
The Impact of Internet Addiction on Mental Health: Exploring the Mediating Effects of Positive Psychological Capital in University Students
 ,
,
Abstract
:
1. Introduction
1.1. Benefits of Psychological Capital
1.2. Conceptual Framework
Internet Addiction, Psychological Capital, and Mental Health
1.3. Gaps in the Literature
1.4. Research Questions and Hypotheses
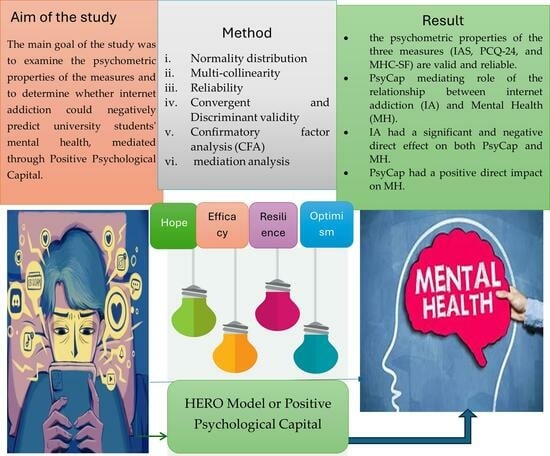
- To what extent do the Amharic versions of the Internet Addiction Scale (IAS), the Psychological Capital Questionnaire (PCQ-24), and the Mental Health Continuum-Short Form (MHC-SF) exhibit high levels of reliability and validity?
- Is there a negative relationship between Internet Addiction (IA) and Psychological Capital (PsyCap) and Mental health (MH) among undergraduate young students?
- Does PsyCap positively predict MH among undergraduate young university students?
- Does PsyCap mediate the relationship between IA and MH among undergraduate young university students?
2. Methods
2.1. Research Design
2.2. Sample and Sampling
2.3. Instruments
2.3.1. Socio-Demographic Information
2.3.2. Internet Addiction Scale (IAS)
2.3.3. Psychological Capital Questionnaire (PCQ-24)
2.3.4. Mental Health Continuum-Short Form [MHC-SF]
2.4. Statistical Data Analysis
- i.
- Normality distribution: The absence of multicollinearity was confirmed by examining the correlation matrices among the constructs, which should be less than 0.90, and by verifying the assumption of normality. Outliers of the constructs were also examined following the procedures of [46,47,48,49,50]. Values of ≤2 or ≤4 for skewness or kurtosis, respectively, indicate the normal data distribution [51,52].
- ii.
- iii.
- Reliability assessment: The researchers evaluated the internal consistency of the subscales using two measures: CR (Composite Reliability) and Cronbach’s alpha coefficient. Excellent internal consistency was indicated by values above 0.90, while values between 0.80 and 0.90 were considered good, and values between 0.70 and 0.80 were deemed acceptable [48,49].
- iv.
- Convergent and Discriminant Validity: Convergent and discriminant validity were evaluated to confirm the construct validity of the measurement instruments. Convergent validity was assessed using the Average Variance Extracted (AVE), where values exceeding 0.5 indicate satisfactory convergent validity. Discriminant validity was examined by comparing the Maximum Shared Variance (MSV) with the AVE values of the variables. Adequate discriminant validity was established when the MSV value was lower than the AVE value, and the squared correlation between sub-constructs was lower than the AVE value, indicating acceptable discriminant validity [46].
- v.
