
Current Perspectives of Mitochondria in Sepsis-Induced Cardiomyopathy


Department of Emergency Medicine, Asahikawa Medical University, Asahikawa 078-8510, Japan
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2024, 25(9), 4710; https://0-doi-org.brum.beds.ac.uk/10.3390/ijms25094710
Submission received: 24 March 2024
/
Revised: 19 April 2024
/
Accepted: 24 April 2024
/
Published: 26 April 2024
(This article belongs to the Special Issue Understanding Sepsis: Pathophysiology, Diagnostics and Early Intervention)
Abstract
:Sepsis-induced cardiomyopathy (SICM) is one of the leading indicators for poor prognosis associated with sepsis. Despite its reversibility, prognosis varies widely among patients. Mitochondria play a key role in cellular energy production by generating adenosine triphosphate (ATP), which is vital for myocardial energy metabolism. Over recent years, mounting evidence suggests that severe sepsis not only triggers mitochondrial structural abnormalities such as apoptosis, incomplete autophagy, and mitophagy in cardiomyocytes but also compromises their function, leading to ATP depletion. This metabolic disruption is recognized as a significant contributor to SICM, yet effective treatment options remain elusive. Sepsis cannot be effectively treated with inotropic drugs in failing myocardium due to excessive inflammatory factors that blunt β-adrenergic receptors. This review will share the recent knowledge on myocardial cell death in sepsis and its molecular mechanisms, focusing on the role of mitochondria as an important metabolic regulator of SICM, and discuss the potential for developing therapies for sepsis-induced myocardial injury.
Keywords:
sepsis; SICM; mitochondria; metabolic switch; cell death; mitophagy; lncRNAs; adrenergic receptor1. Introduction
Sepsis is a severe condition that can be complicated by life-threatening organ dysfunction resulting from an abnormal host response to infection. However, SICM specifically affects the heart [1,2,3,4]. The mortality of patients with SICM is 30–70%, which is 2–3-fold higher than that of patients with non-cardiac-related sepsis [5,6].
Cell death in the myocardium may result in the inability to maintain normal cardiac function because most adult cardiomyocytes are terminally differentiated and non-regenerating cells [7]. Currently, The Nomenclature Committee on Cell Death reports multiple modes of cell death [8]. Cardiomyocytes have specific cell death modality and the key cell death modalities include apoptosis, necroptosis, mitochondrial-mediated necrosis, pyroptosis, ferroptosis, and autophagic cell death [9]. The cell membrane remains intact in the case of apoptosis, ferroptosis, and autophagy, while death by necroptosis, mitochondrial-mediated necrosis, and pyroptosis leads to cell membrane disruption [9]. In sepsis, a complex condition when patient background is included, myocardial cell death is not a single event, but rather causes apoptosis, necroptosis, pyroptosis, and ferroptosis simultaneously or in succession [8].
Sepsis is characterized by the acute release of multiple inflammatory mediators, including tumor necrosis factor (TNF)-α, interleukin (IL)-6, and IL-1β, and excessive release of inflammatory mediators damages tissues and organs. There is also growing evidence linking inflammation and cell death [10,11,12]. Therefore, the pathogenesis of sepsis is intimately involved in inflammation-mediated dysregulation of cell death leading to multiple organ failure.
While evidence of pathological changes in other organs has accumulated, little has been reported on the pathology of SICM. Some animal studies have shown that while myocardial mitochondria did not exhibit morphological abnormalities, there were noticeable alterations in the surrounding endoplasmic reticulum [13]. Furthermore, accumulated lipid droplets were identified in cardiomyocytes implying that impaired transport of fatty acids to mitochondria may be a potential mechanism [14]. These findings suggest SICM is caused by functional disorders in mitochondria. Indeed, SICM is considered reversible in the clinical practice.
Recent studies suggest that the pathogenesis of SICM involves disproportionate expression of pro- and anti-inflammatory cytokines, abnormal expression of Toll-like receptors and related downstream pathways, nitric oxide (NO) release, inducible NO synthase (iNOS) contributing to metabolic disturbances and reactive oxygen species (ROS). These cause complement activation, abnormal calcium processing, downregulation of adrenergic pathways, cardiomyocyte apoptosis, autonomic nervous system dysfunction, coronary microvascular dysfunction, mitochondrial dysfunction, sarcomere and mitochondrial protein downregulation [15,16,17,18]. In the heart, the systemic inflammatory response impairs the ability of energy metabolism to produce adenosine triphosphate (ATP), resulting in cardiac dysfunction [14,19].
Seen from a different perspective, SICM may be regarded as a metabolic disorder. Myocardial energy metabolism encompasses a diverse array of pathways, with mitochondria playing a central role as crucial organelles involved in metabolism. This review aimed to present recent findings in SICM, with a particular focus on abnormalities in mitochondrial function.
2. Methodology Literature Search
Literature searches were conducted using PubMed and major journals of clinical and basic science. Searches focused on mitochondrial roles in sepsis-induced cardiomyopathy. PubMed searches for variations of the terms “mitochondria and sepsis”, “pathophysiology and sepsis induced cardiomyopathy”, and relevant keywords were used to identify relevant papers which are available in English.
3. The Role of Mitochondria as a Powerhouse in Heart
The mitochondria are main source of cardiac energy. Mitochondria produce 95% of cellular ATP [20]. Generally, 60–90% of ATP production is dependent on fatty acids oxidation (FAO), and the remainder originates from the oxidation of glucose and lactic acid, ketone bodies, and amino acids in the heart [21]. The mitochondria are divided into two sections by the inner and outer membranes. The innermost space is called the matrix, and the interstitial space between the inner and outer membranes is called the intermembrane space. Electron transfer in respiratory chain complexes I–IV pumps protons from the mitochondrial matrix into the intermembrane space, creating an electrochemical gradient (∆pH) of protons across the mitochondrial inner membrane. The ∆pH and mitochondrial membrane potential (∆ψm) become the proton motive force, and ATP production is carried out by ATP synthase, called oxidative phosphorylation (OXPHOS) [22,23].
The mitochondria are important for myocardial contraction. In 2010, the previously unidentified mitochondrial Ca2+ uptake protein mitochondrial calcium uptake 1 was identified. Since then, it has been understood there is a coupling between Ca2+ signaling and mitochondrial Ca2+ signaling and mitochondrial metabolism. Ca2+ is involved in cardiomyocyte excitation and contraction. Ca2+ plays a crucial role in the excitation and contraction of cardiomyocytes. It is responsible for orchestrating the excitation–contraction coupling process within cardiomyocytes, where Ca2+ facilitates muscle contraction. Additionally, mitochondrial Ca2+ levels regulate the excitatory and contractile functions of cardiomyocytes. Overall, Ca2+ is central to maintaining the intricate balance in the excitatory-contraction relationship of cardiomyocytes [24,25].
4. Pathophysiology of SICM
The sequence of events leading to SICM involves several circulating factors. These extracellular mediators include both pathogen-associated molecular patterns (PAMPs), such as lipopolysaccharides (LPSs), and host-produced damage-associated molecular patterns (DAMPs). LPSs are exclusively found in the outermost membrane of Gram-negative bacteria and bind to Toll-like receptor 4 to produce inflammatory mediators. DAMPs also include cytokines (IL-1β, TNF, IL-6) [26,27,28], iNOS [29,30,31], ROS [32,33], heat shock proteins, high mobility group box 1, histones, activated complement components, and mitochondrial DNA. Preclinical studies have shown that these molecules directly or indirectly suppress cardiac function. However, no correlation has been found between cytokines measured in septic patients and myocardial dysfunction. This suggests that the ultimate effects of these circulating factors on the heart are likely due to the interaction of a wide range of signaling pathways rather than a single factor. Myocardium from septic animals had normal high-energy phosphate levels and no evidence of cellular hypoxia [34,35,36]. Other abnormalities which proposed to contribute to the SICM etiology include altered calcium transport [37], altered metabolism [38], impaired myocardial electrical conduction [39,40], and adrenergic signaling abnormalities [41,42]. However, none of these mechanisms alone can satisfactorily explain why septic cardiomyocytes, once in a state of functional arrest, rapidly regain function [34]. The mitochondria are strongly associated with the above-mentioned SICM factors, and examining the role of this organelle is worthwhile for discussion.
4.1. Mitochondrial Structural Abnormalities
The role of nuclear fission and fusion was studied in experimental sepsis, but few researches have focused on cardiac mitochondria. Electron microscopy of rat hearts 24 h after endotoxin administration revealed compatible morphological changes with the processes of nuclear fission and fusion [43]. An imbalance in a severe cecal ligation and puncture (CLP) model of mouse sepsis between mitochondrial fission and fusion with dynamin-related protein 1 (Drp1) activation and optic atrophy 1 (OPA1) downregulation was demonstrated in association with mitochondrial structural abnormalities, mitochondrial dysfunction, and reduced cardiac contractility [35]. The heart of LPS-treated mice also showed Drp1 activation, with decreased mitochondrial size, increased fragmentation, and abnormal morphology and function [36]. In contrast, OPA1 expression was mildly increased by sublethal LPS doses [44]. These conflicting results may reflect the extent of myocardial injury and the phase of sepsis.
4.2. Autophagy and Mitophagy in SICM
Autophagy is one of the mechanisms involved in cellular homeostasis and cell death. Autophagy is performed by a process in which damaged proteins and organelles are placed in double-membrane vesicles (autophagosomes) and sent to lysosomes for degradation.
Mitophagy is a type of selective autophagy that aims to remove dysfunctional mitochondria and induce cell death pathways before mitochondrial outer membrane permeability is compromised. Autophagy is activated in the heart during sepsis, but whether this is protective or detrimental is unknown. However, activation of autophagy and mitochondrial depletion in the heart have been observed in a number of rodent CLP and LPS models [36,39,45].
Autophagy activation in the heart has been confirmed within 4 h in a mouse CLP model. The co-localization of autophagosomes and lysosomes is reduced in septic animals despite the increased autophagic vacuoles, suggesting impaired autophagosome interactions and decreased degradation. This incomplete autophagy is associated with cardiac dysfunction, ATP depletion, apoptosis, and necrosis, which are all restored by rapamycin, which stimulates complete autophagy. Similar findings were observed in vitro, where autophagy induction protected cardiomyocytes from LPS-induced cell death, while autophagy inhibition had the opposite result [40].
LPS stimulation was also found to induce not only myocardial autophagy but also more selective mitophagy processes [36]. This removal of damaged mitochondria via activation of mitophagy may facilitate the resolution of cardiac and mitochondrial dysfunction. Defects in sestrin 2, a protein involved in mitochondrial priming in autophagy, were associated with increased mortality. In contrast, loss of Rubicon, a key protein that negatively regulates autophagosome maturation, the Beclin-1 binding protein, enhanced autophagy flux and cardiac function [40,46].
