

SIRT1 Serum Concentrations in Lipodystrophic Syndromes
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. Anthropometric Measurements
4.3. Biochemistry
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Araújo-Vilar, D.; Santini, F. Diagnosis and treatment of lipodystrophy: A step-by-step approach. J. Endocrinol. Invest. 2019, 42, 61–73. [Google Scholar] [CrossRef] [PubMed]
- Garg, A. Lipodystrophies. Am. J. Med. 2000, 108, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Araújo-Vilar, D.; Fernández-Pombo, A.; Cobelo-Gómez, S.; Castro, A.I.; Sánchez-Iglesias, S. Lipodystrophy-associated progeroid syndromes. Hormones 2022, 21, 555–571. [Google Scholar] [CrossRef] [PubMed]
- Akinci, G.; Celik, M.; Akinci, B. Complications of lipodystrophy syndromes. Presse. Med. 2021, 50, 104085. [Google Scholar] [CrossRef] [PubMed]
- Pardini, V.C.; Victória, I.M.; Rocha, S.M.; Andrade, D.G.; Rocha, A.M.; Pieroni, F.B.; Milagres, G.; Purisch, S.; Velho, G. Leptin levels, beta-cell function, and insulin sensitivity in families with congenital and acquired generalized lipoatropic diabetes. J. Clin. Endocrinol. Metab. 1998, 83, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Haque, W.A.; Shimomura, I.; Matsuzawa, Y.; Garg, A. Serum adiponectin and leptin levels in patients with lipodystrophies. J. Clin. Endocrinol. Metab. 2002, 87, 2395. [Google Scholar] [CrossRef]
- Ceccarini, G.; Pelosini, C.; Paoli, M.; Tyutyusheva, N.; Magno, S.; Gilio, D.; Palladino, L.; Sessa, M.R.; Bertelloni, S.; Santini, F. Serum Levels of Adiponectin Differentiate Generalized Lipodystrophies from Anorexia Nervosa. J. Endocrinol. Invest. [CrossRef]
- Guarente, L. Sirtuins, aging, and metabolism. Cold Spring Harb. Symp. Quant. Biol. 2011, 76, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Finkel, T.; Deng, C.X.; Mostoslavsky, R. Recent progress in the biology and physiology of sirtuins. Nature 2009, 460, 587–591. [Google Scholar] [CrossRef] [PubMed]
- Guarente, L. Calorie restriction and sirtuins revisited. Genes Dev. 2013, 27, 2072–2085. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Takahashi, Y. The Essential Role of SIRT1 in Hypothalamic-Pituitary Axis. Front. Endocrinol. 2018, 9, 605. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, T.; Guarente, L. Sirtuins at a glance. J. Cell. Sci. 2011, 124, 833–838. [Google Scholar] [CrossRef]
- Cakir, I.; Perello, M.; Lansari, O.; Messier, N.J.; Vaslet, C.A.; Nillni, E.A. Hypothalamic Sirt1 regulates food intake in a rodent model system. PLoS ONE 2009, 4, e8322. [Google Scholar] [CrossRef]
- Picard, F.; Kurtev, M.; Chung, N.; Topark-Ngarm, A.; Senawong, T.; Machado De Oliveira, R.; Leid, M.; McBurney, M.W.; Guarente, L. Sirt1 promotes fat mobilization in white adipocytes by repressing ppargamma. Nature 2004, 429, 771–776. [Google Scholar] [CrossRef] [PubMed]
