

Integrating Spatial and Non-Spatial Dimensions to Evaluate Access to Rural Primary Healthcare Service: A Case Study of Songzi, China
Abstract
:1. Background
2. Materials and Methods
2.1. Study Area and Data
2.2. Research Methods
2.2.1. Measure Spatial Access
2.2.2. Investigate Non-Spatial Access
2.2.3. Integrating Spatial and Non-Spatial Access
3. Results
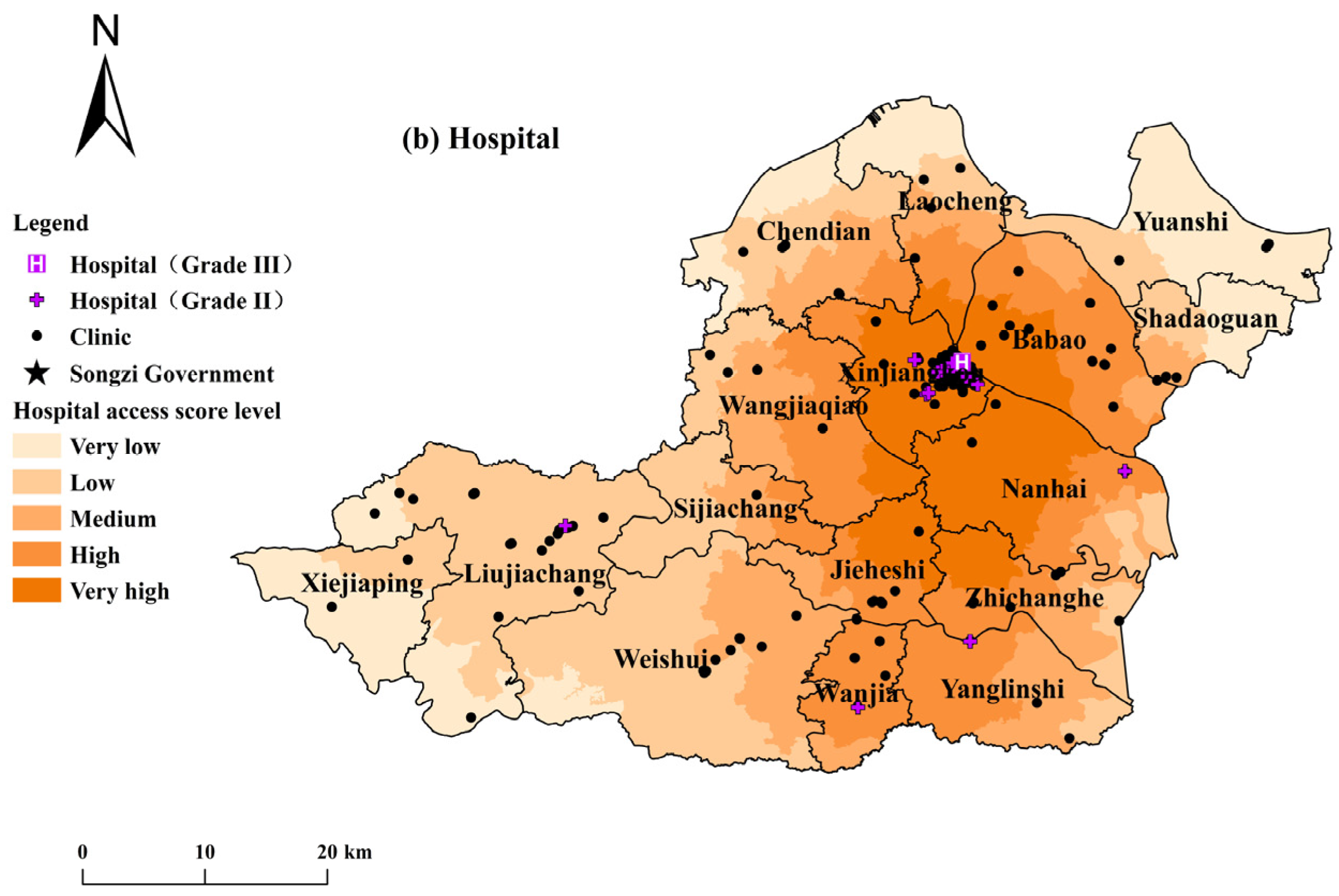
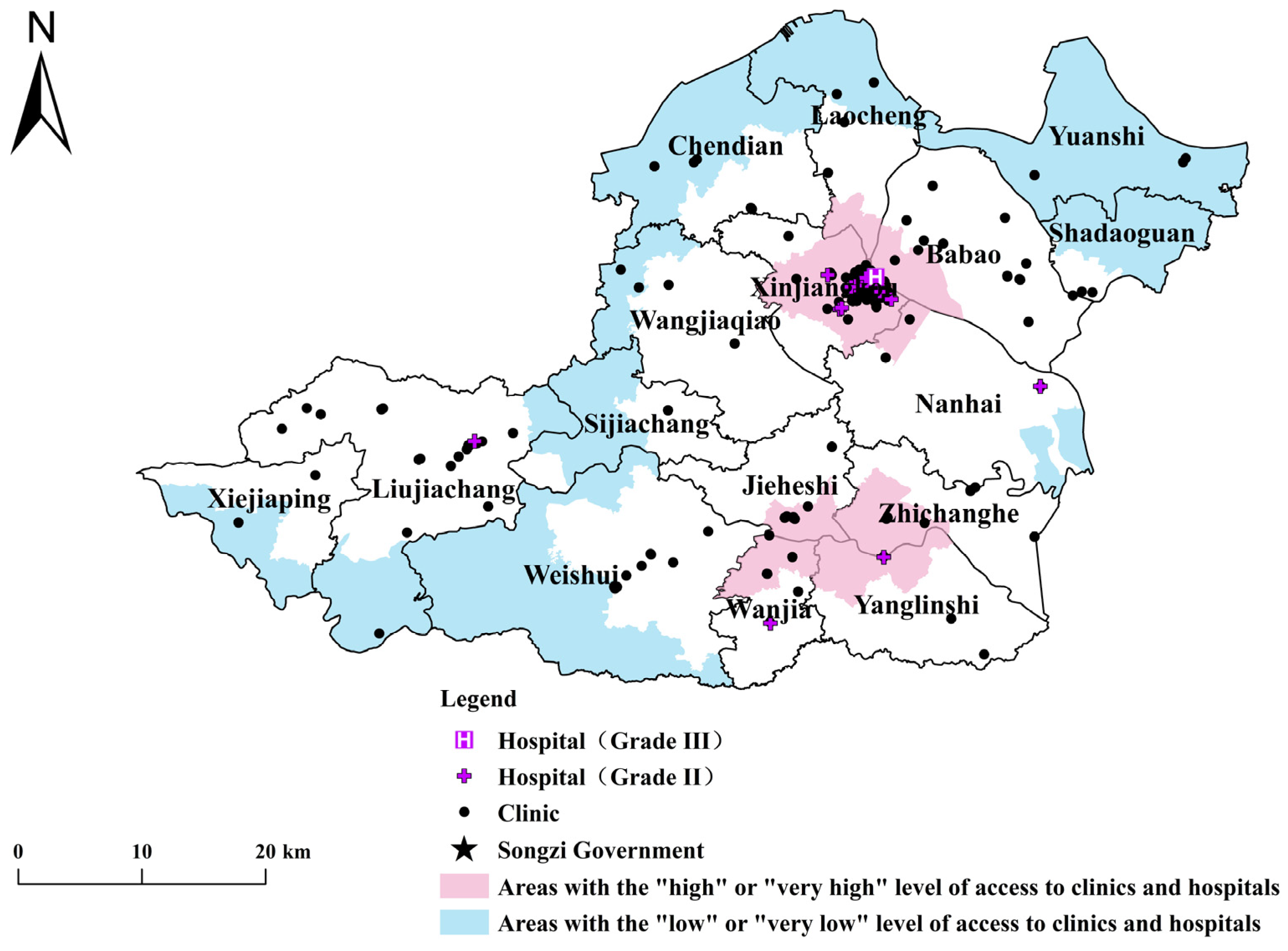
3.1. Spatial Access to Primary Healthcare Services
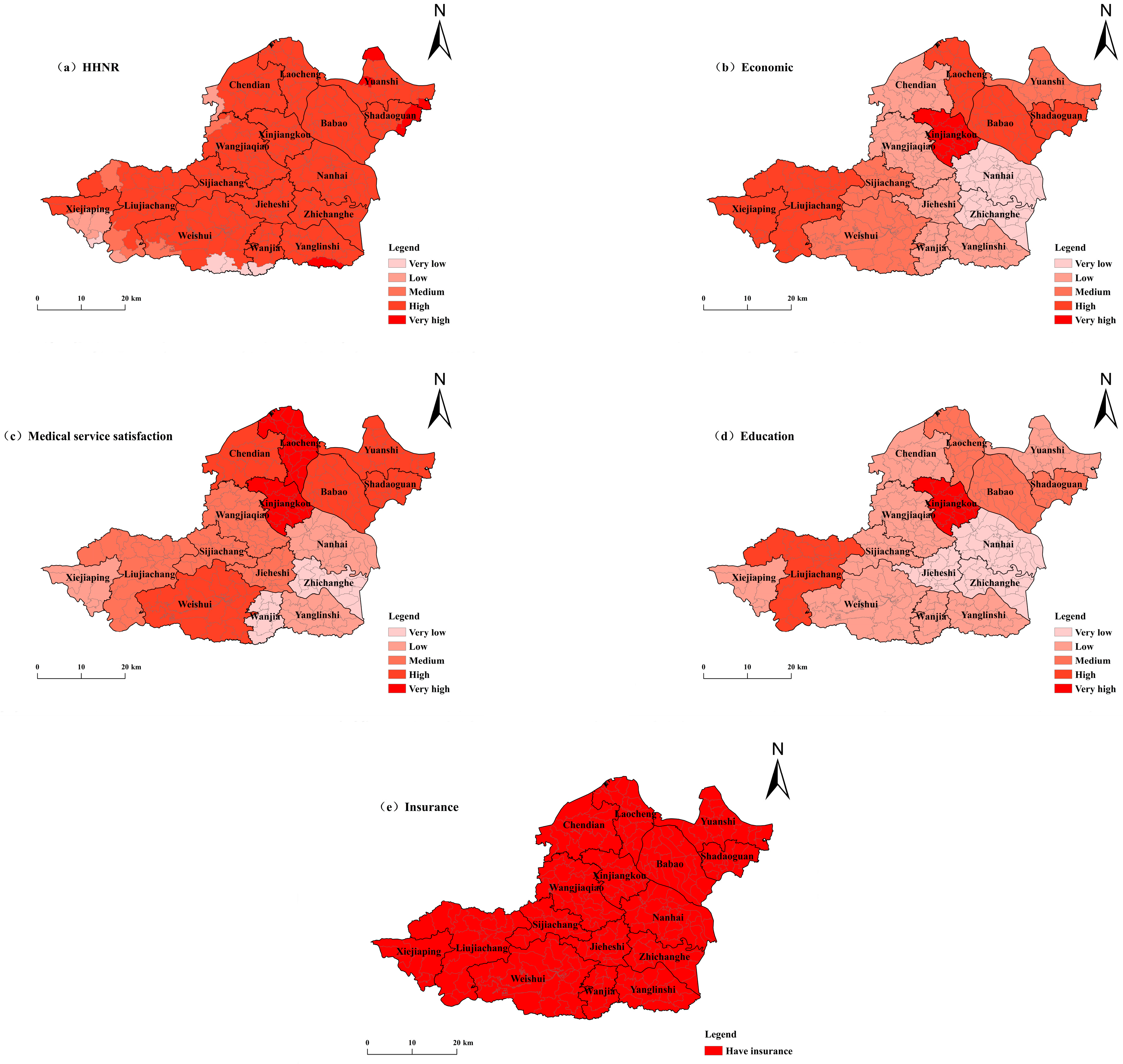
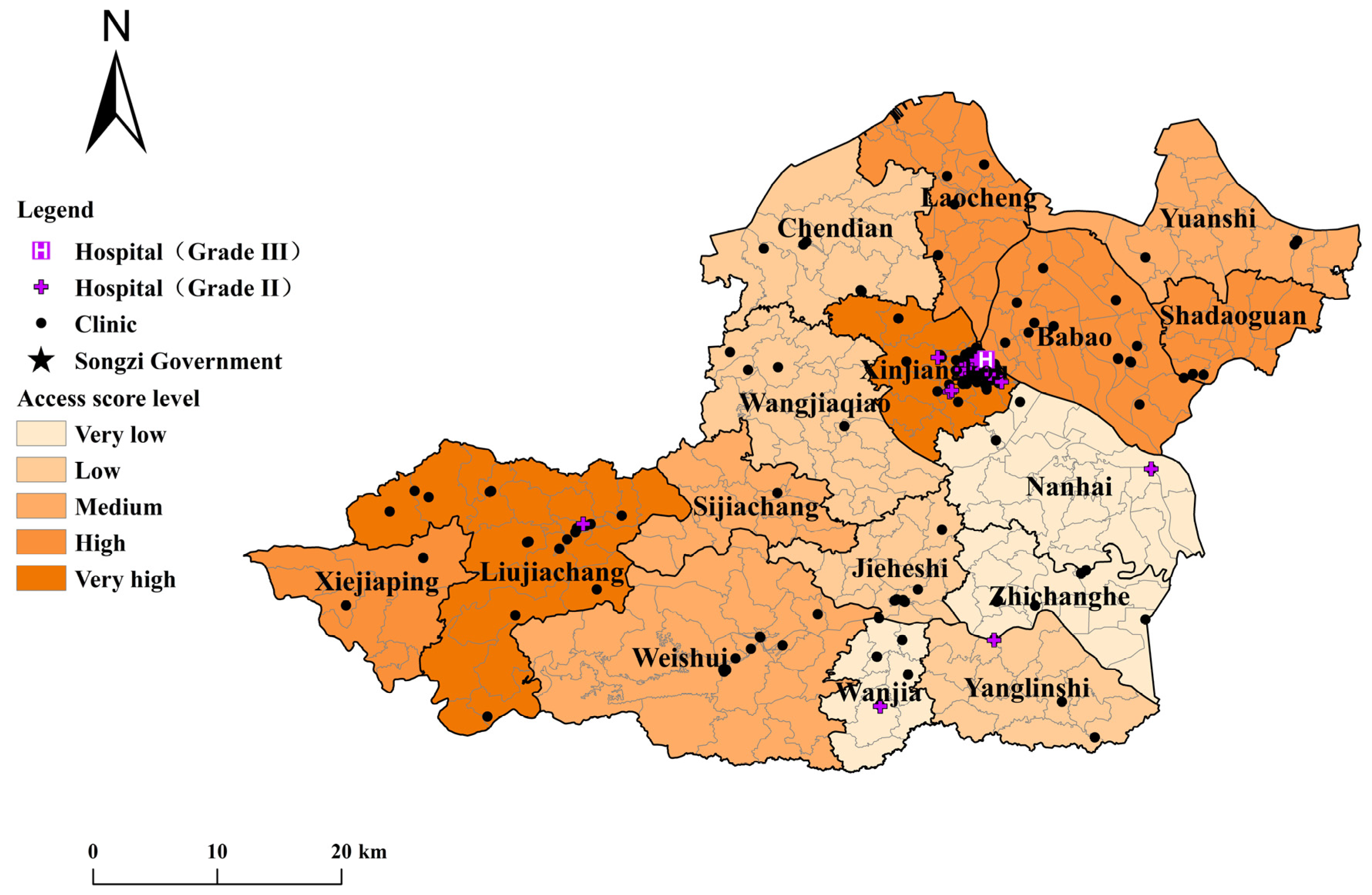
3.2. Integrating Spatial and Non-Spatial Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Graves, B.A. Integrative literature review: A review of literature related to geographical information systems, healthcare access, and health outcomes. Perspect. Health Inf. Manag. AHIMA Am. Health Inf. Manag. Assoc. 2008, 5, 1652–1655. [Google Scholar] [CrossRef]
- Caldwell, J.T.; Ford, C.L.; Wallace, S.P.; Wang, M.C.; Takahashi, L.M. Intersection of living in a rural versus urban area and race/ethnicity in explaining access to health care in the United States. Am. J. Public Health 2016, 106, 1463–1469. [Google Scholar] [CrossRef] [PubMed]