- Confirmatory factor analysis (CFA) and mediation analysis: Confirmatory factor analysis (CFA) and mediation analysis were conducted to examine the factorial validity of the measurement and structural models [46,47,48,49,50]. Maximum likelihood estimation was utilized to identify the measurement and structural relationships within the proposed model. The goodness-of-fit of the models was assessed using several indices, including the normed chi-square (χ2/df), Tucker Lewis Index (TLI), Comparative Fit Index (CFI), Standardized Root Mean Residual (SRMR), and Root Mean Squared Error of Approximation (RMSEA). An excellent and satisfactory fit of the models is typically indicated by χ2/df values below 3 or 5, RMSEA and SRMR values below 0.08 and 0.01, and TLI and CFI values above 0.95 and 0.90, respectively [53]. These indices provide information about how well the proposed models align with the observed data, with lower χ2/df, RMSEA, and SRMR values and higher TLI and CFI values indicating a better fit [53]. To examine indirect effects, the researchers calculated 95% bias-corrected and accelerated confidence intervals using the bootstrap method with 5000 resamples. Through various sophisticated approaches, the researchers successfully addressed the challenges associated with psychometric assessment and mediation analysis, providing valuable insights into the variables and relationships examined in this study.
2.5. Procedures of the Studies
2.5.1. Adaption, Translation, and Validation of the Measures
2.5.2. Ethics of this Study
3. Results
3.1. Results of Preliminary Analysis
3.1.1. Descriptive Statistics, Skewness, and Kurtosis
3.1.2. Multi-Collinearity
3.1.3. Reliability and Validity Evidence of the Main Variables
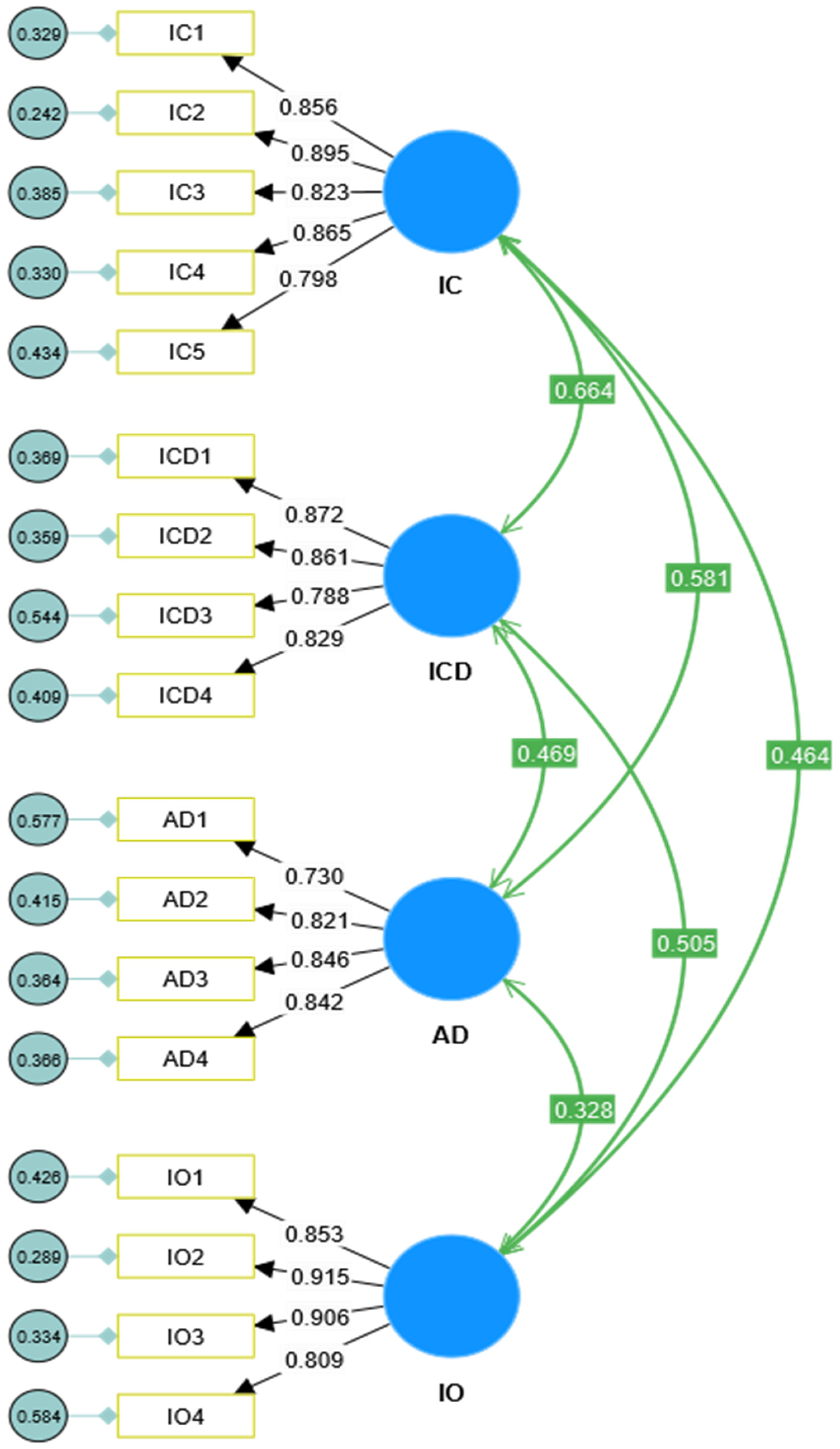
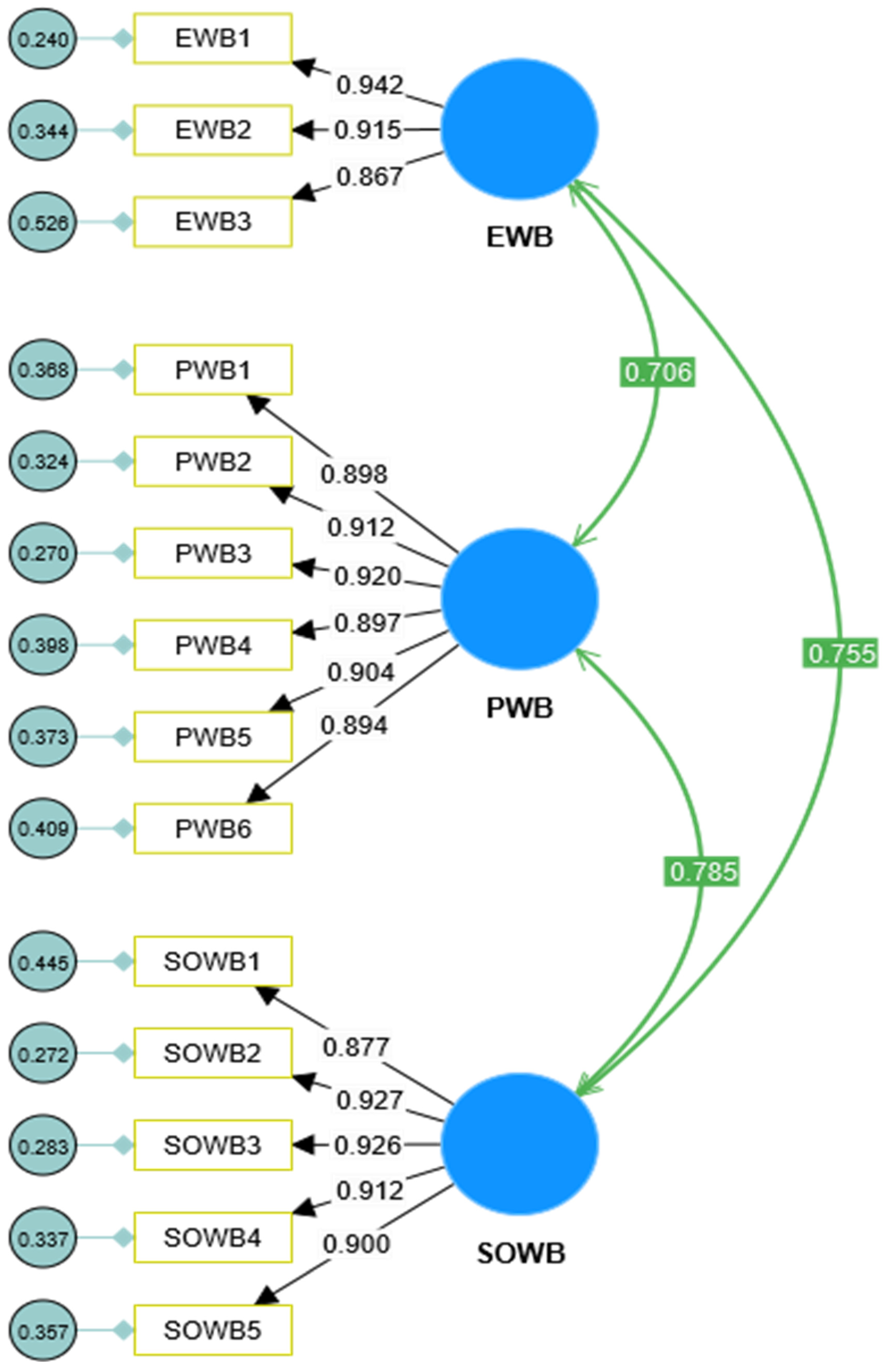
3.1.4. Measurement and Structural Model

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Models | Variables of this Study | Fitness of Indices Using Confirmatory Factorial Analysis of the Variables | ||||
|---|---|---|---|---|---|---|
| χ2 | TLI | CFI | SRMR | RMSEA | ||
| Model 1 | Internet Addiction (see Figure 2) | 364.80 (113) ** | 0.973 | 0.977 | 0.031 | 0.051 |
| Model 2 | PsyCap (see Figure 3) | 2005.74 (246) ** | 0.915 | 0.924 | 0.046 | 0.092 |
| Model 3 | Mental Health (see Figure 4) | 234.75 (74) ** | 0.986 | 0.989 | 0.016 | 0.051 |
| Model 4 | Measurement Model | 4384 (1375) ** | 0.935 | 0.940 | 0.037 | 0.051 |