Cardiac autophagy was upregulated in LPS-treated mice, suggesting that this phenomenon is associated with a detrimental increase in oxidative stress. Cardiac-specific overexpression of the endogenous mitochondrial antioxidant thioredoxin-1 also improved prognosis in CLP mice, but this was associated with stimulation rather than inhibition of autophagy [45]. Pharmacological inhibition of autophagy reversed contractility of neonatal cardiomyocytes but increased apoptosis and mitochondrial dysfunction in both neonatal cardiomyocytes and HL-1 cells [43,47]. Cells replace damaged mitochondria that are removed by mitophagy through mitochondrial biogenesis and interaction between peroxisome proliferator-activated receptors (PPARs) and PPAR-γ co-activator (PGC)-1α and -β. The phenomenon activates multiple transcription factors, including nuclear respiratory factors 1 and 2, to promote the expression of mitochondrial transcription factor A (T-fam). This coordinated signaling cascade increases mitochondrial DNA copy number and mitochondrial mass. Recently, mitochondrial biogenesis in cardiomyocytes has been reported in several experimental sepsis models, which still remains elusive.
4.3. Calcium Transport-Induced Membrane Potential in SICM
Calcium uptake into cardiac mitochondria is facilitated by the presence of microdomains between the sarcoplasmic reticulum (SR), the intracellular calcium store, and the mitochondria. These microdomains bring calcium release sites and calcium uptake sites into proximity and are maintained by tethering proteins, such as mitofusin, which are also involved in the fission or fusion process. This system allows mitochondrial calcium, the main determinant of ATP supply, to be synchronized with the ATP demand generated by the excitation–contraction coupling process [48]. Calcium transport to mitochondria is also essential for maintaining proper mitochondrial antioxidant capacity and mitigating the increase in ROS formation caused by increased ATP synthesis [49]. Calcium loading in mitochondria has detrimental effects and is a major determinant of mPTP opening, especially in the presence of oxidative stress [50]. Thus, it is easy to understand the involvement of calcium transport defects in mitochondria with the pathophysiology of many diseases, including heart failure [51]. Abnormal intracellular calcium homeostasis has been studied in the septic heart. In most septic models, cytosolic calcium transients (i.e., the difference between systolic and diastolic calcium concentration) were decreased, which was associated with increased diastolic cytosolic calcium and decreased SR calcium content [52]. These findings may be attributed to the dysfunction of SR calcium transporters, specifically the “leaky” ryanodine receptor (RyR) and SERCA, which cause increased calcium release and decreased reuptake, respectively. Changes in intracellular calcium concentrations are exacerbated by myofibrillar desensitization to calcium [53] or by altered expression of calcium-processing proteins [54]. Despite a large number of studies suggesting a central role for intracellular calcium imbalance in SICM, few studies have clearly evaluated the role of calcium in myocardial mitochondria. Myocardial mitochondrial calcium concentrations were elevated in endotoxin-treated rats in association with abnormal mitochondrial respiration, membrane potential, and myocardial dysfunction [55,56]. In cardiomyocytes exposed to endotoxin for 1 h, mitochondrial calcium concentration increased in a dose-dependent manner of endotoxin, inducing cell death. The results that treatment of these cardiomyocytes with dantrolene ameliorated the excess calcium concentration in mitochondria and inhibited cell death suggest that SICM induces a defect related to calcium transport in cardiac mitochondria [57].
Experiments of electrical pacing in automobile cardiomyocytes isolated from septic rats evaluated changes in mitochondrial calcium and found that the rate of calcium increase was lower than in control cardiomyocytes and was associated with other signs of mitochondrial dysfunction. Interestingly, the potential contact area between mitochondria and SR was reduced, and the distance between these organelles was increased by electron microscopy [45]. These structural abnormalities in the organelle may cause dysfunction of the mitochondrial-SR microdomain, leading to a reduced rate of calcium uptake. On the other hand, these findings may be an adaptive and protective response to prevent mitochondrial calcium overload at the expense of reduced energy efficiency. Myocardial calcium homeostasis has not been evaluated in human patients with sepsis. However, recent large observational studies have reported that chronic use of calcium antagonists up to hospitalization is associated with reduced mortality from sepsis [58,59], and other experimental studies have revealed specific beneficial effects of calcium antagonists on cardiac function [60,61].
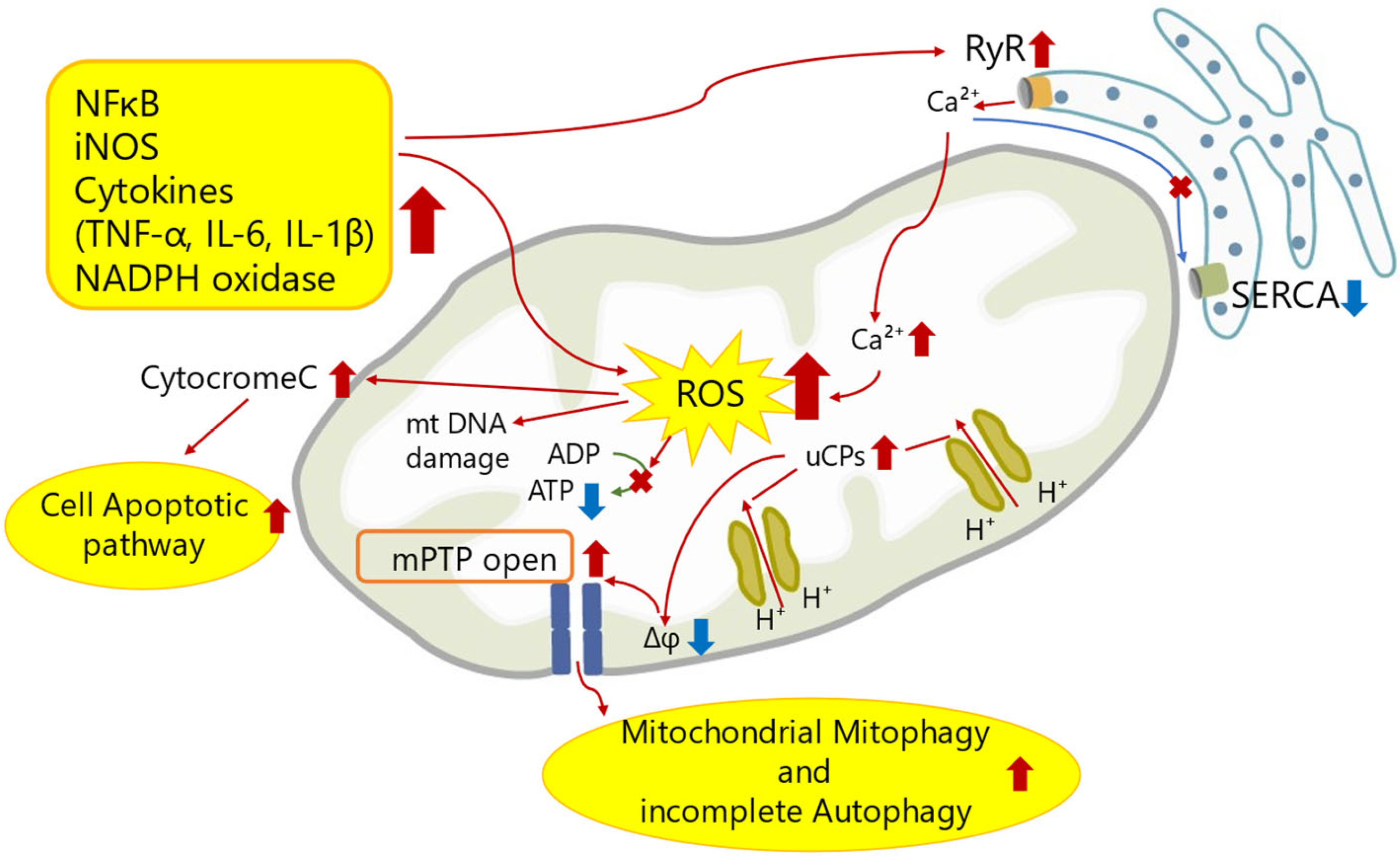
Here, we show a schematic figure of mechanisms of mitochondrial dysfunction in SICM (Figure 1).
4.4. Mitochondrial Metabolic Abnormality in SICM
Lipid metabolism is the primary source of ATP production in the heart. Most patients are starved during sepsis and require energy from lipid mobilization and oxidation [62]. Along with increased catabolism, increased lipolysis in adipose tissue, the largest source of energy in the body, is compensated for by the conversion of triglycerides (TGs) to fatty acids (FAs) and glycerol, which are released into the bloodstream [63]. The released FAs enter the peripheral organs and are oxidized to produce ATP. However, the inflammatory response of sepsis is differentially regulated by various genes related to lipid metabolism. For example, LPS decreases PPAR and PGC1, which regulate oxidative pathways [64], and cluster of differentiation 36 (CD36) and carnitine palmitoyltransferase I (CPT1) dysregulation induce FA transport defects, leading to FAO failure [14,39,65]. In particular, CPT1 reduction prevents FA from entering the mitochondria. This leads to intracellular accumulation of lipids and organ dysfunction, as well as “lipotoxicity”. The association between myocardial lipid accumulation and heart failure in humans has long been reported. Studies reported intramyocardial triacylglycerol accumulation and its transcriptional profile in patients with heart failure, leading to lipotoxicity and contractile dysfunction, as well as documented lipid accumulation in heart samples from patients with severe chronic heart failure undergoing heart transplantation [66,67]. Lipid accumulation has been associated with cell apoptosis mechanisms [68,69], ROS production [70,71], endoplasmic reticulum stress, and cell death [72] and may itself lead to heart failure (Figure 2).
4.5. Pyroptosis in SICM
Pyroptosis is a type of cell death mediated by inflammations. The cell death mechanism can not only defend against microbial infection but also induce excessive host-dependent inflammatory response [73,74]. Cardiomyocytes’ pyroptosis and inflammation contributes to SICM.
LPS activates NLR family pyrin domain containing 3 (NLPR3) in myocardium of septic mice [75]. NLRP3 inflammasome is a macromolecular protein complex that senses the damage and activates inflammatory response. NLPR3 activates caspase 1 followed by IL-1β and induces pyroptosis. Actually, inhibitors of NLPR3 reduces inflammation and preserve cardiac function [76,77].
Gasdermin D (GSDMD) is also involved with pyroptosis [78]. GSDMD is expressed in a variety of cell types and works as a specific substrate of inflammatory caspases. GSDMD not only increases inflammatory factors via activation of NLPR3 but also causes decrease in ATP production by mitochondrial injury. Shanshan et al. reported that LPS increased GSDMD expression and triggered SICM, while Gsdmd−/− mice attenuated cardiac dysfunction in sepsis [79]. In addition, Zhang et al. identified inhibition of caspase 11, and GSDMD improved SICM by attenuating cardiomyocytes’ pyroptosis [80].
4.6. Ferroptosis in SICM
Ferroptosis is a nonapoptotic cell death program distinct from apoptosis or necrosis. This mechanism is featured by iron-dependent lipid peroxidation and involved in various pathological processes, including neurotoxicity, cardiovascular diseases, cancer, and sepsis [81,82]. Ferroptosis is involved with depletion of glutathione (GSH) [83,84] and inactivation of glutathione peroxidase 4 (GPX4) [83,84], which results in metabolic imbalances of iron and lipids. Activation of ferroptosis causes mitochondrial swelling and mitochondrial membrane potential collapse through mitochondrial permeability transition pore (MPTP) opening, ultimately leading to cell death [84], while mitochondrial dysfunction impairs iron metabolism, which results in excessive free iron accumulation in mitochondria and lipid peroxidation of their membranes. Lipid peroxidation accumulation in the mitochondria induces cysteine deprivation and promotes glutaminolysis, thereby activating the tricarboxylic acid cycle. This activity increases mitochondrial hyperpolarization and ROS production, resulting in induction of lipid peroxidation and ferroptosis. Therefore, evidence has identified varied interplay between ferroptosis and mitochondrial dysfunction. Recently, the development of sepsis has been proposed to involve ferroptosis, and many basic studies focus on inhibition of ferroptosis to reduce organ damage including SICM [82,85].
