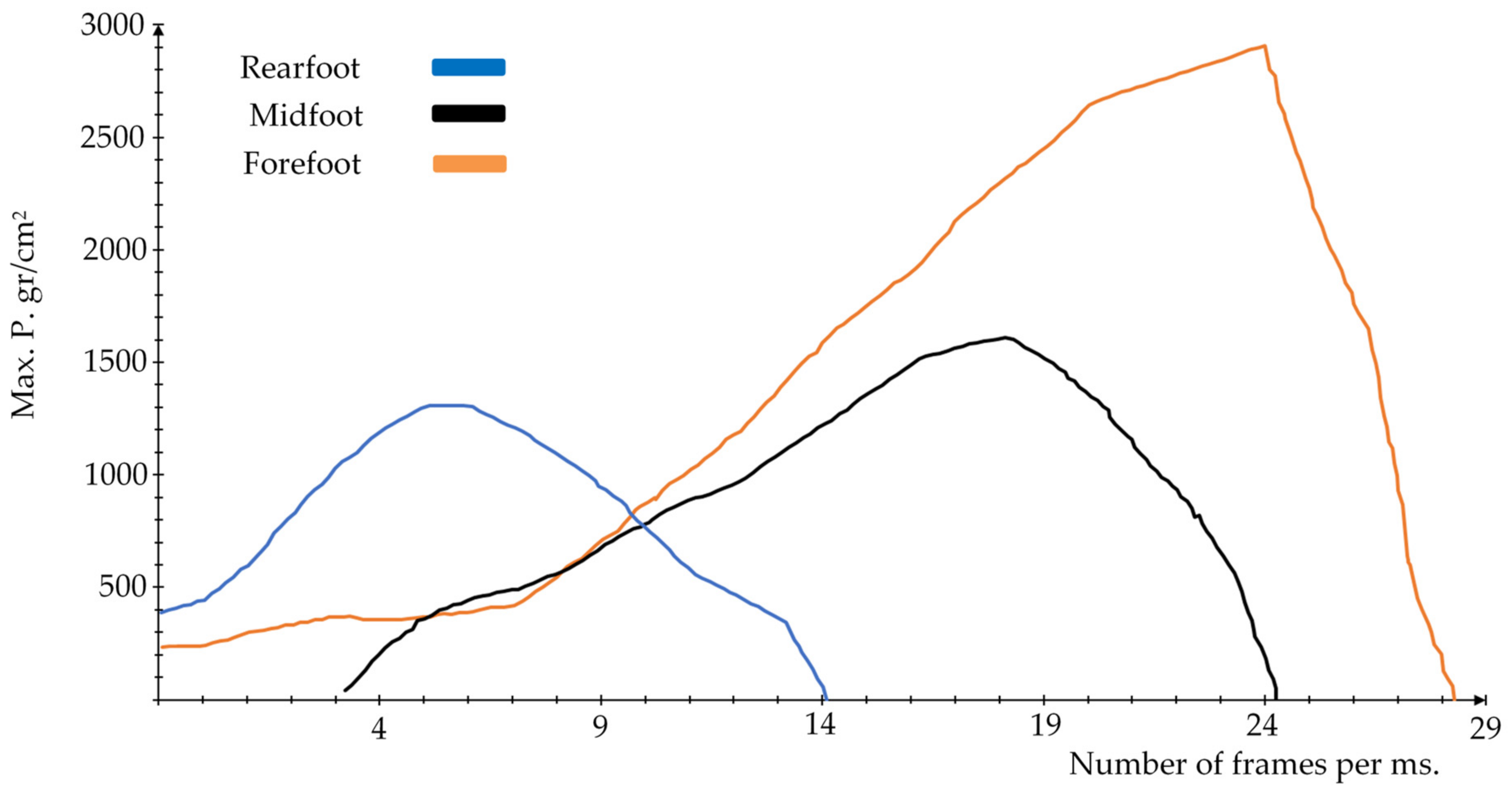
3.1. Results Gait Experimental Baropodometric Testing
3.2. Results of the First Case Study of Finite Element Analyses Simulating the Stance Phases of the Gait Cycle
3.3. Validation and Comparison to First Case Study Results with Experimental Gait Cycle Testing Results
3.4. Results of the Second Case Study of Finite Element Analyses Simulating the Stance Phases of the Gait Cycle
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Analysis | Heel Strike Phase | Loading Response Phase | Mid-Stance Phase | |||
|---|---|---|---|---|---|---|
| Maximum | Minimum | Maximum | Minimum | Maximum | Minimum | |
| Total deformation (mm) | 6.3416 | 0 | 7.1337 | 0 | 6.1659 | 0 |
| Deformation X axis (mm) | 0.9612 | −0.9616 | 1.749 | −1.2735 | 3.0399 | −1.7385 |
| Deformation Y axis (mm) | 6.3411 | −0.0761 | 7.1337 | −0.1915 | 6.1624 | −0.9437 |
| Deformation Z axis (mm) | 1.0297 | −0.8593 | 1.4182 | −1.5603 | 2.1061 | −1.7235 |
| Total elastic strain (mm/mm) | 0.6967 | 8.299 × 10−16 | 0.5902 | 4.39 × 10−16 | 0.9464 | 5.95 × 10−16 |
| Elastic strain X axis (mm/mm) | 0.3455 | −0.2559 | 0.2692 | −0.2004 | 0.4559 | −0.2695 |
| Elastic strain Y axis (mm/mm) | 0.39 | −0.6420 | 0.1909 | −0.4240 | 0.5435 | −0.6249 |
| Elastic strain Z axis (mm/mm) | 0.2724 | −0.2734 | 0.3155 | −0.1925 | 0.3726 | −0.3106 |
| Nominal stress X axis (MPa) | 0.0617 | −0.1174 | 0.0891 | −0.1704 | 0.1152 | −0.1162 |
| Nominal stress Y axis (MPa) | 0.0643 | −0.1495 | 0.0659 | −0.2107 | 0.1247 | −0.1511 |
| Nominal stress Z axis (MPa) | 0.0663 | −0.1102 | 0.0593 | −0.1604 | 0.1442 | −0.1217 |
| Shear stress XY plane (MPa) | 0.0373 | −0.0281 | 0.0488 | −0.0540 | 0.0466 | −0.0634 |
| Shear stress YZ plane (MPa) | 0.0343 | −0.0258 | 0.0537 | −0.0449 | 0.0470 | −0.0383 |
| Shear stress XZ plane (MPa) | 0.0220 | −0.0188 | 0.0331 | −0.0208 | 0.0226 | −0.0252 |
| von Mises stress (MPa) | 0.1334 | 0 | 0.1619 | 0 | 0.1289 | 0 |
| Maximum principal stress (MPa) | 0.0730 | −0.0830 | 0.0905 | −0.1536 | 0.1825 | −0.1088 |
| Minimum principal stress (MPa) | 0.0511 | −0.1672 | 0.0238 | −0.2174 | 0.0713 | −0.1653 |
| Type of Analysis | Heel Rise | Pre-Swing | ||
|---|---|---|---|---|
| Maximum | Minimum | Maximum | Minimum | |
| Total deformation (mm) | 8.1699 | 0 | 9.1625 | 0 |
| Deformation X axis (mm) | 1.6727 | −2.177 | 2.2721 | −2.7693 |
| Deformation Y axis (mm) | 8.1698 | −1.2569 | 9.1615 | −0.7243 |
| Deformation Z axis (mm) | 2.0717 | −2.6718 | 1.5841 | −2.4929 |
| Total elastic strain (mm/mm) | 1.0893 | 4.26 × 10−16 | 1.4249 | 4.029 × 10−16 |
| Elastic strain X axis (mm/mm) | 0.4747 | −0.2871 | 0.7611 | −0.3579 |
| Elastic strain Y axis (mm/mm) | 0.2355 | −0.7421 | 0.4636 | −1.1273 |
| Elastic strain Z axis (mm/mm) | 0.4177 | −0.2561 | 0.5801 | −0.5227 |
| Nominal stress X axis (MPa) | 0.0952 | −0.1973 | 0.1034 | −0.2758 |
| Nominal stress Y axis (MPa) | 0.0752 | −0.3486 | 0.1452 | −0.4176 |
| Nominal stress Z axis (MPa) | 0.1148 | −0.2508 | 0.1210 | −0.3123 |
| Shear stress XY plane (MPa) | 0.0655 | −0.1053 | 0.0704 | −0.1368 |
| Shear stress YZ plane (MPa) | 0.0693 | −0.0728 | 0.0896 | −0.0909 |
| Shear stress XZ plane (MPa) | 0.0366 | −0.0488 | 0.0453 | −0.0437 |
| von Mises stress (MPa) | 0.2005 | 0 | 0.2729 | 0 |
| Maximum principal stress (MPa) | 0.1454 | −0.1783 | 0.1531 | −0.2691 |
| Minimum principal stress (MPa) | 0.0374 | −0.3855 | 0.1013 | −0.4533 |
| Type of Analysis | Heel Strike Phase | Loading Response Phase | Mid-Stance Phase | |||
|---|---|---|---|---|---|---|
| Maximum | Minimum | Maximum | Minimum | Maximum | Minimum | |
| Total deformation (mm) | 5.0269 | 0 | 6.1577 | 0 | 4.9285 | 0 |
| Deformation X axis (mm) | 1.4225 | −0.5925 | 1.8206 | −0.8742 | 1.8526 | −1.3961 |