- Chalkiadaki, A.; and Guarente, L. High-Fat Diet Triggers Inflammation-Induced Cleavage of SIRT1 in Adipose Tissue to Promote Metabolic Dysfunction. Cell Metab. 2012, 16, 180–188. [Google Scholar] [CrossRef] [PubMed]
- 16 Boutant, M.; Cantó, C. SIRT1 metabolic actions: Integrating recent advances from mouse models. Mol. Metab. 2013, 3, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; Zhao, H.; Liu, Y.; Yang, Z.; Yao, H.; Liu, T.; Gou, T.; Wang, L.; Zhang, J.; Tian, Y.; et al. Novel Role of the SIRT1 in Endocrine and Metabolic Diseases. Int. J. Biol. Sci. 2023, 19, 484–501. [Google Scholar] [CrossRef]
- Wang, J.; Zhou, F.; Xiong, C.E.; Wang, G.P.; Chen, L.W.; Zhang, Y.T.; Qi, S.G.; Wang, Z.H.; Mei, C.; Xu, Y.J.; et al. Serum sirtuin1: A potential blood biomarker for early diagnosis of Alzheimer’s disease. Aging 2023, 15, 9464–9478. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Li, J.; Wang, Y.; Zhang, Z.; Yang, H.; Li, Z.; Wang, T.; Peng, T.; Mo, X.; Xu, F. Serum ANGPTL4 and SIRT1 factor levels and the Carotid Atherosclerotic plaque stability relationship analysis. Cell Mol. Biol. 2023, 69, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Niu, H.; Sha, G.; Zhang, Y.; Liu, P.; Li, Y. Serum SIRT1 Is Associated with Frailty and Adipokines in Older Adults. J. Nutr. Health Aging 2019, 23, 246–250. [Google Scholar] [CrossRef]
- Mariani, S.; di Giorgio, M.R.; Martini, P.; Persichetti, A.; Barbaro, G.; Basciani, S.; Contini, S.; Poggiogalle, E.; Sarnicola, A.; Genco, A.; et al. Inverse Association of Circulating SIRT1 and Adiposity: A Study on Underweight, Normal Weight, and Obese Patients. Front. Endocrinol. 2018, 9, 449. [Google Scholar] [CrossRef] [PubMed]
- Mansur, A.P.; Roggerio, A.; Goes, M.F.S.; Avakian, S.D.; Leal, D.P.; Maranhão, R.C.; Strunz, C.M.C. Serum concentrations and gene expression of sirtuin 1 in healthy and slightly overweight subjects after caloric restriction or resveratrol supplementation: A randomized trial. Int. J. Cardiol. 2017, 227, 788–794. [Google Scholar] [CrossRef]
- Mariani, S.; Fiore, D.; Persichetti, A.; Basciani, S.; Lubrano, C.; Poggiogalle, E.; Genco, A.; Donini, L.M.; Gnessi, L. Circulating SIRT1 Increases After Intragastric Balloon Fat Loss in Obese Patients. Obes. Surg. 2016, 26, 1215–1220. [Google Scholar] [CrossRef] [PubMed]
- Akinci, B.; Oral, E.A.; Neidert, A.; Rus, D.; Cheng, W.Y.; Thompson-Leduc, P.; Cheung, H.C.; Bradt, P.; Foss de Freitas, M.C.; Montenegro, R.M.; et al. Comorbidities and Survival in Patients with Lipodystrophy: An International Chart Review Study. J. Clin. Endocrinol. Metab. 2019, 104, 5120–5135. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.J.; Araujo-Vilar, D.; Cheung, P.T.; Dunger, D.; Garg, A.; Jack, M.; Mungai, L.; Oral, E.A.; Patni, N.; Rother, K.I.; et al. The Diagnosis and Management of Lipodystrophy Syndromes: A Multi-Society Practice Guideline. J. Clin. Endocrinol. Metab. 