
The Impact of Hospital Transfers on Surgical Delay and Associated Postoperative Outcomes for Hip Fracture Patients in Scotland: A Cohort Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting, and Participants
2.2. Data Collection
2.3. Sample Size
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Participants
3.2. Unmatched Study Population
3.2.1. Matched Study Population
3.2.2. Matched Study Population Island Sub-Group
3.3. Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-Transfer (n = 19,049) | Transfer (n = 1141) | Total (n = 20,190) | |
|---|---|---|---|
| Sex, n (%) | |||
| Female | 13,446 (70.6) | 799 (70.0) | 14,245 (70.6) |
| Male | 5603 (29.4) | 342 (30.0) | 5945 (29.4) |
| Missing | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Age, n (%) | |||
| 50 to 54 | 300 (1.6) | 30 (2.6) | 330 (1.6) |
| 55 to 59 | 519 (2.7) | 38 (3.3) | 557 (2.8) |
| 60 to 64 | 752 (4.0) | 54 (4.7) | 806 (4.0) |
| 65 to 69 | 1139 (6.0) | 73 (6.4) | 1212 (6.0) |
| 70 to 74 | 2057 (10.8) | 128 (11.2) | 2185 (10.8) |
| 75 to 79 | 2779 (14.6) | 198 (17.4) | 2977 (14.7) |
| 80 to 84 | 3947 (20.7) | 228 (20.0) | 4175 (20.7) |
| 85 to 89 | 4207 (22.1) | 221 (19.4) | 4428 (21.9) |
| 90 to 94 | 2525 (13.3) | 125 (11.0) | 2650 (13.1) |
| 95+ | 824 (4.3) | 46 (4.0) | 870 (4.3) |
| Missing | 0 (0.0) | (0.0) | 0 (0.0) |
| SIMD, n (%) | |||
| 1 | 1842 (9.7) | 66 (5.8) | 1908 (9.5) |
| 2 | 1962 (10.3) | 103 (9.0) | 2065 (10.2) |
| 3 | 1995 (10.5) | 115 (10.1) | 2110 (10.5) |
| 4 | 1822 (9.6) | 109 (9.6) | 1931 (9.6) |
| 5 | 1894 (9.9) | 176 (15.4) | 2070 (10.3) |
| 6 | 1839 (9.7) | 173 (15.2) | 2012 (10.0) |
| 7 | 1803 (9.5) | 124 (10.9) | 1927 (9.5) |
| 8 | 1692 (8.9) | 93 (8.2) | 1785 (8.8) |
| 9 | 1831 (9.6) | 88 (7.7) | 1919 (9.5) |
| 10 | 1724 (9.1) | 47 (4.1) | 1771 (8.8) |
| Missing | 645 (3.4) | 47 (4.1) | 692 (3.4) |
| Residence prior to admission, n (%) | |||
| Home | 15,317 (80.4) | 962 (84.3) | 16,279 (80.6) |
| Not home | 3663 (19.2) | 166 (14.5) | 3829 (19.0) |
| Missing | 69 (0.4) | 13 (1.1) | 82 (0.4) |
| 4AT, n (%) | |||
| Delirium unlikely | 7453 (39.1) | 574 (50.3) | 8027 (39.8) |
| Possible Cognitive impairment | 3823 (20.1) | 214 (18.8) | 4037 (20.0) |
| Possible delirium | 3520 (18.5) | 185 (16.2) | 3705 (18.4) |
| Missing | 4253 (22.3) | 168 (14.7) | 4421 (21.9) |
| ASA, n (%) | |||
| 1 | 296 (1.6) | 33 (2.9) | 329 (1.6) |
| 2 | 3653 (19.1) | 302 (26.5) | 3955 (19.6) |
| 3 | 9229 (48.5) | 597 (52.3) | 9826 (48.7) |
| 4 and 5 | 2301 (12.1) | 188 (16.5) | 2489 (12.3) |
| Missing | 3570 (18.7) | 21 (1.8) | 3591 (17.8) |
| Operation type, n (%) | |||
| Fixation | 8599 (45.1) | 437 (38.3) | 9036 (44.8) |
| Hemi arthroplasty | 9139 (48.0) | 606 (53.1) | 9745 (48.3) |
| THR | 1244 (6.5) | 96 (8.4) | 1340 (6.6) |
| Missing | 67 (0.4) | 2 (0.2) | 69 (0.3) |
References
- Public Health Scotland. Scottish Hip Fracture Audit Annual Report 2021. 2021. Available online: https://www.shfa.scot.nhs.uk/Reports/index.html (accessed on 1 July 2023).
