Real-World Treatment Patterns and Survival Outcomes for Patients with Non-Metastatic Non-Small-Cell Lung Cancer in Sweden: A Nationwide Registry Analysis from the I-O Optimise Initiative


 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Inclusion Criteria and Study Design
2.2. Variables
2.3. Statistical Analysis
2.4. Ethics
3. Results
3.1. Patient Population
3.2. Treatment Patterns
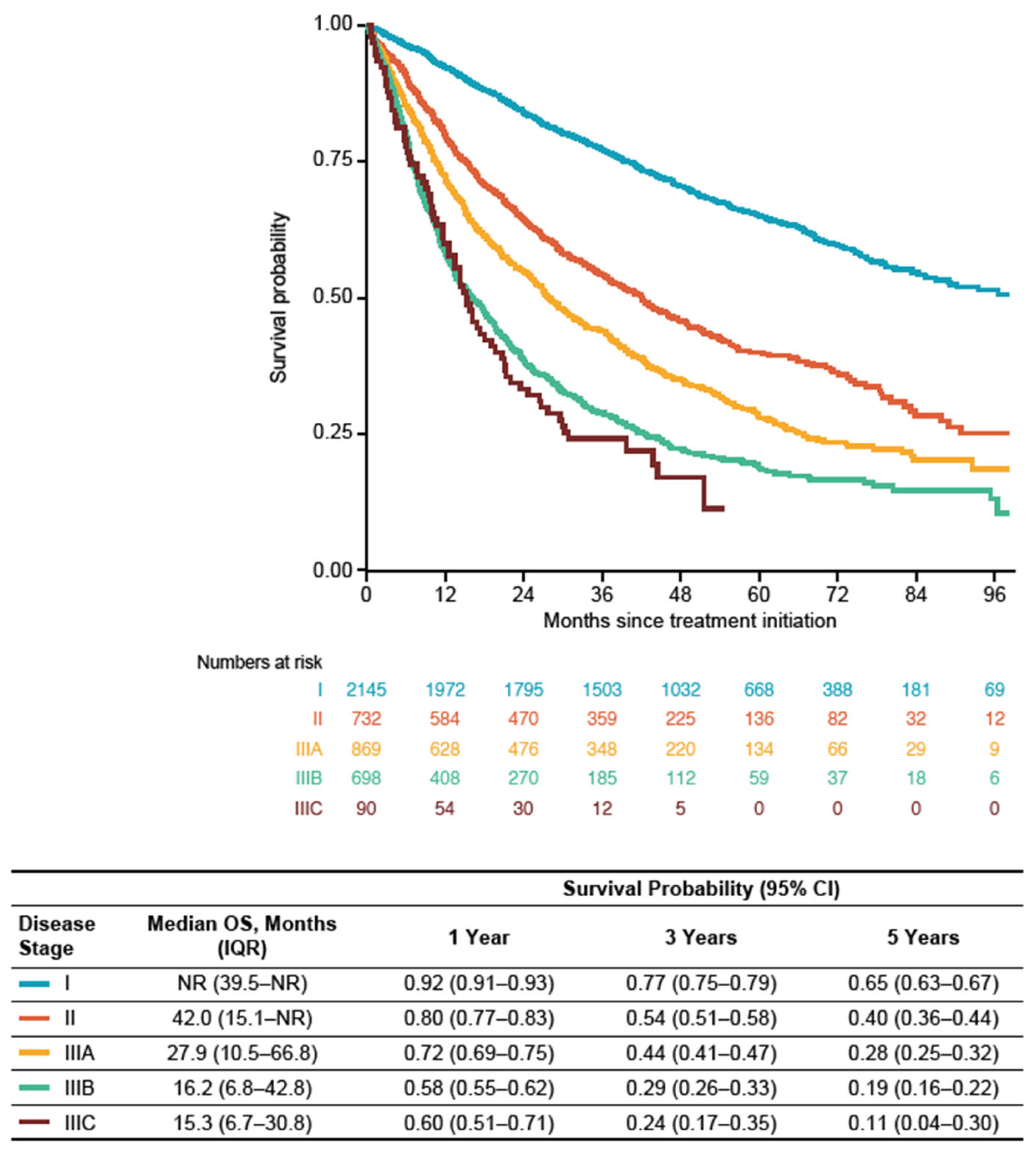
3.3. Overall Survival
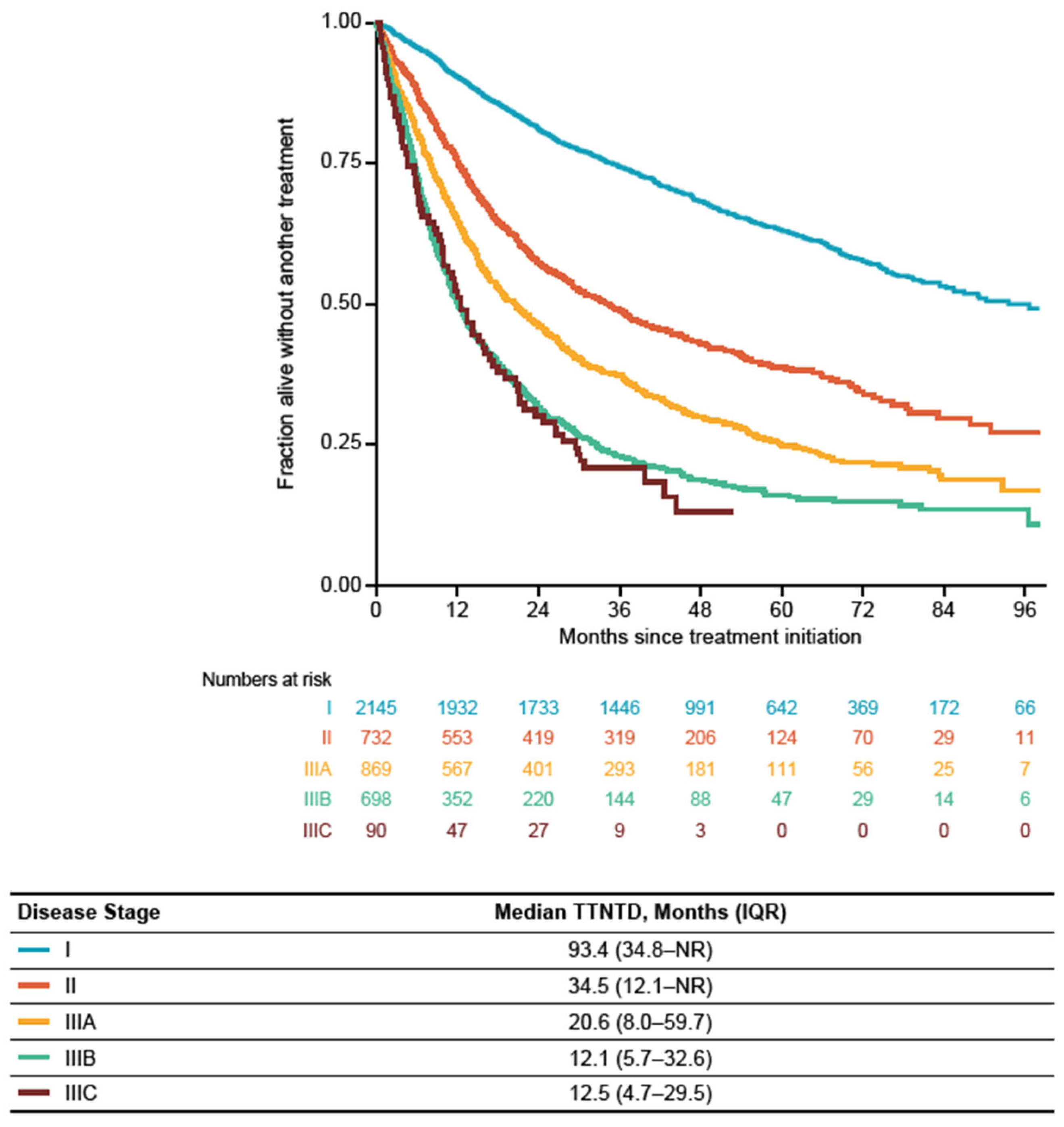
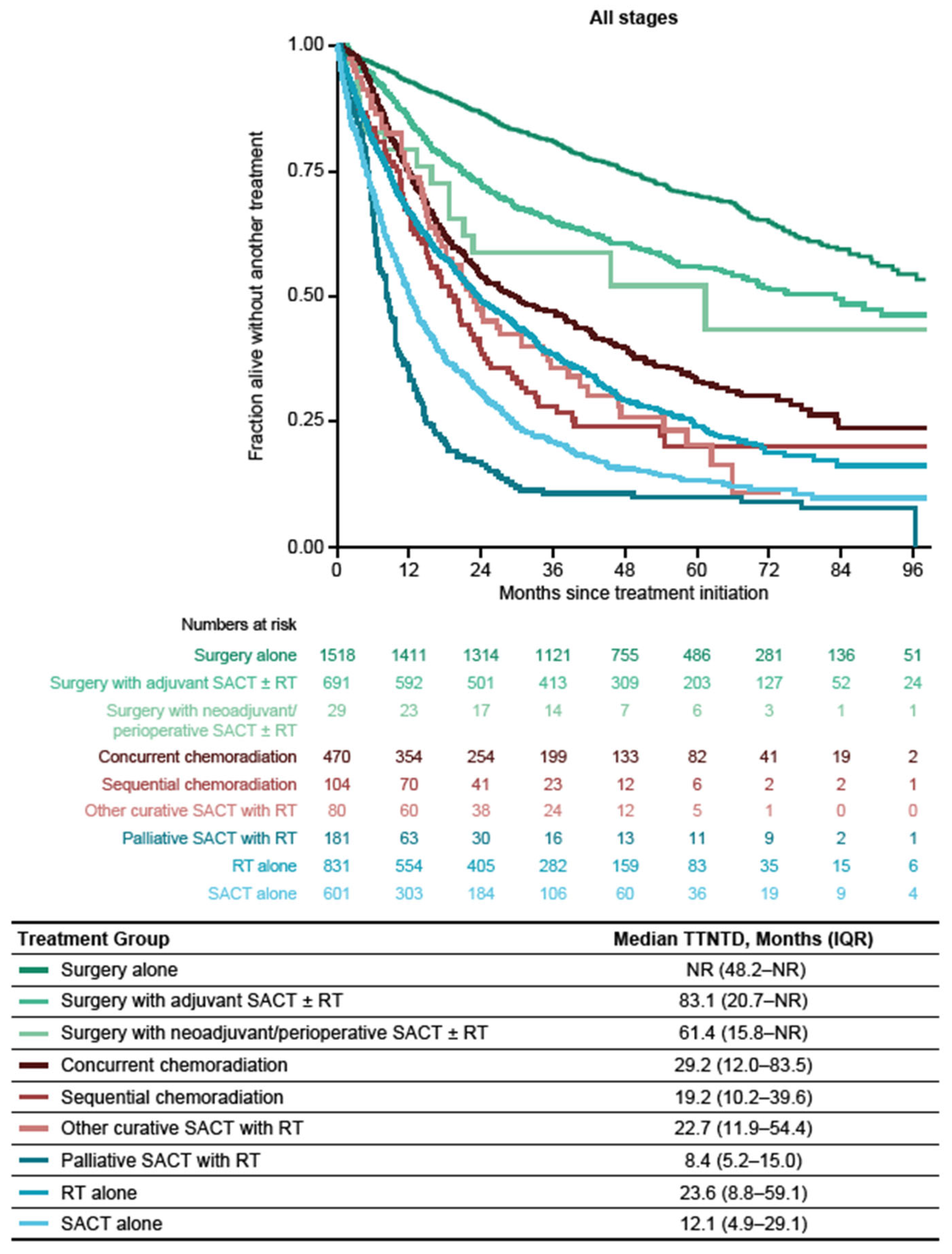
3.4. Time to Next Treatment or Death
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hierarchy Order | Initial Treatment Category | Definition |
|---|---|---|
| 1 | Surgery alone | First treatment recorded is surgery, AND patient has no record of SACT up to 84 days after surgery date, AND patient has no record of RT up to 84 days after surgery date. |
| 2 | Surgery with adjuvant SACT | First treatment recorded is surgery, AND patient has record of (adjuvant) SACT up to 84 days after surgery date, AND patient has no record of RT up to 180 days after SACT start date. |
| 3 | Surgery with adjuvant RT | First treatment record is surgery, AND patient has record of RT start up to 84 days after surgery date, AND patient has no record of SACT up to 180 days after RT start date. |
| 4 | Surgery with adjuvant RT and SACT | First treatment record is surgery, AND patient has record of RT start (OR SACT) up to 84 days after surgery date, AND patient has record of SACT (OR RT) start up to 180 days after RT (OR SACT) start date. |