- Gaffney, A.W.; Hawks, L.; White, A.C.; Woolhandler, S.; Himmelstein, D.; Christiani, D.C.; McCormick, D. Health care disparities across the urban-rural divide: A national study of individuals with COPD. J. Rural Health 2020, 38, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Curtis, S.; Riva, M. Health geographies I: Complexity theory and human health. Prog. Hum. Geogr. 2010, 34, 215–223. [Google Scholar] [CrossRef]
- Joseph, A.; Bantock, P. Measuring potential physical accessibility to general practitioners in rural areas: A method and case study. Soc. Sci. Med. 1982, 16, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Wang, F. Measurement, optimization, and impact of health care accessibility: A methodological review. Ann. Assoc. Am. Geogr. 2012, 102, 1104–1112. [Google Scholar] [CrossRef] [PubMed]
- Gulliford, M.; Figueroa-Munoz, J.; Morgan, M.; Hughes, D.; Gibson, B.; Beech, R.; Hudson, M. What does’ access to healthcare mean? J. Health Serv. Res. Policy 2002, 7, 186–188. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Luo, W. Assessing spatial and nonspatial factors for healthcare access: Towards an integrated approach to defining health professional shortage areas. Health Place 2005, 11, 131–146. [Google Scholar] [CrossRef] [PubMed]