- Horriat, S.; Hamilton, P.D.; Sott, A.H. Financial aspects of arthroplasty options for intra-capsular neck of femur fractures: A cost analysis study to review the financial impacts of implementing NICE guidelines in the NHS organisations. Injury 2015, 46, 363–365. [Google Scholar] [CrossRef] [PubMed]
- Scottish Government. A Scotland for the Future: Opportunities and Challenges of Scotland’s Changing Population. 2021. Available online: https://www.gov.scot/publications/scotland-future-opportunities-challenges-scotlands-changing-population (accessed on 1 July 2023).
- Christensen, K.; Doblhammer, G.; Rau, R.; Vaupel, J.W. Ageing populations: The challenges ahead. Lancet 2009, 374, 1196–1208. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Physicians. National Hip Fracture Database (NHFD) Annual Report 2019. 2019. Available online: https://www.nhfd.co.uk/files/2019ReportFiles/NHFD_2019_Annual_Report_v101.pdf (accessed on 1 July 2023).
- Sim, A.J.; Grant, F.; Ingram, A.K. Surgery in Remote and Rural Scotland. Surg. Clin. N. Am. 2009, 89, 1335–1347. [Google Scholar] [CrossRef] [PubMed]
- Scottish Government. Scottish Standards of Care for Hip Fracture Patients. 2020. Available online: https://www.shfa.scot.nhs.uk/_docs/2020/Scottish-standards-of-care-for-hip-fracture-patients-2020.pdf (accessed on 1 July 2023).
- Farrow, L.; Hall, A.; Wood, A.; Smith, R.; James, K.; Holt, G.; Hutchison, J.; Myint, P.K. Quality of Care in Hip Fracture Patients: The Relationship Between Adherence to National Standards and Improved Outcomes. J. Bone Jt. Surg. 2018, 100, 751–757. [Google Scholar] [CrossRef] [PubMed]
- Moja, L.; Piatti, A.; Pecoraro, V.; Ricci, C.; Virgili, G.; Salanti, G.; Germagnoli, L.; Liberati, A.; Banfi, G. Timing Matters in Hip Fracture Surgery: Patients Operated within 48 Hours Have Better Outcomes. A Meta-Analysis and Meta-Regression of over 190,000 Patients. PLoS ONE 2012, 7, e46175. [Google Scholar] [CrossRef] [PubMed]
- Klestil, T.; Röder, C.; Stotter, C.; Winkler, B.; Nehrer, S.; Luts, M.; Klerings, I.; Wagner, G.; Gartlehner, G.; Nussbaumer-Streit, B. Impact of timing of surgery in elderly hip fracture patients: A systematic review and meta-analysis. Sci. Rep. 2018, 8, 13933. [Google Scholar] [CrossRef]
- A Harvey, L.; A Harris, I.; Mitchell, R.J.; Webster, A.; Cameron, I.D.; Jorm, L.R.; Seymour, H.; Sarrami, P.; Close, J.C. Impact of pre-surgery hospital transfer on time to surgery and 30-day mortality for people with hip fractures. Med. J. Aust. 2021, 215, 87–88. [Google Scholar] [CrossRef]
- Hughes, A.; Brent, L.; Biesma, R.; Kenny, P.J.; Hurson, C.J. The effect of indirect admission via hospital transfer on hip fracture patients in Ireland. Ir. J. Med. Sci. 2019, 188, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Desai, S.J.; Patel, J.; Abdo, H.; Lawendy, A.-R.; Sanders, D. A comparison of surgical delays in directly admitted versus transferred patients with hip fractures: Opportunities for improvement? Can. J. Surg. 2014, 57, 40–43. [Google Scholar] [CrossRef]
- Walsh, M.E.; Blake, C.; Walsh, C.D.; Brent, L.; Sorensen, J. Patient and hospital-level factors associated with time to surgery after hip fracture in Ireland: Analysis of national audit data 2016–2020. Injury 2023, 54, 1733–1739. [Google Scholar] [CrossRef]
- Zeltzer, J.; Mitchell, R.J.; Toson, B.; Harris, I.A.; Close, J. Determinants of time to surgery for patients with hip fracture. ANZ J. Surg. 2014, 84, 633–638. [Google Scholar] [CrossRef] [PubMed]
- A Marley, M.; Lambers, A.; Marley, I.; Welthy, L.; Seymour, H. The Tyranny of Distance: How Hospital Transfer Affects Time to Surgery for Hip Fracture Patients. Cureus 2022, 14, e22662. [Google Scholar] [CrossRef] [PubMed]
- Public Health Scotland. The Scottish Hip Fracture Audit. 2022. Available online: https://www.shfa.scot.nhs.uk/About/index.html (accessed on 1 July 2023).
