
Standard Nutritional Assessment Tools Are Unable to Predict Loss of Muscle Mass in Patients Due to Undergo Pancreatico-Duodenectomy: Highlighting the Need for Detailed Nutritional Assessment
 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
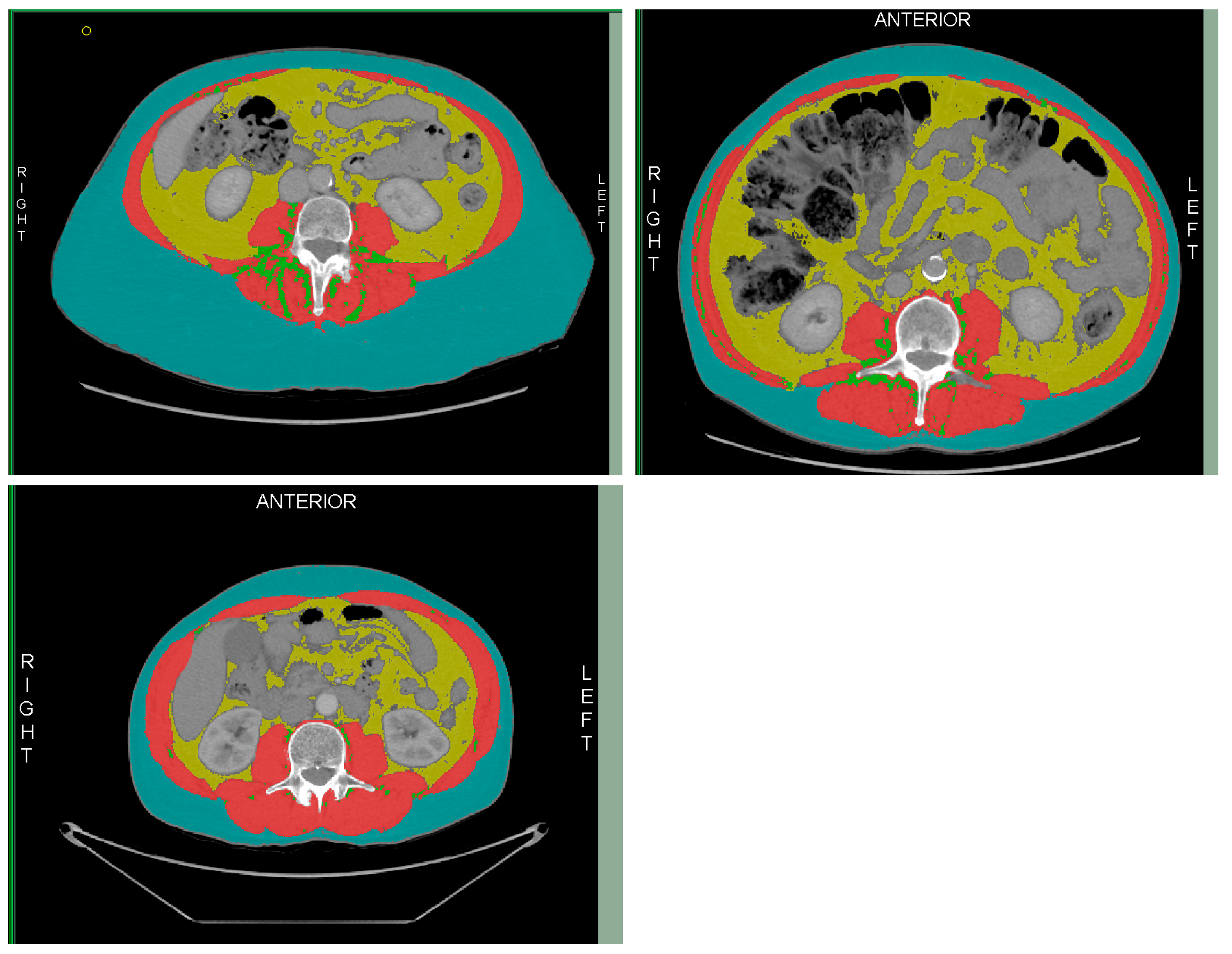
2.1. Technique and Quality Assessment
2.2. Hand-Grip Strength
2.3. Nutritional Markers
- -
- “moderate malnutrition” if there was 5–10% weight loss in 6 months; 10–20% overall weight loss; a BMI < 20 kg/m2 for those under 70 (or <22 kg/m2 for those ≥70 years old) or mild to moderate muscle weakness (low HGS).
