

Predictability of Cardiovascular Risk Scores for Carotid Atherosclerosis in Community-Dwelling Middle-Aged and Elderly Adults
 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Subjects
2.2. Measurements of Anthropometric and Clinical Characteristics
2.3. Determination of Carotid Atherosclerosis (CA)
2.4. Estimation of 10-Year CVD Risks
2.5. Statistical Analyses
3. Results
3.1. Baseline Clinical Characteristic and Prevalence of CP
3.2. Comparisons between CP-Negative and CP-Positive Subjects
3.3. Association Analyses for the Presence of CP and Advanced CA
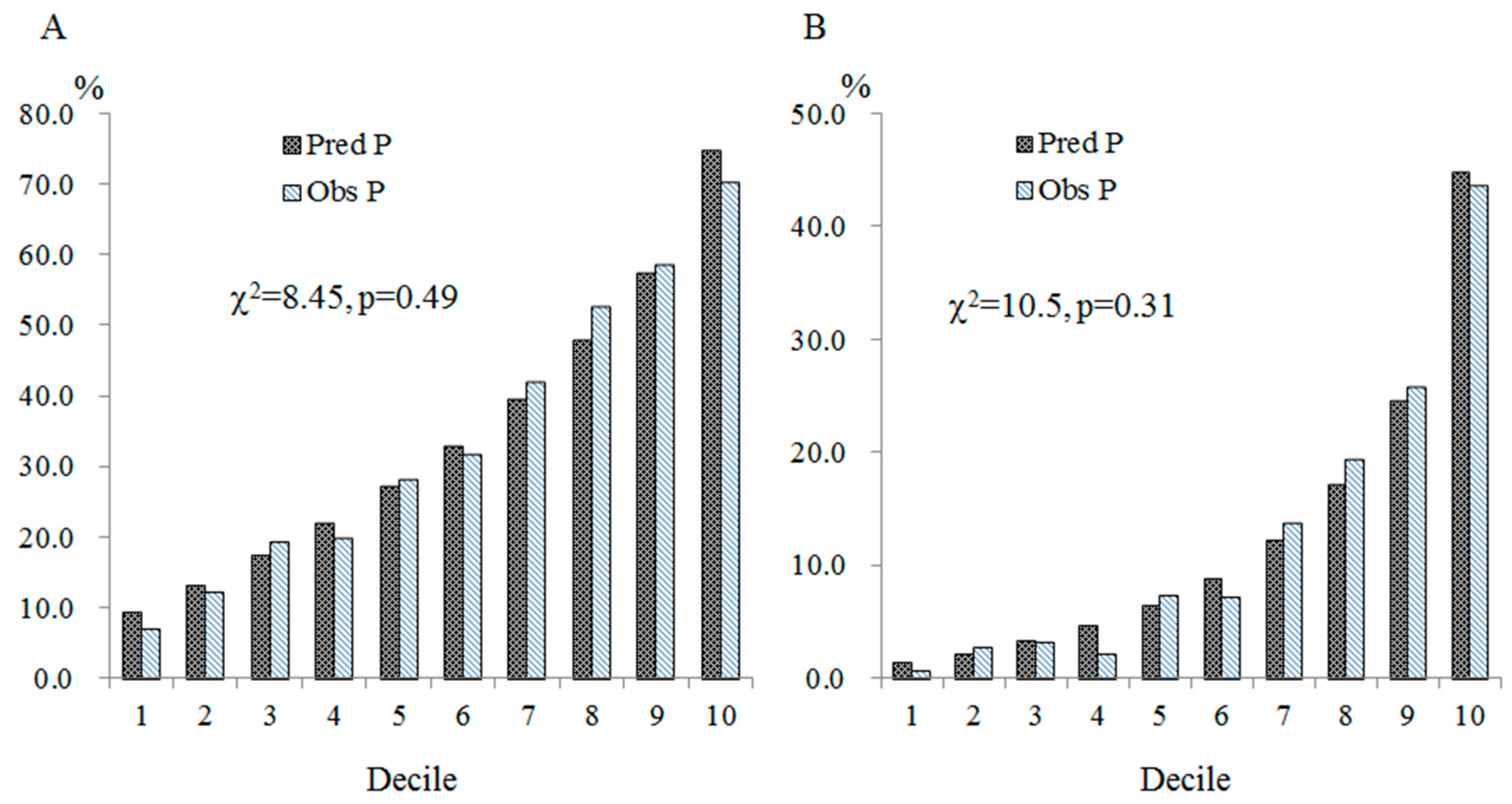
3.4. Calibration of the Prediction Models
3.5. Discrimination Analyses for the Presence of CP
3.6. Discrimination Analyses for the Presence of Advanced CA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- Wilson, P.W.; D’Agostino, R.B.; Levy, D.; Belanger, A.M.; Silbershatz, H.; Kannel, W.B. Prediction of coronary heart disease using risk factor categories. Circulation 1998, 97, 1837–1847. [Google Scholar] [CrossRef] [PubMed]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.J.; Chin, S.L.; Rangarajan, S.; Xavier, D.; Liu, L.; Zhang, H.; Rao-Melacini, P.; Zhang, X.; Pais, P.; Agapay, S.; et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): A case-control study. Lancet 2016, 388, 761–775. [Google Scholar] [CrossRef] [PubMed]
- GBD 2013 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 2287–2323. [Google Scholar] [CrossRef] [PubMed]
- Greenland, P.; Alpert, J.S.; Beller, G.A.; Benjamin, E.J.; Budoff, M.J.; Fayad, Z.A.; Foster, E.; Hlatky, M.A.; Hodgson, J.M.; Kushner, F.G.; et al. 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2010, 56, e50–e103. [Google Scholar] [CrossRef] [PubMed]
- Pennells, L.; Kaptoge, S.; Wood, A.; Sweeting, M.; Zhao, X.; White, I.; Burgess, S.; Willeit, P.; Bolton, T.; Moons, K.G.M.; et al. Equalization of four cardiovascular risk algorithms after systematic recalibration: Individual-participant meta-analysis of 86 prospective studies. Eur. Heart J. 2019, 40, 621–631. [Google Scholar] [CrossRef] [PubMed]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e563–e595. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Bae, J.H.; Moon, M.K.; Oh, S.; Koo, B.K.; Cho, N.H.; Lee, M.K. Validation of risk prediction models for atherosclerotic cardiovascular disease in a prospective Korean community-based cohort. Diabetes Metab. J. 2020, 44, 458–469. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Shen, P.; Zhang, D.; Sun, Y.; Chen, Y.; Liang, J.; Wu, J.; Zhang, J.; Lu, P.; Lin, H.; et al. Evaluation of atherosclerotic cardiovascular risk prediction models in China, results from the CHERRY Study. JACC Asia 2022, 2, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Zhiting, G.; Jiaying, T.; Haiying, H.; Yuping, Z.; Qunfei, Y.; Jingfen, J. Cardiovascular disease risk prediction models in the Chinese population- a systematic review and meta-analysis. BMC Public Health 2022, 22, 1608. [Google Scholar] [CrossRef] [PubMed]