- Scottish Government. Scottish Index of Multiple Deprivation 2020. 2020. Available online: https://www.gov.scot/collections/scottish-index-of-multiple-deprivation-2020/ (accessed on 1 July 2023).
- Public Health Scotland. Scottish Hip Fracture Audit Guidelines Definitions April 2021. 2021. Available online: https://www.shfa.scot.nhs.uk/_docs/2021/Scottish-Hip-Fracture-Audit-Guidelines-Definitions-April-2021-PHS.pdf (accessed on 1 July 2023).
- No Author Listed. 4AT Assessment Test for Delirium & Cognitive Impairment. 2011. Available online: https://www.the4at.com/ (accessed on 1 July 2023).
- Stuart, E.A. Matching methods for causal inference: A review and a look forward. Stat. Sci. 2010, 25, 1–21. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Crook, M.A. The Caldicott report and patient confidentiality. J. Clin. Pathol. 2003, 56, 426–428. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.G.; Quach, P.; von Elm, E.; Guttmann, A.; Moher, D.; Petersen, I.; Sørensen, H.T.; Smeeth, L.; Langan, S.M.; Benchimol, E.I. The Reporting of Studies Conducted Using Observational Routinely-Collected Health Data (RECORD) Statement: Methods for Arriving at Consensus and Developing Reporting Guidelines. PLoS ONE 2015, 10, e0125620. [Google Scholar] [CrossRef] [PubMed]
- Tucker, A.; Donnelly, K.J.; McDonald, S.; Craig, J.; Foster, A.P.; Acton, J.D. The changing face of fractures of the hip in Northern Ireland. Bone Jt. J. 2017, 99-B, 1223–1231. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, J.E.; Fountain, D.M.; Cundall-Curry, D.J.; Carrothers, A.D. Do Patients Taking Warfarin Experience Delays to Theatre, Longer Hospital Stay, and Poorer Survival After Hip Fracture? Clin. Orthop. Relat. Res. 2016, 475, 273–279. [Google Scholar] [CrossRef]
- Simunovic, N.; Devereaux, P.J.; Bhandari, M. Surgery for hip fractures: Does surgical delay affect outcomes? Indian J. Orthop. 2011, 45, 27–32. [Google Scholar] [CrossRef]
- Blink, O. Hip fracture clearance: How much optimisation is necessary? Injury 2020, 51, S111–S117. [Google Scholar] [CrossRef]
- Griffiths, R.; Babu, S.; Dixon, P.; Freeman, N.; Hurford, D.; Kelleher, E.; Moppett, I.; Ray, D.; Sahota, O.; Shields, M.; et al. Guideline for the management of hip fractures 2020. Anaesthesia 2020, 76, 225–237. [Google Scholar] [CrossRef]
- Sheehan, K.J.; Sobolev, B.; Villian, Y.F.; Guy, F. Patient and system factors of time to surgery after hip fracture: A scoping review. BMJ Open 2017, 7, e016939. [Google Scholar] [CrossRef] [PubMed]
- Simuniovic, N.; Devereaux, P.J.; Sprague, S.; Guyatt, G.H.; Schemitsch, E.; DeBeer, J.; Bhandari, M. Effect of early surgery after hip fracture on mortality and complications: Systematic review and meta-analysis. Can. Med. Assoc. J. 2010, 182, 1609–1616. [Google Scholar] [CrossRef]
- Chen, C.-L.; Chen, C.-M.; Wang, C.-Y.; Ko, P.-W.; Chen, C.-H.; Hsieh, C.-P.; Chiu, H.-C. Frailty is Associated with an Increased Risk of Major Adverse Outcomes in Elderly Patients Following Surgical Treatment of Hip Fracture. Sci. Rep. 2019, 9, e19135. [Google Scholar] [CrossRef] [PubMed]
- Dayama, A.; Olorunfemi, O.; Greenbaum, S.; Stone, M.E.; McNelis, J. Impact of frailty on outcomes in geriatric femoral neck fracture management: An analysis of national surgical quality improvement program dataset. Surgery 2016, 28, 185–190. [Google Scholar] [CrossRef]
- Makary, M.A.; Segev, D.L.; Pronovost, P.J.; Syin, D.; Bandeen-Roche, K.; Patel, P.; Takenaga, R.; Devgan, L.; Holzmueller, C.G.; Tian, J.; et al. Frailty as a Predictor of Surgical Outcomes in Older Patients. J. Am. Coll. Surg. 2010, 210, 901–908. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.; Jiang, C.; Shen, J.; Tang, P.; Wang, Y. Preoperative predictors for mortality following hip fracture surgery: A systematic review and meta-analysis. Injury 2012, 43, 676–685. [Google Scholar] [CrossRef] [PubMed]
- Scottish Government. Rural Scotland Key Facts 2021. 2021. Available online: https://www.gov.scot/publications/rural-scotland-key-facts-2021/ (accessed on 1 July 2023).