5. Potential Therapeutic Interventions: Future Perspective
Mitochondria have many important roles for cardiac metabolism, and mitochondrial dysfunction in sepsis leads to cardiac dysfunction. Therefore, mitochondria-targeted metabolic resuscitation may become a promising strategy against SICM.
Here, we discuss three potential approaches of mitochondrial resuscitation in SICM: (1) antioxidative therapy to attenuate oxidative damage in mitochondria, (2) metabolic modulation of ATP production in mitochondria, (3) regulation of noncoding RNA associated with mitochondrial metabolism.
5.1. Therapeutic Strategies for Mitochondria with Antioxidants
Many attempts at mitochondrial therapy with antioxidants have been made in clinical studies, but with limited success [86]. Recently, a multicenter open-label RCT was conducted in severe septic patients with combination therapy of vitamin C, hydrocortisone, and thiamine, which have not shown any significant differences in survival time or free duration of vasopressor administration in comparison to those with only hydrocortisone therapy [87]. This can be predominantly attributed to conventional antioxidants’ nonspecific intracellular localization and inability to transport across multiple biological barriers and exert therapeutic effects in the target cells, the mitochondria [88]. For these reasons, the next challenge was to create antioxidants that had been chemically modified to accumulate selectively in mitochondria. This approach can be broadly divided into two approaches as follows: (1) the mitochondrial matrix has a negative potential in comparison to the cytoplasm and extracellular space, and large diameter cations are selectively sequestered within the mitochondrial matrix; and (2) the use of lipophilic side chains facilitates the movement of molecules through the mitochondrial membrane. Mitoquinone (ubiquinone attached to a triphenyl phosphonium cation), mitotempol (tempol attached to a triphenyl phosphonium cation; a similar structured related molecule is midtempo), SKQ1 (plastoquinone decyltriphenyl phosphonium), and SS-31, a small mitochondrially targeted peptide drug, have been developed using these methods [89]. Damon et al. found that mitoquinone suppresses ROS production and maintains mitochondrial membrane potential in an in vitro endothelial cell model of sepsis and that administration to septic animals reduces liver and kidney damage [90]. Mitoquinone has also been shown in animal models of sepsis to reduce cardiac mitochondrial and contractile dysfunction [91]. Furthermore, Mito-TEMPO, a mitochondria-targeted antioxidant, reduces renal impairment [92] or liver injury [93] in septic animal models, which might have a potential to attenuate SICM. SS-31 therapy effectively protected cardiac function from septic injury by suppressing inflammatory mediators and maintaining mitochondrial membrane potential [94].
The preclinical data of therapeutic approaches targeting mitochondria have accumulated. However, there is still no evidence in septic patients with SICM. Clinical trials need to be conducted to investigate whether mitochondrial-targeted antioxidants make profits without side effects against SICM.
5.2. Therapeutic Strategies for Mitochondrial Metabolism in SICM
Therapeutic strategies targeting different SICM mechanisms, especially mitochondrial targeting, may be necessary to achieve a more effective prognosis in practice. However, real-world clinical SICM therapy application has not yet been realized, probably due to the difficulty in fully modeling the characteristics of sepsis due to the complexity of background factors and mechanisms of metabolic abnormalities in SICM. Here, we discuss the therapeutic strategies for SICM with potential clinical applications.
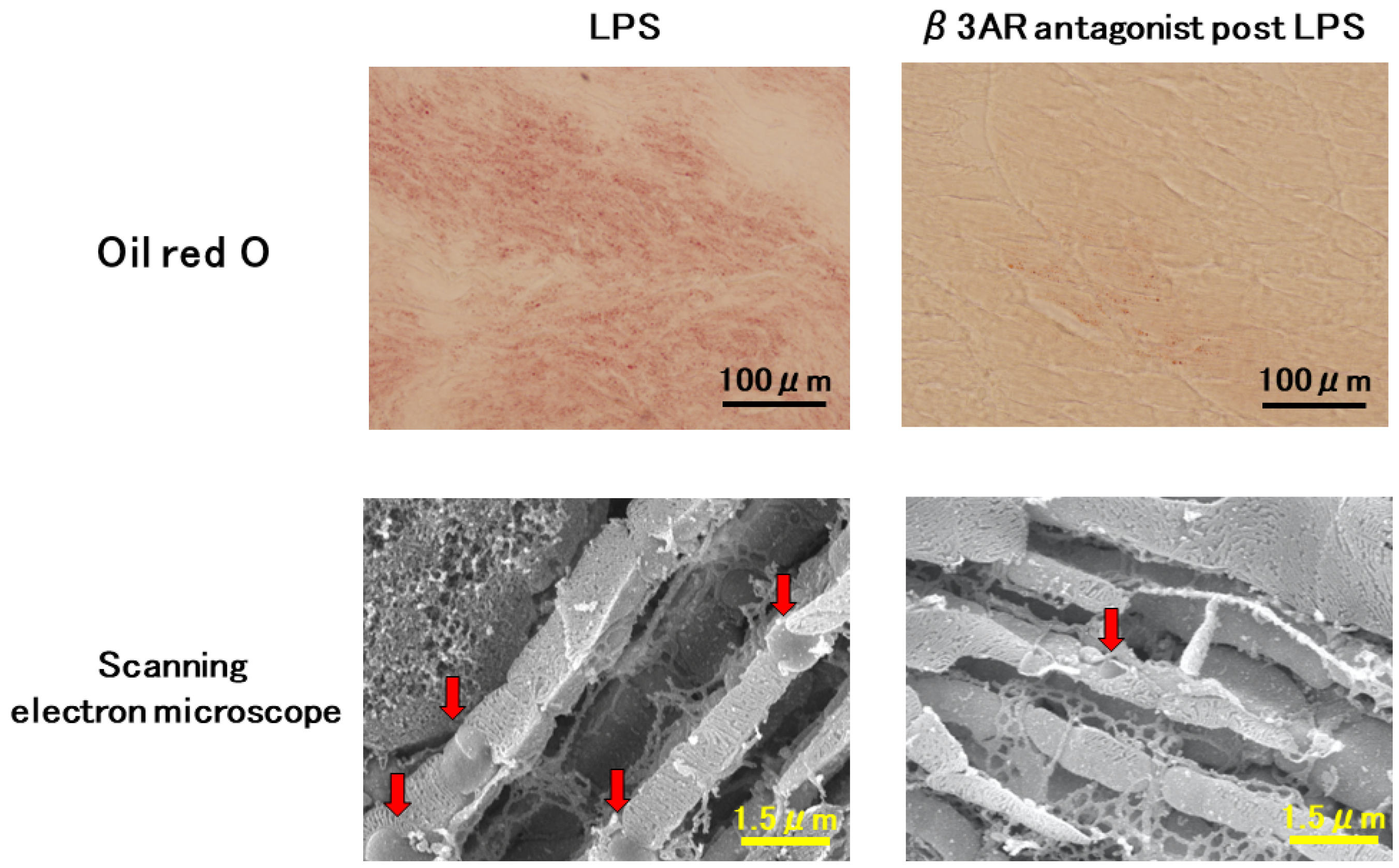
Mitochondrial dysfunction impairs cardiac metabolism in sepsis. As described before, inflammation decreases the expression of CD36 and CPT1, which are important lipid transporters into mitochondria, leading to lipid accumulation. Recently, we reported that beta-3 adrenergic receptor antagonist improves lipid accumulation in SICM [14]. In the study, we found a gap in the recovery time of CD36 and CPT1 expression in LPS-induced septic hearts, suggesting that this time gap may lead to an imbalanced FA supply and demand between the cytoplasm and mitochondria, causing lipid accumulation in the cytoplasm and myocardial tissue of endotoxin model mice. Myocardial lipid droplets (LDs) were observed in histological findings in the myocardium of LPS mice using Oil Red O-stained light microscopy, whereas few LDs were observed in the myocardial mice in the normal control group. SEM with osmium immersion revealed three-dimensional intracellular ultrastructure: myocardial mitochondria in the normal control group of mice were round, plate-like clusters densely packed in the matrix space. The matrix space was sparse in LPS mice, and LDs were found outside the mitochondrial structure. These findings were consistent with light microscopic examination of tissue stained with Oil Red O (Figure 3). Interestingly, this study observed many LDs around the myocardial mitochondria 12 h after LPS injection, indicating cardiac dysfunction, but not at 24 h. This may suggest a strong relationship between lipid dysregulation and reversible cardiac function. Furthermore, in this study, we demonstrated the effects of β3ARs on mitochondrial metabolism in SICM and revealed that β3AR blockade improves cardiac dysfunction and mortality in LPS-induced lipid accumulation. β3ARs are mostly found in adipocytes and are associated with lipolysis, while a few β3ARs are present in the heart. Notably, β3ARs are increased in ischemic heart failure [95], and β3AR stimulation improves cardiac function after myocardial infarction via NOS regulation [96,97]. However, contrary to our expectations, β3ARs blockade significantly improved cardiac ATP and mortality in LPS-induced sepsis mice. This study demonstrated that (1) β3AR is increased in SICM; (2) β3AR blockade maintains cardiac ATP by improving FAO; (3) β3AR blockade prevents myocardial lipid accumulation; and (4) β3AR regulates excess NO, which induces mitochondrial dysfunction. On the other hand, many investigators argue that β3AR activation is useful in improving cardiovascular pathology [98]. Identifying the phase of the “metabolic switch” is important because the pathogenesis of sepsis involves changes in immunity and metabolism over time. Cardiac mitochondrial metabolism in sepsis is complex, but an approach to mitochondrial metabolism could provide a new therapeutic strategy for SICM [14,99].
5.3. Effects of Noncoding RNA Regulation on Mitochondrial Dysfunction in SICM
Recently, the involvement of noncoding RNA (ncRNAs), especially long noncoding RNAs (lncRNAs), in the mitochondria has attracted much attention. Cheng Xing Peng et al. studied the regulatory role of myocardial-infarction-associated transcript (MIAT) in SICM and revealed that knockdown MIAT significantly suppressed mitochondrial ROS production in LPS-treated HL-1 cells. This result suggested that MIAT exacerbates myocardial injury by promoting oxidative stress, and MIAT in SICM directly acts on miR-330-5p to upregulate the TRAF6/NF-kB pathway, thereby promoting inflammation and oxidative stress [100]. Ying Han et al. demonstrated that receptor-activated modifying protein (RMRP) inhibits the post-transcriptional modulatory effect of miR-1-5p on heat shock protein 70 protein 4 (HSPA4) in LPS-induced mitochondrial damage, and RMRP overexpression reduces mitochondrial membrane potential (MMP), intracellular ROS levels, cytoplasmic cytochrome c, caspase-9, and caspase-3, and significantly suppresses cardiomyocyte apoptosis [101]. Bin Shan et al. revealed that H19 modulates MMP by regulating the miR-93-5p/SORBS2 pathway and overexpressing H19 in LPS-induced cardiomyocytes markedly reduced inflammatory factors, including TNF-a, IL-1b, and IL-6, indicating that overexpression of H19 is associated with inflammation [102]. Studies on the involvement of lncRNAs in regulating mitochondrial metabolism in SICM are ongoing, and Dongshi et al. revealed that suppressing LPS-induced X-inactive specific transcript RNA (Xist) expression increases ATP production and reduces LPS-induced myocardial damage [103]. Recent studies supporting the implication of ncRNAs targeting mitochondria in SICM are summarized in Table 1.
