
The Antioxidant Power of a Diet May Improve the Quality of Life of Young Women with Acne Vulgaris

1
Department of Cardiology and Internal Medicine with Cardiac Intensive Care Unit, Medical University of Białystok, M. Skłodowskiej-Curie 24a, 15-276 Białystok, Poland
2
Department of Cosmetology, Faculty of Health Sciences, University of Łomża, Akademicka 14, 18-400 Łomża, Poland
3
Department of Food Biotechnology, Faculty of Health Sciences, Medical University of Białystok, Szpitalna 37, 15-295 Białystok, Poland
*
Author to whom correspondence should be addressed.
Nutrients 2024, 16(9), 1270; https://0-doi-org.brum.beds.ac.uk/10.3390/nu16091270
Submission received: 25 March 2024
/
Revised: 20 April 2024
/
Accepted: 23 April 2024
/
Published: 25 April 2024
(This article belongs to the Special Issue Nutrition and Dermatology—How Much Are They Related?)
Abstract
:Acne vulgaris (AV) significantly reduces the quality of life (QoL) of young people, so it is important to look for factors that can improve their QoL. The aim of this study was to assess the relationship between dietary antioxidants measured using the new DAQI index and QoL measured using standardized tests. The DAQI included the following elements: antioxidant vitamins, minerals, carotenoids, polyphenols, phytosterols, lignans, and the total antioxidant capacity of the diet. The study involved 165 young women with AV, mainly students. A self-report survey was used to collect basic data on their sociodemographic status, anthropometric information, and lifestyle. The energy value of the diet and the content of vitamins, minerals, and carotenoids with antioxidant activity in the diet were estimated using 3-day food diaries and the Diet 6.0 program. The antioxidant potential of the diet and the content of polyphenols, phytosterols, lignans, and selenium were calculated based on the consumption of individual food products and available databases. The results of this study showed that the QoL of the young women with AV was impaired. However, greater adherence to an antioxidant diet reduces the risk of AV impact on the QoL by approximately 30–32% and the risk of depression by 33%. The DAQI may be used as a new indicator of diet quality in acne vulgaris.
1. Introduction
Acne vulgaris (AV) is a chronic skin disease that affects over 9% of the world’s population and over 5% of the European population. It appears mainly during adolescence (85%) but often persists into adulthood [1,2,3]. AV usually presents with comedones, papules, pustules, nodules, and scars, which most often occur on the face [4]. The presence of acne, especially on exposed body parts such as the face, can cause a significant psychological burden, negatively impacting quality of life (QoL) [5]. Therefore, multi-aspect, holistic patient care is important, taking into account both the physical and psychological consequences of acne [6].
The pathophysiology of acne depends on many factors, the most important of which are environmental, genetic, hormonal, and inflammatory factors, as well as gender, age, the presence of acne in the family, a sedentary lifestyle, and eating habits [7]. Many studies have confirmed that health-promoting dietary patterns such as the Mediterranean diet, vegetarian diet, low glycemic index of a diet, dietary probiotics, prebiotics, fiber, and polyunsaturated fatty acids are associated with a reduction in acne lesions. Meanwhile, ultra-processed foods that are rich in saturated fatty acids, sugar, and milk may intensify acne lesions [8,9,10]. Eating habits have been shown to be associated with the QoL in young people with AV [11]. However, although the role of diet in the development and severity of acne has been widely studied, the findings still remain controversial.
In the pathogenesis of AV, oxidative stress plays an important role, defined as a disturbed oxidation–antioxidant balance. A small, physiological amount of reactive oxygen species is needed for the proper functioning of the immune system. However, their overproduction leads to cell damage and, consequently, to skin diseases [12]. Exogenous antioxidants contained in the diet support the action of endogenous antioxidants in eliminating the effects of oxidative stress [13,14,15]. Some authors have shown that selected dietary antioxidants (vitamins, minerals, polyphenols) have a beneficial effect on the prevention and treatment of AV [16,17]. However, it is worth noting that the entire diet contains a variety of antioxidants with complementary effects. Therefore, in this study, we used a new indicator of the antioxidant quality of the diet.
This study presents for the first time the relationship between the DAQI (dietary antioxidant quality index) and the QoL (measured by standardized questionnaires: SWLS, DLQI, CADI and BDI) of young women with AV.
2. Materials and Methods
2.1. Study Population and Data Collection
The study group included 165 young women with AV. All the subjects agreed to participate in this study. The inclusion criteria were as follows: age 18–35 years, presence of acne vulgaris, a diet with a caloric value 500–5000 kcal. The exclusion criteria were as follows: age below 18 years and above 35 years, a diet with a caloric value below 500 kcal and above 5000 kcal, the presence of other skin diseases (rosacea, psoriasis, eczema). Acne was classified by a dermatologist and cosmetologist according to the GAGS (Global Acne Grading Scale) [18,19].
A self-report survey was used to collect baseline data on the subjects’ sociodemographic status, anthropometric information, lifestyle, and acne. On this basis, data were collected regarding body weight, height, level of education, work/study, marital status, smoking, alcohol consumption, and information about acne. The commonly known formula [body weight (kg)/height (m)2] was used to calculate BMI (body mass index). The level of physical activity was assessed using the IPAQ (International Physical Activity Questionnaire) and classified as a low, moderate, and high level of physical activity [20].
The tests assessing the QoL are presented in Table 1.
Food intake was assessed based on 3-day food diaries (two randomly selected weekdays and one weekend day). The participants recorded all the foods and drinks that they consumed during each day of the study. Then, the results from the food diaries were calculated using the Diet 6.0 program. On this basis, the energy value and the content of some vitamins and minerals in the diet were estimated. The selenium, polyphenols, phytosterols, lignans, and antioxidant potential of the diet are not included in this computer program, so we used available databases [26].
2.2. Antioxidant Power of a Diet
The DAQI (dietary antioxidant quality index) described in our previous study was used to assess the antioxidant power of the diet [26]. The DAQI scale consists of the following dietary elements: β-carotene, vitamin C, vitamin E, selenium, iron, zinc, copper, manganese, dietary antioxidant capacity, lignans, polyphenols, and phytosterols. Due to the fact that diets contain a variety of antioxidants, we have developed an index of 12 dietary antioxidants. The minerals included in this index are components of antioxidant enzymes (glutathione peroxidase, superoxide dismutase, and catalase).