| 5 | Surgery with neoadjuvant SACT | First treatment recorded is (neoadjuvant) SACT, AND patient has record of surgery up to 150 days after first SACT regimen start date, AND patient has no record of RT prior to surgery date. |
| 6 | Surgery with perioperative SACT | First treatment recorded is SACT (before surgery), AND patient has record of surgery up to 150 days after first SACT regimen start date, AND patient has record of SACT (administered again) up to 84 days after the date of surgery. |
| 7 | Surgery with neoadjuvant RT | First treatment recorded is RT, AND patient has record of surgery up to 90 days after first (neoadjuvant) RT regimen start date, AND patient has no record of SACT prior to surgery. |
| 8 | Surgery with neoadjuvant SACT and RT | Either of the following applies: (1) First treatment recorded is (neoadjuvant) SACT, AND patient has record of RT start date up to 42 days after SACT start date, AND patient has record of surgery date up to 90 days after RT; OR (2) First treatment is RT, AND patient has (neoadjuvant) SACT start date up to 42 days after RT start date, AND patient has record of surgery up to 90 days after SACT start date. |
| 9 | RT alone | First treatment recorded is RT, AND patient has no record of surgery up to 90 days after RT start date, AND patient has no record of SACT up to 90 days after RT start date. |
| 10 | Palliative SACT with RT | Either sequence combination: [(1) First treatment record is RT with palliative intent, AND patient has record of SACT up to 90 days after first RT start date]; OR [(2) First treatment record is SACT, AND patient has record of RT with palliative intent up to 150 days after first SACT regimen start date]; AND patient has no surgery up to 180 days after first SACT start date. |