| Structural Model | 4660 (1416) ** | 0.932 | 0.935 | 0.046 | 0.052 | |
| Rule of Thumb | >0.90 | >0.90 | >0.08 | >1.00 | ||




3.1.5. Mediation Testing Using Structural Equation Modeling (SEM)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leung, H.; Pakpour, A.H.; Strong, C.; Lin, Y.C.; Tsai, M.C.; Griffiths, M.D.; Lin, C.Y.; Chen, I.H. Measurement invariance across young adults from Hong Kong and Taiwan among three internet-related addiction scales: Bergen Social Media Addiction Scale (BSMAS), Smartphone Application-Based Addiction Scale (SABAS), and Internet Gaming Disorder Scale-Short Form (IGDS-SF9) (Study Part A). Addict. Behav. 2020, 101, 105969. [Google Scholar] [CrossRef] [PubMed]
- Kuss, D.J.; Van Rooij, A.J.; Shorter, G.W.; Griffiths, M.D.; Van De Mheen, D. Internet addiction in adolescents: Prevalence and risk factors. Comput. Hum. Behav. 2013, 29, 1987–1996. [Google Scholar] [CrossRef]
- Shao, X.; Ni, X. How Does Family Intimacy Predict Self-Esteem in Adolescents? Moderation of Social Media Use Based on Gender Difference. SAGE Open 2021, 11. [Google Scholar] [CrossRef]
- Kayiş, A.R.; Satici, S.A.; Yilmaz, M.F.; Şimşek, D.; Ceyhan, E.; Bakioğlu, F. Big five-personality trait and internet addiction: A meta-analytic review. Comput. Hum. Behav. 2016, 63, 35–40. [Google Scholar] [CrossRef]
- Wu, Y.; Xue, Y.; Zhao, X.; Han, S.; Wu, W. Unravelling the veil of appearance anxiety: Exploring social media use among Chinese young people. BMC Psychol. 2024, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.C.; Tung, C. Comparison of Internet addicts and non-addicts in Taiwanese high school. Comput. Hum. Behav. 2007, 23, 79–96. [Google Scholar] [CrossRef]
- Koc, M.; Gulyagci, S. Facebook addiction among Turkish college students: The role of psychological health, demographic, and usage characteristics. Cyberpsychol. Behav. Soc. Netw. 2013, 16, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Luthans, F.; Avolio, B.J.; Avey, J.B.; Norman, S.M. Positive psychological capital: Measurement and relationship with performance and satisfaction. Pers. Psychol. 2007, 60, 541–572. [Google Scholar] [CrossRef]
- Bi, X.; Jin, J. Psychological Capital, College Adaptation, and Internet Addiction: An Analysis Based on Moderated Mediation Model. Front. Psychol. 2021, 12, 712964. [Google Scholar] [CrossRef]
