


Switching from Intravenous to Subcutaneous Biological Therapy for Inflammatory Bowel Disease Patients Remains a Challenge
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Questionnaire
2.3. Ethical Considerations
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics of the Patients
3.2. The Preferred Routes of Medication Delivery among the Entire Study Population
3.3. Comparing Preferences between IV Treatment Every 8 Weeks and SC Every 2 Weeks
3.4. Preferred Routes of Medication Delivery According to the Patients’ Prior Experience
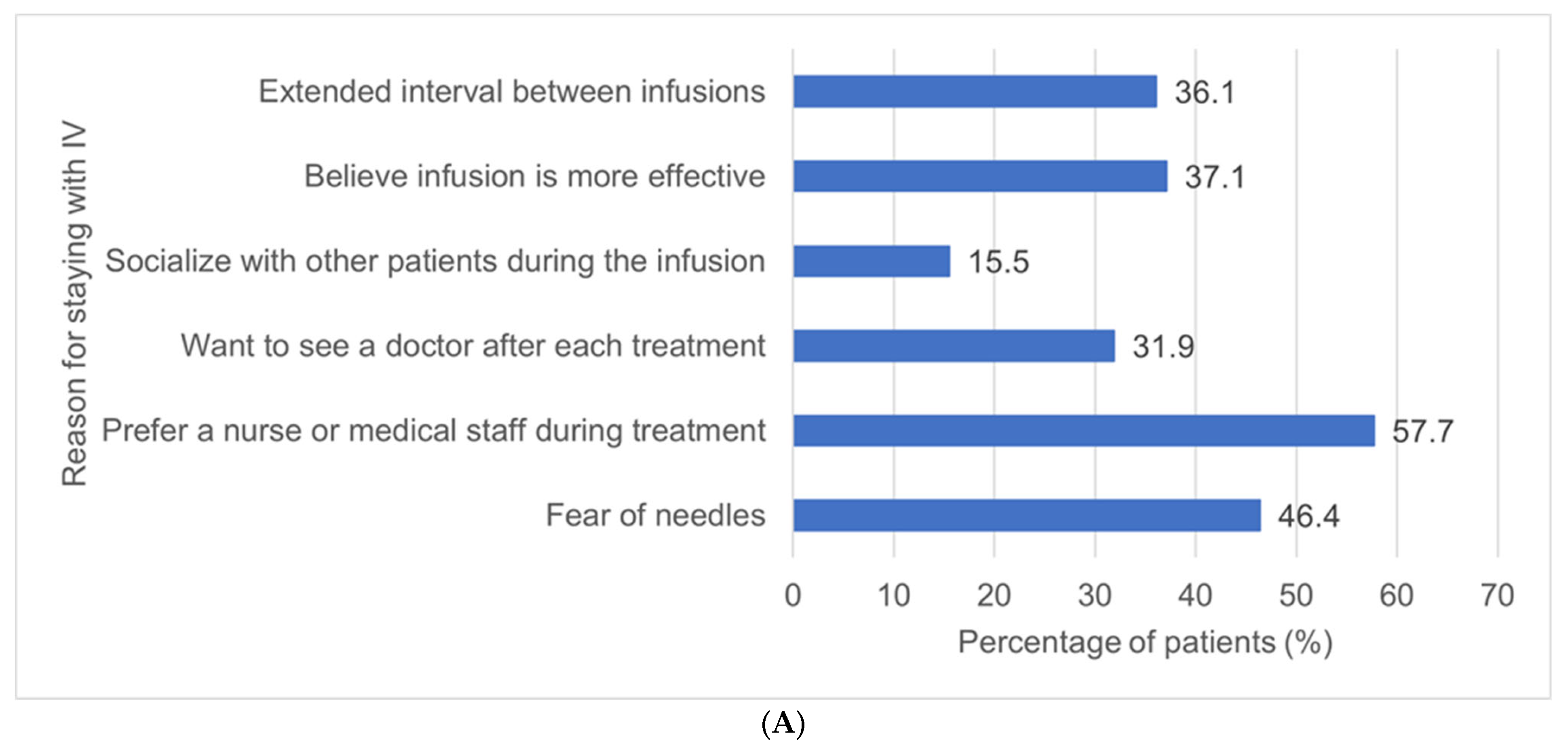
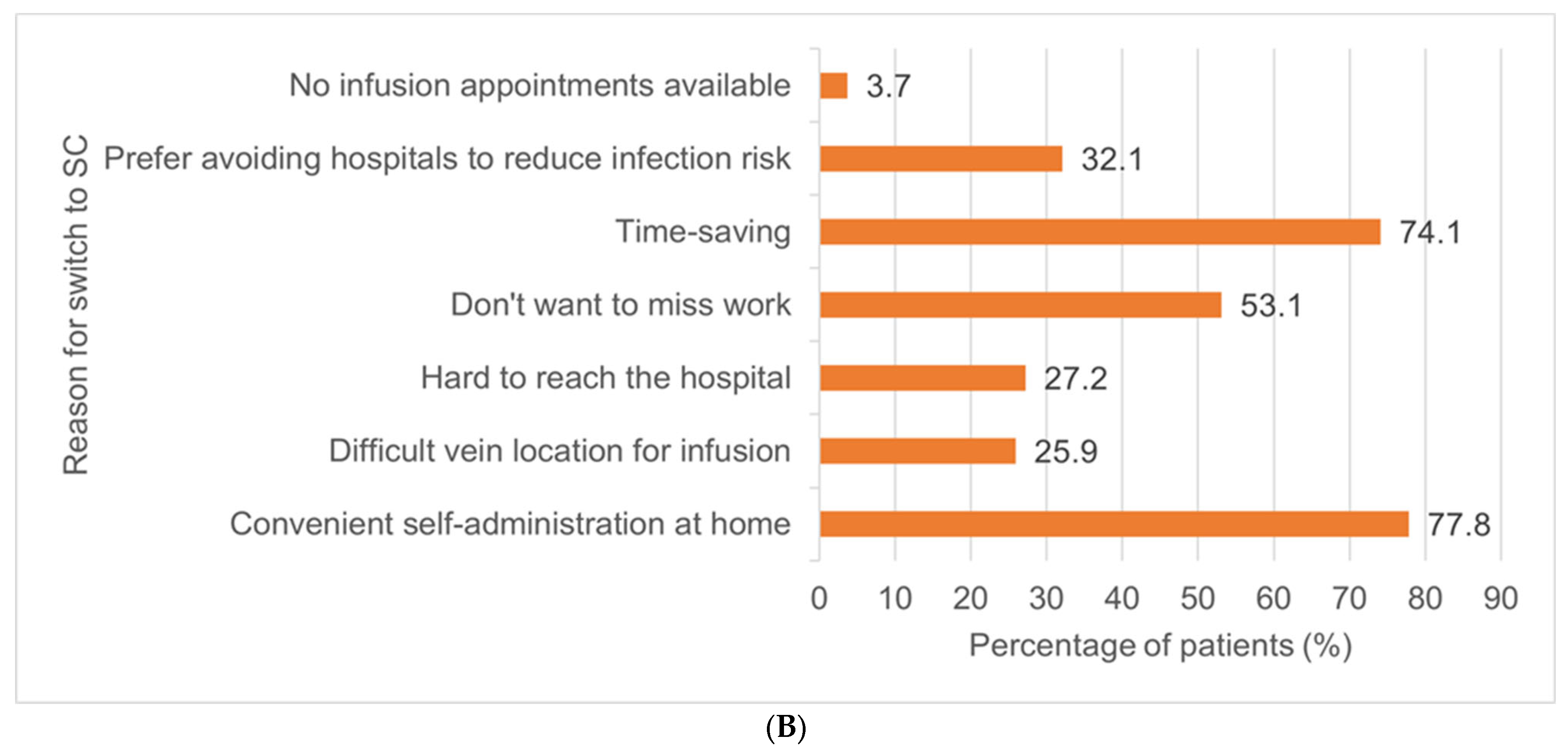
3.5. Interest of Intravenous Patients in Switching to Subcutaneous Treatment
3.6. Comparative Cost Analysis between IV and SC Therapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Takeda Pharma. Vedolizumab Summary of Product Characteristics; European Medicines Agency: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Celltrion Healthcare. Remsima Summary of Product Characteristics; European Medicines Agency: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Darie, A.M.; Sinopoulou, V.; Ajay, V.; Kok, K.B.; Patel, K.V.; Limdi, J.; Arebi, N.; Smith, P.; Din, S.; Din, S.; et al. BSG 2024 IBD Guidelines Protocol (Standard Operating Procedures). BMJ Open Gastroenterol. 2023, 10, e001067. [Google Scholar] [CrossRef]
- Hong, S.N.; Song, J.H.; Kim, S.J.; Park, Y.H.; Choi, C.W.; Kim, J.E.; Kim, E.R.; Chang, D.K.; Kim, Y.-H. One-Year Clinical Outcomes of Subcutaneous Infliximab Maintenance Therapy Compared with Intravenous Infliximab Maintenance Therapy in Patients with Inflammatory Bowel Disease: A Prospective Cohort Study. Inflamm. Bowel Dis. 2023, izad094. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.H.; Gros, B.; Sharma, E.; Lehmann, A.; Lindsay, J.O.; Caulfield, L.; Gaya, D.R.; Taylor, J.; Limdi, J.; Kwok, J.; et al. Safety, Effectiveness, and Treatment Persistence of Subcutaneous Vedolizumab in IBD: A Multicenter Study from the United Kingdom. Inflamm. Bowel Dis. 2023, izad166. [Google Scholar] [CrossRef] [PubMed]