- -
- “Severe malnutrition” if there was >10% weight loss in the last 6 months; >20% overall weight loss; a BMI < 18.5 kg/m2 in those under 70 years old (or <20 kg/m2 in those ≥70 years old) or severe muscle function deficit (low HGS) [20].
2.4. Surgical Outcomes
2.5. Statistical Analysis
3. Results
3.1. Demographics
3.2. Complications
3.3. Nutritional Assessment
3.4. Outcome Data
4. Discussion
4.1. Hand-Grip Strength
4.2. Limitations and Areas for Future Research
4.3. Implications for Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kostalas, M.; Nageswaran, H.; Froghi, S.; Riga, A.; Kumar, R.; Menezes, N.; Worthington, T.R.; Karanjia, N.D. Centralisation for resection of the pancreatic head: A comparison of operative factors and early outcomes during the evolving unit and tertiary unit phases at a UK institution. Am. J. Surg. 2018, 216, 310–313. [Google Scholar] [CrossRef] [PubMed]
- Kanhere, H.A.; Trochsler, M.I.; Kanhere, M.H.; Lord, A.N.; Maddern, G.J. Pancreaticoduodenectomy: Outcomes in a low-volume, specialised Hepato Pancreato Biliary unit. World J. Surg. 2014, 38, 1484–1490. [Google Scholar] [CrossRef] [PubMed]
- NHS England. A02/S/a 2013/14 NHS Standard Contract for Hepatobiliary and Pancreas (Adult) Particulars, Schedule 2—The Services, A—Service Specifications; NHS England: Leeds, UK, 2013. [Google Scholar]
- Jones, R.P.; Psarelli, E.E.; Jackson, R.; Ghaneh, P.; Halloran, C.M.; Palmer, D.H.; Campbell, F.; Valle, J.W.; Faluyi, O.; O’Reilly, D.A.; et al. Patterns of Recurrence After Resection of Pancreatic Ductal Adenocarcinoma: A Secondary Analysis of the ESPAC-4 Randomized Adjuvant Chemotherapy Trial. JAMA Surg. 2019, 154, 1038–1048. [Google Scholar] [CrossRef] [PubMed]
- Minnella, E.M.; Awasthi, R.; Loiselle, S.E.; Agnihotram, R.V.; Ferri, L.E.; Carli, F. Effect of Exercise and Nutrition Prehabilitation on Functional Capacity in Esophagogastric Cancer Surgery: A Randomized Clinical Trial. JAMA Surg. 2018, 153, 1081–1089. [Google Scholar] [CrossRef] [PubMed]
- Fukami, Y.; Saito, T.; Arikawa, T.; Osawa, T.; Komatsu, S.; Kaneko, K.; Ishida, Y.; Maeda, K.; Mori, N.; Sano, T. European Society for Clinical Nutrition and Metabolism (ESPEN) Malnutrition Criteria for Predicting Major Complications After Hepatectomy and Pancreatectomy. World J. Surg. 2020, 45, 243–251. [Google Scholar] [CrossRef]
- Shinkawa, H.; Takemura, S.; Uenishi, T.; Sakae, M.; Ohata, K.; Urata, Y.; Kaneda, K.; Nozawa, A.; Kubo, S. Nutritional risk index as an independent predictive factor for the development of surgical site infection after pancreaticoduodenectomy. Surg. Today 2013, 43, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Peng, P.; Hyder, O.; Firoozmand, A.; Kneuertz, P.; Schulick, R.D.; Huang, D.; Makary, M.; Hirose, K.; Edil, B.; Choti, M.A.; et al. Impact of sarcopenia on outcomes following resection of pancreatic adenocarcinoma. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2012, 16, 1478–1486. [Google Scholar] [CrossRef]