- Zewude, G.T.; Hercz, M. The Teacher Well-Being Scale (TWBS): Construct validity, model comparisons and measurement invariance in an Ethiopian setting. J. Psychol. Afr. 2022, 32, 251–262. [Google Scholar] [CrossRef]
- Alonzo, R.; Hussain, J.; Stranges, S.; Anderson, K.K. Interplay between social media use, sleep quality, and mental health in youth: A systematic review. Sleep Med. Rev. 2021, 56, 101414. [Google Scholar] [CrossRef] [PubMed]
- Canan, F.; Ataoglu, A.; Nichols, L.A.; Yildirim, T.; Ozturk, O. Evaluation of Psychometric Properties of the Internet Addiction Scale in a Sample of Turkish. Cyberpsychol. Behav. Soc. Netw. 2010, 13, 4–7. [Google Scholar] [CrossRef] [PubMed]
- Prasetya, T.A.E.; Wardani, R.W.K. Systematic review of social media addiction among health workers during the pandemic COVID-19. Heliyon 2023, 9, e16784. [Google Scholar] [CrossRef]
- Arslan, G.; Coşkun, M. Social Exclusion, Self-Forgiveness, Mindfulness, and Internet Addiction in College Students: A Moderated Mediation Approach. Int. J. Ment. Health Addict. 2022, 20, 2165–2179. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Wang, Z.; David, P. Social media multitasking (SMM) and well-being: Existing evidence and future directions. Curr. Opin. Psychol. 2022, 47, 101345. [Google Scholar] [CrossRef] [PubMed]
- Woods, H.C.; Scott, H. #Sleepyteens: Social media use in adolescence is associated with poor sleep quality, anxiety, depression and low self-esteem. J. Adolesc. 2016, 51, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Xue, B.; Wang, S.; Chen, D.; Hu, Z.; Feng, Y.; Luo, H. Moral distress, psychological capital, and burnout in registered nurses. Nurs. Ethics 2023, 9697330231202233. [Google Scholar] [CrossRef]
- Boer, M.; Stevens, G.W.J.M.; Finkenauer, C.; de Looze, M.E.; van den Eijnden, R.J.J.M. Social media use intensity, social media use problems, and mental health among adolescents: Investigating directionality and mediating processes. Comput. Hum. Behav. 2021, 116, 106645. [Google Scholar] [CrossRef]
- Ziapour, A.; Lebni, J.Y.; Toghroli, R.; Abbas, J.; NeJhaddadgar, N.; Salahshoor, M.R.; Mansourian, M.; Gilan, H.D.; Kianipour, N.; Chaboksavar, F.; et al. A study of internet addiction and its effects on mental health: A study based on Iranian University Students. J. Educ. Health Promot. 2020, 9, 205. [Google Scholar] [CrossRef]
- Hannah, S.T.; Avolio, B.J. Moral potency: Building the capacity for character-based leadership. Consult. Psychol. J. 2010, 62, 291–310. [Google Scholar] [CrossRef]