The cut-off values of the dietary components are presented in Table 2. The RDA (recommended dietary allowances) for vitamin C, iron, zinc, copper, selenium, and AI (adequate intake) for vitamin E and manganese were adopted in accordance with the nutrition standards of the Polish population [27]. The values that were ≥90% RDA/AI were accepted as normal intake, and values < 90% RDA/AI were classified as abnormal intake. For the remaining dietary components for which no nutrition standards were defined (β-carotene, lignans, phytosterols, polyphenols, and dietary antioxidant potential), values above and below the median were adopted after conversion to a 1000 kcal diet.
2.3. Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics v. 27.0 software (SPSS Inc., Chicago, IL, USA), and a p value of less than 0.05 was accepted as significant. The continuous variables were described as means (M) and standard deviations (SD), whereas the categorical variables were presented as counts (N) with percentages (%). We used the following statistic tests: Mann–Whitney–Wilcoxon, Kruskal–Wallis, and Pearson’s chi-squared. The participants were divided into three groups according to their DAQI tertiles. To assess the association between QoL and DAQI tertiles, multivariate logistic regression models were used. The data are illustrated as odds ratios (ORs) and 95% confidence intervals (CIs). Three models were developed: Model 1—crude data, Model 2—data adjusted for age and daily energy intake; Model 3—data adjusted for variables in Model 2 and BMI, level of physical activity, smoking, and severity of acne.
3. Results
Table 3 showed the general characteristics of the study population (young women with acne vulgaris).
The mean age of the women was 23.65 ± 6.24 (range: 18–35) years. In the study group, 88% were single, 76% were learning, and 65% had middle level of education. Most of the participants had an average BMI (75%), moderate physical activity (55%), and occasionally drank alcohol (58%). However, a large group of women (44%) had a low level of physical activity, 26% smoked cigarettes, 42% drank alcohol once a week or more often, and 14% were overweight. Over 52% of the women had struggled with acne vulgaris for 2 to 5 years, and 27% for over 5 years. Only 20% of the women had acne for less than 2 years. Among the participants, 37% had mild and 54% moderate acne severity. Severe acne affected a small percentage of the study population (9%).
The results of the QoL assessment tests are shown in Table 4. The mean CADI value was 8.14 ± 4.25, indicating a moderate impairment in QoL. In this test, 41% of women declared moderate impairment, 56% no or mild impairment, and only 3% severe impairment.
The mean DLQI value was 9.52 ± 4.36, which confirmed the moderate effect of acne on the QoL. In the DLQI test, 47% of the participants indicated a moderate effect of acne on their QoL, 42% no effect or a small effect, while 11% reported a very large or extremely large effect of acne on their QoL.
The mean SWLS value was average (20.32 ± 4.56). In the SWLS test, 40% of the women had an average life satisfaction, but 28% had a low life satisfaction, and 32% high a life satisfaction.
The mean BDI value indicated the absence of depression in the study group (9.75 ± 6.31). No depression was detected in 70% of the women. However, 25% of the participants had mild depression and 5% had moderate or severe depression.
Figure 1 illustrates the results of the CADI, DLQI, SWLS, and BDI measurements.
The calculation results of the DAQI are presented in Table 5. The obtained results indicate the average antioxidant power of the diet. Most of the participants consumed vitamins and minerals in amounts that were lower than recommended. Similarly, the dietary intake of phytosterols, polyphenols, and lignans and the antioxidant potential of the diet of most of the women were below the median. Only approximately 50% of the subjects consumed β-carotene above the median.
Table 6 illustrates the relationships between the study population characteristics and DAQI tertiles. It was found that DAQI was significantly related to age (p = 0.011), BMI (p = 0.009), energy of diet (p < 0.001), physical activity (p < 0.001), smoking (p < 0.001), and the severity of acne lesions (p = 0.024). There was no association between DAQI and education, working status, marital status, and alcohol intake.
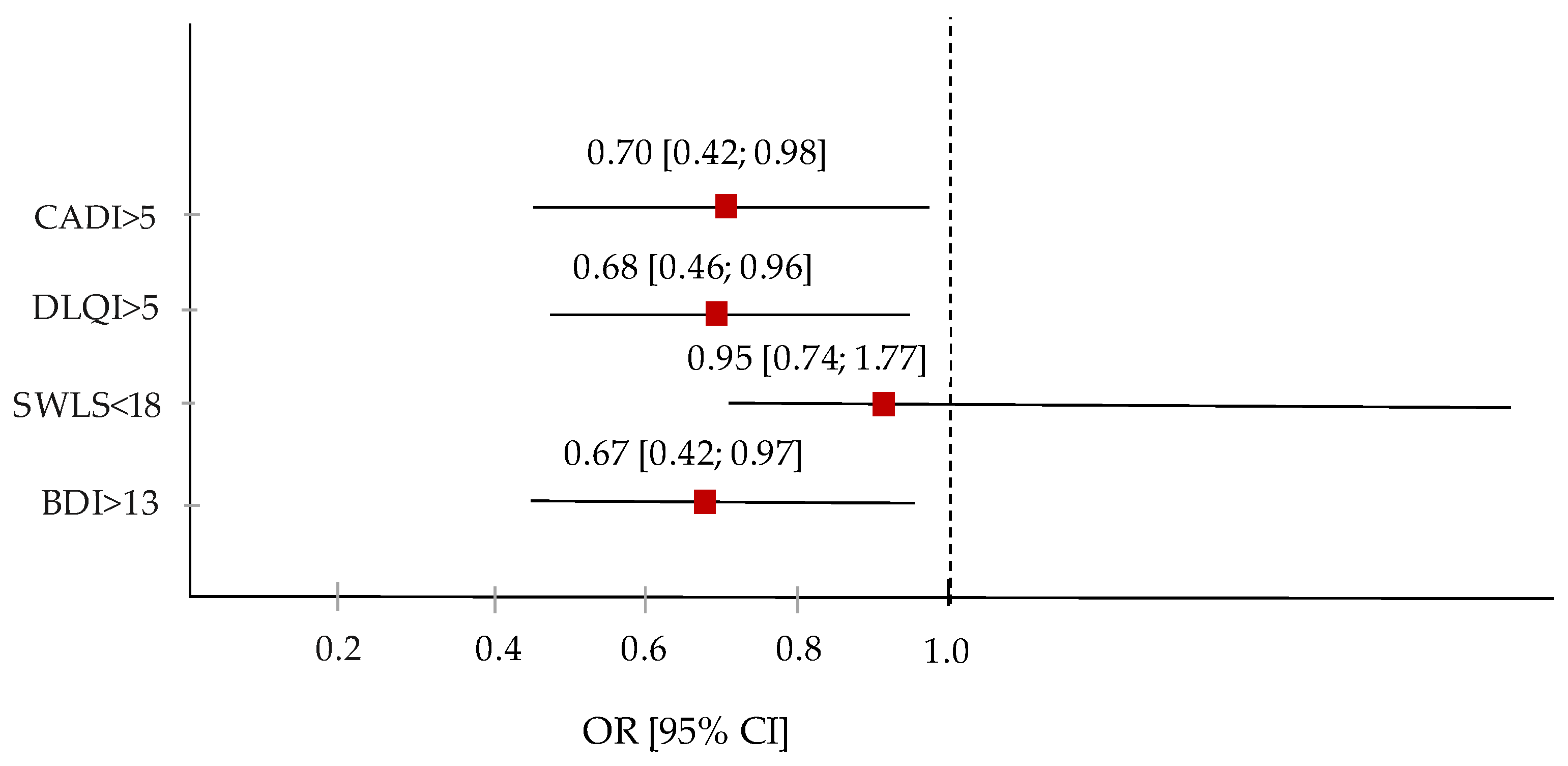
The relationships between DAQI and QoL are presented in Table 7. In Models 1, 2, and 3, the highest tertiles of DAQI compared to the first tertiles reduced the risk of moderate and severe QoL impairment by approximately 30%, as measured by the CADI score (Model 3: OR = 0, 70, 95% CI: 0.42–0.98) and approximately 32% of the moderate, very large, and extremely large impact of acne on the QoL measured based on the DLQI scale (Model 3: OR = 0.68, 95% CI: 0.46 –0.96). Moreover, the highest DAQI tertiles reduced the risk of depression by approximately 33% (Model 3: OR = 0.67, 95% CI: 0.42–0.97). No association was found for SWLS and DAQI.