| 11 | Sequential chemoradiation | First treatment recorded is SACT, AND patient has a record of RT with curative/radical intent, AND RT start date is after SACT end date, AND the RT start date is recorded in the 42-day period after SACT end date, AND patient has no record of surgery in the 90-day period after the end date of RT. |
| 12 | Concurrent chemoradiation | First treatment recorded is SACT, AND patient has a record of RT with curative/radical intent, AND RT start date is before SACT end date, AND patient has no record of IO starting in the 42-day period after the end date of RT, AND patient has no record of surgery in the 90-day period after the end date of RT. |
| 13 | Other curative SACT with RT | Any curative SACT and RT treatment identified that was not classified as chemoradiation by the algorithm as defined above in points 11 and 12: [First treatment record is RT with curative/radical intent, AND patient has record of SACT start date up to 90 days after first RT start date]; OR [First treatment record is SACT start date, AND patient has record of RT with curative/radical intent up to 150 days after first SACT start date], AND patient has no surgery within 180 days after first SACT start date. |
| 14 | Concurrent chemoradiation with IO | First treatment record is SACT, AND patient has record of RT with curative/radical intent, AND RT start date is before SACT end date, AND patient has record of IO start date * up to 42 days after the last RT administration, AND patient has no record of surgery up to 90 days after the end of RT. |