- Luo, W.; Wang, F. Measures of spatial accessibility to health care in a GIS environment: Synthesis and a case study in the Chicago region. Environ. Plan. B Plan. Des. 2003, 30, 865–884. [Google Scholar] [CrossRef]
- Wang, F.; McLafferty, S.; Escamilla, V.; Luo, L. Late-stage breast cancer diagnosis and health care access in Illinois. Prof. Geogr. 2008, 60, 54–69. [Google Scholar] [CrossRef]
- Field, K. Measuring the need for primary health care: An index of relative disadvantage. Appl. Geogr. 2000, 20, 305–332. [Google Scholar] [CrossRef]
- Comber, A.J.; Brunsdon, C.; Radburn, R. A spatial analysis of variations in health access: Linking geography, socioeconomic status and access perceptions. Int. J. Health Geogr. 2011, 10, 44. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, T.; Lucas, K.; Timms, P. Understanding how low-income communities gain access to healthcare services: A qualitative study in São Paulo, Brazil. J. Transp. Health 2019, 15, 100658. [Google Scholar] [CrossRef]
- Wan, N.; Zhan, F.B.; Zou, B.; Chow, E. A relative spatial access assessment approach for analyzing potential spatial access to colorectal cancer services in Texas. Appl. Geogr. 2012, 32, 291–299. [Google Scholar] [CrossRef]