Figure 2 illustrates the odds ratio of the reduced impact of acne vulgaris on quality of life with increasing antioxidant diet quality index.
4. Discussion
Acne vulgaris is a serious social problem that most often affects young people and significantly reduces their quality of life. Therefore, identifying factors that can improve the QoL of people with AV is an important element of modern medicine [28]. It has been proven that only holistic patient care, taking into account physical and emotional aspects, can bring beneficial results [6]. In this study, AV had a moderate impact on the participants’ QoL, as measured by the CADI and DLQI questionnaires. Additionally, the respondents had an average satisfaction with their life as measured by the SWLS questionnaire. Moreover, almost one-third of the subjects showed depression, mostly mild, as measured by the BDI questionnaire. This study included young women aged 18–35, mainly with mild and moderate acne, for whom the condition of the skin is very important. Some authors have shown that in a group of young people, a greater reduction in QoL due to acne was associated with the severity of acne and the female gender [29].
In the prevention and treatment of AV, an important role is played by modifiable lifestyle factors, including an average BMI, moderate physical activity, avoiding smoking and drinking alcohol, and proper eating habits. In our study, a large group of respondents led an unhealthy lifestyle due to smoking, alcohol drinking, and low physical activity. Moreover, most of the participants’ intake of dietary antioxidants (vitamins and minerals) was below the dietary recommendations.
Some authors have shown that a higher BMI is associated with the occurrence of AV due to a higher glycemic load and higher levels of androgens, which cause greater sebum production [30]. However, in our study, as many as three quarters of the participants had an average BMI, and only 14% were overweight.
Smoking causes significant changes in skin microcirculation, keratinocytes, and the synthesis of collagen and elastin, and it also delays wound healing and accelerates skin aging [31]. Moreover, it causes peroxidation of skin lipids [32]. In this study, a quarter of the subjects smoked cigarettes.
The results of other studies have shown that the habit of drinking alcohol is a predisposing factor to the occurrence of acne [33]. Alcohol increases the production of pro-inflammatory cytokines and suppresses the immune system, which leads to changes in the skin microbiome [34]. In our study, almost half of the young women reported drinking alcohol once a week or more often.
It is well known that regular, moderate physical activity has a positive effect on overall health and improves the condition of the skin, its ability to retain moisture, and prevents future skin problems [35]. In our study, almost half of the participants had a low level of physical activity.
The relationship between diet and skin conditions has been studied for a long time. Diet influences the AV through the immune and hormonal system, gut microbiota, and carbohydrate and lipid metabolism. Epidemiological studies indicate that the prevalence of AV is lower in developing countries compared to highly developed countries. The typical Western diet, rich in ultra-processed foods with sugar, saturated fatty acids, and food additives (chemical preservatives, synthetic colorants, flavor enhancers) with a high glycemic index and being poor in polyunsaturated fatty acids, fiber, water, vitamins, and minerals, can predispose individuals to the development of AV [10,36,37]. Many studies have shown that an improper diet has a pro-inflammatory effect and contributes to the disruption of the diversity of the gut microbiome, influencing the development of chronic diseases including dermatological diseases [38,39,40]. Healthy dietary patterns, such as the Mediterranean diet, have been shown to have a protective role in the pathogenesis of acne vulgaris [41,42,43,44]. However, some studies do not confirm this relationship [45].
This study examined for the first time the relationship between the dietary antioxidant quality index and the quality of life of patients with acne vulgaris. The mean DAQI was found to be 8.2 ± 4.8, indicating a moderate antioxidant power of the diet. People with a higher DAQI had a healthier lifestyle, i.e., they had a lower BMI, moderate physical activity, and did not smoke cigarettes. Moreover, a higher DAQI was associated with lower AV severity. In fully adjusted models, regardless of confounding variables, the highest tertiles of DAQI reduced the risk of AV impact on QoL by approximately 30–33%.
The new DAQI was developed by taking into account various antioxidants such as dietary vitamins, carotenoids, minerals, polyphenols, phytosterols, lignans, and the total antioxidant capacity of the diet. Previous research by other authors has shown the beneficial effects of individual antioxidants on the condition of the skin. It was found that plasma levels of vitamins E, A, selenium, and zinc were lower in AV patients compared to the control group [46,47,48]. Moreover, polyphenols inhibited sebum production, lipogenesis, and proliferation of sebaceous cells and had a bactericidal effect on P. acnes [49,50]. Vitamin C was also widely used in skin diseases. It prevented photoaging, discoloration, and tissue inflammation, supported tissue healing, and stimulated collagen production [51]. Oxidative stress in AV is manifested by changes in the activity of antioxidant enzymes, whose cofactors are minerals such as zinc, selenium, copper, manganese, and iron [52]. During oxidative stress, the level of antioxidant systems is exceeded, which causes a change in the function and molecular composition of keratinocytes and sebaceous cells and contributes to the progression of the inflammatory process [53].