| 15 | Other SACT with RT | [First treatment recorded is RT, AND patient has record of SACT start date up to 90 days after first RT start date]; OR [First treatment record is SACT, AND patient has record of RT up to 150 days after first SACT start date], AND patient has no surgery up to 180 days after first SACT start date (no reliance on RT intent). |
| 16 | SACT alone | First treatment record is SACT, AND patient has no record of RT up to 150 days after first SACT start date, AND patient has no record of surgery up to 150 days after SACT start date. |
| 17 | No treatment received | No treatment received within first 6 months following diagnosis: Patient has no record of surgery up to 180 days after diagnosis date, AND patient has no record of SACT up to 180 days after diagnosis date, AND patient has no record of RT up to 180 days after diagnosis date. |
| 18 | Otherwise unclassified | Patients who do not fall into any of the above categories |




References
- Molina, J.R.; Yang, P.; Cassivi, S.D.; Schild, S.E.; Adjei, A.A. Non-small cell lung cancer: Epidemiology, risk factors, treatment, and survivorship. Mayo Clin. Proc. 2008, 83, 584–594. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer. UICC. Global Cancer Observatory: GLOBOCAN. 2020. Available online: https://gco.iarc.fr/ (accessed on 12 October 2023).
- National Lung Cancer Registry. Available online: https://statistik.incanet.se/Lunga/ (accessed on 19 December 2023).