| Deformation Y axis (mm) | 5.0266 | −0.0705 | 6.1576 | −0.1074 | 4.9284 | −0.5991 |
| Deformation Z axis (mm) | 0.6477 | −0.5966 | 0.9268 | −0.7788 | 1.2221 | −1.3223 |
| Total elastic strain (mm/mm) | 0.3596 | 5.6254 × 10−14 | 0.3574 | 7.1839 × 10−14 | 0.7251 | 9.997 × 10−14 |
| Elastic strain X axis (mm/mm) | 0.1172 | −0.1137 | 0.1698 | −0.133 | 0.3588 | −0.2016 |
| Elastic strain Y axis (mm/mm) | 0.2019 | −0.2402 | 0.2964 | −0.2767 | 0.3121 | −0.5439 |
| Elastic strain Z axis (mm/mm) | 0.1603 | −0.1478 | 0.1329 | −0.1842 | 0.2458 | −0.3044 |
| Nominal stress X axis (MPa) | 0.0257 | −0.0571 | 0.0464 | −0.0929 | 0.0995 | −0.3104 |
| Nominal stress Y axis (MPa) | 0.019 | −0.0591 | 0.0415 | −0.099 | 0.0888 | −0.413 |
| Nominal stress Z axis (MPa) | 0.027 | −0.0605 | 0.0439 | −0.0983 | 0.0773 | −0.3432 |
| Shear stress XY plane (MPa) | 0.0143 | −0.0153 | 0.0187 | −0.0188 | 0.061 | −0.0422 |
| Shear stress YZ plane (MPa) | 0.0158 | −0.0196 | 0.0146 | −0.0141 | 0.0564 | −0.0531 |
| Shear stress XZ plane (MPa) | 0.0083 | −0.0112 | 0.0102 | −0.0116 | 0.0265 | −0.0276 |
| von Mises stress (MPa) | 0.0529 | 0 | 0.0707 | 0 | 0.1333 | 0 |
| Maximum principal stress (MPa) | 0.0424 | −0.0536 | 0.0578 | −0.0901 | 0.1196 | −0.3092 |
| Minimum principal stress (MPa) | 0.0157 | −0.0682 | 0.0299 | −0.1024 | 0.0632 | −0.4185 |
| Type of Analysis | Heel Rise | Pre-Swing | ||
|---|---|---|---|---|
| Maximum | Minimum | Maximum | Minimum | |
| Total deformation (mm) | 7.5367 | 0 | 8.4016 | 0 |
| Deformation X axis (mm) | 1.2509 | −1.8733 | 3.0257 | −1.8019 |
| Deformation Y axis (mm) | 7.5367 | −0.9327 | 8.3979 | −0.4156 |
| Deformation Z axis (mm) | 1.7482 | −2.1883 | 2.1923 | −1.6503 |
| Total elastic strain (mm/mm) | 1.0011 | 4.7186 × 10−16 | 1.0424 | 1.5761 × 10−15 |
| Elastic strain X axis (mm/mm) | 0.4901 | −0.2881 | 0.5395 | −0.2877 |
| Elastic strain Y axis (mm/mm) | 0.2103 | −0.7489 | 0.4538 | −0.9172 |
| Elastic strain Z axis (mm/mm) | 0.4304 | −0.2245 | 0.4146 | −0.3263 |
| Nominal stress X axis (MPa) | 0.0912 | −0.1922 | 0.1105 | −0.3156 |
| Nominal stress Y axis (MPa) | 0.0757 | −0.3103 | 0.0724 | −0.3358 |
| Nominal stress Z axis (MPa) | 0.0813 | −0.2218 | 0.0874 | −0.3223 |
| Shear stress XY plane (MPa) | 0.0732 | −0.0897 | 0.0611 | −0.0702 |
| Shear stress YZ plane (MPa) | 0.0543 | −0.0698 | 0.0636 | −0.1045 |
| Shear stress XZ plane (MPa) | 0.0303 | −0.0369 | 0.0417 | −0.028 |
| von Mises stress (MPa) | 0.168 | 0 | 0.1874 | 0 |
| Maximum principal stress (MPa) | 0.14 | −0.1638 | 0.1187 | −0.3047 |
| Minimum principal stress (MPa) | 0.0642 | −0.3242 | 0.0384 | −0.3572 |
References
- Lou, C.; Wang, S.; Liang, T.; Pang, C.; Huang, L.; Run, M.; Liu, X. A Graphene-Based Flexible Pressure Sensor with Applications to Plantar Pressure Measurement and Gait Analysis. Materials 2017, 10, 1068. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Lewis, C.L.; Gill, S.V. Effects of obesity and foot arch height on gaitmechanics: A cross-sectional study. PLoS ONE 2021, 16, e0260398. [Google Scholar] [CrossRef] [PubMed]
- Mei, Q.; Kim, H.K.; Xiang, L.; Shim, V.; Wang, A.; Baker, J.S.; Gu, Y.; Fernandez, J. Toward improved understanding of foot shape, foot posture, and foot biomechanics during running: A narrative review. Front. Physiol. 2022, 13, 1062598. [Google Scholar] [CrossRef]
- Ang, C.K.; Solihin, M.I.; Chan, W.J.; Ong, Y.Y. Study of Plantar Pressure Distribution. MATEC Web. Conf. 2018, 237, 01016. [Google Scholar] [CrossRef]
- Nandikolla, K.V.; Bochen, R.; Meza, S.; Garcia, A. Experimental Gait Analysis to Study Stress Distribution of the Human Foot. J. Med. Eng. 2017, 2017, 3432074. [Google Scholar] [CrossRef] [PubMed]