- Negi, S.I.; Nambi, V. The role of carotid intimal thickness and plaque imaging in risk stratification for coronary heart disease. Curr. Atheroscler. Rep. 2012, 14, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Nezu, T.; Hosomi, N. Usefulness of carotid ultrasonography for risk stratification of cerebral and cardiovascular disease. J. Atheroscler. Thromb. 2020, 27, 1023–1035. [Google Scholar] [CrossRef] [PubMed]
- Naqvi, T.Z.; Lee, M.S. Carotid intima-media thickness and plaque in cardiovascular risk assessment. JACC Cardiovasc. Imaging 2014, 7, 1025–1038. [Google Scholar] [CrossRef]
- Polak, J.F.; Pencina, M.J.; Pencina, K.M.; O’Donnell, C.J.; Wolf, P.A.; D’Agostino, R.B., Sr. Carotid-wall intima-media thickness and cardiovascular events. N. Engl. J. Med. 2011, 365, 213–221. [Google Scholar] [CrossRef]
- Gepner, A.D.; Young, R.; Delaney, J.A.; Tattersall, M.C.; Blaha, M.J.; Post, W.S.; Gottesman, R.F.; Kronmal, R.; Budoff, M.J.; Burke, G.L.; et al. Comparison of coronary artery calcium presence, carotid plaque presence, and carotid intima-media thickness for cardiovascular disease prediction in the Multi-Ethnic Study of Atherosclerosis. Circ. Cardiovasc. Imaging 2015, 8, e002262. [Google Scholar] [CrossRef] [PubMed]
- Baber, U.; Mehran, R.; Sartori, S.; Schoos, M.M.; Sillesen, H.; Muntendam, P.; Garcia, M.J.; Gregson, J.; Pocock, S.; Falk, E.; et al. Prevalence, impact, and predictive value of detecting subclinical coronary and carotid atherosclerosis in asymptomatic adults: The BioImage study. J. Am. Coll. Cardiol. 2015, 65, 1065–1074. [Google Scholar] [CrossRef]
- Amato, M.; Veglia, F.; de Faire, U.; Giral, P.; Rauramaa, R.; Smit, A.J.; Kurl, S.; Ravani, A.; Frigerio, B.; Sansaro, D.; et al. Carotid plaque-thickness and common carotid IMT show additive value in cardiovascular risk prediction and reclassification. Atherosclerosis 2017, 263, 412–419. [Google Scholar] [CrossRef]