- Calvo, V.; Aliaga, C.; Carracedo, C.; Provencio, M. Prognostic factors in potentially resectable stage III non-small cell lung cancer receiving neoadjuvant treatment-a narrative review. Transl. Lung Cancer Res. 2021, 10, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V.; et al. The IASLC Lung Cancer Staging Project: Proposals for revision of the TNM stage groupings in the forthcoming (eighth) edition of the TNM classification for lung cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef]
- Masago, K.; Seto, K.; Fujita, S.; Sasaki, E.; Hosoda, W.; Kuroda, H. Long-term recurrence of completely resected NSCLC. JTO Clin. Res. Rep. 2020, 1, 100076. [Google Scholar] [CrossRef] [PubMed]
- Auperin, A.; Le Pechoux, C.; Rolland, E.; Curran, W.J.; Furuse, K.; Fournel, P.; Belderbos, J.; Clamon, G.; Ulutin, H.C.; Paulus, R.; et al. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J. Clin. Oncol. 2010, 28, 2181–2190. [Google Scholar] [CrossRef] [PubMed]
- Postmus, P.E.; Kerr, K.M.; Oudkerk, M.; Senan, S.; Waller, D.A.; Vansteenkiste, J.; Escriu, C.; Peters, S.; Committee, E.G. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv1–iv21. [Google Scholar] [CrossRef] [PubMed]
- Vansteenkiste, J.; De Ruysscher, D.; Eberhardt, W.E.; Lim, E.; Senan, S.; Felip, E.; Peters, S.; Group, E.G.W. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24, vi89–vi98. [Google Scholar] [CrossRef] [PubMed]
- Forde, P.M.; Spicer, J.; Lu, S.; Provencio, M.; Mitsudomi, T.; Awad, M.M.; Felip, E.; Broderick, S.R.; Brahmer, J.R.; Swanson, S.J.; et al. Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. N. Engl. J. Med. 2022, 386, 1973–1985. [Google Scholar] [CrossRef]
- Felip, E.; Altorki, N.; Zhou, C.; Csoszi, T.; Vynnychenko, I.; Goloborodko, O.; Luft, A.; Akopov, A.; Martinez-Marti, A.; Kenmotsu, H.; et al. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB-IIIA non-small-cell lung cancer (IMpower010): A randomised, multicentre, open-label, phase 3 trial. Lancet 2021, 398, 1344–1357. [Google Scholar] [CrossRef]
- O’Brien, M.; Paz-Ares, L.; Marreaud, S.; Dafni, U.; Oselin, K.; Havel, L.; Esteban, E.; Isla, D.; Martinez-Marti, A.; Faehling, M.; et al. Pembrolizumab versus placebo as adjuvant therapy for completely resected stage IB-IIIA non-small-cell lung cancer (PEARLS/KEYNOTE-091): An interim analysis of a randomised, triple-blind, phase 3 trial. Lancet Oncol. 2022, 23, 1274–1286. [Google Scholar] [CrossRef] [PubMed]
- Remon, J.; Soria, J.C.; Peters, S.; Esmo Guidelines Committee. Early and locally advanced non-small-cell lung cancer: An update of the ESMO Clinical Practice Guidelines focusing on diagnosis, staging, systemic and local therapy. Ann. Oncol. 2021, 32, 1637–1642. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology: Non-Small Cell Lung Cancer. V2.2023. Available online: https://education.nccn.org/node/92905 (accessed on 4 October 2023).
- European Society for Medical Oncology. ESMO Oncology News: EMA Recommends Extension of Indications for Nivolumab. Available online: https://www.esmo.org/oncology-news/ema-recommends-extension-of-indications-for-nivolumab2 (accessed on 12 October 2023).
- Wait, S.; Alvarez-Rosete, A.; Osama, T.; Bancroft, D.; Cornelissen, R.; Marusic, A.; Garrido, P.; Adamek, M.; van Meerbeeck, J.; Snoeckx, A.; et al. Implementing lung cancer screening in Europe: Taking a systems approach. JTO Clin. Res. Rep. 2022, 3, 100329. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.J.; Stone, E.; Baldwin, D.R.; Vliegenthart, R.; Lee, P.; Fintelmann, F.J. Lung cancer screening. Lancet 2023, 401, 390–408. [Google Scholar] [CrossRef] [PubMed]