To date, researchers at Zhejiang University have identified 471 upregulated lncRNAs and 804 downregulated lncRNAs in myocardium of septic mice using gene chip hybridization technology. Finally, this group found that partial lncRNAs are mainly enriched in inflammation, immunity, energy metabolism, and cell death and predicted that certain lncRNAs may be involved with mitochondrial dysfunction [104]. Whether other lncRNAs participate in the regulation of mitochondrial function and the specific regulatory mechanisms of the involved lncRNAs in SICM remains unclear, although the aforementioned lncRNAs were implicated in SICM by regulating mitochondrial function and apoptosis. The involvement of lncRNAs in mitochondrial metabolic disturbances in SICM awaits further elucidation.
5.4. Blockade of β Adrenergic Receptor in Sepsis
Parker et al. first proposed in a 1984 study that patients with sepsis exhibited intrinsic myocardial dysfunction, with an increased volume and a decreased ejection fraction, which was reversible. Although cardiovascular abnormalities in sepsis were known since the 1950s [108,109], the concept of reversible cardiac dysfunction in sepsis is novel. To our best knowledge, the mechanism of cardiac dysfunction in sepsis might be different from that of myocardial ischemia. For example, a clinical study demonstrated that coronary flow in patients with septic shock is similar to or higher than that in patients without septic shock [110]. A high level of circulating catecholamines downregulates the response of the adrenergic receptor (AR) in cardiomyocytes in the state of SICM, thereby blunting the contractile response of cardiomyocytes to catecholamines [111,112,113]. This means that vasopressors for maintaining blood pressure do not work as SICM treatment.
Recent studies have shown that βAR blockers have received unprecedented attention as a septic shock treatment. Catecholamine overstimulation in septic shock may play an important role in SICM development through calcium overload and βAR signaling and βARs downregulation [113,114,115]. In addition, β signaling-mediated calcium loading results in opening of mitochondrial permeability transition pore (MPTP) and increased ROS production that triggers mitochondrial dysfunction and apoptosis [116]. Accumulated evidence has reported that βAR blockade for sepsis reduces arrhythmogenesis, prevents SICM, and even improves mortality [117,118,119]. Notably, βAR blockers are an attractive strategy against sepsis and inhibit the excessive release of catecholamines and mitochondrial dysfunction, preventing the hypermetabolic state in sepsis. Furthermore, β1AR blockade decreases heart rate and prolongs the filling time of the left ventricle, thereby increasing single-beat output and maintaining cardiac output.
5.5. Other Approaches
Having discussed mitochondrial treatment in the myocardium, we discuss approaches to treating mitochondrial dysfunction itself, not just in the myocardium.
One approach to treat mitochondrial dysfunction is to activate cellular programs that replenish damaged proteins and promote mitochondrial biogenesis. PGC1α, a transcriptional activator that interacts with PPAR gamma, is recognized as an important regulator that determines the cellular production of mtDNA-dependent mitochondrial proteins. Various agents were identified as agonists of the PPAR γ, including pioglitazone and rosiglitazone. Studies revealed that these agents can potently induce mitochondrial biosynthesis in animals and humans and prevent cell dysfunction and cell death in response to mitochondria-damaging stimuli [120].
Another way to promote mitochondrial biosynthesis is with sirtuin activators. Resveratrol is a potent sirtuin-1 (Sirt1) activator, that promotes mitochondrial biogenesis, enhances oxidative metabolic capacity, and shows efficacy in animal models of cardiovascular disease, metabolic syndromes, and muscle disease. Additionally, the administration of human recombinant transcription Factor A, a mitochondrial protein with mitochondrial target sequences modulates mtDNA replication, and rhTFAM reduces mortality in animal models of sepsis [121,122,123].
Another approach is to regulate pyroptosis in cardiomyocytes. GSDMD-dependent pyroptosis is considered to be one of the causes of SICM. Irisin, which is a product of fibronectin type III domain-containing protein 5, protects heart from inflammation via upregulation of mitochondrial ubiquitin ligase (MITOL). Irisin attenuates cardiac dysfunction and cardiac damage in sepsis by activating MITOL and inhibiting GSDMD-dependent pyroptosis in vivo and in vitro [124].
In addition, inhibition of ferroptosis may be also effective. Ferroptosis is one of the critical mechanisms contributing to SICM. Ferrostatin-1 (Fer-1) is a suppressor of ferroptosis by inhibition of lipid peroxidation. Fer-1 improves survival rate and cardiac dysfunction of septic mice by attenuating ROS damage in mitochondrial [125]. Moreover, Resveratrol, a Sirt1 activator, also inhibits ferroptosis. Zeng et al. reported the SICM in CLP rats was induced by mitochondrial dysfunction, increased lipid peroxidation, and reduction in Sirt1/NF-E2-related factor 2 (Nirf2) axis which induces ferroptosis. Intriguingly, high dose of Resveratrol attenuates ferroptosis via upregulation of Sirt1/Nrf2 signaling pathways and improves SICM [126].
Another method to restore mitochondrial function is to directly transplant high-quality normal mitochondria into target tissues. In vivo, mitochondria injected or perfused into cardiac tissue are rapidly taken up by cardiac cells. Furthermore, these studies reveal that mitochondrial transplantation increases myocardial energy production and decreases cell death [127,128].
6. Conclusions
SICM represents a significant manifestation of sepsis linked with a poor prognosis, and this review delineates the involvement of mitochondrial dysfunction in the SICM pathogenesis. The mechanisms leading to mitochondrial dysfunction range from mitochondrial structural disorders to abnormal mitochondrial metabolism, and the temporal sequence of these mechanisms are not clearly understood. Evidence has accumulated from numerous laboratory experiments and clinical data that ATP depletion due to metabolic abnormalities is a contributing factor in SICM, which may involve mechanisms that differ from known metabolic pathways in SICM. Furthermore, even the extent to which each mechanism contributes to mitochondrial dysfunction is currently unknown. Mitochondrial metabolism, which is activated in sepsis, can be protective if moderate and progress detrimentally if excessive. This means that SICM may represent an adaptive protective mechanism with a trade-off between short-term organ function and long-term tissue viability. On the other hand, persistent mitochondrial abnormalities that do not recover may be involved in the transition from adaptive to maladaptive organ dysfunction. Therefore, the therapeutic strategy for SICM would be to ensure that the protective effect is not compromised and to provide timely therapeutic intervention.
We need to establish a definition and diagnostic criteria for SICM. We believe that increased knowledge of the molecular mechanisms associated with myocardial cell death and its mitochondrial dysfunction in sepsis will facilitate the development of targeted therapies for SICM.
Author Contributions
T.K. and S.K. equally drafted this paper and prepared the figures and tables; M.O., the corresponding author, completed this manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
The present review was supported by Japan Society for the Promotion of Science Grant 20K17852, 21K09009, and The Suhara Memorial Foundation.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data available in a publicly accessible repository.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
SICM, sepsis-induced cardiomyopathy; ATP, adenosine triphosphate; TNF, tumor necrosis factor; IL, interleukin; NO, nitric oxide; iNOS, inducible NO synthase; ROS, reactive oxygen species; FAO, fatty acid oxidation; OXOHOS, oxidative phosphorylation; PAMPS, pathogen-associated molecular patterns; LPS, lipopolysaccharide; DAMPS, damage-associated molecular patterns, CLP, cecal ligation and puncture; Drp1, dynamin-related protein 1; OPA1, optic atrophy 1; PGC, peroxisome proliferator-activated receptor gamma coactivator; PPAR, peroxisome proliferator-activated receptor; T-fam, transcription factor A; SR, sarcoplasmic reticulum; mPTP, mitochondrial permeability transition pore; RyR, ryanodine receptor; SERCA, sarcoplasmic/endoplasmic reticulum Ca-ATPase; ADP, adenosine diphosphate; mt, mitochondria; NF, nuclear factor; NADPH, nicotinamide adenine dinucleotide phosphate; UCPs, uncoupling proteins; TG, triglyceride; FA, fatty acid; CPT, carnitine palmitoyl transferase; PDK, phosphoinositide-dependent kinase; CoA, coenzyme A; CD36, cluster of differentiation 36; ACSL, long-chain acyl CoA synthase; FABP, Fatty Acid Binding Protein; TCA, tricarboxylic acid; LDs, lipid droplets; NLR, Nucleotide-binding multimeric domain-like receptors; NLRP3, NLR family pyrin domain containing 3; GSDMD, Gasdermin D; GSH, glutathione; GPX4, glutathione peroxidase 4; AR, adrenergic receptor, SEM, scanning electron microscope; lncRNAs, long noncoding RNAs; MIAT, myocardial infarction-associated transcript; TRAF, TNF receptor-associated factor; RMRP, receptor-activated modifying protein; HSPA4, heat shock protein 70 kD protein 4; MMP, mitochondrial membrane potential; Xist, X-inactive specific transcript RNA; HL-1, cardiac muscle cells; SORBS2, sorbin and src-homology 3 domian containing2; NDUFA4, NADH dehydrogenase ubiquinone 1 alpha sub complex subunit 4; SOX2, SRY-box transcription factor 2; EZH2, enhancer of zeste 2 polycomb repressive complex 2 subunit; USP22, ubiquitin specific peptidase 22; Nrf2, NF-E2-related factor 2; MITOL, mitochondrial ubiquitin ligase; Fer-1, Ferrostatin-1; rhTFAM, recombinant human TFAM protein.