- Amini, N.; Spolverato, G.; Gupta, R.; Margonis, G.A.; Kim, Y.; Wagner, D.; Rezaee, N.; Weiss, M.J.; Wolfgang, C.L.; Makary, M.M.; et al. Impact Total Psoas Volume on Short- and Long-Term Outcomes in Patients Undergoing Curative Resection for Pancreatic Adenocarcinoma: A New Tool to Assess Sarcopenia. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2015, 19, 1593–1602. [Google Scholar] [CrossRef]
- Pecorelli, N.; Capretti, G.; Sandini, M.; Damascelli, A.; Cristel, G.; De Cobelli, F.; Gianotti, L.; Zerbi, A.; Braga, M. Impact of Sarcopenic Obesity on Failure to Rescue from Major Complications Following Pancreaticoduodenectomy for Cancer: Results from a Multicenter Study. Ann. Surg. Oncol. 2018, 25, 308–317. [Google Scholar] [CrossRef]
- Bauer, J.; Morley, J.E.; Schols, A.; Ferrucci, L.; Cruz-Jentoft, A.J.; Dent, E.; Baracos, V.E.; Crawford, J.A.; Doehner, W.; Heymsfield, S.B.; et al. Sarcopenia: A Time for Action. An SCWD Position Paper. J. Cachexia Sarcopenia Muscle 2019, 10, 956–961. [Google Scholar] [CrossRef]
- Mourtzakis, M.; Prado, C.M.; Lieffers, J.R.; Reiman, T.; McCargar, L.J.; Baracos, V.E. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl. Physiol. Nutr. Metab. 2008, 33, 997–1006. [Google Scholar] [CrossRef] [PubMed]
- Vogele, D.; Otto, S.; Sollmann, N.; Haggenmuller, B.; Wolf, D.; Beer, M.; Schmidt, S.A. Sarcopenia—Definition, Radiological Diagnosis, Clinical Significance. Rofo 2023, 195, 393–405. [Google Scholar] [CrossRef] [PubMed]
- Contreras-Bolivar, V.; Sanchez-Torralvo, F.J.; Ruiz-Vico, M.; Gonzalez-Almendros, I.; Barrios, M.; Padin, S.; Alba, E.; Olveira, G. GLIM Criteria Using Hand Grip Strength Adequately Predict Six-Month Mortality in Cancer Inpatients. Nutrients 2019, 11, 2043. [Google Scholar] [CrossRef] [PubMed]
- Tomovision. Slice-0-matic Alberta Protocol Users Manual. 2017. Available online: https://tomovision.com/Sarcopenia_Help/index.htm (accessed on 11 February 2024).
- Byrne, C.A.; Zhang, Y.; Fantuzzi, G.; Geesey, T.; Shah, P.; Gomez, S.L. Validation of skeletal muscle and adipose tissue measurements using a fully automated body composition analysis neural network versus a semi-automatic reference program with human correction in patients with lung cancer. Heliyon 2022, 8, e12536. [Google Scholar] [CrossRef]
- van der Werf, A.; Langius, J.A.E.; de van der Schueren, M.A.E.; Nurmohamed, S.A.; van der Pant, K.; Blauwhoff-Buskermolen, S.; Wierdsma, N.J. Percentiles for skeletal muscle index, area and radiation attenuation based on computed tomography imaging in a healthy Caucasian population. Eur. J. Clin. Nutr. 2018, 72, 288–296. [Google Scholar] [CrossRef]
- Ryu, Y.; Shin, S.H.; Kim, J.H.; Jeong, W.K.; Park, D.J.; Kim, N.; Heo, J.S.; Choi, D.W.; Han, I.W. The effects of sarcopenia and sarcopenic obesity after pancreaticoduodenectomy in patients with pancreatic head cancer. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2020, 22, 1782–1792. [Google Scholar] [CrossRef] [PubMed]