- Bergqvist, V.; Holmgren, J.; Klintman, D.; Marsal, J. Real-World Data on Switching from Intravenous to Subcutaneous Vedolizumab Treatment in Patients with Inflammatory Bowel Disease. Aliment. Pharmacol. Ther. 2022, 55, 1389–1401. [Google Scholar] [CrossRef] [PubMed]
- Volkers, A.; Straatmijer, T.; Duijvestein, M.; Sales, A.; Levran, A.; van Schaik, F.; Maljaars, J.; Gecse, K.; Ponsioen, C.; Grootjans, J.; et al. Real-World Experience of Switching from Intravenous to Subcutaneous Vedolizumab Maintenance Treatment for Inflammatory Bowel Diseases. Aliment. Pharmacol. Ther. 2022, 56, 1044–1054. [Google Scholar] [CrossRef] [PubMed]
- Cerna, K.; Duricova, D.; Lukas, M.; Kolar, M.; Machkova, N.; Hruba, V.; Mitrova, K.; Kubickova, K.; Kostrejova, M.; Jirsa, J.; et al. Subcutaneous Infliximab in Refractory Crohn’s Disease Patients: A Possible Biobetter? Crohns Colitis 360 2023, 5, otad040. [Google Scholar] [CrossRef]
- Buisson, A.; Nachury, M.; Reymond, M.; Yzet, C.; Wils, P.; Payen, L.; Laugie, M.; Manlay, L.; Mathieu, N.; Pereira, B.; et al. Effectiveness of Switching From Intravenous to Subcutaneous Infliximab in Patients with Inflammatory Bowel Diseases: The REMSWITCH Study. Clin. Gastroenterol. Hepatol. 2023, 21, 2338–2346.e3. [Google Scholar] [CrossRef]
- Harno-Tasihin, J.; Siregar, L.; Paajanen, M.; Arkkila, P.; Punkkinen, J. Switching from Intravenous to Subcutaneous Infliximab and Vedolizumab in Patients with Inflammatory Bowel Disease: Impact on Trough Levels, Day Hospital Visits, and Medical Expenses. Scand. J. Gastroenterol. 2023, 1–8. [Google Scholar] [CrossRef]
- Buisson, A.; Serrero, M.; Orsat, L.; Nancey, S.; Rivière, P.; Altwegg, R.; Peyrin-Biroulet, L.; Nachury, M.; Hébuterne, X.; Gilletta, C.; et al. Comparative Acceptability of Therapeutic Maintenance Regimens in Patients with Inflammatory Bowel Disease: Results From the Nationwide ACCEPT2 Study. Inflamm. Bowel Dis. 2023, 29, 579–588. [Google Scholar] [CrossRef]