The pathogenesis of acne vulgaris is not fully known. However, the determination of oxidative stress biomarkers, especially lipid peroxidation in acne patients, confirms the important role of oxidative stress. Inflammation caused by oxidative stress of the pilosebaceous unit and oxidation of sebum initiates the development of acne [54]. A well-composed diet is a source of various antioxidants (vitamins, minerals, polyphenols) that may support the treatment of acne and improve quality of life [55].
Limitations
This study has some limitations. First, food intake was assessed based on 3-day food diaries, which did not take into account usual eating habits. Second, the available databases on dietary antioxidant potential, selenium, polyphenols, lignans, and phytosterols did not include all foods and dishes, so we used similar products to calculate any missing data.
The strength of this study is that a new index was used to assess the antioxidant power of the diet. Moreover, standardized questionnaires were used to assess the QoL of young women with AV. Furthermore, the relationship between QoL and dietary antioxidants is rarely studied.
5. Conclusions
The results of this study showed that the QoL of young women with AV is impaired. However, greater adherence to an antioxidant diet reduces the risk of AV impact on QoL by approximately 30–32% and the risk of depression by 33%. The DAQI may be used as a new indicator of diet quality in acne vulgaris.
Author Contributions
Conceptualization, M.E.Z.; methodology, M.E.Z., K.Z.-K. and B.J.; formal analysis, M.E.Z.; investigation, M.E.Z.; data curation, M.E.Z. and B.J.; writing—original draft preparation, M.E.Z. and K.Z.-K.; writing—review and editing, B.J.; visualization, M.E.Z. and K.Z.-K.; supervision, M.E.Z.; project administration, M.E.Z.; funding acquisition, M.E.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by statutory grant from Medical University of Białystok, Poland.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Łomża University Ethics Committee (No. 517301, 8 May 2017).
Informed Consent Statement
Informed consent was obtained from all the subjects involved in this study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to due to the protection of personal data of research participants.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Chen, H.; Zhang, T.C.; Yin, X.L.; Man, J.Y.; Yang, X.R.; Lu, M. Magnitude and temporal trend of acne vulgaris burden in 204 countries and territories from 1990 to 2019: An analysis from the Global Burden of Disease Study 2019. Br. J. Dermatol. 2022, 186, 673–683. [Google Scholar] [CrossRef] [PubMed]
- Heng, A.H.S.; Chew, F.T. Systematic review of the epidemiology of acne vulgaris. Sci. Rep. 2020, 10, 5754. [Google Scholar] [CrossRef] [PubMed]
- Richard, M.A.; Paul, C.; Nijsten, T.; Gisondi, P.; Salavastru, C.; Taieb, C.; Trakatelli, M.; Puig, L.; Stratigos, A. EADV burden of skin diseases project team. Prevalence of most common skin diseases in Europe: A population-based study. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 1088–1096. [Google Scholar] [CrossRef]
- Zaenglein, A.L. Acne vulgaris. N. Engl. J. Med. 2018, 379, 1343–1352. [Google Scholar] [CrossRef]
- Jankowska, B.; Zujko, M.E. The effectiveness of pyruvic acid peeling in improving the quality of life of patients with acne vulgaris. J. Clin. Med. 2023, 12, 3592. [Google Scholar] [CrossRef] [PubMed]
- Morshed, A.S.M.; Noor, T.; Uddin Ahmed, M.A.; Mili, F.S.; Ikram, S.; Rahman, M.; Ahmed, S.; Uddin, M.B. Understanding the impact of acne vulgaris and associated psychological distress on self-esteem and quality of life via regression modeling with CADI, DLQI, and WHOQoL. Sci. Rep. 2023, 13, 21084. [Google Scholar] [CrossRef] [PubMed]
- Heng, A.H.S.; Say, Y.H.; Sio, Y.Y.; Ng, Y.T.; Chew, F.T. Epidemiological risk factors associated with acne vulgaris presentation, severity, and scarring in a Singapore Chinese population: A cross-sectional study. Dermatology 2022, 238, 226–235. [Google Scholar] [CrossRef]
- Baldwin, H.; Tan, J. Effects of diet on acne and its response to treatment. Am. J. Clin. Dermatol. 2021, 22, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Penso, L.; Touvier, M.; Deschasaux, M.; Szabo de Edelenyi, F.; Hercberg, S.; Ezzedine, K.; Sbidian, E. Association between adult acne and dietary behaviors: Findings from the NutriNet-Santé prospective cohort study. JAMA Dermatol. 2020, 156, 854–862. [Google Scholar] [CrossRef]
- Meixiong, J.; Ricco, C.; Vasavda, C.; Ho, B.K. Diet and acne: A systematic review. JAAD Int. 2022, 7, 95–112. [Google Scholar] [CrossRef]
- Łożyńska, K.; Głąbska, D. Association between nutritional behaviours and acne-related quality of life in a population of Polish male adolescents. Nutrients 2022, 14, 2677. [Google Scholar] [CrossRef] [PubMed]
- Bungau, A.F.; Radu, A.F.; Bungau, S.G.; Vesa, C.M.; Tit, D.M.; Endres, L.M. Oxidative stress and metabolic syndrome in acne vulgaris: Pathogenetic connections and potential role of dietary supplements and phytochemicals. Biomed. Pharmacother. 2023, 164, 115003. [Google Scholar] [CrossRef]
- Zujko, M.E.; Waśkiewicz, A.; Drygas, W.; Cicha-Mikołajczyk, A.; Zujko, K.; Szcześniewska, D.; Kozakiewicz, K.; Witkowska, A.M. Dietary habits and dietary antioxidant intake are related to socioeconomic status in Polish adults: A nationwide study. Nutrients 2020, 12, 518. [Google Scholar] [CrossRef]