- Stratton, R.J.; Hackston, A.; Longmore, D.; Dixon, R.; Price, S.; Stroud, M.; King, C.; Elia, M. Malnutrition in hospital outpatients and inpatients: Prevalence, concurrent validity and ease of use of the ‘malnutrition universal screening tool’ (‘MUST’) for adults. Br. J. Nutr. 2004, 92, 799–808. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Wente, M.N.; Bassi, C.; Dervenis, C.; Fingerhut, A.; Gouma, D.J.; Izbicki, J.R.; Neoptolemos, J.P.; Padbury, R.T.; Sarr, M.G.; Traverso, L.W.; et al. Delayed gastric emptying (DGE) after pancreatic surgery: A suggested definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2007, 142, 761–768. [Google Scholar] [CrossRef]
- Bassi, C.; Marchegiani, G.; Dervenis, C.; Sarr, M.; Abu Hilal, M.; Adham, M.; Allen, P.; Andersson, R.; Asbun, H.J.; Besselink, M.G.; et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 Years After. Surgery 2017, 161, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Wente, M.N.; Veit, J.A.; Bassi, C.; Dervenis, C.; Fingerhut, A.; Gouma, D.J.; Izbicki, J.R.; Neoptolemos, J.P.; Padbury, R.T.; Sarr, M.G.; et al. Postpancreatectomy hemorrhage (PPH): An International Study Group of Pancreatic Surgery (ISGPS) definition. Surgery 2007, 142, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Mukaka, M.M. Statistics corner: A guide to appropriate use of correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar] [PubMed]
- Probst, P.; Haller, S.; Bruckner, T.; Ulrich, A.; Strobel, O.; Hackert, T.; Diener, M.K.; Buchler, M.W.; Knebel, P. Prospective trial to evaluate the prognostic value of different nutritional assessment scores in pancreatic surgery (NURIMAS Pancreas). Br. J. Surg. 2017, 104, 1053–1062. [Google Scholar] [CrossRef] [PubMed]
- Jager-Wittenaar, H.; Ottery, F.D. Assessing nutritional status in cancer: Role of the Patient-Generated Subjective Global Assessment. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Jager-Wittenaar, H.; de Bats, H.F.; Welink-Lamberts, B.J.; Gort-van Dijk, D.; van der Laan, B.; Ottery, F.D.; Roodenburg, J.L.N. Self-Completion of the Patient-Generated Subjective Global Assessment Short Form Is Feasible and Is Associated With Increased Awareness on Malnutrition Risk in Patients with Head and Neck Cancer. Nutr. Clin. Pract. Off. Publ. Am. Soc. Parenter. Enter. Nutr. 2020, 35, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Klassen, P.; Baracos, V.; Gramlich, L.; Nelson, G.; Mazurak, V.; Martin, L. Computed-Tomography Body Composition Analysis Complements Pre-Operative Nutrition Screening in Colorectal Cancer Patients on an Enhanced Recovery after Surgery Pathway. Nutrients 2020, 12, 3745. [Google Scholar] [CrossRef] [PubMed]
- Alhmly, H.F.; Fielding, R.A. A Critical Review of Current Worldwide Definitions of Sarcopenia. Calcif. Tissue Int. 2024, 114, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Ackermans, L.; Rabou, J.; Basrai, M.; Schweinlin, A.; Bischoff, S.C.; Cussenot, O.; Cancel-Tassin, G.; Renken, R.J.; Gomez, E.; Sanchez-Gonzalez, P.; et al. Screening, diagnosis and monitoring of sarcopenia: When to use which tool? Clin. Nutr. ESPEN 2022, 48, 36–44. [Google Scholar] [CrossRef]