- Pirker, W.; Katzenschlager, R. Gait disorders in adults and the elderly. Wien. Klin. Wochenschr. 2017, 129, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Cicirelli, G.; Impedovo, D.; Dentamaro, V.; Marani, R.; Pirlo, G.; D’Orazio, T.R. Human Gait Analysis in Neurodegenerative Diseases: A Review. IEEE J. Biomed. Health Inform. 2022, 26, 229–242. [Google Scholar] [CrossRef]
- Stöckel, T.; Jacksteit, R.; Behrens, M.; Skripitz, R.; Bader, R.; Mau-Moeller, A. The mental representation of the human gait in young and older adults. Front. Psychol. 2015, 6, 943. [Google Scholar] [CrossRef] [PubMed]
- Hulleck, A.A.; Menoth-Mohan, D.; Abdallah, N.; El-Rich, M.; Khalaf, K. Present and future of gait assessment in clinical practice: Towards the application of novel trends and technologies. Front. Med. Technol. 2022, 4, 901331. [Google Scholar] [CrossRef]
- Taş, S.; Çetin, A. An investigation of the relationship between plantar pressure distribution and the morphologic and mechanic properties of the intrinsic foot muscles and plantar fascia. Gait Post. 2019, 72, 217–221. [Google Scholar] [CrossRef]
- Rusu, L.; Paun, E.; Marin, M.I.; Hemanth, J.; Rusu, M.R.; Calina, M.L.; Bacanoiu, M.V.; Danoiu, M.; Danciulescu, D. Plantar Pressure and Contact Area Measurement of Foot Abnormalities in Stroke Rehabilitation. Brain Sci. 2021, 11, 1213. [Google Scholar] [CrossRef]
- Abdul Razak, A.H.; Zayegh, A.; Begg, R.K.; Wahab, Y. Foot Plantar Pressure Measurement System: A Review. Sensors 2012, 12, 9884–9912. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.-L.; Dai, Y.-N.; Grimaldi, N.S.; Lin, J.-J.; Hu, B.-Y.; Wu, Y.-F.; Gao, S. Plantar Pressure-Based Insole Gait Monitoring Techniques for Diseases Monitoring and Analysis: A Review. Adv. Mater. Technol. 2022, 7, 2100566. [Google Scholar] [CrossRef]
- Jones, A.D.; Crossland, S.R.; Nixon, J.E.; Siddle, H.J.; Russell, D.A.; Culmer, P.R. STrain Analysis and Mapping of the Plantar Surface (STAMPS): A novel technique of plantar load analysis during gait. Proc. Inst. Mech. Eng. H 2023, 237, 841–854. [Google Scholar] [CrossRef] [PubMed]
- Crossland, S.R.; Siddle, H.J.; Culmer, P.; Brockett, C.L. A plantar surface shear strain methodology utilising Digital Image Correlation. J. Mech. Behav. Biomed. Mater. 2022, 136, 105482. [Google Scholar] [CrossRef] [PubMed]
- Syed, N.; Karvannan, H.; Maiya, A.G.; Binukumar, B.; Prem, V.; Chakravarty, R.D. Plantar pressure distribution among asymptomatic individuals: A cross-sectional study. Foot Ankle Spec. 2012, 5, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Chatwin, K.E.; Abbott, C.A.; Boulton, A.J.M.; Bowling, F.L.; Reeves, N.D. The role of foot pressure measurement in the prediction and prevention of diabetic foot ulceration—A comprehensive review. Diabetes Metab. Res. Rev. 2020, 36, e3258. [Google Scholar] [CrossRef] [PubMed]
- Trejo-Enriquez, A.; Urriolagoitia-Sosa, G.; Romero-Ángeles, B.; García-Laguna, M.Á.; Guzmán-Baeza, M.; Martínez-Reyes, J.; Rojas-Castrejon, Y.Y.; Gallegos-Funes, F.J.; Patiño-Ortiz, J.; Urriolagoitia-Calderón, G.M. Numerical Evaluation Using the Finite Element Method on Frontal Craniocervical Impact Directed at Intervertebral Disc Wear. Appl. Sci. 2023, 13, 11989. [Google Scholar] [CrossRef]
- Maya-Anaya, D.; Urriolagoitia-Sosa, G.; Romero-Ángeles, B.; Martinez-Mondragon, M.; German-Carcaño, J.M.; Correa-Corona, M.I.; Trejo-Enríquez, A.; Sánchez-Cervantes, A.; Urriolagoitia-Luna, A.; Urriolagoitia-Calderón, G.M. Numerical Analysis Applying the Finite Element Method by Developing a Complex Three-Dimensional Biomodel of the Biological Tissues of the Elbow Joint Using Computerized Axial Tomography. Appl. Sci. 2023, 13, 8903. [Google Scholar] [CrossRef]