- Jiang, Q.; Chen, Z.; Zhang, Z.; Zuo, C. Investigating links between Internet literacy, Internet use, and Internet addiction among Chinese youth and adolescents in the digital age. Front. Psychiatry 2023, 14, 1233303. [Google Scholar] [CrossRef]
- Sondhi, N.; Joshi, H. Multidimensional Assessment of Internet Addiction: Scale Development and Validation. Glob. Bus. Rev. 2024, 25, 85–98. [Google Scholar] [CrossRef]
- Alshakhsi, S.; Chemnad, K.; Almourad, M.B.; Altuwairiqi, M.; McAlaney, J.; Ali, R. Problematic internet usage: The impact of objectively Recorded and categorized usage time, emotional intelligence components and subjective happiness about usage. Heliyon 2022, 8, e11055. [Google Scholar] [CrossRef]
- Bohlmeijer, E.; Westerhof, G. The Model for Sustainable Mental Health: Future Directions for Integrating Positive Psychology Into Mental Health Care. Front. Psychol. 2021, 12, 747999. [Google Scholar] [CrossRef] [PubMed]
- Keyes, C.L.M. The Mental Health Continuum: From Languishing to Flourishing in Life. J. Health Soc. Behav. 2002, 43, 207–222. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Wang, J.; Zhang, X.; Pei, Y.; Tang, J.; Zhu, Y.; Liu, X.; Xu, H. Network connectivity between anxiety, depressive symptoms and psychological capital in Chinese university students during the COVID-19 campus closure. J. Affect. Disord. 2023, 329, 11–18. [Google Scholar] [CrossRef]
- Zewude, G.T.; Hercz, M. Does Work Task Motivation Mediate the Relationship Between Psychological Capital and Teacher Well-being? Psihologija 2024, 57, 129–153. [Google Scholar] [CrossRef]
- Zheng, Q.; Liu, S.; Zheng, J.; Gu, M.; He, W. College students’ loneliness and problematic mobile phone use: Mediation by fear of missing out. J. Psychol. Afr. 2023, 33, 115–121. [Google Scholar] [CrossRef]
- Preston, A.; Rew, L.; Young, C.C. A Systematic Scoping Review of Psychological Capital Related to Mental Health in Youth. J. Sch. Nurs. 2023, 39, 72–86. [Google Scholar] [CrossRef]
- Davis, R.A. A cognitive-behavioral model of pathological Internet use. Comput. Hum. Behav. 2001, 17, 187–195. [Google Scholar] [CrossRef]
- Fredrickson, B.L. The broaden-and-build theory of positive emotions. Philos Trans R Soc Lond B Biol Sci. 2004, 359, 1367–1377. [Google Scholar] [CrossRef] [PubMed]