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, C.; Scherag, A.; Adhikari, N.K.; Hartog, C.S.; Tsaganos, T.; Schlattmann, P.; Angus, D.C.; Reinhart, K.; International Forum of Acute Care Trialists. Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. Am. J. Respir. Crit. Care Med. 2016, 193, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Antonucci, E.; Fiaccadori, E.; Donadello, K.; Taccone, F.S.; Franchi, F.; Scolletta, S. Myocardial depression in sepsis: From pathogenesis to clinical manifestations and treatment. J. Crit. Care 2014, 29, 500–511. [Google Scholar] [CrossRef]
- Ehrman, R.R.; Sullivan, A.N.; Favot, M.J.; Sherwin, R.L.; Reynolds, C.A.; Abidov, A.; Levy, P.D. Pathophysiology, echocardiographic evaluation, biomarker findings, and prognostic implications of septic cardiomyopathy: A review of the literature. Crit. Care 2018, 22, 112. [Google Scholar] [CrossRef]
- Orde, S.R.; Pulido, J.N.; Masaki, M.; Gillespie, S.; Spoon, J.N.; Kane, G.C.; Oh, J.K. Outcome prediction in sepsis: Speckle tracking echocardiography based assessment of myocardial function. Crit. Care 2014, 18, R149. [Google Scholar] [CrossRef]
- Vieillard-Baron, A.; Caille, V.; Charron, C.; Belliard, G.; Page, B.; Jardin, F. Actual incidence of global left ventricular hypokinesia in adult septic shock. Crit. Care Med. 2008, 36, 1701–1706. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, O.; Bhardwaj, R.D.; Bernard, S.; Zdunek, S.; Barnabé-Heider, F.; Walsh, S.; Zupicich, J.; Alkass, K.; Buchholz, B.A.; Druid, H.; et al. Evidence for cardiomyocyte renewal in humans. Science 2009, 324, 98–102. [Google Scholar] [CrossRef]
- Galluzzi, L.; Vitale, I.; Aaronson, S.A.; Abrams, J.M.; Adam, D.; Agostinis, P.; Alnemri, E.S.; Altucci, L.; Amelio, I.; Andrews, D.W.; et al. Molecular mechanisms of cell death: Recommendations of the Nomenclature Committee on Cell Death 2018. Cell Death Differ. 2018, 25, 486–541. [Google Scholar] [CrossRef] [PubMed]
- Mishra, P.K.; Adameova, A.; Hill, J.A.; Baines, C.P.; Kang, P.M.; Downey, J.M.; Narula, J.; Takahashi, M.; Abbate, A.; Piristine, H.C.; et al. Guidelines for evaluating myocardial cell death. Am. J. Physiol. Heart Circ. Physiol. 2019, 317, H891–H922. [Google Scholar] [CrossRef]
- Nedeva, C. Inflammation and Cell Death of the Innate and Adaptive Immune System during Sepsis. Biomolecules 2021, 11, 1011. [Google Scholar] [CrossRef]
- Picca, A.; Calvani, R.; Coelho-Junior, H.J.; Marzetti, E. Cell Death and Inflammation: The Role of Mitochondria in Health and Disease. Cells 2021, 10, 537. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Yan, Y.; Niu, F.; Wang, Y.; Chen, X.; Su, G.; Liu, Y.; Zhao, X.; Qian, L.; Liu, P.; et al. Ferroptosis: A cell death connecting oxidative stress, inflammation and cardiovascular diseases. Cell Death Discov. 2021, 7, 193. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Peng, X.; Guo, L.; Zhao, Y.; Cheng, Q. Sepsis causes heart injury through endoplasmic reticulum stress-mediated apoptosis signaling pathway. Int. J. Clin. Exp. Pathol. 2020, 13, 964–971. [Google Scholar] [PubMed]
- Kawaguchi, S.; Okada, M.; Ijiri, E.; Koga, D.; Watanabe, T.; Hayashi, K.; Kashiwagi, Y.; Fujita, S.; Hasebe, N. β3-Adrenergic receptor blockade reduces mortality in endotoxin-induced heart failure by suppressing induced nitric oxide synthase and saving cardiac metabolism. Am. J. Physiol. Heart Circ. Physiol. 2020, 318, H283–H294. [Google Scholar] [CrossRef] [PubMed]
- Guo, R.; Li, G. Tanshinone modulates the expression of Bcl-2 and Bax in cardiomyocytes and has a protective effect in a rat model of myocardial ischemia-reperfusion. Hell. J. Cardiol. 2018, 59, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Savill, J.; Fadok, V. Corpse clearance defines the meaning of cell death. Nature 2000, 407, 784–788. [Google Scholar] [CrossRef] [PubMed]
- Haslett, C. Granulocyte apoptosis and inflammatory disease. Br. Med. Bull. 1997, 53, 669–683. [Google Scholar] [CrossRef]
- Zorc-Pleskovic, R.; Alibegović, A.; Zorc, M.; Milutinović, A.; Radovanović, N.; Petrović, D. Apoptosis of cardiomyocytes in myocarditis. Folia Biol. 2006, 52, 6–9. [Google Scholar]
- Singer, M. The role of mitochondrial dysfunction in sepsis-induced multi-organ failure. Virulence 2014, 5, 66–72. [Google Scholar] [CrossRef]
- Moriyama, S.; Okamoto, K.; Tabira, Y.; Kikuta, K.; Kukita, I.; Hamaguchi, M.; Kitamura, N. Evaluation of oxygen consumption and resting energy expenditure in critically ill patients with systemic inflammatory response syndrome. Crit. Care Med. 1999, 27, 2133–2136. [Google Scholar] [CrossRef]
- Lopaschuk, G.D.; Karwi, Q.G.; Tian, R.; Wende, A.R.; Abel, E.D. Cardiac Energy Metabolism in Heart Failure. Circ. Res. 2021, 128, 1487–1513. [Google Scholar] [CrossRef] [PubMed]
- Mokranjac, D.; Neupert, W. Energetics of protein translocation into mitochondria. Biochim. Biophys. Acta 2008, 1777, 758–762. [Google Scholar] [CrossRef] [PubMed]
- Preau, S.; Vodovar, D.; Jung, B.; Lancel, S.; Zafrani, L.; Flatres, A.; Oualha, M.; Voiriot, G.; Jouan, Y.; Joffre, J.; et al. Energetic dysfunction in sepsis: A narrative review. Ann. Intensive Care 2021, 11, 104. [Google Scholar] [CrossRef] [PubMed]
- Perocchi, F.; Gohil, V.M.; Girgis, H.S.; Bao, X.R.; McCombs, J.E.; Palmer, A.E.; Mootha, V.K. MICU1 encodes a mitochondrial EF hand protein required for Ca2+ uptake. Nature 2010, 467, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, R.; Zhang, H.; Kim, J.W.; Shimoda, L.; Dang, C.V.; Semenza, G.L. HIF-1 regulates cytochrome oxidase subunits to optimize efficiency of respiration in hypoxic cells. Cell 2007, 129, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Thota, V.; Dee, L.; Olson, J.; Uretz, E.; Parrillo, J.E. Tumor necrosis factor alpha and interleukin 1beta are responsible for in vitro myocardial cell depression induced by human septic shock serum. J. Exp. Med. 1996, 183, 949–958. [Google Scholar] [CrossRef] [PubMed]
- Pathan, N.; Franklin, J.L.; Eleftherohorinou, H.; Wright, V.J.; Hemingway, C.A.; Waddell, S.J.; Griffiths, M.; Dennis, J.L.; Relman, D.A.; Harding, S.E.; et al. Myocardial depressant effects of interleukin 6 in meningococcal sepsis are regulated by p38 mitogen-activated protein kinase. Crit. Care Med. 2011, 39, 1692–1711. [Google Scholar] [CrossRef]
- Cain, B.S.; Meldrum, D.R.; Dinarello, C.A.; Meng, X.; Joo, K.S.; Banerjee, A.; Harken, A.H. Tumor necrosis factor-alpha and interleukin-1beta synergistically depress human myocardial function. Crit. Care Med. 1999, 27, 1309–1318. [Google Scholar] [CrossRef]
- Kumar, A.; Brar, R.; Wang, P.; Dee, L.; Skorupa, G.; Khadour, F.; Schulz, R.; Parrillo, J.E. Role of nitric oxide and cGMP in human septic serum-induced depression of cardiac myocyte contractility. Am. J. Physiol. 1999, 276, R265–R276. [Google Scholar] [CrossRef]
- Schulz, R.; Nava, E.; Moncada, S. Induction and potential biological relevance of a Ca2+-independent nitric oxide synthase in the myocardium. Br. J. Pharmacol. 1992, 105, 575–580. [Google Scholar] [CrossRef]
- Decking, U.K.; Flesche, C.W.; Gödecke, A.; Schrader, J. Endotoxin-induced contractile dysfunction in guinea pig hearts is not mediated by nitric oxide. Am. J. Physiol. 1995, 268, H2460–H2465. [Google Scholar] [CrossRef] [PubMed]
- Solomon, M.A.; Correa, R.; Alexander, H.R.; Koev, L.A.; Cobb, J.P.; Kim, D.K.; Roberts, W.C.; Quezado, Z.M.; Scholz, T.D.; Cunnion, R.E.; et al. Myocardial energy metabolism and morphology in a canine model of sepsis. Am. J. Physiol. 1994, 266, H757–H768. [Google Scholar] [CrossRef] [PubMed]
- Haileselassie, B.; Su, E.; Pozios, I.; Niño, D.F.; Liu, H.; Lu, D.Y.; Ventoulis, I.; Fulton, W.B.; Sodhi, C.P.; Hackam, D.; et al. Myocardial oxidative stress correlates with left ventricular dysfunction on strain echocardiography in a rodent model of sepsis. Intensive Care Med. Exp. 2017, 5, 21. [Google Scholar] [CrossRef] [PubMed]
- Singer, M. Critical illness and flat batteries. Crit. Care 2017, 21, 309. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Villamil, J.P.; D’Annunzio, V.; Finocchietto, P.; Holod, S.; Rebagliati, I.; Pérez, H.; Peralta, J.G.; Gelpi, R.J.; Poderoso, J.J.; Carreras, M.C. Cardiac-specific overexpression of thioredoxin 1 attenuates mitochondrial and myocardial dysfunction in septic mice. Int. J. Biochem. Cell Biol. 2016, 81, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Preau, S.; Delguste, F.; Yu, Y.; Remy-Jouet, I.; Richard, V.; Saulnier, F.; Boulanger, E.; Neviere, R. Endotoxemia Engages the RhoA Kinase Pathway to Impair Cardiac Function By Altering Cytoskeleton, Mitochondrial Fission, and Autophagy. Antioxid. Redox Signal 2016, 24, 529–542. [Google Scholar] [CrossRef] [PubMed]
- Hobai, I.A.; Edgecomb, J.; LaBarge, K.; Colucci, W.S. Dysregulation of intracellular calcium transporters in animal models of sepsis-induced cardiomyopathy. Shock 2015, 43, 3–15. [Google Scholar] [CrossRef]
- Drosatos, K.; Lymperopoulos, A.; Kennel, P.J.; Pollak, N.; Schulze, P.C.; Goldberg, I.J. Pathophysiology of sepsis-related cardiac dysfunction: Driven by inflammation, energy mismanagement, or both? Curr. Heart Fail. Rep. 2015, 12, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Drosatos, K.; Khan, R.S.; Trent, C.M.; Jiang, H.; Son, N.H.; Blaner, W.S.; Homma, S.; Schulze, P.C.; Goldberg, I.J. Peroxisome proliferator-activated receptor-γ activation prevents sepsis-related cardiac dysfunction and mortality in mice. Circ. Heart Fail. 2013, 6, 550–562. [Google Scholar] [CrossRef]