- Cruz-López, S.; Urriolagoitia-Sosa, G.; Romero-Ángeles, B.; Urriolagoitia-Calderón, G.M.; Marquet-Rivera, R.A.; Hernández-Vázquez, R.A.; Mastache-Miranda, O.A.; Vázquez-Feijo, J.A. Biomechanical analysis of the femur bone with the cotyle of the hip prosthesis. MOJ Appl. Bionics Biomech. 2023, 7, 11–12. [Google Scholar] [CrossRef]
- Martinez-Mondragon, M.; Urriolagoitia-Sosa, G.; Romero-Ángeles, B.; Pérez-Partida, J.C.; Cruz-Olivares, I.M.; Urriolagoitia-Calderón, G. Bilinear Numerical Analysis of the Structural Behavior of a Dental Implant Applied as a Biomaterial Carbon Fiber Reinforced Polyether-Ether-Ketone (CFR-PEEK): A Finite Element Analysis. Dent. Hypoth. 2023, 14, 45–48. [Google Scholar]
- Telfer, S.; Erdemir, A.; Woodburn, J.; Cavanagh, P.R. What Has Finite Element Analysis Taught Us about Diabetic Foot Disease and Its Management? A Systematic Review. PLoS ONE 2014, 9, e109994. [Google Scholar] [CrossRef] [PubMed]
- Rai, D.V.; Aggarwal, L.M. The Study of Plantar Pressure Distribution in Normal and Pathological Foot. Pol. J. Med. Phys. Eng. 2006, 12, 25–34. [Google Scholar]
- Ukobitz, D.; Faullant, R. Leveraging 3D Printing Technologies: The Case of Mexico’s Footwear Industry. Res.—Technol. Manag. 2021, 64, 20–30. [Google Scholar] [CrossRef]
- Jandova, S.; Mendricky, R. Benefits of 3D Printed and Customized Anatomical Footwear Insoles for Plantar Pressure Distribution. 3D Print. Addit. Manuf. 2022, 9, 547–556. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.H.; Trubayev, S.; Shehab, E. 3D Printed Large-Scale Insole and Its Challenges. In Proceedings of the 8th Brunei International Conference on Engineering and Technology 2021, Universiti Teknologi Brunei, Seri Begawan, Brunei Darussalam, 8–10 November 2021. [Google Scholar]
- Shaikh, S.; Jamdade, B.; Chanda, A. Effects of Customized 3D-Printed Insoles in Patients with Foot-Related Musculoskeletal Ailments—A Survey-Based Study. Prosthesis 2023, 5, 550–561. [Google Scholar] [CrossRef]
- Chen, R.K.; Jin, Y.-A.; Wensman, J.; Shih, A. Additive manufacturing of custom orthoses and prostheses—A review. Addit. Manuf. 2016, 12, 77–89. [Google Scholar] [CrossRef]
- Wu, S.; Zeng, T.; Liu, Z.; Ma, G.; Xiong, Z.; Zuo, L.; Zhou, Z. 3D Printing Technology for Smart Clothing: A Topic Review. Materials 2022, 15, 7391. [Google Scholar] [CrossRef]
- Kumar, R.; Sarangi, S.K. 3D-Printed Orthosis: A Review on Design Process and Material Selection for Fused Deposition Modeling Process. In Advances in Materials Processing and Manufacturing Applications, 1st ed.; Patnaik, A., Kozeschnik, E., Kukshal, V., Eds.; Springer Singapore Publishing: Singapore, 2021; Volume 1, pp. 531–538. [Google Scholar]
- Rodriguez-Colon, R.; Nayak, V.V.; Parente, P.E.L.; Leucht, P.; Tovar, N.; Lin, C.C.; Rezzadeh, K.; Hacquebord, J.H.; Coelho, P.G.; Witek, L. The presence of 3D printing in orthopedics: A clinical and material review. J. Orthop. Res. 2023, 41, 601–613. [Google Scholar] [CrossRef]
- Kumar, P.; Rajak, D.K.; Abubakar, M.; Ali, S.G.M.; Hussain, M. 3D Printing Technology for Biomedical Practice: A Review. J. Mater. Eng. Perform. 2021, 30, 5342–5355. [Google Scholar] [CrossRef]
- Gelaziene, E.; Milasiene, D. Influence of the Type of Plastic and Printing Technologies on the Compressive Behavior of 3D-Printed Heel Prototypes. Materials 2023, 16, 1930. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, R.; Coelho, C.; Oliveira, J.; Gomes, J.; Pinto, V.V.; Ferreira, M.J.; Nóbrega, J.M.; Silva, A.F.D.; Carneiro, O.S. Towards Customized Footwear with Improved Comfort. Materials 2021, 14, 1738. [Google Scholar] [CrossRef]
- Rico-Baeza, G.; Pérez-Soto, G.I.; Morales-Hernández, L.A.; Cuan-Urquizo, E.; Camarillo-Gómez, K.A. Additively Manufactured Foot Insoles Using Body-Centered Cubic (BCC) and Triply Periodic Minimal Surface (TPMS) Cellular Structures. Appl. Sci. 2023, 13, 12665. [Google Scholar] [CrossRef]