- Flaherty, J.A. Developing instruments for cross cultural research. J. Nerv. Ment. Dis. 1988, 176, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Essel, H.B.; Vlachopoulos, D.; Nyadu-Addo, R.; Tachie-Menson, A.; Baah, P.K.; Owusu-Antwi, C. The Impact of Mental Health Predictors of Internet Addiction among Pre-Service Teachers in Ghana. Behav. Sci. 2023, 13, 20. [Google Scholar] [CrossRef] [PubMed]
- Kuss, D.J.; Kristensen, A.M.; Lopez-Fernandez, O. Internet addictions outside of Europe: A systematic literature review. Comput. Hum. Behav. 2021, 115, 106621. [Google Scholar] [CrossRef]
- Seligman, M.E.P. Flourish: A Visionary New Understanding of Happiness and Well-Being; Free Press: New York, NY, USA, 2011. [Google Scholar]
- Dutt, B. Social media wellbeing: Perceived wellbeing amidst social media use in Norway. Soc. Sci. Humanit. Open 2023, 7, 100436. [Google Scholar] [CrossRef]
- Luthans, F.; Youssef, C.M.; Avolio, B.J. Psychological Capital: Developing the Human Competitive Edge; Oxford University Press: New York, NY, USA, 2015. [Google Scholar]
- Echeverría, G.; Torres, M.; Pedrals, N.; Padilla, O.; Rigotti, A.; Bitran, M. Validation of a Spanish Version of the Mental Health Continuum-Short Form Questionnaire. Psicothema 2017, 29, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Strang, K.D. The Palgrave Handbook of Research Design in Business and Management; Springer Science and Business Media LLC.: Dordrecht, The Netherlands, 2015. [Google Scholar] [CrossRef]
- Dirzyte, A.; Perminas, A.; Biliuniene, E. Psychometric properties of satisfaction with life scale (Swls) and psychological capital questionnaire (pcq-24) in the lithuanian population. Int. J. Environ. Res. Public Health 2021, 18, 2608. [Google Scholar] [CrossRef] [PubMed]
- Görgens-Ekermans, G.; Herbert, M. Psychological capital: Internal and external validity of the Psychological Capital Questionnaire (PCQ-24) on a South African sample. SA J. Ind. Psychol. 2013, 39, 1–12. [Google Scholar] [CrossRef]
- Choisay, F.; Fouquereau, E.; Coillot, H.; Chevalier, S. Validation of the French Psychological Capital Questionnaire (F-PCQ-24) and its measurement invariance using bifactor exploratory structural equation modeling framework. Mil. Psychol. 2021, 33, 50–65. [Google Scholar] [CrossRef]
- Cid, D.T.; do Carmo Fernandes Martins, M.; Dias, M.; Fidelis, A.C.F. Psychological capital questionnaire (PCQ-24): Preliminary evidence of psychometric validity of the Brazilian version. Psico-USF 2020, 25, 63–74. [Google Scholar] [CrossRef]