- Choi, M.H.; Yoon, S.B.; Lee, K.; Song, M.; Lee, I.S.; Lee, M.A.; Hong, T.H.; Choi, M.G. Preoperative sarcopenia and post-operative accelerated muscle loss negatively impact survival after resection of pancreatic cancer. J. Cachexia Sarcopenia Muscle 2018, 9, 326–334. [Google Scholar] [CrossRef]
- Abe, T.; Amano, H.; Kobayashi, T.; Hanada, K.; Hattori, M.; Nakahara, M.; Ohdan, H.; Noriyuki, T. Preoperative anthropomorphic and nutritious status and fistula risk score for predicting clinically relevant postoperative pancreatic fistula after pancreaticoduodenectomy. BMC Gastroenterol. 2020, 20, 264. [Google Scholar] [CrossRef]
- Pecorelli, N.; Carrara, G.; De Cobelli, F.; Cristel, G.; Damascelli, A.; Balzano, G.; Beretta, L.; Braga, M. Effect of sarcopenia and visceral obesity on mortality and pancreatic fistula following pancreatic cancer surgery. Br. J. Surg. 2016, 103, 434–442. [Google Scholar] [CrossRef]
- Nauheim, D.O.; Hackbart, H.; Papai, E.; Moskal, D.; Yeo, C.J.; Lavu, H.; Nevler, A. Preoperative sarcopenia is a negative predictor for enhanced postoperative recovery after pancreaticoduodenectomy. Langenbeck’s Arch. Surg./Dtsch. Ges. Fur Chir. 2022, 407, 2355–2362. [Google Scholar] [CrossRef]
- Ali, N.A.; O’Brien, J.M., Jr.; Hoffmann, S.P.; Phillips, G.; Garland, A.; Finley, J.C.; Almoosa, K.; Hejal, R.; Wolf, K.M.; Lemeshow, S.; et al. Acquired weakness, handgrip strength, and mortality in critically ill patients. Am. J. Respir. Crit. Care Med. 2008, 178, 261–268. [Google Scholar] [CrossRef]
- Kohler, M.; Olesen, S.S.; Rasmussen, H.H. Body composition predicts clinical outcome in patients with intestinal failure on long-term home parenteral nutrition. Clin. Nutr. ESPEN 2018, 28, 193–200. [Google Scholar] [CrossRef]
- Lakenman, P.; Ottens-Oussoren, K.; Witvliet-van Nierop, J.; van der Peet, D.; de van der Schueren, M. Handgrip Strength Is Associated With Treatment Modifications During Neoadjuvant Chemoradiation in Patients with Esophageal Cancer. Nutr. Clin. Pract. Off. Publ. Am. Soc. Parenter. Enter. Nutr. 2017, 32, 652–657. [Google Scholar] [CrossRef]
- Kimber, J.S.; Woodman, R.J.; Narayana, S.K.; John, L.; Ramachandran, J.; Schembri, D.; Chen, J.W.C.; Muller, K.R.; Wigg, A.J. Association of physiological reserve measures with adverse outcomes following liver transplantation. JGH Open 2022, 6, 132–138. [Google Scholar] [CrossRef]
- Mendes, J.; Alves, P.; Amaral, T.F. Comparison of nutritional status assessment parameters in predicting length of hospital stay in cancer patients. Clin. Nutr. 2014, 33, 466–470. [Google Scholar] [CrossRef]
- Marano, L.; Carbone, L.; Poto, G.E.; Gambelli, M.; Nguefack Noudem, L.L.; Grassi, G.; Manasci, F.; Curreri, G.; Giuliani, A.; Piagnerelli, R.; et al. Handgrip strength predicts length of hospital stay in an abdominal surgical setting: The role of frailty beyond age. Aging Clin. Exp. Res. 2022, 34, 811–817. [Google Scholar] [CrossRef]
- Hillman, T.E.; Nunes, Q.M.; Hornby, S.T.; Stanga, Z.; Neal, K.R.; Rowlands, B.J.; Allison, S.P.; Lobo, D.N. A practical posture for hand grip dynamometry in the clinical setting. Clin. Nutr. 2005, 24, 224–228. [Google Scholar] [CrossRef]