- Kermavnar, T.; Shannon, A.; O’Sullivan, L.W. The application of additive manufacturing/3D printing in ergonomic aspects of product design: A systematic review. Appl. Ergon. 2021, 97, 103528. [Google Scholar] [CrossRef] [PubMed]
- Walker, K.J.; Przestrzelski, B.T.; Kaluf, B.; Driggers, N.H.; Ballard, W.D., 2nd; Pruett, T.C.; Hoeffner, S.L.; DesJardins, J.D. Novel 3D-printed foot orthoses with variable hardness: A comfort comparison to traditional orthoses. Med. Eng. Phys. 2023, 115, 103978. [Google Scholar] [CrossRef] [PubMed]
- Hudak, Y.F.; Li, J.S.; Cullum, S.; Strzelecki, B.M.; Richburg, C.; Kaufman, G.E.; Abrahamson, D.; Heckman, J.T.; Ripley, B.; Telfer, S.; et al. A novel workflow to fabricate a patient-specific 3D printed accommodative foot orthosis with personalized latticed metamaterial. Med. Eng. Phys. 2022, 104, 103802. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.C.L.; Lin, G.; Wang, M.J.J. Comparing 3D foot scanning with conventional measurement methods. J. Foot Ankle Res. 2014, 7, 44. [Google Scholar] [CrossRef]
- Sacco, R.; Munoz, M.-A.; Billuart, F.; Lalevée, M.; Beldame, J. Validation of an Automated Optical Scanner for a Comprehensive Anthropometric Analysis of the Foot and Ankle. Bioengineering 2023, 10, 968. [Google Scholar] [CrossRef] [PubMed]
- Silva, R.; Silva, B.; Fernandes, C.; Morouço, P.; Alves, N.; Veloso, A. A Review on 3D Scanners Studies for Producing Customized Orthoses. Sensors 2024, 24, 1373. [Google Scholar] [CrossRef]
- Barrios-Muriel, J.; Romero-Sánchez, F.; Alonso-Sánchez, F.J.; Rodríguez Salgado, D. Advances in Orthotic and Prosthetic Manufacturing: A Technology Review. Materials 2020, 13, 295. [Google Scholar] [CrossRef]
- Farhan, M.; Wang, J.Z.; Bray, P.; Burns, J.; Cheng, T.L. Comparison of 3D scanning versus traditional methods of capturing foot and ankle morphology for the fabrication of orthoses: A systematic review. J. Foot Ankle Res. 2021, 14, 2. [Google Scholar] [CrossRef] [PubMed]
- Rogati, G.; Leardini, A.; Ortolani, M.; Caravaggi, P. Semi-automatic measurements of foot morphological parameters from 3D plantar foot scans. J. Foot Ankle Res. 2021, 14, 18. [Google Scholar] [CrossRef] [PubMed]
- Chhikara, K.; Sidhu, S.S.; Gupta, S.; Saharawat, S.; Kataria, C.; Chanda, A. Development and Effectiveness Testing of a Novel 3D-Printed Multi-Material Orthosis in Nurses with Plantar Foot Pain. Prosthesis 2023, 5, 73–87. [Google Scholar] [CrossRef]
- Hasibuzzaman, M.; Wahab, A.A.; Seng, G.H.; Ramlee, M.H. Three-dimensional printed orthosis in biomedical application: A short review. J. Phys. Conf. Ser. 2021, 2071, 012025. [Google Scholar] [CrossRef]
- Agarwal, R.; Malhotra, S.; Gupta, V.; Jain, V. The application of Three-dimensional printing on foot fractures and deformities: A mini-review. Ann. 3D Print. Med. 2022, 5, 100046. [Google Scholar] [CrossRef]
- Negru, N.; Leba, M.; Rosca, S.; Marica, L.; Ionica, A. A new approach on 3D scanning-printing technologies with medical applications. IOP Conf. Ser. Mater. Sci. Eng. 2019, 572, 012049. [Google Scholar] [CrossRef]
- Brognara, L.; Mafla-España, M.A.; Gil-Molina, I.; Castillo-Verdejo, Y.; Cauli, O. The Effects of 3D Custom Foot Orthotics with Mechanical Plantar Stimulation in Older Individuals with Cognitive Impairment: A Pilot Study. Brain Sci. 2022, 12, 1669. [Google Scholar] [CrossRef]
- Anggoro, P.W.; Tauviqirrahman, M.; Jamari, J.; Bayuseno, A.P.; Bawono, B.; Avelina, M.M. Computer-aided reverse engineering system in the design and production of orthotic insole shoes for patients with diabetes. Cogent Eng. 2018, 5, 1470916. [Google Scholar] [CrossRef]