- Cyuńczyk, M.; Zujko, M.E.; Jamiołkowski, J.; Zujko, K.; Łapińska, M.; Zalewska, M.; Kondraciuk, M.; Witkowska, A.M.; Kamiński, K.A. Dietary total antioxidant capacity is inversely associated with prediabetes and insulin resistance in Bialystok PLUS population. Antioxidants 2022, 11, 283. [Google Scholar] [CrossRef]
- Zujko, M.E.; Rożniata, M.; Zujko, K. Individual diet modification reduces the metabolic syndrome in patients before pharmacological treatment. Nutrients 2021, 13, 2102. [Google Scholar] [CrossRef]
- Podgórska, A.; Puścion-Jakubik, A.; Markiewicz-Żukowska, R.; Gromkowska-Kępka, K.J.; Socha, K. Acne vulgaris and intake of selected dietary nutrients—A summary of information. Healthcare 2021, 9, 668. [Google Scholar] [CrossRef] [PubMed]
- Guo, M.; An, F.; Wei, X.; Hong, M.; Lu, Y. Comparative effects of Schisandrin A, B, and C on acne-related inflammation. Inflammation 2017, 40, 2163–2172. [Google Scholar] [CrossRef] [PubMed]
- Doshi, A.; Zaheer, A.; Stiller, M.J. A comparison of current acne grading systems and proposal of a novel system. Int. J. Dermatol. 1997, 36, 416–418. [Google Scholar] [CrossRef]
- Zaenglein, A.L.; Pathy, A.L.; Schlosser, B.J.; Alikhan, A.; Baldwin, H.E.; Berson, D.S.; Bowe, W.P.; Graber, E.M.; Harper, J.C.; Kang, S.; et al. Guidelines of care for the management of acne vulgaris. J. Am. Acad. Dermatol. 2016, 74, 945–973.e33. [Google Scholar] [CrossRef]
- Biernat, E.; Stupnicki, R.; Gajewski, A.K. Międzynarodowy Kwestionariusz Aktywności Fizycznej (IPAQ)—Wersja Polska [International Physical Activity Questionnaire (IPAQ)—Polish Version]. Wychow. Fiz. Sport [Phys. Educ. Sport] 2007, 51, 47–54. (In Polish) [Google Scholar]
- Motley, R.J.; Finlay, A.Y. Practical use of a disability index in the routine management of acne. Clin. Exp. Dermatol. 1992, 17, 1–3. [Google Scholar] [CrossRef]
- Abdelrazik, Y.T.; Ali, F.M.; Salek, M.S.; Finlay, A.Y. Clinical experience and psychometric properties of the Cardiff Acne Disability Index (CADI). Br. J. Dermatol. 2021, 185, 711–724. [Google Scholar] [CrossRef]
- Finlay, A.Y.; Khan, G.K. Dermatology Life Quality Index (DLQI)—A simple practical measure for routine clinical use. Clin. Exp. Dermatol. 1994, 19, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Pavot, W.; Diener, E. Review of the satisfaction with life scale. Psychol. Assess. 1993, 5, 164–172. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Zujko-Kowalska, K.; Masłowska, J.; Knaś-Dawidziuk, M.; Hamulka, J.; Zujko, M.E. Dietary antioxidants may support cosmetic treatment in patients with rosacea. Antioxidants 2024, 13, 381. [Google Scholar] [CrossRef]
- Jarosz, M.; Rychlik, E.; Stoś, K.; Charzewska, J. Normy Żywienia dla Populacji Polski i ich Zastosowanie [Nutrition Standards for the Polish Population and Their Application]; National Institute of Public Health-National Institute of Hygiene: Warsaw, Poland, 2020.
- Gupta, A.; Sharma, Y.K.; Dash, K.N.; Chaudhari, N.D.; Jethani, S. Quality of life in acne vulgaris: Relationship to clinical severity and demographic data. Indian J. Dermatol. Venereol. Leprol. 2016, 82, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Dabash, D.; Salahat, H.; Awawdeh, S.; Hamadani, F.; Khraim, H.; Koni, A.A.; Zyoud, S.H. Prevalence of acne and its impact on quality of life and practices regarding self-treatment among medical students. Sci. Rep. 2024, 14, 4351. [Google Scholar] [CrossRef]
- Witkam, W.C.A.M.; Dal Belo, S.E.; Pourhamidi, S.; Raynaud, E.; Moreau, M.; Aguilar, L.; Jansen, P.W.; Nijsten, T.E.C.; Pardo, L.M. The epidemiology of acne vulgaris in a multiethnic adolescent population from Rotterdam, the Netherlands: A cross-sectional study. J. Am. Acad. Dermatol. 2024, 90, 552–560. [Google Scholar] [CrossRef]
- Capitanio, B.; Sinagra, J.L.; Ottaviani, M.; Bordignon, V.; Amantea, A.; Picardo, M. Acne and smoking. Dermato-Endocrinology 2009, 1, 129–135. [Google Scholar] [CrossRef]
- Pelle, E.; Miranda, E.P.; Fthenakis, C.; Mammone, T.; Marenus, K.; Maes, D. Cigarette smoke-induced lipid peroxidation in human skin and its inhibition by topically applied antioxidants. Skin. Pharmacol. Appl. Skin Physiol. 2002, 15, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Say, Y.H.; Heng, A.H.S.; Reginald, K.; Wong, Y.R.; The, K.F.; Rawanan Shah, S.M.; Sio, Y.Y.; Ng, Y.T.; Matta, S.A.; Pang, S.L.; et al. Modifiable and non-modifiable epidemiological risk factors for acne, acne severity and acne scarring among Malaysian Chinese: A cross-sectional study. BMC Public Health 2021, 21, 601. [Google Scholar] [CrossRef]
- Dreno, B.; Shourick, J.; Kerob, D.; Bouloc, A.; Taïeb, C. The role of exposome in acne: Results from an international patient survey. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Ryosuke, O.; Yoshie, S.; Hiromi, A. The association between activity levels and skin moisturizing function in adults. Dermatol. Rep. 2021, 13, 8811. [Google Scholar]
- Kucharska, A.; Szmurło, A.; Sińska, B. Significance of diet in treated and untreated acne vulgaris. Adv. Dermatol. Allergol. 2016, 33, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Kowalska, H.; Sysa-Jędrzejowska, A.; Woźniacka, A. Role of diet in the aetiopathogenesis of acne. Dermatol. Rev. 2018, 105, 51–62. [Google Scholar]