- Yuan, H.; Perry, C.N.; Huang, C.; Iwai-Kanai, E.; Carreira, R.S.; Glembotski, C.C.; Gottlieb, R.A. LPS-induced autophagy is mediated by oxidative signaling in cardiomyocytes and is associated with cytoprotection. Am. J. Physiol. Heart Circ. Physiol. 2009, 296, H470–H479. [Google Scholar] [CrossRef]
- Andreis, D.T.; Singer, M. Catecholamines for inflammatory shock: A Jekyll-and-Hyde conundrum. Intensive Care Med. 2016, 42, 1387–1397. [Google Scholar] [CrossRef]
- Redfors, B.; Shao, Y.; Omerovic, E. Is stress-induced cardiomyopathy (takotsubo) the cause of elevated cardiac troponins in a subset of septic patients? Intensive Care Med. 2014, 40, 757–758. [Google Scholar] [CrossRef] [PubMed]
- Zou, X.; Xu, J.; Yao, S.; Li, J.; Yang, Y.; Yang, L. Endoplasmic reticulum stress-mediated autophagy protects against lipopolysaccharide-induced apoptosis in HL-1 cardiomyocytes. Exp. Physiol. 2014, 99, 1348–1358. [Google Scholar] [CrossRef]
- Piquereau, J.; Godin, R.; Deschênes, S.; Bessi, V.L.; Mofarrahi, M.; Hussain, S.N.; Burelle, Y. Protective role of PARK2/Parkin in sepsis-induced cardiac contractile and mitochondrial dysfunction. Autophagy 2013, 9, 1837–1851. [Google Scholar] [CrossRef] [PubMed]
- Vanasco, V.; Saez, T.; Magnani, N.D.; Pereyra, L.; Marchini, T.; Corach, A.; Vaccaro, M.I.; Corach, D.; Evelson, P.; Alvarez, S. Cardiac mitochondrial biogenesis in endotoxemia is not accompanied by mitochondrial function recovery. Free Radic. Biol. Med. 2014, 77, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Bae, S.H.; Ryu, J.C.; Kwon, Y.; Oh, J.H.; Kwon, J.; Moon, J.S.; Kim, K.; Miyawaki, A.; Lee, M.G.; et al. SESN2/sestrin2 suppresses sepsis by inducing mitophagy and inhibiting NLRP3 activation in macrophages. Autophagy 2016, 12, 1272–1291. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X. Intensified quality control of isolation, disinfection and sterilization. Zhonghua Hu Li Za Zhi 1991, 26, 533–535. [Google Scholar] [PubMed]
- Kohlhaas, M.; Maack, C. Calcium release microdomains and mitochondria. Cardiovasc. Res. 2013, 98, 259–268. [Google Scholar] [CrossRef]
- Kohlhaas, M.; Liu, T.; Knopp, A.; Zeller, T.; Ong, M.F.; Böhm, M.; O’Rourke, B.; Maack, C. Elevated cytosolic Na+ increases mitochondrial formation of reactive oxygen species in failing cardiac myocytes. Circulation 2010, 121, 1606–1613. [Google Scholar] [CrossRef]
- Brookes, P.S.; Yoon, Y.; Robotham, J.L.; Anders, M.W.; Sheu, S.S. Calcium, ATP, and ROS: A mitochondrial love-hate triangle. Am. J. Physiol. Cell Physiol. 2004, 287, C817–C833. [Google Scholar] [CrossRef]
- Santulli, G.; Xie, W.; Reiken, S.R.; Marks, A.R. Mitochondrial calcium overload is a key determinant in heart failure. Proc. Natl. Acad. Sci. USA 2015, 112, 11389–11394. [Google Scholar] [CrossRef] [PubMed]
- Rudiger, A.; Dyson, A.; Felsmann, K.; Carré, J.E.; Taylor, V.; Hughes, S.; Clatworthy, I.; Protti, A.; Pellerin, D.; Lemm, J.; et al. Early functional and transcriptomic changes in the myocardium predict outcome in a long-term rat model of sepsis. Clin. Sci. 2013, 124, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Ferdinandy, P.; Danial, H.; Ambrus, I.; Rothery, R.A.; Schulz, R. Peroxynitrite is a major contributor to cytokine-induced myocardial contractile failure. Circ. Res. 2000, 87, 241–247. [Google Scholar] [CrossRef]
- Bosson, S.; Kuenzig, M.; Schwartz, S.I. Increased survival with calcium antagonists in antibiotic-treated bacteremia. Circ. Shock 1986, 19, 69–74. [Google Scholar] [PubMed]
- Meldrum, D.R.; Ayala, A.; Perrin, M.M.; Ertel, W.; Chaudry, I.H. Diltiazem restores IL-2, IL-3, IL-6, and IFN-γ synthesis and decreases host susceptibility to sepsis following hemorrhage. J. Surg. Res. 1991, 51, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Hotchkiss, R.S.; Osborne, D.F.; Lappas, G.D.; Karl, I.E. Calcium antagonists decrease plasma and tissue concentrations of tumor necrosis factor-alpha, interleukin-1 beta, and interleukin-1 alpha in a mouse model of endotoxin. Shock 1995, 3, 337–342. [Google Scholar] [PubMed]
- Bosson, S.; Kuenzig, M.; Schwartz, S.I. Verapamil improves cardiac function and increases survival in canine E. coli endotoxin shock. Circ. Shock 1985, 16, 307–316. [Google Scholar]
- Wiewel, M.A.; van Vught, L.A.; Scicluna, B.P.; Hoogendijk, A.J.; Frencken, J.F.; Zwinderman, A.H.; Horn, J.; Cremer, O.L.; Bonten, M.J.; Schultz, M.J.; et al. Prior Use of Calcium Channel Blockers Is Associated With Decreased Mortality in Critically Ill Patients with Sepsis: A Prospective Observational Study. Crit. Care Med. 2017, 45, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.C.; Lee, M.G.; Lee, W.C.; Lai, C.C.; Chao, C.C.; Hsu, W.H.; Chang, S.S.; Lee, M. Preadmission Use of Calcium Channel Blocking Agents Is Associated with Improved Outcomes in Patients With Sepsis: A Population-Based Propensity Score-Matched Cohort Study. Crit. Care Med. 2017, 45, 1500–1508. [Google Scholar] [CrossRef]
- Wasyluk, W.; Nowicka-Stążka, P.; Zwolak, A. Heart Metabolism in Sepsis-Induced Cardiomyopathy-Unusual Metabolic Dysfunction of the Heart. Int. J. Environ. Res. Public Health 2021, 18, 7598. [Google Scholar] [CrossRef]
- Wang, S.; Kandadi, M.R.; Ren, J. Double knockout of Akt2 and AMPK predisposes cardiac aging without affecting lifespan: Role of autophagy and mitophagy. Biochim. Biophys. Acta Mol. Basis Dis. 2019, 1865, 1865–1875. [Google Scholar] [CrossRef]
- Nordenström, J.; Carpenter, W.A.; Askanazi, J.; Robin, A.P.; Elwyn, D.H.; Hensle, T.W.; Kinney, J.M. Metabolic utilization of intravenous fat emulsion during total parenteral nutrition. Ann. Surg. 1982, 196, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Rittig, N.; Bach, E.; Thomsen, H.H.; Pedersen, S.B.; Nielsen, T.S.; Jørgensen, J.O.; Jessen, N.; Møller, N. Regulation of Lipolysis and Adipose Tissue Signaling during Acute Endotoxin-Induced Inflammation: A Human Randomized Crossover Trial. PLoS ONE 2016, 11, e0162167. [Google Scholar] [CrossRef] [PubMed]
- Hiukka, A.; Maranghi, M.; Matikainen, N.; Taskinen, M.R. PPARα: An emerging therapeutic target in diabetic microvascular damage. Nat. Rev. Endocrinol. 2010, 6, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Drosatos, K.; Drosatos-Tampakaki, Z.; Khan, R.; Homma, S.; Schulze, P.C.; Zannis, V.I.; Goldberg, I.J. Inhibition of c-Jun-N-terminal kinase increases cardiac peroxisome proliferator-activated receptor α expression and fatty acid oxidation and prevents lipopolysaccharide-induced heart dysfunction. J. Biol. Chem. 2011, 286, 36331–36339. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Adrogue, J.V.; Golfman, L.; Uray, I.; Lemm, J.; Youker, K.; Noon, G.P.; Frazier, O.H.; Taegtmeyer, H. Intramyocardial lipid accumulation in the failing human heart resembles the lipotoxic rat heart. Faseb J. 2004, 18, 1692–1700. [Google Scholar] [CrossRef] [PubMed]
- Chokshi, A.; Drosatos, K.; Cheema, F.H.; Ji, R.; Khawaja, T.; Yu, S.; Kato, T.; Khan, R.; Takayama, H.; Knöll, R.; et al. Ventricular assist device implantation corrects myocardial lipotoxicity, reverses insulin resistance, and normalizes cardiac metabolism in patients with advanced heart failure. Circulation 2012, 125, 2844–2853. [Google Scholar] [CrossRef]
- Hickson-Bick, D.L.; Buja, L.M.; McMillin, J.B. Palmitate-mediated alterations in the fatty acid metabolism of rat neonatal cardiac myocytes. J. Mol. Cell Cardiol. 2000, 32, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Sparagna, G.C.; Hickson-Bick, D.L.; Buja, L.M.; McMillin, J.B. A metabolic role for mitochondria in palmitate-induced cardiac myocyte apoptosis. Am. J. Physiol. Heart Circ. Physiol. 2000, 279, H2124–H2132. [Google Scholar] [CrossRef]
- Listenberger, L.L.; Ory, D.S.; Schaffer, J.E. Palmitate-induced apoptosis can occur through a ceramide-independent pathway. J. Biol. Chem. 2001, 276, 14890–14895. [Google Scholar] [CrossRef]
- Du, X.; Edelstein, D.; Obici, S.; Higham, N.; Zou, M.H.; Brownlee, M. Insulin resistance reduces arterial prostacyclin synthase and eNOS activities by increasing endothelial fatty acid oxidation. J. Clin. Investig. 2006, 116, 1071–1080. [Google Scholar] [CrossRef] [PubMed]
- Borradaile, N.M.; Buhman, K.K.; Listenberger, L.L.; Magee, C.J.; Morimoto, E.T.; Ory, D.S.; Schaffer, J.E. A critical role for eukaryotic elongation factor 1A-1 in lipotoxic cell death. Mol. Biol. Cell 2006, 17, 770–778. [Google Scholar] [CrossRef] [PubMed]
- Evavold, C.L.; Hafner-Bratkovič, I.; Devant, P.; D’Andrea, J.M.; Ngwa, E.M.; Boršić, E.; Doench, J.G.; LaFleur, M.W.; Sharpe, A.H.; Thiagarajah, J.R.; et al. Control of gasdermin D oligomerization and pyroptosis by the Ragulator-Rag-mTORC1 pathway. Cell 2021, 184, 4495–4511. [Google Scholar] [CrossRef] [PubMed]
- Rao, Z.; Zhu, Y.; Yang, P.; Chen, Z.; Xia, Y.; Qiao, C.; Liu, W.; Deng, H.; Li, J.; Ning, P.; et al. Pyroptosis in inflammatory diseases and cancer. Theranostics 2022, 12, 4310–4329. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Zhou, H.; Wu, H.; Wu, Q.; Duan, M.; Deng, W.; Tang, Q. STING-IRF3 contributes to lipopolysaccharide-induced cardiac dysfunction, inflammation, apoptosis and pyroptosis by activating NLRP3. Redox Biol. 2019, 24, 101215. [Google Scholar] [CrossRef]
- Toldo, S.; Abbate, A. The role of the NLRP3 inflammasome and pyroptosis in cardiovascular diseases. Nat. Rev. Cardiol. 2024, 21, 219–237. [Google Scholar] [CrossRef]
- Fujimura, K.; Karasawa, T.; Komada, T.; Yamada, N.; Mizushina, Y.; Baatarjav, C.; Matsumura, T.; Otsu, K.; Takeda, N.; Mizukami, H.; et al. NLRP3 inflammasome-driven IL-1β and IL-18 contribute to lipopolysaccharide-induced septic cardiomyopathy. J. Mol. Cell. Cardiol. 2023, 180, 58–68. [Google Scholar] [CrossRef]