- Bibby, N.; Rajai, A.; O’Reilly, D.A. From prehab to rehab: Nutritional support for people undergoing pancreatic cancer surgery. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2023, 36, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Goonetilleke, K.S.; Hathurusinghe, H.R.; Burden, S.; Siriwardena, A.K. Nutritional and anthropometric assessment of the scope for dietary optimization during staging prior to pancreaticoduodenectomy. JOP J. Pancreas 2008, 9, 415–421. [Google Scholar]
- Werba, G.; Sparks, A.D.; Lin, P.P.; Johnson, L.B.; Vaziri, K. The PrEDICT-DGE score as a simple preoperative screening tool identifies patients at increased risk for delayed gastric emptying after pancreaticoduodenectomy. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2022, 24, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Besselink, M.G.; van Rijssen, L.B.; Bassi, C.; Dervenis, C.; Montorsi, M.; Adham, M.; Asbun, H.J.; Bockhorn, M.; Strobel, O.; Buchler, M.W.; et al. Definition and classification of chyle leak after pancreatic operation: A consensus statement by the International Study Group on Pancreatic Surgery. Surgery 2017, 161, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Belyaev, O.; Munding, J.; Herzog, T.; Suelberg, D.; Tannapfel, A.; Schmidt, W.E.; Mueller, C.A.; Uhl, W. Histomorphological features of the pancreatic remnant as independent risk factors for postoperative pancreatic fistula: A matched-pairs analysis. Pancreatol. Off. J. Int. Assoc. Pancreatol. 2011, 11, 516–524. [Google Scholar] [CrossRef]
- Buehring, B.; Siglinsky, E.; Krueger, D.; Evans, W.; Hellerstein, M.; Yamada, Y.; Binkley, N. Comparison of muscle/lean mass measurement methods: Correlation with functional and biochemical testing. Osteoporos. Int. 2018, 29, 675–683. [Google Scholar] [CrossRef]
- Neidlein, S.; Wirth, R.; Pourhassan, M. Iron deficiency, fatigue and muscle strength and function in older hospitalized patients. Eur. J. Clin. Nutr. 2021, 75, 456–463. [Google Scholar] [CrossRef]
- Deprato, A.; Verhoeff, K.; Purich, K.; Kung, J.Y.; Bigam, D.L.; Dajani, K.Z. Surgical outcomes and quality of life following exercise-based prehabilitation for hepato-pancreatico-biliary surgery: A systematic review and meta-analysis. Hepatobiliary Pancreat. Dis. Int. 2022, 21, 207–217. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Males | Females | |
|---|---|---|
| Skeletal muscle area (cm2) | 134.0 | 89.2 |
| Skeletal muscle index (cm2/m2) | 41.6 | 32 |
| Muscle radiation attenuation (HU) | 29.3 | 22 |
| Demographics | Pre-Operative Nutritional Assessment | ||
|---|---|---|---|
| Patient demographics (n = 184) | MUST score (n = 173) | ||
| Male gender | 102 (55%) | Mean MUST score | 1.2 (SD 1.48) |
| Mean age (SD) | 65.1 (10.5) | MUST ≥ 2 | 57 (33%) |
| Operation type | MUST < 2 | 116 (67%) | |
| Pancreatico-duodenectomy | 152 (83%) | BMI (n = 179) | |
| Full Whipple | 23 (13%) | BMI < 20 kg/m2 | 21 (10%) |
| Total pancreatectomy | 4 (2%) | BMI > 20 kg/m2 | 158 (90%) |