- Mo, S.; Leung, S.H.S.; Chan, Z.Y.S.; Sze, L.K.Y.; Mok, K.M.; Yung, P.S.H.; Ferber, R.; Cheung, R.T.H. The biomechanical difference between running with traditional and 3D printed orthoses. J. Sports Sci. 2019, 37, 2191–2197. [Google Scholar] [CrossRef]
- Wang, Y.; Jiang, W.; Gan, Y.; Yu, Y.; Dai, K. Clinical Observation of 3D Printing Technology in Insoles for Flexible Flatfoot Patients. J. Shanghai Jiaotong Univ. 2021, 26, 398–403. [Google Scholar] [CrossRef]
- Mueller, J.; Richter, M.; Schaefer, K.; Ganz, J.; Lohscheller, J.; Mueller, S. How to measure children’s feet: 3D foot scanning compared with established 2D manual or digital methods. J. Foot Ankle Res. 2023, 16, 21. [Google Scholar] [CrossRef]
- Lin, K.-W.; Chou, L.-W.; Su, Y.-T.; Wei, S.-H.; Chen, C.-S. Biomechanical Effect of 3D-Printed Foot Orthoses in Patients with Knee Osteoarthritis. Appl. Sci. 2021, 11, 4200. [Google Scholar] [CrossRef]
- Shih, K.-S.; Jhou, S.-Y.; Hsu, W.-C.; Hsu, C.-C.; Chen, J.-W.; Yeh, J.-C.; Hung, Y.-C. A Biomechanical Investigation of Athletic Footwear Traction Performance: Integration of Gait Analysis with Computational Simulation. Appl. Sci. 2020, 10, 1672. [Google Scholar] [CrossRef]
- Niu, J.; Liu, J.; Zheng, Y.; Ran, L.; Chang, Z. Are arch-conforming insoles a good fit for diabetic foot? Insole customized design by using finite element analysis. Hum. Factors Ergon. Manuf. 2020, 30, 303–310. [Google Scholar] [CrossRef]
- Zhang, H.; Lin-Lv, M.; Yang, J.; Niu, W.; Cheung, J.C.; Sun, W.; Wong, D.W.; Ni, M. Computational modelling of foot orthosis for midfoot arthritis: A Taguchi approach for design optimization. Acta Bioeng. Biomech. 2020, 22, 75–83. [Google Scholar] [PubMed]
- Serrato-Pedrosa, J.A.; Urriolagoitia-Sosa, G.; Romero-Ángeles, B.; Urriolagoitia-Calderón, G.M.; Cruz-López, S.; Urriolagoitia-Luna, A.; Carbajal-López, D.E.; Guereca-Ibarra, J.R.; Murillo-Aleman, G. Biomechanical Evaluation of Plantar Pressure Distribution towards a Customized 3D Orthotic Device: A Methodological Case Study through a Finite Element Analysis Approach. Appl. Sci. 2024, 14, 1650. [Google Scholar] [CrossRef]
- Jastifer, J.R. Intrinsic muscles of the foot: Anatomy, function, rehabilitation. Phys. Ther. Sport 2023, 61, 27–36. [Google Scholar] [CrossRef]
- Zulkifli, S.S.; Loh, W.P. A state-of-the-art review of foot pressure. Foot Ankle Surg. 2020, 26, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.D.; De Siqueira, J.; Nixon, J.E.; Siddle, H.J.; Culmer, P.R.; Russell, D.A. Plantar shear stress in the diabetic foot: A systematic review and meta-analysis. Diabet. Med. 2022, 39, e14661. [Google Scholar] [CrossRef]
- Oliveira, L.B.; Maranho, D.A.; Cliquet, A.; Dinato, M.C.M.E.; Pagnano, R.G. Reliability of wireless insole baropodometry of normal individual’s gait. Acta Ortop. Bras. 2021, 29, 238–241. [Google Scholar] [CrossRef]
- Chevalier, T.L.; Hodgins, H.; Chockalingam, N. Plantar pressure measurements using an in-shoe system and a pressure platform: A comparison. Gait Posture 2010, 31, 397–399. [Google Scholar] [CrossRef] [PubMed]
- Luboz, V.; Perrier, A.; Bucki, M.; Diot, B.; Cannard, F.; Vuillerme, N.; Payan, Y. Influence of the calcaneus shape on the risk of posterior heel ulcer using 3D patient-specific biomechanical modeling. Ann. Biomed. Eng. 2015, 43, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Mo, Z.; Guo, J.; Fan, Y. The effect of arch height and material hardness of personalized insole on correction and tissues of flatfoot. J. Heathc. Eng. 2017, 2017, 8614341. [Google Scholar] [CrossRef]
- Kharazi, M.; Bohm, S.; Theodorakis, C.; Mersmann, F.; Arampatzis, A. Quantifying mechanical loading and elastic strain energy of the human Achilles tendon during walking and running. Sci. Rep. 2021, 11, 5830. [Google Scholar] [CrossRef] [PubMed]