- Ekman, S.; Griesinger, F.; Baas, P.; Chao, D.; Chouaid, C.; O’Donnell, J.C.; Penrod, J.R.; Daumont, M.; Lacoin, L.; McKenney, A.; et al. I-O Optimise: A novel multinational real-world research platform in thoracic malignancies. Future Oncol. 2019, 15, 1551–1563. [Google Scholar] [CrossRef] [PubMed]
- Ganti, A.K.; Klein, A.B.; Cotarla, I.; Seal, B.; Chou, E. Update of incidence, prevalence, survival, and initial treatment in patients with non-small cell lung cancer in the US. JAMA Oncol. 2021, 7, 1824–1832. [Google Scholar] [CrossRef] [PubMed]
- Ekman, S.; Horvat, P.; Rosenlund, M.; Kejs, A.M.; Patel, D.; Juarez-Garcia, A.; Lacoin, L.; Daumont, M.J.; Penrod, J.R.; Brustugun, O.T.; et al. Epidemiology and survival outcomes for patients with NSCLC in Scandinavia in the preimmunotherapy era: A SCAN-LEAF retrospective analysis from the I-O Optimise initiative. JTO Clin. Res. Rep. 2021, 2, 100165. [Google Scholar] [CrossRef]
- Jazieh, A.R.; Onal, H.C.; Tan, D.S.W.; Soo, R.A.; Prabhash, K.; Kumar, A.; Huggenberger, R.; Robb, S.; Cho, B.C. Real-world treatment patterns and clinical outcomes in patients with stage III NSCLC: Results of KINDLE, a multicountry observational study. J. Thorac. Oncol. 2021, 16, 1733–1744. [Google Scholar] [CrossRef] [PubMed]
- PDQ Adult Treatment Editorial Board. Non-small cell lung cancer treatment (PDQ®): Health professional version. In PDQ Cancer Information Summaries [Internet]; National Cancer Institute: Bethesda, MD, USA, 2002. [Google Scholar]
- Akhtar-Danesh, G.G.; Finley, C.; Seow, H.Y.; Shakeel, S.; Akhtar-Danesh, N. Change in treatment modality and trends in survival among stage I non-small cell lung cancer patients: A population-based study. J. Thorac. Dis. 2020, 12, 4670–4679. [Google Scholar] [CrossRef] [PubMed]
- Snee, M.; Cheeseman, S.; Thompson, M.; Riaz, M.; Sopwith, W.; Lacoin, L.; Chaib, C.; Daumont, M.J.; Penrod, J.R.; Hall, G. Treatment patterns and survival outcomes for patients with non-small cell lung cancer in the UK in the preimmunology era: A REAL-Oncology database analysis from the I-O Optimise initiative. BMJ Open 2021, 11, e046396. [Google Scholar] [CrossRef] [PubMed]
- Provencio, M.; Carcereny, E.; Lopez Castro, R.; Calvo, V.; Rodriguez Abreu, D.; Cobo, M.; Ortega, A.L.; Bernabe, R.; Guirado, M.; Massuti, B.; et al. Real-world treatment patterns and survival outcomes for patients with stage III non-small cell lung cancer in Spain: A nationwide cohort study. Transl. Lung Cancer Res. 2023, 12, 2113–2128. [Google Scholar] [CrossRef] [PubMed]
- Soares, M.; Antunes, L.; Redondo, P.; Borges, M.; Hermans, R.; Patel, D.; Grimson, F.; Munro, R.; Chaib, C.; Lacoin, L.; et al. Real-world treatment patterns and survival outcomes for advanced non-small cell lung cancer in the pre-immunotherapy era in Portugal: A retrospective analysis from the I-O Optimise initiative. BMC Pulm. Med. 2020, 20, 240. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.; Ridge, C.A.; Nicholson, A.G.; Mirsadraee, S. The 8(th) lung cancer TNM classification and clinical staging system: Review of the changes and clinical implications. Quant. Imaging Med. Surg. 2018, 8, 709–718. [Google Scholar] [CrossRef] [PubMed]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Wang, S.; Zhou, Y.; Lai, S.; Xiao, G.; Gazdar, A.; Xie, Y. Evaluation of the 7(th) and 8(th) editions of the AJCC/UICC TNM staging systems for lung cancer in a large North American cohort. Oncotarget 2017, 8, 66784–66795. [Google Scholar] [CrossRef] [PubMed]