- Wu, T.W.; Chou, C.L.; Cheng, C.F.; Lu, S.X.; Wang, L.Y. Prevalences of diabetes mellitus and carotid atherosclerosis and their relationships in middle-aged adults and elders: A community-based study. J. Formos. Med. Assoc. 2022, 121, 1133–1140. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.-W.; Chan, H.-L.; Hung, C.-L.; Lu, I.-J.; Wang, S.-D.; Wang, S.-W.; Wu, Y.-J.; Wang, L.-Y.; Yeh, H.-I.; Wei, Y.-H.; et al. Differential patterns of effects of age and sex on metabolic syndrome in Taiwan: Implication for the inadequate internal consistency of the current criteria. Diabetes Res. Clin. Pract. 2014, 105, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.-L.; Wu, Y.-J.; Hung, C.-L.; Liu, C.-C.; Wang, S.-D.; Wu, T.-W.; Wang, L.-Y.; Yeh, H.-I. Segment-specific prevalence of carotid artery plaque and stenosis in middle-aged adults and elders in Taiwan: A community-based study. J. Formos. Med. Assoc. 2019, 118, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.H.; Korcarz, C.E.; Hurst, R.T.; Lonn, E.; Kendall, C.B.; Mohler, E.R.; Najjar, S.S.; Rembold, C.M.; Post, W.S. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: A consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. J. Am. Soc. Echocardiogr. 2008, 21, 93–111. [Google Scholar] [PubMed]
- Touboul, P.J.; Hennerici, M.G.; Meairs, S.; Adams, H.; Amarenco, P.; Bornstein, N.; Csiba, L.; Desvarieux, M.; Ebrahim, S.; Hernandez, R.H.; et al. Mannheim carotid intima-media thickness and plaque consensus (2004–2006–2011). An update on behalf of the advisory board of the 3rd, 4th and 5th watching the risk symposia, at the 13th, 15th and 20th European Stroke Conferences, Mannheim, Germany, 2004, Brussels, Belgium, 2006, and Hamburg, Germany, 2011. Cerebrovasc. Dis. 2012, 34, 290–296. [Google Scholar] [PubMed]
- Rothwell, P.M.; Warlow, C.P. Low risk of ischemic stroke in patients with reduced internal carotid artery lumen diameter distal to severe symptomatic carotid stenosis: Cerebral protection due to low poststenotic flow? On behalf of the European Carotid Surgery Trialists’ Collaborative Group. Stroke 2000, 31, 622–630. [Google Scholar] [PubMed]
- D’Agostino, R.B., Sr.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General cardiovascular risk profile for use in primary care: The Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef]
- Goff, D.C., Jr.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’Agostino, R.B., Sr.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, C.J.; et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63 Pt B, 2935–2959. [Google Scholar] [CrossRef] [PubMed]
- Ahn, H.-R.; Shin, M.-H.; Yun, W.-J.; Kim, H.-Y.; Lee, Y.-H.; Kweon, S.-S.; Rhee, J.-A.; Choi, J.-S.; Choi, S.-W. Comparison of the Framingham Risk Score, UKPDS Risk Engine, and SCORE for predicting carotid atherosclerosis and peripheral arterial disease in Korean type 2 diabetic patients. Korean J. Fam. Med. 2011, 32, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Masson, W.; De Francesca, S.; Molinero, M.; Siniawski, D.; Mulassi, A.; Morales, F.E.; Huerin, M.; Lobo, M.; Molinero, G. Estimation of cardiovascular risk and detection of subclinical carotid atheromatosis in patients with diabetes without a history of cardiovascular disease. Arch. Endocrinol. Metab. 2017, 61, 122–129. [Google Scholar] [CrossRef]