- Bojsen-Møller, F.; Lamoreux, L. Significance of free-dorsiflexion of the toes in walking. Acta. Orthop. Scand. 1979, 50, 471–479. [Google Scholar] [CrossRef]
- Shaulian, H.; Gefen, A.; Wolf, A. Computational modeling of the plantar tissue stresses induced by the clinical practice of off-loading of the diabetic foot. In The Science, Etiology and Mechanobiology of Diabetes and its Complications, 1st ed.; Gefen, A., Ed.; Academic Press: London, UK, 2021; Volume 1, p. 38. [Google Scholar]
- Chokhandre, S.; Halloran, J.P.; van den Bogert, A.J.; Erdemir, A. A three-dimensional inverse finite element analysis of the heel pad. J. Biomech. Eng. 2012, 134, 031002. [Google Scholar] [CrossRef] [PubMed]
- Strzalkowski, N.D.; Triano, J.J.; Lam, C.K.; Templeton, C.A.; Bent, L.R. Thresholds of skin sensitivity are partially influenced by mechanical properties of the skin on the foot sole. Physiol. Rep. 2015, 3, e12425. [Google Scholar] [CrossRef]
- Zhang, M.; Mak, A.F.T. In vivo friction properties of human skin. Prosthet. Orthot. Int. 1999, 23, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Van Alsenoy, K.; van der Linden, M.L.; Ryu, J.H.; Girard, O.; Al Raisi, L.; Santos, D. Isolated and combined effects of EVA and TPU custom foot orthoses on constant speed, treadmill running kinematics. Front. Earth Sci. 2023, 11, 1170661. [Google Scholar] [CrossRef]
- Zolfagharian, A.; Lakhi, M.; Ranjbar, S.; Bodaghi, M. Custom Shoe Sole Design and Modeling Toward 3D Printing. Int. J. Bioprint. 2021, 7, 396. [Google Scholar] [CrossRef]
- Xie, J.; Zhou, Z.; Luo, T.; Pang, H.; Meng, X.; Zhou, F. Study on Design and Additive Manufacturing of Customized Bionic Sports Sole for the Elderly. IEEE Access 2021, 9, 69830–69838. [Google Scholar] [CrossRef]
- Li, J.; Shu, W.; Yang, Y.; Yan, R. Parametric modeling and performance analysis of a personalized insole based on 3D scanning and selective laser sintering. Int. J. Comp. Integr. Manuf. 2020, 33, 936–945. [Google Scholar] [CrossRef]
- Ravi, T.; Ranganathan, R.; Ramesh, S.P.; Dandotiya, D.S. 3D Printed Personalized Orthotic Inserts Using Photogrammetry and FDM Technology. In Fused Deposition Modeling Based 3D Printing. Materials Forming, Machining and Tribology, 1st ed.; Dave, H.K., Davim, J.P., Eds.; Springer International Publishing: Cham, Switzerland, 2021; Volume 1, pp. 349–361. [Google Scholar]
- Danko, M.; Sekac, J.; Dzivakova, E.; Zivcak, J.; Hudak, R. 3D Printing of Individual Running Insoles—A Case Study. Orthop. Res. Rev. 2023, 15, 105–118. [Google Scholar] [CrossRef] [PubMed]
- Brognara, L.; Navarro-Flores, E.; Iachemet, L.; Serra-Catalá, N.; Cauli, O. Beneficial Effect of Foot Plantar Stimulation in Gait Parameters in Individuals with Parkinson’s Disease. Brain Sci. 2020, 10, 69. [Google Scholar] [CrossRef]
- Anggoro, P.W.; Bawono, B.; Jamari, J.; Tauviqirrahman, M.; Bayuseno, A.P. Advanced design and manufacturing of custom orthotics insoles based on hybrid Taguchi-response surface method. Heliyon 2021, 7, e06481. [Google Scholar] [CrossRef]
- Yildiz, K.; Medetalibeyoglu, F.; Kaymaz, I.; Ulusoy, G.R. Triad of foot deformities and its conservative treatment: With a 3D customized insole. Proc. Inst. Mech. Eng. Part. H J. Eng. Med. 2021, 235, 780–791. [Google Scholar] [CrossRef]
- Nouman, M.; Chong, D.Y.R.; Srewaradachpisal, S.; Chatpun, S. The Effect of Customized Insole Pads on Plantar Pressure Distribution in a Diabetic Foot with Neuropathy: Material and Design Study Using Finite Element Analysis Approach. Appl. Sci. 2023, 13, 399. [Google Scholar] [CrossRef]
- Nouman, M.; Dissaneewate, T.; Chong, D.Y.R.; Chatpun, S. Effects of thickness and length of custom made insole on plantar pressure for diabetic foot with neuropathy: A finite element approach. Songklanakarin J. Sci. Technol. 2021, 43, 1677–1684. [Google Scholar]