- Matsumoto, T.; Imai, K.; Goda, Y.; Fujimitsu, Y.; Kajioka, T.; Kihara, H.; Funaki, Y.; Imaki, S.; Ueno, M. Questionnaire Survey for IBD Patients in Japan; A Web-Based J-CUP Survey. Crohns Colitis 360 2023, 5, otad069. [Google Scholar] [CrossRef]
- Brunet-Houdard, S.; Monmousseau, F.; Berthon, G.; Des Garets, V.; Laharie, D.; Picon, L.; Fotsing, G.; Gargot, D.; Charpentier, C.; Buisson, A.; et al. How Are Patients’ Preferences for Anti-TNF Influenced by Quality of Life? A Discrete Choice Experiment in Crohn’s Disease Patients. Scand. J. Gastroenterol. 2022, 57, 1312–1320. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, D.; Settanni, C.R.; Parisio, L.; Orgiana, N.; Poscia, A.; Schiavoni, E.; Turchini, L.; Cascio, A.L.; Germini, F.; Sblendorio, E.; et al. Transition from Intravenous to Subcutaneous Biological Therapies in Inflammatory Bowel Disease: An Online Survey of Patients. Indian J. Gastroenterol. 2024. [Google Scholar] [CrossRef] [PubMed]
- Remy, C.; Caron, B.; Gouynou, C.; Haghnejad, V.; Jeanbert, E.; Netter, P.; Danese, S.; Peyrin-Biroulet, L. Inflammatory Bowel Disease Patients’ Acceptance for Switching from Intravenous Infliximab or Vedolizumab to Subcutaneous Formulation: The Nancy Experience. J. Clin. Med. 2022, 11, 7296. [Google Scholar] [CrossRef]
- Irvine, E.; Zhou, Q.; Thompson, A.K. The Short Inflammatory Bowel Disease Questionnaire: A Quality of Life Instrument for Community Physicians Managing Inflammatory Bowel Disease. CCRPT Investigators. Canadian Crohn’s Relapse Prevention Trial. Am. J. Gastroenterol. 1996, 91, 1571–1578. [Google Scholar]
- The Department for Planning, Budgeting and Pricing Ministry of Health. Available online: https://www.gov.il/he/departments/dynamiccollectors/drug-prices?skip=0 (accessed on 22 December 2023).
- Strik, A.S.; van de Vrie, W.; Bloemsaat-Minekus, J.P.J.; Nurmohamed, M.; Bossuyt, P.J.J.; Bodelier, A.; Rispens, T.; van Megen, Y.J.B.; D’Haens, G.R. Serum Concentrations after Switching from Originator Infliximab to the Biosimilar CT-P13 in Patients with Quiescent Inflammatory Bowel Disease (SECURE): An Open-Label, Multicentre, Phase 4 Non-Inferiority Trial. Lancet Gastroenterol. Hepatol. 2018, 3, 404–412. [Google Scholar] [CrossRef]