- Mitu, O.; Crisan, A.; Redwood, S.; Cazacu-Davidescu, I.-E.; Mitu, I.; Costache, I.-I.; Onofrei, V.; Miftode, R.-S.; Costache, A.-D.; Haba, C.M.S.; et al. The Relationship between cardiovascular risk scores and several markers of subclinical atherosclerosis in an asymptomatic population. J. Clin. Med. 2021, 10, 955. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Liu, J.; Xie, W.; Qi, Y. Cardiovascular risk assessment: A global perspective. Nat. Rev. Cardiol. 2015, 12, 301–311. [Google Scholar] [CrossRef] [PubMed]
- van der Meer, I.M.; Bots, M.L.; Hofman, A.; del Sol, A.I.; van der Kuip, D.A.; Witteman, J.C. Predictive value of noninvasive measures of atherosclerosis for incident myocardial infarction: The Rotterdam Study. Circulation 2004, 109, 1089–1094. [Google Scholar] [CrossRef] [PubMed]
- Plichart, M.; Celermajer, D.S.; Zureik, M.; Helmer, C.; Jouven, X.; Ritchie, K.; Tzourio, C.; Ducimetière, P.; Empana, J.-P. Carotid intima-media thickness in plaque-free site, carotid plaques and coronary heart disease risk prediction in older adults. The Three-City Study. Atherosclerosis 2011, 219, 917–924. [Google Scholar] [CrossRef] [PubMed]
- Finn, C.; Giambrone, A.E.; Gialdini, G.; Delgado, D.; Baradaran, H.; Kamel, H.; Gupta, A. The association between carotid artery atherosclerosis and silent brain infarction: A systematic review and meta-analysis. J. Stroke Cerebrovasc. Dis. 2017, 26, 1594–1601. [Google Scholar] [CrossRef] [PubMed]
- Polak, J.F.; Szklo, M.; Kronmal, R.A.; Burke, G.L.; Shea, S.; Zavodni, A.E.; O’Leary, D.H. The value of carotid artery plaque and intima-media thickness for incident cardiovascular disease: The multi-ethnic study of atherosclerosis. J. Am. Heart Assoc. 2013, 2, e000087. [Google Scholar] [CrossRef] [PubMed]
- Nambi, V.; Chambless, L.; Folsom, A.R.; He, M.; Hu, Y.; Mosley, T.; Volcik, K.; Boerwinkle, E.; Ballantyne, C.M. Carotid intima-media thickness and presence or absence of plaque improves prediction of coronary heart disease risk: The ARIC (Atherosclerosis Risk in Communities) study. J. Am. Coll. Cardiol. 2010, 55, 1600–1607. [Google Scholar] [CrossRef] [PubMed]