| Additional procedures | BMI > 30 kg/m2 | 21 (10%) | |
| Liver resection | 2 | BMI < 30 kg/m2 | 158 (90%) |
| Vascular resection | 2 | HGS (n = 132) | |
| Hemi-colectomy | 1 | HGS < 85% normal | 59 (45%) |
| Histology | HGS > 85% normal | 73 (55%) | |
| Pancreatic ductal carcinoma | 67 (36%) | GLIM criteria (n = 153) | |
| Cholangiocarcinoma | 25 (14%) | Severe malnutrition | 66 (43%) |
| Cancer of the ampulla | 20 (11%) | Not severe malnutrition | 87 (57%) |
| Chronic pancreatitis | 18 (10%) | Malnutrition | 107 (71%) |
| Intraductal papillary mucinous neoplasm | 15 (8%) | No evidence malnutrition | 46 (29%) |
| Tubular villous adenoma | 13 (7%) | CT analysis (n = 122) | |
| Neuroendocrine tumours | 8 (4%) | Low skeletal muscle index | 29 (24%) |
| Cancer of the duodenum | 8 (4%) | Normal skeletal muscle index | 91 (76%) |
| Bile duct stones/cholangitis | 4 (2%) | High fat to muscle mass ratio (VFA/SMI) | 57 (48%) |
| Familial adenomatous polyposis | 2 | Poor muscle quality | 15 (12%) |
| Brunner’s gland hamartoma | 1 | Normal muscle quality | 106 (88%) |
| Autoimmune pancreatitis | 1 | Weight loss (n = 173) | |
| Gangliocytic paraganglioma | 1 | >5% weight loss | 96 (55%) |
| Surgical Outcome | |||
|---|---|---|---|
| Complications (n = 184) | Other complications | ||
| 30-day/90-day mortality | 2 (1.1%)/2 (1.1%) | Home with NJ feeding | 8 (4%) |
| All Clavien–Dindo scores ≥ 3 | 31 (17%) | Infectious complication | 27 (15%) |
| Re-lapatorotomy | 5 (2.7%) | Chyle leak | 16 (9%) |
| Pancreatic fistula | Post pancreatectomy haemorrhage | 12 (7%) | |
| All | 57 (31%) | Bile leak | 8 (4%) |
| Grade A | 21 (11%) | Parenteral nutrition related complications | |
| Grade B | 30 (16%) | All | 4 (2%) |
| Grade C | 6 (3%) | Line sepsis | 2 |
| Clinically relevant pancreatic fistula | 36 (19%) | Electrolyte imbalance | 1 |
| Delayed gastric emptying | Hypertriglyceridaemia | 1 | |
| All | 33 (18%) | Length of stay | |
| Grade A | 5 (3%) | Median (IQR) | 10 days (7–17) |
| Grade B | 18 (10%) | ||
| Grade C | 10 (5%) | ||
| Risk Score | Risk Score Present | Mean Length of Stay (SD) | Mann–Whitney | Clavien–Dindo Complications ≥ 3 | Chi-Squared |
|---|---|---|---|---|---|
| Whole population | 14.17 (12.0) | 31/185 (17%) | |||
| MUST score (n = 173) | |||||
| MUST ≥ 2 | 57 (33%) | 15.09 (11.7) | p = 0.160 | 8/57 (14%) | p = 0.281 |
| MUST < 2 | 116 (67%) | 13.9 (12.6) | 22/116 (19%) | ||
| Body mass index (BMI) (n = 179) | |||||
| BMI < 20 kg/m2 | 21 (10%) | 12.86 (11.2) | p = 0.915 | 2/21 (10%) | p = 0.271 |
| BMI > 20 kg/m2 | 158 (90%) | 14.42 (12.3) | 28/158 (18%) | ||
| BMI > 30 kg/m2 | 21 (10%) | 20.55 (19.2) | p = 0.131 | 7/21 (33%) | p = 0.039 |
| BMI < 30 kg/m2 | 158 (90%) | 13.48 (10.8) | 23/158 (15%) | ||
| Hand-grip strength (HGS) (n = 132) | |||||
| HGS < 85% normal | 59 (45%) | 13.41 (12.7) | p = 0.905 | 13/60 (22%) | p = 0.114 |
| HGS > 85% normal | 73 (55%) | 12.59 (9.4) | 9/73 (12%) | ||
| GLIM criteria (n = 153) | |||||
| Severe malnutrition | 66 (43%) | 13.85 (11.0) | p = 0.870 | 9/66 (14%) | p = 0.287 |