- Okami, J.; Shintani, Y.; Okumura, M.; Ito, H.; Ohtsuka, T.; Toyooka, S.; Mori, T.; Watanabe, S.I.; Date, H.; Yokoi, K.; et al. Demographics, safety and quality, and prognostic information in both the seventh and eighth editions of the TNM classification in 18,973 surgical cases of the Japanese Joint Committee of Lung Cancer Registry Database in 2010. J. Thorac. Oncol. 2019, 14, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Neppl, C.; Keller, M.D.; Scherz, A.; Dorn, P.; Schmid, R.A.; Zlobec, I.; Berezowska, S. Comparison of the 7th and 8th edition of the UICC/AJCC TNM staging system in primary resected squamous cell carcinomas of the lung—A single center analysis of 354 cases. Front. Med. 2019, 6, 196. [Google Scholar] [CrossRef] [PubMed]
- Casal-Mourino, A.; Ruano-Ravina, A.; Lorenzo-Gonzalez, M.; Rodriguez-Martinez, A.; Giraldo-Osorio, A.; Varela-Lema, L.; Pereiro-Brea, T.; Barros-Dios, J.M.; Valdes-Cuadrado, L.; Perez-Rios, M. Epidemiology of stage III lung cancer: Frequency, diagnostic characteristics, and survival. Transl. Lung Cancer Res. 2021, 10, 506–518. [Google Scholar] [CrossRef] [PubMed]
- Delgado, A.; Guddati, A.K. Clinical endpoints in oncology—A primer. Am. J. Cancer Res. 2021, 11, 1121–1131. [Google Scholar] [PubMed]
- Branchoux, S.; Sofeu, C.L.; Gaudin, A.F.; Kurt, M.; Moshyk, A.; Italiano, A.; Bellera, C.; Rondeau, V. Time to next treatment or death as a candidate surrogate endpoint for overall survival in advanced melanoma patients treated with immune checkpoint inhibitors: An insight from the phase III CheckMate 067 trial. ESMO Open 2022, 7, 100340. [Google Scholar] [CrossRef] [PubMed]
- de Jong, D.; Das, J.P.; Ma, H.; Pailey Valiplackal, J.; Prendergast, C.; Roa, T.; Braumuller, B.; Deng, A.; Dercle, L.; Yeh, R.; et al. Novel targets, novel treatments: The changing landscape of non-small cell lung cancer. Cancers 2023, 15, 2855. [Google Scholar] [CrossRef] [PubMed]
- Lazzari, C.; Spagnolo, C.C.; Ciappina, G.; Di Pietro, M.; Squeri, A.; Passalacqua, M.I.; Marchesi, S.; Gregorc, V.; Santarpia, M. Immunotherapy in early-stage non-small cell lung cancer (NSCLC): Current evidence and perspectives. Curr. Oncol. 2023, 30, 3684–3696. [Google Scholar] [CrossRef] [PubMed]
- TECENTRIQ® (Atezolizumab) [Summary of Product Characteristics]; Roche Pharma AG: Grenzach-Wyhlen, Germany, 2022.
- TECENTRIQ® (Atezolizumab) [Prescribing Information]; Genentech, Inc.: South San Francisco, CA, USA, 2022.
- OPDIVO® (Nivolumab) [Prescribing Information]; Bristol Myers Squibb: Princeton, NJ, USA, 2022.






| Overall Patient Population N = 17,433 | Stage I | Stage II | Stage IIIA | Stage IIIB | Stage IIIC |
|---|---|---|---|---|---|
| (n = 7153) | (n = 2675) | (n = 3679) | (n = 3727) | (n = 199) | |
| Age at diagnosis, years | |||||
| Median (IQR) | 71.0 (65.0–76.0) | 71.0 (65.0–77.0) | 71.0 (65.0–77.0) | 71.0 (64.0–77.0) | 72.0 (65.5–77.0) |
| Female, n (%) | 3988 (55.8) | 1257 (47.0) | 1833 (49.8) | 1725 (46.3) | 96 (48.2) |
| Smoking status, n (%) | |||||
| Smoker | 2715 (38.0) | 1106 (41.3) | 1544 (42.0) | 1607 (43.1) | 72 (36.2) |
| Former smoker | 3523 (49.3) | 1341 (50.1) | 1805 (49.1) | 1786 (47.9) | 106 (53.3) |
| Never smoker | 885 (12.4) | 219 (8.2) | 313 (8.5) | 307 (8.2) | 21 (10.6) |
| NA | 30 (0.4) | 9 (0.3) | 17 (0.5) | 27 (0.7) | 0 (0.0) |
| ECOG performance status at diagnosis, n (%) | |||||
| 0 | 3491 (48.8) | 976 (36.5) | 1137 (30.9) | 790 (21.2) | 51 (25.6) |