- Gaibazzi, N.; Rigo, F.; Facchetti, R.; Carerj, S.; Giannattasio, C.; Moreo, A.; Mureddu, G.F.; Salvetti, M.; Grolla, E.; Faden, G.; et al. Differential incremental value of ultrasound carotid intima-media thickness, carotid plaque, and cardiac calcium to predict angiographic coronary artery disease across Framingham risk score strata in the APRES multicentre study. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 991–1000. [Google Scholar] [CrossRef]
- Tang, W.; Shen, X.; Li, H.; Bai, Y.; Zhang, B.; Guo, Z.; Wu, H.; Li, P.; Zhao, X. The independent and incremental value of ultrasound carotid plaque length to predict the presence and severity of coronary artery disease: Analysis from the carotid plaque length prospective registry. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 389–396. [Google Scholar] [CrossRef]


{kind=link}
| All (n = 3908) | ||
|---|---|---|
| Mean | (SD) | |
| Age at enrollment (years) | 56.0 | (8.9) |
| BMI (kg/m2) | 24.6 | (3.6) |
| WHR (%) | 88.6 | (7.1) |
| TC (mg/dL) | 204.8 | (38.6) |
| HDL-C (mg/dL) | 55.6 | (15.0) |
| LDL-C (mg/dL) | 121.4 | (32.5) |
| Triglyceride (mg/dL) | 118.5 | (89.8) |
| Glucose (mg/dL) | 97.0 | (25.2) |
| SBP (mm Hg) | 126.5 | (18.7) |
| DBP (mm Hg) | 76.3 | (12.6) |
| PCE (%) | 7.0 | (8.1) |
| FRS (%) | 11.9 | (11.5) |
| n | (%) | |
| Male sex | 1375 | (35.2) |
| Cigarette smoking | 414 | (10.6) |
| Hypertension | 926 | (23.7) |
| DM | 420 | (10.8) |
| Presence of carotid plaque | 1344 | (34.4) |
| Mild carotid atherosclerosis | 847 | (21.7) |
| Advanced carotid atherosclerosis | 497 | (12.7) |
| No CA | Presence of CA | p-Value of Significance Test | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| (A, n = 2564) | All (B, n = 1344) | Mild CA (C, n = 847) | Advanced CA (D, n = 497) | |||||||
| Continuous variable | Mean | (SD) | Mean | (SD) | Mean | (SD) | Mean | (SD) | A vs. B 1 | A, C, & D 2 |
| Age (years) | 53.6 | (8.5) | 60.7 | (7.9) | 59.1 | (7.9) | 63.4 | (7.2) | <0.0001 | <0.0001 |
| BMI (kg/m2) | 24.4 | (3.6) | 24.9 | (3.4) | 24.8 | (3.5) | 25.1 | (3.3) | <0.0001 | 0.0017 |
| WHR (%) | 87.6 | (7.1) | 90.5 | (6.8) | 89.7 | (7.1) | 91.8 | (6.1) | <0.0001 | <0.0001 |
| TC (mg/dL) | 204.1 | (37.6) | 206.2 | (40.3) | 206.3 | (38.5) | 206.0 | (43.2) | 0.11 | 0.44 |
| HDL-C (mg/dL) | 56.6 | (15.2) | 53.9 | (14.4) | 55.0 | (14.7) | 52.0 | (13.8) | <0.0001 | <0.0001 |
| LDL-C (mg/dL) | 119.9 | (31.7) | 124.2 | (33.9) | 123.8 | (32.5) | 124.9 | (36.3) | <0.0001 | 0.0086 |
| TG (mg/dL) | 116.9 | (96.1) | 121.7 | (76.3) | 118.9 | (77.5) | 126.5 | (74.0) | 0.11 | 0.074 |
| Glucose (mg/dL) | 95.0 | (22.3) | 100.9 | (29.5) | 98.1 | (27.1) | 105.5 | (32.7) | <0.0001 | <0.0001 |
| SBP (mm Hg) | 124.2 | (18.4) | 130.8 | (18.4) | 129.7 | (18.4) | 132.7 | (18.3) | <0.0001 | <0.0001 |