- Shi, J.; Zhao, Y.; Wang, K.; Shi, X.; Wang, Y.; Huang, H.; Zhuang, Y.; Cai, T.; Wang, F.; Shao, F. Cleavage of GSDMD by inflammatory caspases determines pyroptotic cell death. Nature 2015, 526, 660–665. [Google Scholar] [CrossRef]
- Dai, S.; Ye, B.; Zhong, L.; Chen, Y.; Hong, G.; Zhao, G.; Su, L.; Lu, Z. GSDMD Mediates LPS-Induced Septic Myocardial Dysfunction by Regulating ROS-dependent NLRP3 Inflammasome Activation. Front. Cell Dev. Biol. 2021, 9, 779432. [Google Scholar] [CrossRef]
- Zhang, W.W.; Wang, S.S.; Ding, Y.D.; Wu, X.Y.; Chen, T.; Gao, Y.; Jin, S.W.; Zhang, P.H. Cardiac Resolvin D2 ameliorates sepsis-induced cardiomyopathy via inhibiting Caspase-11/GSDMD dependent pyroptosis. Free Radic. Biol. Med. 2024, 215, 64–76. [Google Scholar] [CrossRef]
- Fang, X.; Wang, H.; Han, D.; Xie, E.; Yang, X.; Wei, J.; Gu, S.; Gao, F.; Zhu, N.; Yin, X.; et al. Ferroptosis as a target for protection against cardiomyopathy. Proc. Natl. Acad. Sci. USA 2019, 116, 2672–2680. [Google Scholar] [CrossRef] [PubMed]
- Ye, H.; Hu, H.; Zhou, X.; Dong, M.; Ren, J. Targeting ferroptosis in the maintenance of mitochondrial homeostasis in the realm of septic cardiomyopathy. Curr. Opin. Pharmacol. 2024, 74, 102430. [Google Scholar] [CrossRef] [PubMed]
- Stockwell, B.R.; Jiang, X.; Gu, W. Emerging Mechanisms and Disease Relevance of Ferroptosis. Trends Cell Biol. 2020, 30, 478–490. [Google Scholar] [CrossRef] [PubMed]
- Forcina, G.C.; Dixon, S.J. GPX4 at the Crossroads of Lipid Homeostasis and Ferroptosis. Proteomics 2019, 19, e1800311. [Google Scholar] [CrossRef] [PubMed]
- Huo, L.; Liu, C.; Yuan, Y.; Liu, X.; Cao, Q. Pharmacological inhibition of ferroptosis as a therapeutic target for sepsis-associated organ damage. Eur. J. Med. Chem. 2023, 257, 115438. [Google Scholar] [CrossRef] [PubMed]
- Zabet, M.H.; Mohammadi, M.; Ramezani, M.; Khalili, H. Effect of high-dose Ascorbic acid on vasopressor’s requirement in septic shock. J. Res. Pharm. Pract. 2016, 5, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Fujii, T.; Luethi, N.; Young, P.J.; Frei, D.R.; Eastwood, G.M.; French, C.J.; Deane, A.M.; Shehabi, Y.; Hajjar, L.A.; Oliveira, G.; et al. Effect of Vitamin C, Hydrocortisone, and Thiamine vs Hydrocortisone Alone on Time Alive and Free of Vasopressor Support Among Patients with Septic Shock: The VITAMINS Randomized Clinical Trial. JAMA 2020, 323, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Liaw, K.; Sharma, R.; Zhang, Z.; Kannan, S.; Kannan, R.M. Targeting Mitochondrial Dysfunction and Oxidative Stress in Activated Microglia using Dendrimer-Based Therapeutics. Theranostics 2018, 8, 5529–5547. [Google Scholar] [CrossRef]
- Szeto, H.H. Cell-permeable, mitochondrial-targeted, peptide antioxidants. Aaps J. 2006, 8, E277–E283. [Google Scholar] [CrossRef]
- Lowes, D.A.; Thottakam, B.M.; Webster, N.R.; Murphy, M.P.; Galley, H.F. The mitochondria-targeted antioxidant MitoQ protects against organ damage in a lipopolysaccharide-peptidoglycan model of sepsis. Free Radic. Biol. Med. 2008, 45, 1559–1565. [Google Scholar] [CrossRef]
- Supinski, G.S.; Murphy, M.P.; Callahan, L.A. MitoQ administration prevents endotoxin-induced cardiac dysfunction. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2009, 297, R1095–R1102. [Google Scholar] [CrossRef]
- Patil, N.K.; Parajuli, N.; MacMillan-Crow, L.A.; Mayeux, P.R. Inactivation of renal mitochondrial respiratory complexes and manganese superoxide dismutase during sepsis: Mitochondria-targeted antioxidant mitigates injury. Am. J. Physiol. Renal Physiol. 2014, 306, F734–F743. [Google Scholar] [CrossRef]
- Wang, P.F.; Xie, K.; Cao, Y.X.; Zhang, A. Hepatoprotective Effect of Mitochondria-Targeted Antioxidant Mito-TEMPO against Lipopolysaccharide-Induced Liver Injury in Mouse. Mediat. Inflamm. 2022, 2022, 6394199. [Google Scholar] [CrossRef]
- Liu, Y.; Yang, W.; Sun, X.; Xie, L.; Yang, Y.; Sang, M.; Jiao, R. SS31 Ameliorates Sepsis-Induced Heart Injury by Inhibiting Oxidative Stress and Inflammation. Inflammation 2019, 42, 2170–2180. [Google Scholar] [CrossRef]
- Cannavo, A.; Koch, W.J. Targeting β3-Adrenergic Receptors in the Heart: Selective Agonism and β-Blockade. J. Cardiovasc. Pharmacol. 2017, 69, 71–78. [Google Scholar] [CrossRef]
- Aragón, J.P.; Condit, M.E.; Bhushan, S.; Predmore, B.L.; Patel, S.S.; Grinsfelder, D.B.; Gundewar, S.; Jha, S.; Calvert, J.W.; Barouch, L.A.; et al. Beta3-adrenoreceptor stimulation ameliorates myocardial ischemia-reperfusion injury via endothelial nitric oxide synthase and neuronal nitric oxide synthase activation. J. Am. Coll. Cardiol. 2011, 58, 2683–2691. [Google Scholar] [CrossRef]
- Niu, X.; Watts, V.L.; Cingolani, O.H.; Sivakumaran, V.; Leyton-Mange, J.S.; Ellis, C.L.; Miller, K.L.; Vandegaer, K.; Bedja, D.; Gabrielson, K.L.; et al. Cardioprotective effect of beta-3 adrenergic receptor agonism: Role of neuronal nitric oxide synthase. J. Am. Coll. Cardiol. 2012, 59, 1979–1987. [Google Scholar] [CrossRef] [PubMed]
- Michel, L.Y.M.; Farah, C.; Balligand, J.L. The Beta3 Adrenergic Receptor in Healthy and Pathological Cardiovascular Tissues. Cells 2020, 9, 2584. [Google Scholar] [CrossRef]
- Kawaguchi, S.; Okada, M. Cardiac Metabolism in Sepsis. Metabolites 2021, 11, 846. [Google Scholar] [CrossRef] [PubMed]
- Xing, P.C.; An, P.; Hu, G.Y.; Wang, D.L.; Zhou, M.J. LncRNA MIAT Promotes Inflammation and Oxidative Stress in Sepsis-Induced Cardiac Injury by Targeting miR-330-5p/TRAF6/NF-κB Axis. Biochem. Genet. 2020, 58, 783–800. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Cai, Y.; Lai, X.; Wang, Z.; Wei, S.; Tan, K.; Xu, M.; Xie, H. lncRNA RMRP Prevents Mitochondrial Dysfunction and Cardiomyocyte Apoptosis via the miR-1-5p/hsp70 Axis in LPS-Induced Sepsis Mice. Inflammation 2020, 43, 605–618. [Google Scholar] [CrossRef]
- Shan, B.; Li, J.Y.; Liu, Y.J.; Tang, X.B.; Zhou, Z.; Luo, L.X. LncRNA H19 Inhibits the Progression of Sepsis-Induced Myocardial Injury via Regulation of the miR-93-5p/SORBS2 Axis. Inflammation 2021, 44, 344–357. [Google Scholar] [CrossRef] [PubMed]
- Liang, D.; Jin, Y.; Lin, M.; Xia, X.; Chen, X.; Huang, A. Down-regulation of Xist and Mir-7a-5p improves LPS-induced myocardial injury. Int. J. Med. Sci. 2020, 17, 2570–2577. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Zheng, X.; Zheng, M.; Wang, L.; Chen, Y.; Shen, Y. Identification of mitochondrial function-associated lncRNAs in septic mice myocardium. J. Cell. Biochem. 2021, 122, 53–68. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Bei, Y.; Shen, S.; Huang, P.; Shi, J.; Zhang, J.; Sun, Q.; Chen, Y.; Yang, Y.; Xu, T.; et al. miR-21-3p controls sepsis-associated cardiac dysfunction via regulating SORBS2. J. Mol. Cell. Cardiol. 2016, 94, 43–53. [Google Scholar] [CrossRef]
- Chen, M.; Guan, Y.; Li, A.; Zhao, Y.Z.; Zhang, L.; Zhang, L.; Gong, Y. LncRNA SOX2OT Mediates Mitochondrial Dysfunction in Septic Cardiomyopathy. DNA Cell Biol. 2019, 38, 1197–1206. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Ye, W.; Shi, B. LncRNA MALAT1 Regulates USP22 Expression through EZH2-Mediated H3K27me3 Modification to Accentuate Sepsis-Induced Myocardial Dysfunction. Cardiovasc. Toxicol. 2022, 22, 813–830. [Google Scholar] [CrossRef] [PubMed]
- Parker, M.M.; Shelhamer, J.H.; Bacharach, S.L.; Green, M.V.; Natanson, C.; Frederick, T.M.; Damske, B.A.; Parrillo, J.E. Profound but reversible myocardial depression in patients with septic shock. Ann. Intern. Med. 1984, 100, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Waisbren, B.A. Bacteremia due to gram-negative bacilli other than the Salmonella; A clinical and therapeutic study. AMA Arch. Intern. Med. 1951, 88, 467–488. [Google Scholar] [CrossRef]
- Cunnion, R.E.; Schaer, G.L.; Parker, M.M.; Natanson, C.; Parrillo, J.E. The coronary circulation in human septic shock. Circulation 1986, 73, 637–644. [Google Scholar] [CrossRef]
- Gulick, T.; Chung, M.K.; Pieper, S.J.; Lange, L.G.; Schreiner, G.F. Interleukin 1 and tumor necrosis factor inhibit cardiac myocyte beta-adrenergic responsiveness. Proc. Natl. Acad. Sci. USA 1989, 86, 6753–6757. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, N.; Hattori, Y.; Akaishi, Y.; Suzuki, Y.; Kemmotsu, O.; Gando, S. Impairment of cardiac β-adrenoceptor cellular signaling by decreased expression of Gsα in septic rabbits. Anesthesiology 2000, 93, 1465–1473. [Google Scholar] [CrossRef] [PubMed]
- Rudiger, A.; Singer, M. Mechanisms of sepsis-induced cardiac dysfunction. Crit. Care Med. 2007, 35, 1599–1608. [Google Scholar] [CrossRef] [PubMed]
- Hunter, J.D.; Doddi, M. Sepsis and the heart. Br. J. Anaesth. 2010, 104, 3–11. [Google Scholar] [CrossRef] [PubMed]
- de Montmollin, E.; Aboab, J.; Mansart, A.; Annane, D. Bench-to-bedside review: β-adrenergic modulation in sepsis. Crit. Care 2009, 13, 230. [Google Scholar] [CrossRef] [PubMed]
- Kontogiannis, C.; Kosmopoulos, M.; Georgiopoulos, G.; Spartalis, M.; Paraskevaidis, I.; Chatzidou, S. Mitochondria in β-adrenergic signaling: Emerging therapeutic perspectives in heart failure and ventricular arrhythmias. J. Thorac. Dis. 2018, 10, S4183–S4185. [Google Scholar] [CrossRef] [PubMed]
- Kakihana, Y.; Nishida, O.; Taniguchi, T.; Okajima, M.; Morimatsu, H.; Ogura, H.; Yamada, Y.; Nagano, T.; Morishima, E.; Matsuda, N. Efficacy and safety of landiolol, an ultra-short-acting β1-selective antagonist, for treatment of sepsis-related tachyarrhythmia (J-Land 3S): A multicentre, open-label, randomised controlled trial. Lancet Respir. Med. 2020, 8, 863–872. [Google Scholar] [CrossRef] [PubMed]