| Not severe malnutrition | 87 (57%) | 14.12 (12.9) | 16/87 (18%) | ||
| Malnutrition | 107 (71%) | 14.44 (12.6) | p = 0.477 | 17/108 (16%) | p = 0.463 |
| No evidence malnutrition | 46 (29%) | 12.96 (10.7) | 8/45 (18%) | ||
| CT analysis (n = 121 for skeletal muscle index, n = 122 for muscle quality) | |||||
| Low skeletal muscle index | 29 (24%) | 12.31 (10.4) | p = 0.385 | 6/28 (21%) | p = 0.333 |
| Normal skeletal muscle index | 91 (76%) | 14.2 (13.0) | 14/92 (15%) | ||
| Sarcopenia and BMI > 30 kg/m2 | 1 | Not suitable for analysis | |||
| VFA/SMI ≥ 2.5 (Sarcopenic obesity) | 57 (48%) | 16.01 (14.7) | p = 0.006 | 13/60 (22%) | p = 0.391 |
| VFA/SMI < 2.5 | 61 (52%) | 11.27 (9.2) | 9/58 (16%) | ||
| Poor muscle quality | 15 (12%) | 13.73 (6.6) | p = 0.179 | 3/15 (20%) | p = 0.498 |
| Normal muscle quality | 106 (88%) | 13.8 (13.0) | 18/107 (17%) | ||
| Nutritional Assessment Tool | Skeletal Muscle Index | Muscle Quality |
|---|---|---|
| Correlation Co-Efficient | ||
| BMI | 0.457 (p < 0.001) | −0.273 (p = 0.003) |
| Percentage weight loss | −0.261 (p = 0.004) | −0.167 (p = 0.69) |
| MUST score | −0.262 (p = 0.005) | −0.098 (p = 0.291) |
| GLIM criteria for malnutrition present | −0.379 (p < 0.001) | −0.192 (p = 0.036) |
| Hand-grip strength—dominant hand | ||
| Mean | 0.468 (p < 0.001) | 0.284 (p = 0.005) |
| Per cent of normal | 0.207 (p = 0.049) | 0.085 (p = 0.42) |
| Highest | 0.24 (p = 0.022) | 0.445 (p < 0.001) |
| Percentage Difference | −0.297 (p = 0.659) | 0.047 (p = 0.659) |
| Absolute Difference | −0.093 (p = 0.382) | 0.084 (p = 0.423) |
| Hand-grip strength—non-dominant | ||
| Mean | 0.097 (p = 0.350) | 0.108 (p = 0.294) |
| Per cent of normal | −0.033 (p = 0.755) | −0.112 (p = 0.288) |
| Highest | 0.431 (p < 0.001) | 0.321 (p = 0.002) |
| Percentage Difference | −0.107 (p = 0.328) | 0.00 (p = 0.998) |
| Absolute Difference | −0.130 (p = 0.224) | −0.056 (p = 0.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phillips, M.E.; Robertson, M.D.; Bennett-Eastley, K.; Rowe, L.; Frampton, A.E.; Hart, K.H. Standard Nutritional Assessment Tools Are Unable to Predict Loss of Muscle Mass in Patients Due to Undergo Pancreatico-Duodenectomy: Highlighting the Need for Detailed Nutritional Assessment. Nutrients 2024, 16, 1269. https://0-doi-org.brum.beds.ac.uk/10.3390/nu16091269
Phillips ME, Robertson MD, Bennett-Eastley K, Rowe L, Frampton AE, Hart KH. Standard Nutritional Assessment Tools Are Unable to Predict Loss of Muscle Mass in Patients Due to Undergo Pancreatico-Duodenectomy: Highlighting the Need for Detailed Nutritional Assessment. Nutrients. 2024; 16(9):1269. https://0-doi-org.brum.beds.ac.uk/10.3390/nu16091269
Chicago/Turabian StylePhillips, Mary E., M. Denise Robertson, Kate Bennett-Eastley, Lily Rowe, Adam E. Frampton, and Kathryn H. Hart. 2024. "Standard Nutritional Assessment Tools Are Unable to Predict Loss of Muscle Mass in Patients Due to Undergo Pancreatico-Duodenectomy: Highlighting the Need for Detailed Nutritional Assessment" Nutrients 16, no. 9: 1269. https://0-doi-org.brum.beds.ac.uk/10.3390/nu16091269