- Teckle, P.; Hannaford, P.; Sutton, M. Is the health of people living in rural areas different from those in cities? Evidence from routine data linked with the Scottish Health Survey. BMC Health Serv. Res. 2012, 12, 43. [Google Scholar] [CrossRef]
- Ricci, W.M.; Brandt, A.M.; McAndrew, C.; Gardner, M.J. Factors affecting delay to surgery and length of stay for patients with hip fracture. J. Orthop. Trauma 2015, 29, e109–e114. [Google Scholar] [CrossRef] [PubMed]
- Lefaivre, K.A.; Macadam, S.A.; Davidson, D.J.; Gandhi, R.; Chan, H.; Broekhuyse, H.M.; Fu, M.C.; Boddapati, V.; Gausden, E.B.; Samuel, A.M.; et al. Length of stay, mortality, morbidity and delay to surgery in hip fractures. J. Bone Jt. Surg. 2009, 91, 922–927. [Google Scholar] [CrossRef]
- Murphy, J.R.; Loh, J.; Smith, N.C.; Stone, N.C. Association of length of hospital stay with delay to surgical fixation of hip fracture. Can. J. Surg. 2022, 65, E188–E192. [Google Scholar] [CrossRef] [PubMed]
- Guest, J.F.; Keating, T.; Gould, D.; Wigglesworth, N. Modelling the annual NHS costs and outcomes attributable to healthcare-associated infections in England. BMJ Open 2020, 10, e033367. [Google Scholar] [CrossRef]
- Rojas-Garcia, A.; Turner, S.; Pizzo, E.; Hudson, E.; Thomas, J.; Raine, R. Impact and experiences of delayed discharge: A mixed-studies systematic review. Health Expect. 2018, 21, 41–56. [Google Scholar] [CrossRef]
- Dong, Y.; Peng, C.J. Principled missing data methods for researchers. SpringerPlus 2013, 2, 222. [Google Scholar] [CrossRef]
- Lee, J.H.; Huber, J.C. Evaluation of Multiple Imputation with Large Proportions of Missing Data: How Much Is Too Much? Iran. J. Public Health 2021, 50, 1372–1380. [Google Scholar] [CrossRef] [PubMed]
- Baser, O. Choosing propensity score matching over regression adjustment for causal inference: When, why and how it makes sense. J. Med. Econ. 2007, 10, 379–391. [Google Scholar] [CrossRef]
- Amoah, J.; Stuart, E.A.; Cosgrove, S.E.; Harris, A.D.; Han, J.H.; Lautenbach, E.; Tamma, P.D. Comparing Propensity Score Methods Versus Traditional Regression Analysis for the Evaluation of Observational Data: A Case Study Evaluating the Treatment of Gram-Negative Bloodstream Infections. Clin. Infect. Dis. 2020, 71, e497–e505. [Google Scholar] [CrossRef] [PubMed]