- Smith, P.J.; Critchley, L.; Storey, D.; Gregg, B.; Stenson, J.; Kneebone, A.; Rimmer, T.; Burke, S.; Hussain, S.; Yi Teoh, W.; et al. Efficacy and Safety of Elective Switching from Intravenous to Subcutaneous Infliximab [CT-P13]: A Multicentre Cohort Study. J. Crohns Colitis 2022, 16, 1436. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.J.; Fumery, M.; Leong, R.W.; Novak, K.; Dignass, A. Real-World Experience with Subcutaneous Infliximab: Broadening Treatment Strategies for Inflammatory Bowel Disease. Expert. Rev. Clin. Immunol. 2023, 19, 1143–1156. [Google Scholar] [CrossRef] [PubMed]
- Michielan, A.; Martinato, M.; Favarin, A.; Zanotto, V.; Caccaro, R.; Caruso, A.; Sturniolo, G.C.; D’Incà, R. A Nurse-Led Accelerated Procedure for Infliximab Infusion Is Well Tolerated and Effective in Patients with Inflammatory Bowel Disease. Dig. Liver Dis. 2015, 47, 372–377. [Google Scholar] [CrossRef]
- Jonaitis, L.; Marković, S.; Farkas, K.; Gheorghe, L.; Krznarić, Ž.; Salupere, R.; Mokricka, V.; Spassova, Z.; Gatev, D.; Grosu, I.; et al. Intravenous versus Subcutaneous Delivery of Biotherapeutics in IBD: An Expert’s and Patient’s Perspective. BMC Proc. 2021, 15, 25. [Google Scholar] [CrossRef]
- Overton, P.M.; Shalet, N.; Somers, F.; Allen, J.A. Patient Preferences for Subcutaneous versus Intravenous Administration of Treatment for Chronic Immune System Disorders: A Systematic Review. Patient Prefer. Adherence 2021, 15, 811–834. [Google Scholar] [CrossRef]
- Burdge, G.; Hardman, A.; Carbery, I.; Broglio, G.; Greer, D.; Selinger, C.P. Uptake of a Switching Program for Patients Receiving Intravenous Infliximab and Vedolizumab to Subcutaneous Preparations. J. Clin. Med. 2022, 11, 5669. [Google Scholar] [CrossRef]
- Van Deen, W.K.; Khalil, C.; Bonthala, N.N.; Gale, R.; Patel, D.B.; Warui, E.; Melmed, G.Y.; Spiegel, B.M.R. Inflammatory Bowel Disease Patients’ Preferences for Subcutaneous versus Intravenous Therapies: A Mixed-Methods Study. Dig. Dis. 2023, 41, 412–421. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | IBD Patients n = 454 |