| DBP (mm Hg) | 75.7 | (12.7) | 77.6 | (12.3) | 77.3 | (12.1) | 78.2 | (12.7) | <0.0001 | 0.0003 |
| PCE (%) | 4.8 | (6.0) | 11.1 | (9.7) | 8.8 | (8.2) | 15.0 | (10.8) | <0.0001 | <0.0001 |
| FRS (%) | 9.0 | (8.7) | 17.3 | (13.8) | 14.4 | (12.1) | 22.1 | (15.2) | <0.0001 | <0.0001 |
| Categorical variable | n | (%) | n | (%) | n | (%) | n | (%) | ||
| Male sex | 774 | (30.2) | 601 | (44.7) | 337 | (39.8) | 264 | (53.1) | <0.0001 | <0.0001 |
| Cigarette smoking | 238 | (9.3) | 176 | (13.1) | 92 | (10.9) | 84 | (16.9) | 0.0002 | <0.0001 |
| Hypertension | 429 | (16.7) | 497 | (37.0) | 268 | (31.6) | 229 | (46.1) | <0.0001 | <0.0001 |
| DM | 195 | (7.6) | 225 | (16.7) | 108 | (12.8) | 117 | (23.5) | <0.0001 | <0.0001 |
| Model 1 | Model 2 | Model 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Coeff. 1 | OR | (95% CI) | Coeff. 1 | OR | (95% CI) | Coeff. 1 | OR | (95% CI) | |
| Intercept | −7.3995 | 1.00 | −5.5606 | 1.00 | −4.8718 | 1.00 | |||
| Age (per 5.0 years) | 0.4858 | 1.63 *** | (1.55–1.70) | 0.3839 | 1.47 *** | (1.40–1.54) | 0.3304 | 1.39 *** | (1.32–1.47) |
| Sex (M/F) | 0.4596 | 1.58 *** | (1.35–1.86) | - | - | ||||
| Cigarette smoking (Y/N) | 0.5380 | 1.71 *** | (1.33–2.20) | - | - | ||||
| Hypertension (Y/N) | 0.5388 | 1.71 *** | (1.48–1.99) | - | - | ||||
| DM (Y/N) | 0.5029 | 1.65 *** | (1.32–2.07) | - | - | ||||
| LDL-C (per 10.0 mg/dL) | 0.0557 | 1.06 *** | (1.03–1.08) | - | - | ||||
| FRS (per 5.0%) | - | 0.2094 | 1.23 *** | (1.19–1.28) | - | ||||
| PCE (per 5.0%) | - | - | 0.3053 | 1.36 *** | (1.28–1.44) | ||||
| AUROC (95% CI) | 0.7588 | (0.7432–0.7744) | 0.7534 | (0.7376–7692) | 0.7509 | (0.7350–0.7667) | |||
| Model 1 | Model 2 | Model 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Coeff. 1 | OR | (95% CI) | Coeff. 1 | OR | (95% CI) | Coeff. 1 | OR | (95% CI) | |
| Intercept | −10.9722 | 1.00 | −8.4351 | 1.00 | −7.2098 | 1.00 | |||
| Age (per 5.0 years) | 0.6192 | 1.86 *** | (1.72–2.00) | 0.4920 | 1.64 *** | (1.52–1.76) | 0.3927 | 1.48 *** | (1.37–1.61) |
| Sex (M/F) | 0.5913 | 1.81 *** | (1.45–2.26) | - | - | ||||
| Hypertension (Y/N) | 0.6583 | 1.93 *** | (1.55–2.40) | - | - | ||||
| LDL-C (per 10.0 mg/dL) | 0.0799 | 1.08 *** | (1.05–1.12) | - | - | ||||
| DM (Y/N) | 0.7446 | 2.11 *** | (1.61–2.75) | - | - | ||||
| Cigarette smoking (Y/N) | 0.8186 | 2.27 *** | (1.64–3.14) | - | - | ||||
| FRS (per 5.0%) | - | 0.2142 | 1.24 *** | (1.19–1.29) | - | ||||
| PCE (per 5.0%) | - | - | 0.3246 | 1.38 *** | (1.30–1.48) | ||||
| AUROC (95% CI) | 0.8152 | (0.7964–0.8339) | 0.8034 | (0.7836–0.8232) | 0.8010 | (0.7811–0.8209) | |||
| Presence of CP | Presence of Advanced CA | |||
|---|---|---|---|---|