- Sankar, A.; Johnson, S.R.; Beattie, W.S.; Tait, G.; Wijeysundera, D.N. Reliability of the American Society of Anesthesiologists physical status scale in clinical practice. Br. J. Anaesth. 2014, 113, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Middleton, M. Orthogeriatrics and Hip Fracture Care in the UK: Factors Driving Change to More Integrated Models of Care. Geriatrics 2018, 3, 55. [Google Scholar] [CrossRef]
- Middleton, M.; Wan, B.; da Assunçāo, R. Improving hip fracture outcomes with integrated orthogeriatric care: A comparison between two accepted orthogeriatric models. Age Ageing 2016, 46, 465–470. [Google Scholar] [CrossRef]
- Van Heghe, A.; Mordant, G.; Dupont, J.; Dejaeger, M.; Laurent, M.R.; Gielen, E. Effects of Orthogeriatric Care Models on Outcomes of Hip Fracture Patients: A Systematic Review and Meta-Analysis. Calcif. Tissue Int. 2021, 110, 162–184. [Google Scholar] [CrossRef] [PubMed]




| Unmatched | Matched | |||||||
|---|---|---|---|---|---|---|---|---|
| Non-Transfer (n = 19,049) | Transfer (n = 1141) | Std Diff, % | p-Value | Non- Transfer (n = 1141) | Transfer (n = 1141) | Std Diff, % | p-Value | |
| Sex, n (%) | ||||||||
| Female | 13,446 (70.6) | 799 (70.0) | −1.2 | 0.712 a | 805 (70.6) | 799 (70.0) | −1.2 | 0.819 a |
| Male | 5603 (29.4) | 342 (30.0) | 1.2 | 336 (29.4) | 342 (30.0) | 1.2 | ||
| Age, n (%) | ||||||||
| 50 to 54 | 300 (1.6) | 30 (2.6) | 6.6 | 0.003 b | 28 (2.5) | 30 (2.6) | 1.1 | 0.999 b |
| 55 to 59 | 519 (2.7) | 38 (3.3) | 3.4 | 38 (3.3) | 38 (3.3) | 0.0 | ||
| 60 to 64 | 752 (4.0) | 54 (4.7) | 3.7 | 46 (4.0) | 54 (4.7) | 3.3 | ||
| 65 to 69 | 1139 (6.0) | 73 (6.4) | 1.7 | 77 (6.7) | 73 (6.4) | −1.4 | ||
| 70 to 74 | 2057 (10.8) | 128 (11.2) | 1.3 | 129 (11.3) | 128 (11.2) | −0.3 | ||
| 75 to 79 | 2779 (14.6) | 198 (17.4) | 7.3 | 198 (17.4) | 198 (17.4) | 0.0 | ||
| 80 to 84 | 3947 (20.7) | 228 (20.0) | −1.9 | 223 (19.5) | 228 (20.0) | 1.1 | ||
| 85 to 89 | 4207 (22.1) | 221 (19.4) | −6.9 | 230 (20.2) | 221 (19.4) | −2.0 | ||
| 90 to 94 | 2525 (13.3) | 125 (11.0) | −7.4 | 126 (11.0) | 125 (11.0) | −0.3 | ||
| 95+ | 824 (4.3) | 46 (4.0) | −1.5 | 46 (4.0) | 46 (4.0) | 0.0 | ||
| SIMD, n (%) | ||||||||
| 1 | 1897 (10.0) | 72 (6.3) | −15.0 | <0.001 b | 79 (6.9) | 72 (6.3) | −2.5 | 1.000 b |