- Ackland, G.L.; Yao, S.T.; Rudiger, A.; Dyson, A.; Stidwill, R.; Poputnikov, D.; Singer, M.; Gourine, A.V. Cardioprotection, attenuated systemic inflammation, and survival benefit of β1-adrenoceptor blockade in severe sepsis in rats. Crit. Care Med. 2010, 38, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Tan, K.; Harazim, M.; Tang, B.; McLean, A.; Nalos, M. The association between premorbid beta blocker exposure and mortality in sepsis—A systematic review. Crit. Care 2019, 23, 298. [Google Scholar] [CrossRef]
- Miglio, G.; Rosa, A.C.; Rattazzi, L.; Collino, M.; Lombardi, G.; Fantozzi, R. PPARγ stimulation promotes mitochondrial biogenesis and prevents glucose deprivation-induced neuronal cell loss. Neurochem. Int. 2009, 55, 496–504. [Google Scholar] [CrossRef]
- Sun, A.Y.; Wang, Q.; Simonyi, A.; Sun, G.Y. Resveratrol as a therapeutic agent for neurodegenerative diseases. Mol. Neurobiol. 2010, 41, 375–383. [Google Scholar] [CrossRef]
- Thomas, R.R.; Khan, S.M.; Smigrodzki, R.M.; Onyango, I.G.; Dennis, J.; Khan, O.M.; Portell, F.R.; Bennett, J.P., Jr. RhTFAM treatment stimulates mitochondrial oxidative metabolism and improves memory in aged mice. Aging 2012, 4, 620–635. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.R.; Khan, S.M.; Portell, F.R.; Smigrodzki, R.M.; Bennett, J.P., Jr. Recombinant human mitochondrial transcription factor A stimulates mitochondrial biogenesis and ATP synthesis, improves motor function after MPTP, reduces oxidative stress and increases survival after endotoxin. Mitochondrion 2011, 11, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Xiong, X.; Lu, L.; Wang, Z.; Ma, J.; Shao, Y.; Liu, Y.; Zhai, M.; Jin, P.; Yang, J.; Zheng, Q.; et al. Irisin attenuates sepsis-induced cardiac dysfunction by attenuating inflammation-induced pyroptosis through a mitochondrial ubiquitin ligase-dependent mechanism. Biomed. Pharmacother. 2022, 152, 113199. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Wang, W.; Zhou, H.; Wu, Q.; Duan, M.; Liu, C.; Wu, H.; Deng, W.; Shen, D.; Tang, Q. Ferritinophagy-mediated ferroptosis is involved in sepsis-induced cardiac injury. Free Radic. Biol. Med. 2020, 160, 303–318. [Google Scholar] [CrossRef]
- Zeng, Y.; Cao, G.; Lin, L.; Zhang, Y.; Luo, X.; Ma, X.; Aiyisake, A.; Cheng, Q. Resveratrol Attenuates Sepsis-Induced Cardiomyopathy in Rats through Anti-Ferroptosis via the Sirt1/Nrf2 Pathway. J. Investig. Surg. 2023, 36, 2157521. [Google Scholar] [CrossRef] [PubMed]
- Cowan, D.B.; Yao, R.; Thedsanamoorthy, J.K.; Zurakowski, D.; Del Nido, P.J.; McCully, J.D. Transit and integration of extracellular mitochondria in human heart cells. Sci. Rep. 2017, 7, 17450. [Google Scholar] [CrossRef]
- McCully, J.D.; Cowan, D.B.; Emani, S.M.; Del Nido, P.J. Mitochondrial transplantation: From animal models to clinical use in humans. Mitochondrion 2017, 34, 127–134. [Google Scholar] [CrossRef]
Figure 1.
A schematic figure of mechanisms of mitochondrial dysfunction in SICM. The inflammatory response of sepsis attenuates Ca2+ uptake in the sarcoplasmic reticulum by upregulation of RyR and downregulation of SERCA. This abnormal Ca2+ flux increases Ca2+ concentration in mitochondria, followed by abnormal mitochondrial membrane potential and promoting mPTP opening. Theses leads to excess ROS generation, mitochondrial DNA damage, mitochondrial mitophagy, incomplete autophagy, and cell apoptotic pathway. Red arrows indicate increased expression or activity. Blue arrows indicate decreased expression or activity. A cross mark indicates no function. Abbreviations are described at the end of this manuscript.
Figure 1.
A schematic figure of mechanisms of mitochondrial dysfunction in SICM. The inflammatory response of sepsis attenuates Ca2+ uptake in the sarcoplasmic reticulum by upregulation of RyR and downregulation of SERCA. This abnormal Ca2+ flux increases Ca2+ concentration in mitochondria, followed by abnormal mitochondrial membrane potential and promoting mPTP opening. Theses leads to excess ROS generation, mitochondrial DNA damage, mitochondrial mitophagy, incomplete autophagy, and cell apoptotic pathway. Red arrows indicate increased expression or activity. Blue arrows indicate decreased expression or activity. A cross mark indicates no function. Abbreviations are described at the end of this manuscript.

Figure 2.
A schematic figure of metabolic dysregulation in SICM. ATP synthesis in the heart is mainly dependent on fatty acid oxidation (FAO). The inflammatory response in sepsis is induced by many inflammatory mediators such as NFκB, iNOS, cytokines, and ROS, which dysregulate various genes related to FAO. Inflammation reduces CD36, FABP, and ACLS, which are cell surface transporters for fatty acids (FAs) into cells, and also reduces CPT1, which is an important enzyme for intracellular FAs to enter mitochondria. In addition, inflammatory mediators also decrease PPARs and PGC1α essential for β-oxidation. As a result, compromised ATP production induces intracellular lipid accumulation, called lipotoxicity, leading to cell death. Red arrows indicate increased expression or production. Blue arrows indicate decreased expression or production. Cross marks indicate no function. Abbreviations are described at the end of this manuscript.
Figure 2.
A schematic figure of metabolic dysregulation in SICM. ATP synthesis in the heart is mainly dependent on fatty acid oxidation (FAO). The inflammatory response in sepsis is induced by many inflammatory mediators such as NFκB, iNOS, cytokines, and ROS, which dysregulate various genes related to FAO. Inflammation reduces CD36, FABP, and ACLS, which are cell surface transporters for fatty acids (FAs) into cells, and also reduces CPT1, which is an important enzyme for intracellular FAs to enter mitochondria. In addition, inflammatory mediators also decrease PPARs and PGC1α essential for β-oxidation. As a result, compromised ATP production induces intracellular lipid accumulation, called lipotoxicity, leading to cell death. Red arrows indicate increased expression or production. Blue arrows indicate decreased expression or production. Cross marks indicate no function. Abbreviations are described at the end of this manuscript.

Figure 3.
Histological analysis of septic myocardium. Oil Red O staining demonstrates the accumulation of lipid droplets (LDs) in heart tissues of LPS injected mice. β3AR antagonist significantly reduces LDs in heart tissues post LPS injection. Electron microscope analyses also exhibits a lot of LDs around mitochondria in LPS treated heart tissues. β3AR antagonist clearly attenuates accumulation of LDs. Red arrows show lipid droplets. LPS, lipopolysaccharide; β3AR, beta 3 adrenergic receptor.
Figure 3.
Histological analysis of septic myocardium. Oil Red O staining demonstrates the accumulation of lipid droplets (LDs) in heart tissues of LPS injected mice. β3AR antagonist significantly reduces LDs in heart tissues post LPS injection. Electron microscope analyses also exhibits a lot of LDs around mitochondria in LPS treated heart tissues. β3AR antagonist clearly attenuates accumulation of LDs. Red arrows show lipid droplets. LPS, lipopolysaccharide; β3AR, beta 3 adrenergic receptor.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Noncoding RNA regulation for mitochondria in SICM.
| NcRNA | Expression in Sepsis | Experimental Models | Mechanisms of Actions | Roles | Reference |
|---|---|---|---|---|---|
| LncRNA RMPP | ↓ | LPS treated C57BL/6 mice and cardiac muscle cells (HL-1) | Regulation of miR-1-5p/HSP 70 axis | reduction of MMP and ROS | [95] |
| LncRNA H19 | ↓ | H9C2 cell line | Regulation of miR-93-5p/SORBS2 axis | Attenuation of MMP and inflammation | [96] |
| LncRNA MIAT | ↑ | LPS treated male BALB/c mice and HL-1 cells | Regulation of miR-330-5p/TRAF6/NF-κB axis | Promotion of inflammation and mitochondrial ROS | [94] |
| MiR-210-3p | ↑ | CLP treated male Sprague Dawley rats and H9C2 cells | Regulation of NDUFA4 | Promotion of cardiomyocyte apoptosis and mitochondrial dysfunction | [104] |
| MiR-21-3p | ↑ | LPS treated C57BL/6/mice and human plasma | Regulation of SORBS2 | Attenuation of myocardial mitochondrial ultrastructure damage and autophagy | [105] |
| LncRNA SOX2OT | ↑ | LPS treated mice and LPS treated H9C2 | Regulation of SOX2 | Promotion of mitochondrial dysfunction with reduction of MMP and increase in ROS | [106] |
| LncRNA MALAT1 | ↑ | LPS treated H9C2 and CLP treated rats | Regulation of EZH2/USP22 axis | Attenuation of cardiac injury and Nrf2 expression | [107] |
Upward arrows indicate increased expression and downward arrows indicate decreased expression.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kuroshima, T.; Kawaguchi, S.; Okada, M. Current Perspectives of Mitochondria in Sepsis-Induced Cardiomyopathy. Int. J. Mol. Sci. 2024, 25, 4710. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms25094710
AMA Style
Kuroshima T, Kawaguchi S, Okada M. Current Perspectives of Mitochondria in Sepsis-Induced Cardiomyopathy. International Journal of Molecular Sciences. 2024; 25(9):4710. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms25094710
Chicago/Turabian StyleKuroshima, Tatsuki, Satoshi Kawaguchi, and Motoi Okada. 2024. "Current Perspectives of Mitochondria in Sepsis-Induced Cardiomyopathy" International Journal of Molecular Sciences 25, no. 9: 4710. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms25094710
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.