| AUROC | (95% CI) | AUROC | (95% CI) | |
| FRS | 0.7233 1 | (0.7068~0.7398) | 0.7736 4 | (0.7527~0.7945) |
| +Sex | 0.7277 1,2 | (0.7113~0.7442) | 0.7771 4,5 | (0.7564~0.7978) |
| +Age | 0.7533 2 | (0.7375~0.7691) | 0.8034 5 | (0.7835~0.8232) |
| +SMK | 0.7269 1 | (0.7104~0.7434) | 0.7766 4 | (0.7559~0.7974) |
| +DM | 0.7234 1 | (0.7069~0.7399) | 0.7745 4 | (0.7536~0.7954) |
| +HTN | 0.7239 1 | (0.7074~0.7405) | 0.7736 4 | (0.7528~0.7944) |
| +SBP | 0.7267 1,2 | (0.7103~0.7431) | 0.7840 4,5 | (0.7641~0.8039) |
| +CHO | 0.7232 1 | (0.7066~0.7397) | 0.7738 4 | (0.7529~0.7947) |
| +LDL-C | 0.7209 2 | (0.7043~0.7375) | 0.7724 4 | (0.7514~0.7934) |
| +HDL-C | 0.7234 1 | (0.7068~0.7401) | 0.7728 4 | (0.7514~0.7942) |
| +BMI | 0.7259 1 | (0.7094~0.7424) | 0.7758 4 | (0.7549~0.7966) |
| +WHR | 0.7194 1 | (0.7026~0.7362) | 0.7704 4 | (0.7491~0.7916) |
| PCE | 0.7454 1 | (0.7294~0.7614) | 0.8010 | (0.7819~0.8202) |
| +Sex | 0.7476 | (0.7315~0.7636) | 0.8026 | (0.7832~0.8220) |
| +Age | 0.7508 1 | (0.7349~0.7666) | 0.8010 | (0.7811~0.8208) |
| +SMK | 0.7476 | (0.7316~0.7635) | 0.8023 6 | (0.7833~0.8214) |
| +DM | 0.7453 1 | (0.7293~0.7613) | 0.7998 | (0.7805~0.8192) |
| +HTN | 0.7443 1 | (0.7283~0.7603) | 0.7992 | (0.7799~0.8185) |
| +SBP | 0.7435 1,3 | (0.7274~0.7596) | 0.8029 | (0.7837~0.8221) |
| +CHO | 0.7443 1 | (0.7282~0.7603) | 0.8010 | (0.7819~0.8202) |
| +LDL-C | 0.7406 1,3 | (0.7244~0.7568) | 0.7987 | (0.7792~0.8182) |
| +HDL-C | 0.7453 1 | (0.7292~0.7614) | 0.8007 | (0.7813~0.8201) |
| +BMI | 0.7460 1 | (0.7300~0.7620) | 0.8004 | (0.7809~0.8199) |
| +WHR | 0.7380 1,3 | (0.7216~0.7543) | 0.7953 | (0.7754~0.8152) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chou, C.-L.; Liu, C.-C.; Wu, T.-W.; Cheng, C.-F.; Lu, S.-X.; Wu, Y.-J.; Wang, L.-Y. Predictability of Cardiovascular Risk Scores for Carotid Atherosclerosis in Community-Dwelling Middle-Aged and Elderly Adults. J. Clin. Med. 2024, 13, 2563. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092563
Chou C-L, Liu C-C, Wu T-W, Cheng C-F, Lu S-X, Wu Y-J, Wang L-Y. Predictability of Cardiovascular Risk Scores for Carotid Atherosclerosis in Community-Dwelling Middle-Aged and Elderly Adults. Journal of Clinical Medicine. 2024; 13(9):2563. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092563
Chicago/Turabian StyleChou, Chao-Liang, Chun-Chieh Liu, Tzu-Wei Wu, Chun-Fang Cheng, Shu-Xin Lu, Yih-Jer Wu, and Li-Yu Wang. 2024. "Predictability of Cardiovascular Risk Scores for Carotid Atherosclerosis in Community-Dwelling Middle-Aged and Elderly Adults" Journal of Clinical Medicine 13, no. 9: 2563. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092563