- Ilaria, P.; Ersilia, T.; Nicoletta, B.; Federica, T.; Andrea, V.; Nevena, S.; Concetta, P. The role of the Western diet on atopic dermatitis: Our experience and review of the current literature. Nutrients 2023, 15, 3896. [Google Scholar] [CrossRef] [PubMed]
- Manzel, A.; Muller, D.N.; Hafler, D.A.; Erdman, S.E.; Linker, R.A.; Kleinewietfeld, M. Role of “Western diet” in inflammatory autoimmune diseases. Curr. Allergy Asthma Rep. 2014, 14, 404. [Google Scholar] [CrossRef]
- Zinöcker, M.K.; Lindseth, I.A. The Western diet–microbiome-host interaction and its role in metabolic disease. Nutrients 2018, 10, 365. [Google Scholar] [CrossRef]
- Skroza, N.; Tolino, E.; Semyonov, L.; Proietti, I.; Bernardini, N.; Nicolucci, F.; La Viola, G.; Del Prete, G.; Saulle, R.; Potenza, C.; et al. Mediterranean diet and familial dysmetabolism as factors influencing the development of acne. Scand. J. Public Health 2012, 40, 466–474. [Google Scholar] [CrossRef]
- Ah-Thiane, L.; Nguyen, J.M.; Khammari, A.; Dréno, B. Lifestyle habits and impact of the Mediterranean diet on facial acne severity in French women: A case-control study. Int. J. Women’s Dermatol. 2022, 8, e017. [Google Scholar] [CrossRef] [PubMed]
- Bertolani, M.; Rodighiero, E.; Saleri, R.; Pedrazzi, G.; Bertoli, S.; Leone, A.; Feliciani, C.; Lotti, T.; Satolli, F. The influence of Mediterranean diet in acne pathogenesis and the correlation with insulin-like growth factor-1 serum levels: Implications and results. Dermatol. Rep. 2021, 14, 9143. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Donnarumma, M.; Cacciapuoti, S.; Muscogiuri, G.; De Gregorio, L.; Blasio, C.; Savastano, S.; Colao, A.; Fabbrocini, G. Phase angle and Mediterranean diet in patients with acne: Two easy tools for assessing the clinical severity of disease. J. Transl. Med. 2021, 19, 171. [Google Scholar] [CrossRef] [PubMed]
- Taha, S.; Shakhshir, M.; Zyoud, S.H. Acne vulgaris and adherence to the Mediterranean diet among university students: A case-control study. J. Health Popul. Nutr. 2024, 43, 41. [Google Scholar] [CrossRef] [PubMed]
- El-Akawi, Z.; Abdel-Latif, N.; Abdul-Razzak, K. Does the plasma level of vitamins A and E affect acne condition? Clin. Exp. Dermatol. 2006, 31, 430–434. [Google Scholar] [CrossRef]
- Bowe, W.P.; Joshi, S.S.; Shalita, A.R. Diet and acne. J. Am. Acad. Dermatol. 2010, 63, 124–141. [Google Scholar] [CrossRef] [PubMed]
- Yee, B.E.; Richards, P.; Sui, J.Y.; Marsch, A.F. Serum zinc levels and efficacy of zinc treatment in acne vulgaris: A systematic review and meta-analysis. Dermatol. Ther. 2020, 33, e14252. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Takahashi, A.; Kojima, M.; Akimoto, N.; Yano, M.; Ito, A. A citrus polymethoxy flavonoid, nobiletin inhibits sebum production and sebocyte proliferation, and augments sebum excretion in hamsters. J. Investig. Dermatol. 2007, 127, 2740–2748. [Google Scholar] [CrossRef] [PubMed]
- Taylor, E.J.; Yu, Y.; Champer, J.; Kim, J. Resveratrol demonstrates antimicrobial effects against Propionibacterium acnes in vitro. Dermatol. Ther. 2014, 4, 249–257. [Google Scholar] [CrossRef]
- Telang, P.S. Vitamin C in dermatology. Indian Dermatol. Online J. 2013, 4, 143–146. [Google Scholar] [CrossRef]
- Arican, O.; Kurutas, E.B.; Sasmaz, S. Oxidative stress in patients with acne vulgaris. Mediat. Inflamm. 2005, 2005, 380–384. [Google Scholar] [CrossRef] [PubMed]
- Popa, G.L.; Mitran, C.I.; Mitran, M.I.; Tampa, M.; Matei, C.; Popa, M.I.; Georgescu, S.R. Markers of oxidative stress in patients with acne: A literature review. Life 2023, 13, 1433. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.; Zhang, B.; Jiang, M.; Gong, E.; Zhang, Y.; Lee, S.W. Oxidative stress in acne vulgaris. J. Clin. Dermatol. Ther. 2016, 3, 020. [Google Scholar] [CrossRef] [PubMed]
- Melnik, B.C. Linking diet to acne metabolomics, inflammation, and comedogenesis: An update. Clin. Cosmet. Investig. Dermatol. 2015, 8, 371–388. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Quality of life measured using CADI, DLQI, SWLS, and BDI questionnaires.

Figure 2.
Odds ratio of reduced impact of AV on QoL with increasing DAQI. The red squares and horizontal lines represent the odds ratio (OR) and 95% CI, and the dashed line shows Tecyl 1.
Figure 2.
Odds ratio of reduced impact of AV on QoL with increasing DAQI. The red squares and horizontal lines represent the odds ratio (OR) and 95% CI, and the dashed line shows Tecyl 1.


{kind=link}
{kind=link}
Table 1.
Characteristics of tests for assessing quality of life.
| Tests Assessing the QoL | Points | Outcomes |
|---|---|---|
| CADI [21,22] (Cardiff Acne Disability Index) | 0 | No impairment |
| 1–5 | Mild impairment | |
| 6–10 | Moderate impairment | |
| 11–15 | Severe impairment | |
| DLQI [23] (Dermatology Life Quality Index) | 0–1 | No effect |
| 2–5 | Small effect | |
| 6–10 | Moderate effect | |
| 11–20 | Very large effect | |
| 21–30 | Extremely large effect | |
| SWLS [24] (Satisfaction With Life Scale) | 5–17 | Low satisfaction |
| 18–23 | Average satisfaction | |
| 24–35 | High satisfaction | |
| BDI [25] (Beck Depression Inventory) | 0–13 | No depression |
| 14–19 | Mild depression | |
| 20–28 | Moderate depression | |
| 29–63 | Severe depression |
Table 2.