2016, 101, 4500–4511. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.M.; Lun, M.; Wang, M.; Senyo, S.E.; Guillermier, C.; Patwari, P.; and Steinhauser, M.L. Loss of white adipose hyperplastic potential is associated with enhanced susceptibility to insulin resistance. Cell Metab. 2014, 20, 1049–1058. [Google Scholar] [CrossRef] [PubMed]
- Akinci, B.; Meral, R.; Oral, E.A. Phenotypic and Genetic Characteristics of Lipodystrophy: Pathophysiology, Metabolic Abnormalities, and Comorbidities. Curr. Diab. Rep. 2018, 18, 143. [Google Scholar] [CrossRef]
- Chehab, F.F. Obesity and lipodystrophy--where do the circles intersect? Endocrinology 2008, 149, 925–934. [Google Scholar] [CrossRef]
- Lim, K.; Haider, A.; Adams, C.; Sleigh, A.; Savage, D.B. Lipodistrophy: A paradigm for understanding the consequences of "overloading" adipose tissue. Physiol. Rev. 2021, 101, 907–993. [Google Scholar] [CrossRef] [PubMed]
- Pardo, P.S.; Boriek, A.M. SIRT1 Regulation in Ageing and Obesity. Mech. Ageing Dev. 2020, 188, 111249. [Google Scholar] [CrossRef] [PubMed]
- Perrini, S.; Porro, S.; Nigro, P.; Cignarelli, A.; Caccioppoli, C.; Genchi, V.A.; Martines, G.; De Fazio, M.; Capuano, P.; Natalicchio, A.; et al. Reduced SIRT1 and SIRT2 expression promotes adipogenesis of human visceral adipose stem cells and associates with accumulation of visceral fat in human obesity. Int. J. Obes. 2020, 44, 307–319. [Google Scholar] [CrossRef]
- Mariani, S.; Di Rocco, G.; Toietta, G.; Russo, M.A.; Petrangeli, E.; Salvatori, L. Sirtuins 1-7 expression in human adipose-derived stem cells from subcutaneous and visceral fat depots: Influence of obesity and hypoxia. Endocrine. 2017, 57, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Li, X. SIRT1 and energy metabolism. Acta Biochim. Biophys. Sin. 2013, 45, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Vigouroux, C.; Caron-Debarle, M.; Le Dour, C.; Magré, J.; Capeau, J. Molecular mechanisms of human lipodystrophies: From adipocyte lipid droplet to oxidative stress and lipotoxicity. Int. J. Biochem. Cell Biol. 2011, 43, 862–876. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Lee, L.; Kudlow, B.A.; Dos Santos, H.G.; Sletvold, O.; Shafeghati, Y.; Botha, E.G.; Garg, A.; Hanson, N.B.; Martin, G.M.; et al. LMNA mutations in atypical Werner’s syndrome. Lancet 2003, 362, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Guillín-Amarelle, C.; Sánchez-Iglesias, S.; Castro-Pais, A.; Rodriguez-Cañete, L.; Ordóñez-Mayán, L.; Pazos, M.; González-Méndez, B.; Rodríguez-García, S.; Casanueva, F.F.; Fernández-Marmiesse, A.; et al. Type 1 familial partial lipodystrophy: Understanding the Köbberling syndrome. Endocrine 2016, 54, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Magno, S.; Ceccarini, G.; Corvillo, F.; Pelosini, C.; Gilio, D.; Paoli, M.; Fornaciari, S.; Pandolfo, G.; Sanchez-Iglesias, S.; Nozal, P.; et al. Clinical characteristics of patients with acquired partial lipodystrophy: A multicenter retrospective study. J. Clin. Endocrinol. Metab. 2023, dgad700. [Google Scholar] [CrossRef] [PubMed]