- Penchansky, R.; Thomas, J.W. The concept of access: Definition and relationship to consumer satisfaction. Med. Care 1981, 19, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Streeter, R.A.; Snyder, J.E.; Kepley, H.; Stahl, A.L.; Li, T.; Washko, M.M. The geographic alignment of primary care Health Professional Shortage Areas with markers for social determinants of health. PLoS ONE 2020, 15, e0231443. [Google Scholar] [CrossRef]
- Tanser, F.; Gijsbertsen, B.; Herbst, K. Modelling and understanding primary health care accessibility and utilization in rural South Africa: An exploration using a geographical information system. Soc. Sci. Med. 2006, 63, 691–705. [Google Scholar] [CrossRef]
- Dai, D. Black residential segregation, disparities in spatial access to health care facilities, and late-stage breast cancer diagnosis in metropolitan Detroit. Health Place 2010, 16, 1038–1052. [Google Scholar] [CrossRef] [PubMed]
- Neutens, T. Accessibility, equity and health care: Review and research directions for transport geographers. J. Transp. Geogr. 2015, 43, 14–27. [Google Scholar] [CrossRef]
- Malpas, J. Putting Space in Place: Philosophical Topography and Relational Geography. Environ. Plan. D Soc. Space 2012, 30, 226–242. [Google Scholar] [CrossRef]