| 1 | 2805 (39.2) | 1099 (41.1) | 1556 (42.3) | 1513 (40.6) | 75 (37.7) |
| 2 | 654 (9.1) | 393 (14.7) | 604 (16.4) | 836 (22.4) | 43 (21.6) |
| 3 | 134 (1.9) | 141 (5.3) | 266 (7.2) | 386 (10.4) | 23 (11.6) |
| 4 | 21 (0.3) | 29 (1.1) | 52 (1.4) | 104 (2.8) | <5 |
| NA | 48 (0.7) | 37 (1.4) | 64 (1.7) | 98 (2.6) | 6 (3.0) |
| Histology, n (%) | |||||
| Adenocarcinoma | 5134 (71.8) | 1440 (53.8) | 1841 (50.0) | 1877 (50.4) | 91 (45.7) |
| Large cell carcinoma | 344 (4.8) | 189 (7.1) | 387 (10.5) | 441 (11.8) | 19 (9.5) |
| Squamous cell NSCLC | 1513 (21.2) | 943 (35.3) | 1321 (35.9) | 1278 (34.3) | 83 (41.7) |
| NSCLC, not otherwise specified | 162 (2.3) | 103 (3.9) | 130 (3.5) | 131 (3.5) | 6 (3.0) |
| Treatment Subgroup | Stage I | Stage II | Stage IIIA | Stage IIIB | Stage IIIC |
|---|---|---|---|---|---|
| N = 5147 | (n = 2259) | (n = 819) | (n = 1051) | (n = 879) | (n = 139) |
| Treatment type, n (%) | |||||
| Any surgery as initial treatment | 1578 (69.9) | 460 (56.2) | 184 (17.5) | 16 (1.8) | 0 (0.0) |
| Any RT as initial treatment | 525 (23.2) | 196 (23.9) | 245 (23.3) | 211 (24.0) | 31 (22.3) |
| Any SACT as initial treatment | 365 (16.2) | 359 (43.8) | 396 (37.7) | 399 (45.4) | 65 (46.8) |
| Initial treatment received, n (%) | |||||
| Surgery alone | 1269 (56.2) | 179 (21.9) | 67 (6.4) | <5 | 0 (0.0) |
| Surgery with adjuvant SACT ± RT | 308 (13.6) | 272 (33.2) | 100 (9.5) | 11 (1.3) | 0 (0.0) |
| Surgery with perioperative SACT or neoadjuvant SACT ± RT | <5 | 9 (1.1) | 17 (1.6) | <5 | 0 (0.0) |
| RT alone | 488 (21.6) | 127 (15.5) | 112 (10.7) | 96 (10.9) | 8 (5.8) |
| Palliative SACT with RT | 9 (0.4) | 18 (2.2) | 52 (4.9) | 85 (9.7) | 17 (12.2) |
| Sequential chemoradiation | <5 | 9 (1.1) | 44 (4.2) | 45 (5.1) | <5 |
| Concurrent chemoradiation | 15 (0.7) | 48 (5.9) | 239 (22.7) | 154 (17.5) | 14 (10.1) |
| Other curative SACT with RT | 10 (0.4) | 9 (1.1) | 37 (3.5) | 18 (2.0) | 6 (4.3) |
| Other SACT with RT | 0 (0.0) | <5 | 7 (0.7) | 7 (0.8) | 0 (0.0) |
| SACT alone | 41 (1.8) | 56 (6.8) | 185 (17.6) | 277 (31.5) | 42 (30.2) |
| No treatment received | 114 (5.0) | 87 (10.6) | 182 (17.3) | 181 (20.6) | 49 (35.3) |
| Otherwise unclassified | <5 | <5 | 9 (0.9) | 0 (0.0) | 0 (0.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oskarsdottir, G.N.; Lampa, E.; Berglund, A.; Rosengren, L.; Ulvestad, M.; Boros, M.; Daumont, M.J.; Rault, C.; Emanuel, G.; Leal, C.; et al. Real-World Treatment Patterns and Survival Outcomes for Patients with Non-Metastatic Non-Small-Cell Lung Cancer in Sweden: A Nationwide Registry Analysis from the I-O Optimise Initiative. Cancers 2024, 16, 1655. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16091655
Oskarsdottir GN, Lampa E, Berglund A, Rosengren L, Ulvestad M, Boros M, Daumont MJ, Rault C, Emanuel G, Leal C, et al. Real-World Treatment Patterns and Survival Outcomes for Patients with Non-Metastatic Non-Small-Cell Lung Cancer in Sweden: A Nationwide Registry Analysis from the I-O Optimise Initiative. Cancers. 2024; 16(9):1655. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16091655
Chicago/Turabian StyleOskarsdottir, Gudrun N., Erik Lampa, Anders Berglund, Linda Rosengren, Maria Ulvestad, Miklos Boros, Melinda J. Daumont, Caroline Rault, Gabrielle Emanuel, Cátia Leal, and et al. 2024. "Real-World Treatment Patterns and Survival Outcomes for Patients with Non-Metastatic Non-Small-Cell Lung Cancer in Sweden: A Nationwide Registry Analysis from the I-O Optimise Initiative" Cancers 16, no. 9: 1655. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16091655