The cut-off values of the dietary components of DAQI.
| Dietary Components | Score 1 | Score 0 |
|---|---|---|
| DTAC/1000 kcal [mmol] | ≥Me | <Me |
| DP/1000 kcal [mg] | ≥Me | <Me |
| DPH/1000 kcal | ≥Me | <Me |
| DL/1000 kcal | ≥Me | <Me |
| β-carotene/1000 kcal [µg] | ≥Me | <Me |
| Vitamin E [mg] | ≥90% AI (≥7.2) | <90% AI (<7.2) |
| Vitamin C [mg] | ≥90% RDA (≥67.5) | <90% RDA (<67.5) |
| Iron [mg] | ≥90% RDA (≥16.2) | <90% RDA (<16.2) |
| Zinc [mg] | ≥90% RDA (≥7.2) | <90% RDA (<7.2) |
| Copper [mg] | ≥90% RDA (≥0.81) | <90% RDA (<0.81) |
| Manganese [mg] | ≥90% AI (≥1.62) | <90% AI (<1.62) |
| Selenium [µg] | ≥90% RDA (≥49.5) | <90% RDA (<49.5) |
| Overall score | Minimum 12 | Maximum 0 |
Me—median, RDA—recommended dietary allowances, AI—adequate intake, DL—dietary lignans, DTAC—dietary total antioxidant capacity, DP—dietary polyphenols, DPH—dietary phytosterols.
Table 3.
General characteristics of the studied group with acne.
| Variable | Women |
|---|---|
| Age (year), X ± SD (range) | 23.65 ± 6.24 (18–35) |
| BMI (kg/m2), X ± SD (range) | 24.35 ± 6.22 |
| BMI, N (%) | |
| Underweight (<18.5 kg/m2) | 18 (10.91) |
| Normal (18.5–24.9 kg/m2) | 124 (75.15) |
| Overweight (25.0–29.9 kg/m2) | 23 (13.94) |
| Level of education, N (%) | |
| Higher | 48 (29.09) |
| Middle | 107 (64.85) |
| Bellow middle | 10 (6.06) |
| Working status, N (%) | |
| Working | 37 (22.42) |
| Learning | 126 (76.36) |
| Not working and learning | 2 (1.22) |
| Marital status, N (%) | |
| Married/cohabiting | 20 (12.12) |
| Single | 145 (87.88) |
| Physical activity, N (%) | |
| High level | 3 (1.81) |
| Moderate level | 90 (54.55) |
| Low level | 72 (43.64) |
| Smoking, N (%) | 43 (26.06) |
| Alcohol intake, N (%) | |
| More than once a week | 27 (16.36) |
| Once a week | 42 (25.45) |
| Occasionally or never | 96 (58.19) |
| Acne duration (years), N (%) | |
| <2 | 33 (20.00) |
| 2–5 | 87 (52.73) |
| >5 | 45 (27.27) |
| Acne severity, N (%) | |
| Mild | 61 (36.97) |
| Moderate | 89 (53.94) |
| Severe | 15 (9.09) |
X—mean; SD—standard deviation; N—number; BMI—body mass index.
Table 4.
Tests assessing the quality of life.
| QoL Scores | Results |
|---|---|
| CADI, X ± SD | 8.14 ± 4.25 |
| No impairment, N (%) | 45 (27.27) |
| Mild impairment, N (%) | 48 (29.09) |
| Moderate impairment, N (%) | 67 (40.61) |
| Severe impairment, N (%) | 5 (3.03) |
| DLQI, X ± SD | 9.52 ± 4.36 |
| No effect, N (%) | 26 (15.76) |
| Small effect, N (%) | 43 (26.06) |
| Moderate effect, N (%) | 78 (47.27) |
| Very large effect, N (%) | 15 (9.09) |
| Extremely large effect, N (%) | 3 (1.82) |
| SWLS, X ± SD | 20.32 ± 4.56 |
| Low satisfaction, N (%) | 46 (27.88) |
| Average satisfaction, N (%) | 66 (40.00) |
| High satisfaction, N (%) | 53 (32.12) |
| BDI, X ± SD | 9.75 ± 6.31 |
| No depression, N (%) | 115 (69.70) |
| Mild depression, N (%) | 42 (25.45) |
| Moderate depression, N (%) | 5 (3.03) |
| Severe depression, N (%) | 3 (1.82) |
X—mean; SD—standard deviation; N—number; QoL—quality of life; SWLS—satisfaction with life scale; CADI—Cardiff acne disability index; BDI—Beck depression inventory; DLQI—dermatology life quality index.
Table 5.
Calculation of DAQI.
| No. | Variables | X ± SD | Range | ≥Me, N (%) |
|---|---|---|---|---|
| Energy of diet (kcal/d.) | 1625.7 ± 583.4 | 577.4–4556.6 | - | |
| 1. | DTAC (mmol/d.) | 10.8 ± 7.2 | 4.5–34.8 | - |
| DTAC/1000 kcal | 6.5 ± 4.1 | - | 39 (23.6) | |
| 2. | DP (mg/d.) | 1715.7 ± 583.2 | 543.2–3455.4 | - |
| DP/1000 kcal | 993.8 ± 312.5 | - | 45 (27.3) | |
| 3. | DPH (mg/d.) | 223.5 ± 194.3 | 22.4–623.5 | - |
| DPH/1000 kcal | 137.2 ± 119.5 | - | 51 (30.9) | |
| 4. | DL (µg/d.) | 784.7 ± 545.2 | 27.8–1458.4 | - |
| DL/1000 kcal | 483.1 ± 335.4 | - | 49 (29.7) | |
| 5. | β-carotene (µg/d.) | 3462.4 ± 2345.2 | 135.2–6556.7 | - |
| β-carotene/1000 kcal | 2130.5 ± 1376.5 | - | 87 (52.7) | |
| Variables | X ± SD | Range | ≥90% RDA, N (%) | |
| 6. | Vitamin C (mg/d.) | 56.5 ± 36.2 | 5.2–267.5 | 42 (25.5) |
| 7. | Zinc (mg/d.) | 4.8 ± 3.5 | 1.8–21.4 | 53 (32.1) |
| 8. | Iron (mg/d.) | 7.4 ± 5.5 | 4.2–28.9 | 56 (33.9) |
| 9. | Copper (mg/d.) | 0.7 ± 0.4 | 0.2–3.5 | 68 (41.2) |
| 10. | Selenium (µg/d.) | 33.5 ± 19.3 | 11.5–154.3 | 70 (42.4) |
| Variables | X ± SD | Range | ≥90% AI, N (%) | |
| 11. | Vitamin E (mg/d.) | 6.2 ± 4.48 | 1.65–28.4 | 51 (30.9) |
| 12. | Manganese (mg/d.) | 1.4 ± 1.2 | 0.4–8.5 | 72 (43.6) |
| DAQI, X ± SD (range) | 8.2 ± 4.8 (3–12) | |||
Me—mediane; X—mean; SD—standard deviation; N—number; RDA—recommended dietary allowances; AI—adequate intake; DTAC—dietary total antioxidant capacity; DP—dietary polyphenols; DPH—dietary phytosterols; DL—dietary lignans; DAQI—dietary antioxidant quality index.