- Simandan, D. The wise stance in human geography. Trans. Inst. Br. Geogr. 2011, 36, 188–192. [Google Scholar] [CrossRef]
- Shah, T.I.; Bell, S.; Wilson, K. Spatial accessibility to health care services: Identifying underserviced neighbourhoods in Canadian urban areas. PLoS ONE 2016, 11, e0168208. [Google Scholar] [CrossRef] [PubMed]
- Luo, W.; Yao, J.; Mitchell, R.; Zhang, X. Spatiotemporal access to emergency medical services in Wuhan, China: Accounting for scene and transport time intervals. Int. J. Health Geogr. 2020, 19, 52. [Google Scholar] [CrossRef] [PubMed]
- Okuyama, K.; Akai, K.; Kijima, T.; Abe, T.; Isomura, M.; Nabika, T. Effect of geographic accessibility to primary care on treatment status of hypertension. PLoS ONE 2019, 14, e0213098. [Google Scholar] [CrossRef] [PubMed]
- Berenbrok, L.A.; Tang, S.; Gabriel, N.; Guo, J.; Sharareh, N.; Patel, N.; Dickson, S.; Hernandez, I. Access to community pharmacies: A nationwide geographic information systems cross-sectional analysis. J. Am. Pharm. Assoc. 2022, 62, 1816–1822. [Google Scholar] [CrossRef] [PubMed]
- Amaral, P.V.; Murray, A.T. Equity in regional access to renal dialysis in Brazil. Reg. Sci. Policy Pract. 2016, 8, 27–44. [Google Scholar] [CrossRef]