- Tews, D.; Schulz, A.; Denzer, C.; von Schnurbein, J.; Ceccarini, G.; Debatin, K.M.; Wabitsch, M. Lipodystrophy as a Late Effect after Stem Cell Transplantation. J. Clin. Med. 2021, 10, 1559. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; DSM-5; American Psychiatric Association: Washington, DC, USA; London, UK, 2013. [Google Scholar]
- Lindvall Dahlgren, C.; Wisting, L.; Rø, Ø. Feeding and eating disorders in the DSM-5 era: A systematic review of prevalence rates in non-clinical male and female samples. J. Eat. Disord. 2017, 5, 56. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Lipodystrophy | Anorexia Nervosa | Normal Weight | Obesity | |
|---|---|---|---|---|
| Subjects | 32 | 24 | 22 | 24 |
| Gender (male/female) | 5/27 | 6/18 | 1/21 | 2/22 |
| Age (years) | 40.28 ± 3.94 | 27.96 ± 2.57 | 29.81 ± 1.87 | 35.71 ± 2.6 |
| BMI (Kg/m2) | 22.44 ± 0.95 | 15.43 ± 0.36 | 22.36 ± 0.27 | 37.77 ± 0.79 |
| Total fat (%) | 25.92 ± 1.7 | 16 ± 1.15 | 27.06 ± 1.45 | 41.33 ± 0.85 |
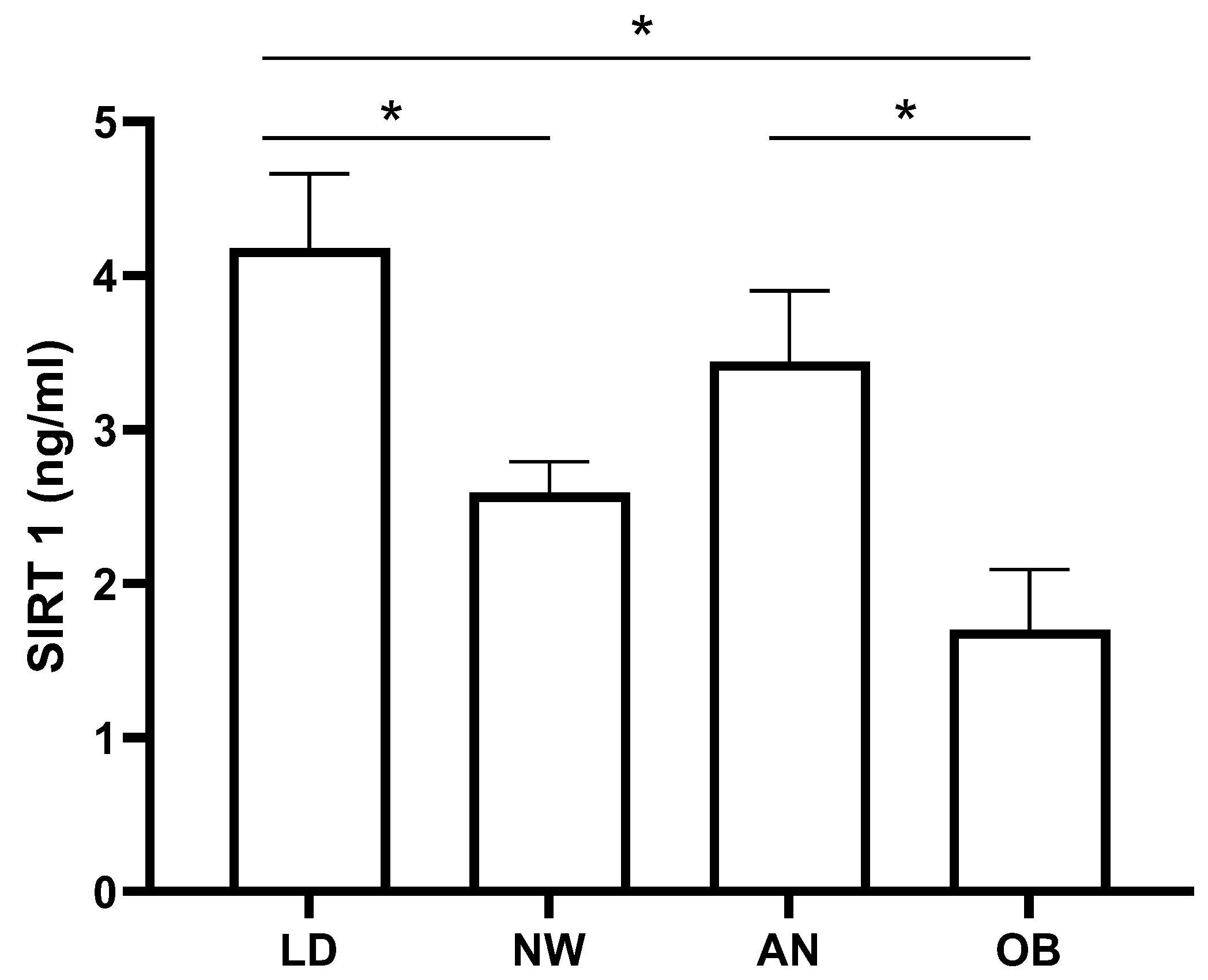
| SIRT1 (ng/mL) | 4.18 ± 0.48 | 3.44 ± 0.46 | 2.59 ± 0.2 | 1.7 ± 0.39 |
| FPG (mg/dL) | 99.06 ± 4.55 | 72.92 ± 1.76 | 82.45 ± 0.2 | 89.25 ± 1.62 |
| Total cholesterol (mg/dL) | 168.9 ± 5.53 | 178.08 ± 11.11 | 181.5 ± 6.66 | 168.41 ± 9.42 |
| LDL cholesterol (mg/dL) | 101.52 ± 6.95 | 88.17 ± 8.97 | 97.77 ± 5.32 | 100.74 ± 6.65 |
| Triglycerides (mg/dL) | 178.9 ± 26.29 | 95.5 ± 11.93 | 93.86 ± 12.47 | 104.63 ± 10.99 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvatori, L.; Magno, S.; Ceccarini, G.; Tozzi, R.; Contini, S.; Pelosini, C.; Santini, F.; Gnessi, L.; Mariani, S. SIRT1 Serum Concentrations in Lipodystrophic Syndromes. Int. J. Mol. Sci. 2024, 25, 4785. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms25094785
Salvatori L, Magno S, Ceccarini G, Tozzi R, Contini S, Pelosini C, Santini F, Gnessi L, Mariani S. SIRT1 Serum Concentrations in Lipodystrophic Syndromes. International Journal of Molecular Sciences. 2024; 25(9):4785. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms25094785
Chicago/Turabian StyleSalvatori, Luisa, Silvia Magno, Giovanni Ceccarini, Rossella Tozzi, Savina Contini, Caterina Pelosini, Ferruccio Santini, Lucio Gnessi, and Stefania Mariani. 2024. "SIRT1 Serum Concentrations in Lipodystrophic Syndromes" International Journal of Molecular Sciences 25, no. 9: 4785. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms25094785