| 2 | 2024 (10.6) | 105 (9.2) | −4.9 | 109 (9.6) | 105 (9.2) | −1.2 | ||
| 3 | 2058 (10.8) | 118 (10.3) | −1.5 | 114 (10.0) | 113 (9.9) | 1.2 | ||
| 4 | 1883 (9.9) | 113 (9.9) | 0.1 | 114 (10.0) | 113 (9.9) | −0.3 | ||
| 5 | 1954 (10.3) | 185 (16.2) | 16.2 | 189 (16.6) | 185 (16.2) | −1.0 | ||
| 6 | 1914 (10.0) | 177 (15.5) | 15.1 | 178 (15.6) | 177 (15.5) | −0.2 | ||
| 7 | 1883 (9.9) | 127 (11.1) | 4.0 | 120 (10.5) | 127 (11.1) | 2.0 | ||
| 8 | 1760 (9.2) | 97 (8.5) | −2.7 | 95 (8.3) | 97 (8.5) | 0.6 | ||
| 9 | 1893 (9.9) | 95 (8.3) | −5.8 | 91 (8.0) | 95 (8.3) | 1.3 | ||
| 10 | 1783 (9.4) | 52 (4.6) | −23.0 | 52 (4.6) | 52 (4.6) | 0.0 | ||
| Residence prior to admission, n (%) | ||||||||
| Home | 15,372 (80.7) | 970 (85.0) | 12.1 | <0.001 a | 982 (86.1) | 970 (85.0) | −3.0 | 0.513 a |
| Not home | 3677 (19.3) | 171 (15.0) | −12.1 | 159 (13.9) | 171 (15.0) | 3.0 | ||
| 4AT, n (%) | ||||||||
| Delirium unlikely | 9625 (50.5) | 669 (58.6) | 16.5 | <0.001 b | 678 (59.4) | 669 (58.6) | −1.6 | 0.928 b |
| Possible cognitive impairment | 4947 (26.0) | 256 (22.4) | −8.5 | 252 (22.1) | 256 (22.4) | 0.8 | ||
| Possible delirium | 4477 (23.5) | 216 (18.9) | −11.7 | 211 (18.5) | 216 (18.9) | 1.1 | ||
| ASA, n (%) | ||||||||
| 1 | 360 (1.9) | 34 (3) | 6.4 | <0.001 b | 37 (3.2) | 34 (3.0) | −1.5 | 0.902 b |
| 2 | 4462 (23.4) | 309 (27.1) | 8.2 | 320 (28.1) | 309 (27.1) | −2.2 | ||
| 3 | 11,357 (59.6) | 608 (53.3) | −12.7 | 607 (53.2) | 608 (53.3) | 0.2 | ||
| 4 and 5 | 2870 (15.1) | 188 (16.5) | 4.0 | 177 (15.5) | 190 (16.7) | 2.8 | ||
| Operation type, n (%) | ||||||||
| Fixation | 8631 (45.3) | 439 (38.5) | −14.1 | <0.001 b | 432 (37.9) | 439 (38.5) | 1.3 | 0.945 b |
| Hemi arthroplasty | 9170 (48.1) | 606 (53.1) | 10.0 | 614 (53.8) | 606 (53.1) | −1.4 | ||
| THR | 1248 (6.6) | 96 (8.4) | 6.7 | 95 (8.3) | 96 (8.4) | 0.3 | ||
| Non-Transfer (n = 19,049) | Transfer (n = 1141) | OR (95% CI) | p-Value | |
|---|---|---|---|---|
| Surgery within 36 h, n (%) | 14 320 (75.6) | 711 (63.6) | 0.56 (0.50 to 0.64) | <0.001 a |
| Time to surgery (hours), median (IQR) | 21.2 (15.3 to 35.7) | 30.1 (18.2 to 41.1) | - | <0.001 b |
| 30-day mortality, n (%) | 1270 (6.7) | 56 (5.2) | 0.72 (0.54 to 0.94) | 0.022 a |