- Luo, W.; Yao, J.; Mitchell, R.; Zhang, X.; Li, W. Locating emergency medical services to reduce urban-rural inequalities. Socio-Econ. Plan. Sci. 2022, 84, 101416. [Google Scholar] [CrossRef]
- Ahmed, S.; Adams, A.M.; Islam, R.; Hasan, S.M.; Panciera, R. Impact of traffic variability on geographic accessibility to 24/7 emergency healthcare for the urban poor: A GIS study in Dhaka, Bangladesh. PLoS ONE 2019, 14, e0222488. [Google Scholar] [CrossRef]
- Yip, W.; Fu, H.; Chen, A.T.; Zhai, T.; Jian, W.; Xu, R.; Pan, J.; Hu, M.; Zhou, Z.; Chen, Q.; et al. 10 years of healthcare reform in China: Progress and gaps in universal health coverage. Lancet 2019, 394, 1192–1204. [Google Scholar] [CrossRef]
- Agbenyo, F.; Nunbogu, A.M.; Dongzagla, A. Accessibility mapping of health facilities in rural Ghana. J. Transp. Health 2017, 6, 73–83. [Google Scholar] [CrossRef]
- Songzi Council. Data from the Seventh National Census of Songzi. Available online: http://www.hbsz.gov.cn/content_group/sydd/202106/t20210630_614385.html (accessed on 30 October 2023).
- China National Health Commission. Transcript of the Press Conference of the National Health Commission. Available online: http://www.nhc.gov.cn/xcs/s3574/202307/a6cdc063f8074eadac781e84c9dadc7a.shtml (accessed on 30 October 2023).