|---|---|
| Age (median, (IQR)) | 42 (29–57) |
| Female gender (n, %) | 253 (55.7) |
| Smoking (n, %) | 80 (17.6%) |
| BMI (median, (IQR)) | 24.4 (21.4–28.0) |
| Employment status | |
| Currently not employed (n, %) | 138 (30.4) |
| Full-time job (n, %) | 242 (53.3) |
| Part-time job (n, %) | 74 (16.3) |
| Independent arrival to infusion center (n, %) | 414 (91.2) |
| Living with other people | 397 (87.4) |
| IBD type | |
| Crohn’s disease (n, %) | 307 (67.6) |
| Ulcerative colitis (n, %) | 147 (32.4) |
| Age at diagnosis (median, (IQR)) | 25 (18–39) |
| Active disease (n, %) | 223 (49.1) |
| Current use of corticosteroids (n, %) | 41 (9) |
| Another systemic disease 1 (n, %) | 165 (36.3) |
| Current IBD treatment 2 | |
| Per os (n, %) | 132 (29.1) |
| Subcutaneous (n, %) | 232 (51.1) |
| Intravenous (n, %) | 296 (65.2) |
| Poor compliance with medication intake (n, %) | 191 (42.1) |
| Per os (n, %) | 120 (62.8) |
| Subcutaneous (n, %) | 42 (22.0) |
| Intravenous (n, %) | 29 (15.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Richter, V.; Cohen, D.L.; Kriger-Sharabi, O.; Zelnik Yovel, D.; Kochen, N.; Broide, E.; Shirin, H. Switching from Intravenous to Subcutaneous Biological Therapy for Inflammatory Bowel Disease Patients Remains a Challenge. J. Clin. Med. 2024, 13, 1357. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13051357
Richter V, Cohen DL, Kriger-Sharabi O, Zelnik Yovel D, Kochen N, Broide E, Shirin H. Switching from Intravenous to Subcutaneous Biological Therapy for Inflammatory Bowel Disease Patients Remains a Challenge. Journal of Clinical Medicine. 2024; 13(5):1357. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13051357
Chicago/Turabian StyleRichter, Vered, Daniel L. Cohen, Ofra Kriger-Sharabi, Dana Zelnik Yovel, Nadav Kochen, Efrat Broide, and Haim Shirin. 2024. "Switching from Intravenous to Subcutaneous Biological Therapy for Inflammatory Bowel Disease Patients Remains a Challenge" Journal of Clinical Medicine 13, no. 5: 1357. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13051357