| 60-day mortality, n (%) | 2079 (11.0) | 90 (9.1) | 0.71 (0.57 to 0.88) | 0.003 a |
| Return to residence, n (%) | 11 459 (60.2) | 727 (63.7) | 1.16 (1.03 to 1.32) | 0.017 a |
| Postoperative mobilisation, n (%) | 13 450 (70.6) | 859 (75.3) | 1.27 (1.11 to 1.46) | <0.001 a |
| Acute LOS (days), median (IQR) | 9 (6 to 14) | 9 (6 to 14.5) | - | 0.553 b |
| Total LOS (days), median (IQR) | 16 (8 to 35) | 16 (8 to 33) | - | 0.706 b |
| Non-Transfer (n = 1141) | Transfer (n = 1141) | OR (95% CI) | p-Value | |
|---|---|---|---|---|
| Surgery within 36 h, n (%) | 852 (75.3) | 711 (63.6) | 0.57 (0.48 to 0.69) | <0.001 a |
| Time to surgery (hours), median (IQR) | 20.3 (14.5 to 35.9) | 30.1 (18.2 to 41.1) | - | <0.001 b |
| 30-day mortality, n (%) | 60 (5.3) | 56 (4.9) | 0.93 (0.64 to 1.36) | 0.714 a |
| 60-day mortality, n (%) | 106 (9.4) | 90 (8.1) | 0.85 (0.63 to 1.14) | 0.284 a |
| Return to residence, n (%) | 751 (65.8) | 727 (63.7) | 0.91 (0.77 to 1.08) | 0.293 a |
| Postoperative mobilisation, n (%) | 852 (74.7) | 859 (75.3) | 1.03 (0.85 to 1.25) | 0.735 a |
| Acute LOS (days), median (IQR) | 9 (6 to 13) | 9 (6 to 14.5) | - | 0.064 b |
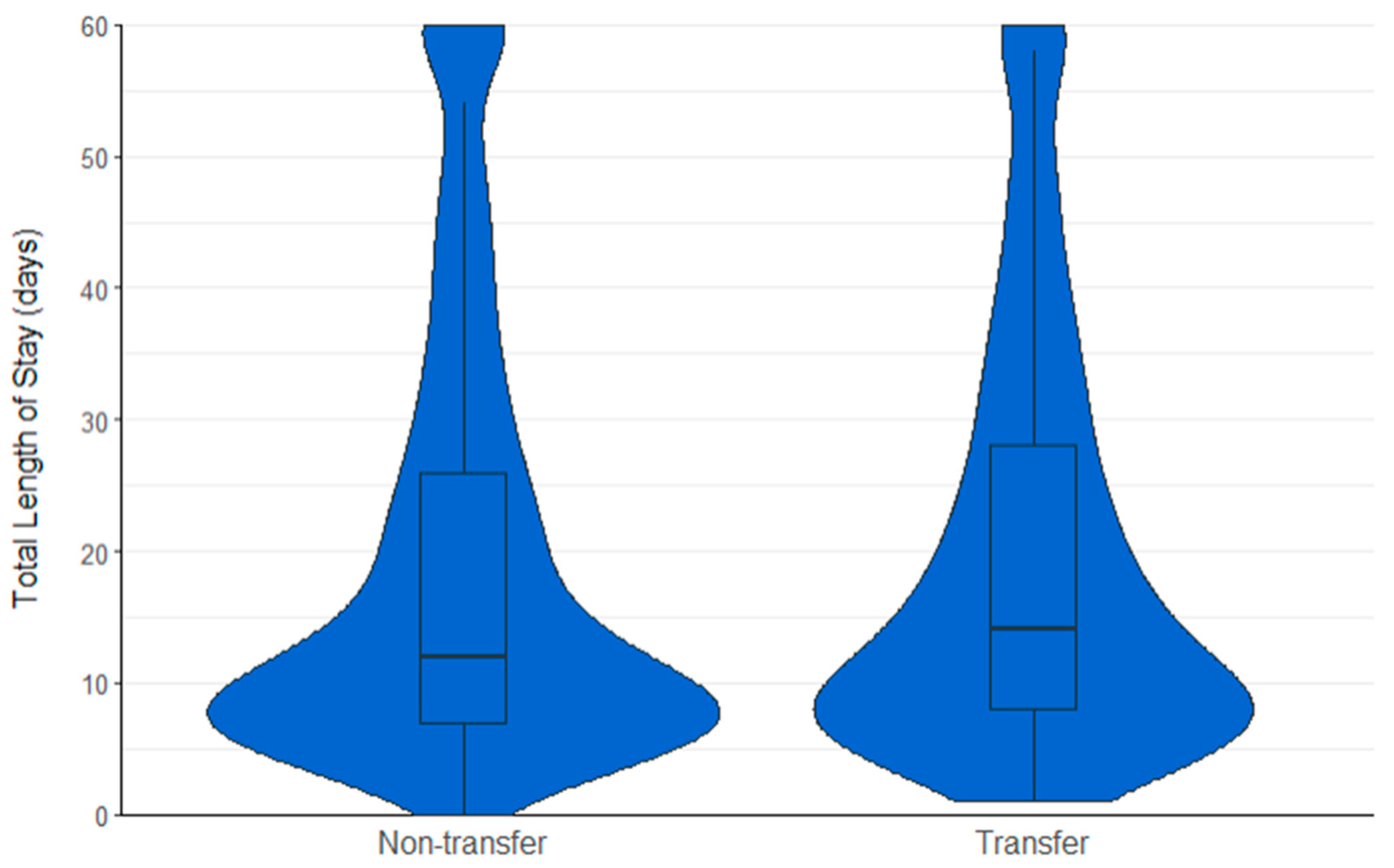
| Total LOS (days), median (IQR) | 13 (8 to 30) | 16 (8 to 33) | - | 0.024 b |
| Non-Transfer (n = 1141) | Transfer (Mainland) (n = 999) | Transfer (Island) (n = 142) | OR (95% CI) | p-Value | |
|---|---|---|---|---|---|
| Surgery within 36 h, n (%) | 852 (75.3) | 655 (66.8) | 56 (40.6) | Mainland = 0.42 (0.23 to 0.74) Island = 0.22 (0.16 to 0.32) | Mainland <0.001 a Island <0.001 a |
| Time to surgery (hours), median (IQR) | 20.3 (14.5 to 35.9) | 28.1 (17.5 to 39.9) | 39.7 (29.0 to 58.5) | Mainland = 5.6 (3.2 to 8.0) Island = 21.2 (16.1 to 26.2) | Mainland <0.001 b Island <0.001 b |
| 30-day mortality, n (%) | 60 (5.3) | 52 (5.2) | 4 (2.9) | Mainland = 0.99 (0.68 to 1.45) Island = 0.52 (0.16 to 1.30) | Mainland = 0.967 a Island = 0.217 a |
| 60-day mortality, n (%) | 106 (9.4) | 80 (9.8) | 10 (8.1) | Mainland = 0.86 (0.64 to 1.17) Island = 0.76 (0.36 to 1.41) | Mainland = 0.351 a Island = 0.415 a |
| Return to residence, n (%) | 751 (65.8) | 640 (64.1) | 87 (61.3) | Mainland = 0.93 (0.77 to 1.11) Island = 0.82 (0.58 to 1.18) | Mainland = 0.396 a Island = 0.283 a |