- Tang, L.; Wang, L.; Bao, W.; Zhu, S.; Li, D.; Zhao, N.; Liu, C. Functional gradient structural design of customized diabetic insoles. Songklanakarin J. Mech. Behav. Biomed. Mater. 2019, 94, 279–287. [Google Scholar] [CrossRef]
- Lemmon, D.; Shiang, T.; Hashmi, A.; Ulbrecht, J.S.; Cavanagh, P.R. The effect of insoles in therapeutic footwear—A finite element approach. J. Biomech. 1997, 30, 615–620. [Google Scholar] [CrossRef]
- Rawlings, N. The Way We Stand: A Sequential Case Study on Foot Angle. J. Biosci. Med. 2023, 11, 79–89. [Google Scholar] [CrossRef]
- Ghazali, M.J.; Ren, X.; Rajabi, A.; Zamri, W.F.H.W.; Mohd Mustafah, N.; Ni, J. Finite Element Analysis of Cushioned Diabetic Footwear Using Ethylene Vinyl Acetate Polymer. Polymers 2021, 13, 2261. [Google Scholar] [CrossRef]
- Akrami, M.; Qian, Z.; Zou, Z.; Howard, D.; Nester, C.J.; Ren, L. Subject-specific finite element modelling of the human foot complex during walking: Sensitivity analysis of material properties, boundary and loading conditions. Biomech. Model Mechanobiol. 2018, 17, 559–576. [Google Scholar] [CrossRef]
- Wang, Y.; Li, Z.; Wong, D.W.; Cheng, C.K.; Zhang, M. Finite element analysis of biomechanical effects of total ankle arthroplasty on the foot. J. Orthop. Translat. 2017, 12, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.M.; Lee, S.J.; Lee, P.V.S. Plantar pressure relief under the metatarsal heads: Therapeutic insole design using three-dimensional finite element model of the foot. J. Biomech. 2015, 48, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Budhabhatti, S.P.; Erdemir, A.; Petre, M.; Sferra, J.; Donley, B.; Cavanagh, P.R. Finite element modeling of the first ray of the foot: A tool for the design of interventions. J. Biomech. Eng. 2007, 129, 750–756. [Google Scholar] [CrossRef]
- Mo, F.; Li, Y.; Li, J.; Zhou, S.; Yang, Z. A three-dimensional finite element foot-ankle model and its personalisation methods analysis. Int. J. Mech. Sci. 2022, 219, 107108. [Google Scholar] [CrossRef]






















| Material | Young’s Modulus (MPa) | Poisson’s Ratio |
|---|---|---|
| Foot skin | 0.2 | 0.485 |
| Foot muscles | 0.06 | 0.495 |
| Plate support | 210,000 | 0.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serrato-Pedrosa, J.A.; Urriolagoitia-Sosa, G.; Romero-Ángeles, B.; Carrasco-Hernández, F.; Gallegos-Funes, F.J.; Trejo-Enriquez, A.; Carbajal-López, A.; Gomez-Niebla, J.A.; Correa-Corona, M.I.; Urriolagoitia-Calderón, G.M. Numerical Analysis of the Plantar Pressure Points during the Stance Phases for the Design of a 3D-Printable Patient-Specific Insole. Prosthesis 2024, 6, 429-456. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis6030032
Serrato-Pedrosa JA, Urriolagoitia-Sosa G, Romero-Ángeles B, Carrasco-Hernández F, Gallegos-Funes FJ, Trejo-Enriquez A, Carbajal-López A, Gomez-Niebla JA, Correa-Corona MI, Urriolagoitia-Calderón GM. Numerical Analysis of the Plantar Pressure Points during the Stance Phases for the Design of a 3D-Printable Patient-Specific Insole. Prosthesis. 2024; 6(3):429-456. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis6030032
Chicago/Turabian StyleSerrato-Pedrosa, Jesus Alejandro, Guillermo Urriolagoitia-Sosa, Beatriz Romero-Ángeles, Francisco Carrasco-Hernández, Francisco Javier Gallegos-Funes, Alfonso Trejo-Enriquez, Alfredo Carbajal-López, Jorge Alberto Gomez-Niebla, Martin Ivan Correa-Corona, and Guillermo Manuel Urriolagoitia-Calderón. 2024. "Numerical Analysis of the Plantar Pressure Points during the Stance Phases for the Design of a 3D-Printable Patient-Specific Insole" Prosthesis 6, no. 3: 429-456. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis6030032