- Cheng, J.M.; Zhang, W.M.; Jin, H. Comprehensive safety evaluation of metallurgical crane based on AHP and entropy weight method. IOP Conf. Ser. Mater. Sci. Eng. 2021, 1043, 042050. [Google Scholar] [CrossRef]
- Yao, J.; Zhang, X.; Murray, A.T. Location optimization of urban fire stations: Access and service coverage. Comput. Environ. Urban Syst. 2019, 73, 184–190. [Google Scholar] [CrossRef]
- Zhang, F.; Li, D.; Ahrentzen, S.; Zhang, J. Assessing spatial disparities of accessibility to community-based service resources for Chinese older adults based on travel behavior: A city-wide study of Nanjing, China. Habitat Int. 2019, 88, 101984. [Google Scholar] [CrossRef]
- Shucksmith, M. Young People and Social Exclusion in Rural Areas. Sociol. Rural. 2004, 44, 43–59. [Google Scholar] [CrossRef]
- Walsh, K.C.; Jennings, M.K.; Stoker, L. The Effects of Social Class Identification on Participatory Orientations towards Government. Br. J. Political Sci. 2004, 34, 469–495. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| District | Population Density (People/km2) | Number of Villages | Per Capita Annual Income (RMB yuan) | Number of Hospitals | Number of Clinics |
|---|---|---|---|---|---|
| Xinjiangkou | 1587 | 10 | 8820 | 10 | 83 |
| Shadaoguan | 460 | 6 | 5149 | 0 | 2 |
| Wanshi | 352 | 17 | 4106 | 0 | 3 |
| Babao | 436 | 17 | 5400 | 0 | 14 |
| Laocheng | 368 | 17 | 4892 | 0 | 4 |
| Chendian | 234 | 12 | 3253 | 0 | 5 |
| Nanhai | 316 | 21 | 2896 | 1 | 6 |
| Weishui | 223 | 25 | 4040 | 0 | 13 |
| Liujiachang | 225 | 21 | 6500 | 1 | 20 |
| Jieheshi | 441 | 14 | 3345 | 0 | 10 |
| Wangjiaqiao | 266 | 21 | 3557 | 0 | 5 |
| Sijiachang | 279 | 13 | 3895 | 0 | 1 |
| Wanjia | 358 | 8 | 3085 | 1 | 5 |
| Zhichanghe | 321 | 12 | 2548 | 1 | 8 |
| Yanglinshi | 337 | 13 | 3350 | 0 | 2 |
| Xiejiaping | 133 | 8 | 4800 | 0 | 2 |
| Non-Spatial Factors | Collected Way | Question | Rank | Indicator Character |
|---|---|---|---|---|
| Age | Worldpop Dataset | None | None | - |
| Income | Questionnaire | What is your annual income range? | 1: Above 10 k; 2: 10–30 k; 3: 30–50 k; 4: 50–80 k; 5: 80–150 k; 6: Above 150 k (Unit: RMB) | + |
| Education level | Questionnaire | What is your highest educational degree? | 1: Primary school or Below; 2: Junior high school; 3: Senior high school; 4: Junior College; 5: University degree or Above | + |
| Health Insurance | Questionnaire | Do you have a health insurance? | 1: Yes; 0: No | + |
| Satisfaction level | Questionnaire | How satisfied you are with local medical services | 1: Great dissatisfaction; 2: Dissatisfaction; 3: Not bad; 4: Satisfaction; 5: Great satisfaction | + |
| Indicators | Indicator Character | Weight | Remark | |
|---|---|---|---|---|
| Spatial factors | Accessibility of clinic | Positive | 0.2298 | Clinic’s G-2SFCA scores |
| Accessibility of hospital | Positive | 0.1354 | Hospital’s G-2SFCA scores | |
| Non spatial factors | Age | Negative | 0.0102 | HHNR (children aged 0–5, women aged 15–44, and elderly people aged 65 and above) to the total population |
| household income | Positive | 0.2545 | Per capita annual income of residents | |
| Medical service satisfaction | Positive | 0.0792 | Residents’ satisfaction with medical facilities and services | |
| Healthcare insurance | Positive | 0.0000 | Whether residents have health insurance (1—Yes; 0—No) | |
| Education | Positive | 0.2908 | Education level of residents (1–5 indicates education level from low to high) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, T.; Luo, W.; Tian, L.; Li, J. Integrating Spatial and Non-Spatial Dimensions to Evaluate Access to Rural Primary Healthcare Service: A Case Study of Songzi, China. ISPRS Int. J. Geo-Inf. 2024, 13, 142. https://0-doi-org.brum.beds.ac.uk/10.3390/ijgi13050142
Yang T, Luo W, Tian L, Li J. Integrating Spatial and Non-Spatial Dimensions to Evaluate Access to Rural Primary Healthcare Service: A Case Study of Songzi, China. ISPRS International Journal of Geo-Information. 2024; 13(5):142. https://0-doi-org.brum.beds.ac.uk/10.3390/ijgi13050142
Chicago/Turabian StyleYang, Taohua, Weicong Luo, Lingling Tian, and Jinpeng Li. 2024. "Integrating Spatial and Non-Spatial Dimensions to Evaluate Access to Rural Primary Healthcare Service: A Case Study of Songzi, China" ISPRS International Journal of Geo-Information 13, no. 5: 142. https://0-doi-org.brum.beds.ac.uk/10.3390/ijgi13050142