| Postoperative mobilisation, n (%) | 852 (74.7) | 744 (74.5) | 115 (81.0) | Mainland = 0.99 (0.81 to 1.20) Island = 1.44 (0.94 to 2.28) | Mainland = 0.917 a Island = 0.101 a |
| Acute LOS, median (IQR) | 9 (6 to 13) | 9 (6 to 14) | 10 (8 to 16) | - | Mainland = 0.330 vs. non-transfer; 0.005 vs. island Island < 0.001 vs. non-transfer; 0.005 against mainland |
| Total LOS, median (IQR) | 13 (8 to 30) | 15 (8 to 32) | 23 (12 to 17) | - | Mainland = 0.271 vs. non-transfer, <0.001 against island. Island <0.001 against non-transfer; <0.001 against mainland |
| Non-Transfer (n = 137) | Transfer (n = 137) | OR (95% CI) | p-Value | |
|---|---|---|---|---|
| Surgery within 36 h, n (%) | 114 (83.2) | 92 (67.6) | 0.42 (0.23 to 0.74) | 0.003 a |
| Time to surgery (hours), median (IQR) | 19.4 (14.2 to 28.8) | 26.4 (17.5 to 38.2) | - | <0.001 b |
| 30-day mortality, n (%) | 14 (10.2) | 21 (15.3) | 1.59 (0.78 to 3.34) | 0.208 a |
| 60-day mortality, n (%) | 29 (21.2) | 32 (23.4) | 1.14 (0.65 to 2.03) | 0.640 a |
| Return to residence, n (%) | 103 (75.2) | 95 (69.3) | 0.74 (0.44 to 1.27) | 0.821 a |
| Postoperative mobilisation, n (%) | 79 (57.7) | 71 (51.8) | 0.78 (0.49 to 1.27) | 0.332 a |
| Acute LOS, median (IQR) | 8 (6 to 11) | 7 (5 to 10.3) | - | 0.091 b |
| Total LOS, median (IQR) | 9 (6 to 14) | 8 (5 to 17) | - | 0.286 b |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lennox, L.; Myint, P.K.; Baliga, S.; Farrow, L. The Impact of Hospital Transfers on Surgical Delay and Associated Postoperative Outcomes for Hip Fracture Patients in Scotland: A Cohort Study. J. Clin. Med. 2024, 13, 2546. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092546
Lennox L, Myint PK, Baliga S, Farrow L. The Impact of Hospital Transfers on Surgical Delay and Associated Postoperative Outcomes for Hip Fracture Patients in Scotland: A Cohort Study. Journal of Clinical Medicine. 2024; 13(9):2546. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092546
Chicago/Turabian StyleLennox, Liam, Phyo K. Myint, Santosh Baliga, and Luke Farrow. 2024. "The Impact of Hospital Transfers on Surgical Delay and Associated Postoperative Outcomes for Hip Fracture Patients in Scotland: A Cohort Study" Journal of Clinical Medicine 13, no. 9: 2546. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092546