Table 6.
Characteristics of the study population based on DAQI tertiles.
| DAQI | p-Value | |||
|---|---|---|---|---|
| T1 (1–4) | T2 (5–8) | T3 (9–12) | ||
| Number of participants | 42 | 85 | 38 | |
| Age (years), X ± SD | 22.25 ± 6.12 | 23.27 ± 6.85 | 24.62 ± 6.24 | 0.011 |
| BMI (kg/m2) | 25.45 ± 5.43 | 24.11 ± 5.47 | 22.67 ± 4.23 | 0.009 |
| Level of education, N (%) | ||||
| Higher | 15 (35.71) | 20 (23.53) | 13 (34.21) | 0.545 |
| Middle | 22 (52.38) | 60 (70.59) | 25 (65.79) | |
| Bellow middle | 5 (11.91) | 5 (5.88) | 0 (0.00) | |
| Working status, N (%) | ||||
| Working | 10 (23.81) | 15 (17.65) | 12 (31.58) | 0.684 |
| Learning | 32 (76.19) | 68 (80.00) | 26 (68.42) | |
| Not working and learning | 0 (0.00) | 2 (2.35) | 0 (0.00) | |
| Marital status, N (%) | ||||
| Married/cohabiting | 5 (11.90) | 10 (11.76) | 5 (13.16) | 0.828 |
| Single | 37 (88.10) | 75 (88.24) | 33 (86.84) | |
| Energy of diet (kcal/d.), X ± SD | 1545.2 ± 534.1 | 1694.2 ± 545.8 | 1843.2 ± 634.5 | <0.001 |
| Physical activity, N (%) | ||||
| High | 0 (0.00) | 0 (0.00) | 3 (7.89) | <0.001 |
| Moderate | 17 (40.48) | 47 (55.29) | 26 (68.43) | |
| Low | 25 (59.52) | 38 (44.71) | 9 (23.68) | |
| Smoking, N (%) | 20 (47.62) | 18 (21.18) | 5 (13.16) | <0.001 |
| Alcohol intake, N (%) | ||||
| More than once a week | 7 (16.67) | 14 (16.47) | 6 (15.79) | 0.576 |
| Once a week | 11 (26.19) | 21 (24.71) | 10 (26.32) | |
| Occasionally | 24 (57.14) | 50 (58.82) | 22 (57.89) | |
| Acne severity, N (%) | ||||
| Mild | 15 (35.71) | 31 (36.47) | 15 (39.47) | 0.024 |
| Moderate | 22 (52.38) | 47 (55.29) | 20 (52.63) | |
| Severe | 5 (11.91) | 7 (8.24) | 3 (7.90) | |
X—mean; SD—standard deviation; T—tertile; N—number; BMI—body mass index; DAQI—dietary antioxidant quality index.
Table 7.
Association between DAQI and QoL.
| DAQI | |||
|---|---|---|---|
| T1 | T2 | T3 | |
| CADI | 9.72 ± 5.28 | 8.43 ± 4.24 | 7.12 ± 4.81 |
| p < 0.001 | |||
| CADI > 5 points | |||
| Model 1 [OR (95% CI)] 1 | 1 | 0.64 (0.52–1.93) | 0.59 (0.44–0.95) * |
| Model 2 [OR (95% CI)] 2 | 1 | 0.67 (0.57–1.85) | 0.62 (0.45–0.97) * |
| Model 3 [OR (95% CI)] 3 | 1 | 0.68 (0.55–1.77) | 0.70 (0.42–0.98) * |
| DLQI | 10.75 ± 6.12 | 9.29 ± 5.67 | 7.94 ± 4.83 |
| p < 0.001 | |||
| DLQI > 5 points | |||
| Model 1 [OR (95% CI)] 1 | 1 | 0.64 (0.54–1.15) | 0.61 (0.45–0.96) * |
| Model 2 [OR (95% CI)] 2 | 1 | 0.65 (0.53–1.23) | 0.63 (0.42–0.95) * |
| Model 3 [OR (95% CI)] 3 | 1 | 0.67 (0.55–1.26) | 0.68 (0.46–0.96) * |
| SWLS | 18.24 ± 5.38 | 21.2 ± 4.93 | 23.45 ± 5.83 |
| p < 0.001 | |||
| SWLS < 18 points | |||
| Model 1 [OR (95% CI)] 1 | 1 | 0.83 (0.57–1.42) | 0.94 (0.65–1.69) |
| Model 2 [OR (95% CI)] 2 | 1 | 0.89 (0.49–1.57) | 0.92 (0.62–1.72) |
| Model 3 [OR (95% CI)] 3 | 1 | 0.96 (0.64–1.68) | 0.95 (0.74–1.77) |
| BDI | 7.42 ± 4.35 | 10.21 ± 5.17 | 13.12 ± 5.85 |
| p < 0.001 | |||
| BDI > 13 points | |||
| Model 1 [OR (95% CI)] 1 | 1 | 0.59 (0.45–0.95) * | 0.61 (0.45–0.96) * |
| Model 2 [OR (95% CI)] 2 | 1 | 0.54 (0.46–1.13) | 0.63 (0.41–0.95) * |
| Model 3 [OR (95% CI)] 3 | 1 | 0.52 (0.48–1.15) | 0.67 (0.42–0.97) * |
OR—odds ratio; CI—confidence interval; 1—crude data, 2—data adjusted for age and daily energy intake, 3—data adjusted for variables in Model 2 and for BMI, smoking, level of physical activity and severity of acne; *—p < 0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Zujko-Kowalska, K.; Jankowska, B.; Zujko, M.E. The Antioxidant Power of a Diet May Improve the Quality of Life of Young Women with Acne Vulgaris. Nutrients 2024, 16, 1270. https://0-doi-org.brum.beds.ac.uk/10.3390/nu16091270
AMA Style
Zujko-Kowalska K, Jankowska B, Zujko ME. The Antioxidant Power of a Diet May Improve the Quality of Life of Young Women with Acne Vulgaris. Nutrients. 2024; 16(9):1270. https://0-doi-org.brum.beds.ac.uk/10.3390/nu16091270
Chicago/Turabian StyleZujko-Kowalska, Kinga, Beata Jankowska, and Małgorzata Elżbieta Zujko. 2024. "The Antioxidant Power of a Diet May Improve the Quality of Life of Young Women with Acne Vulgaris" Nutrients 16, no. 9: 1270. https://0-doi-org.brum.beds.ac.uk/10.3390/nu16091270
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.