- Hedrih, V. Adapting Psychological Tests and Measurement Instruments for Cross-Cultural Research; Routledge: London, UK, 2020. [Google Scholar]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [PubMed]
- Davidov, E.; Schmidt, P.; Billiet, J.; Meuleman, B. Cross-Cultural Analysis:Methods and Application, 2nd ed.; Taylor & Francis Group, LLC.: Abingdon, UK, 2018. [Google Scholar]
- Hair, J.; Black, W.; Babin, B.; Anderson, R. Multivariate Data Analysis, 8th ed.; Ainscow, A., Ed.; Cengage India: New Delhi, India, 2019. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; The Guilford Press: New York, NY, USA; London, UK, 2016; Volume 4. [Google Scholar]
- Zewude, G.T.; Mária, H.; Taye, B.; Demissew, S. COVID-19 Stress and Teachers Well-Being: The Mediating Role of Sense of Coherence and Resilience. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 1–22. [Google Scholar] [CrossRef] [PubMed]
- George, D.; Mallery, P. IBM SPSS Statistics 26 Step by Step: A Simple Guide and Reference; Routledge: London, UK, 2020; Volume 16. [Google Scholar]
- Zewude, G.T.; Hercz, M. Psychometric Properties and Measurement Invariance of the PERMA Profiler in an Ethiopian Higher Education Setting. Pedagogika 2022, 146, 209–236. [Google Scholar] [CrossRef]
- Kim, H.-Y. Statistical notes for clinical researchers: Assessing normal distribution (2) using skewness and kurtosis. Restor. Dent. Endod. 2013, 38, 52–54. [Google Scholar] [CrossRef] [PubMed]
- Mishra, P.; Pandey, C.M.; Singh, U.; Gupta, A.; Sahu, C.; Keshri, A. Descriptive statistics and normality tests for statistical data. Ann. Card. Anaesth. 2019, 22, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Zhang, C.; Li, G.; Fan, Z.; Tang, X.; Zhang, F. Psychological Capital Mediates the Relationship Between Problematic Smartphone Use and Learning Burnout in Chinese Medical Undergraduates and Postgraduates: A Cross-Sectional Study. Front. Psychol. 2021, 12, 600352. [Google Scholar] [CrossRef]
- Young, K.S. Internet addiction: The emergence of a new clinical disorder. Cyberpsychol. Behav. 1998, 1, 237–244. [Google Scholar] [CrossRef]
- Zewude, G.T.; Hercz, M. Psychological Capital and Teacher Well-being: The Mediation Role of Coping with Stress. Eur. J. Educ. Res. 2021, 10, 1227–1245. [Google Scholar] [CrossRef]
- Turliuc, M.N.; Candel, O.S. The relationship between psychological capital and mental health during the COVID-19 pandemic: A longitudinal mediation model. J. Health Psychol. 2022, 27, 1913–1925. [Google Scholar] [CrossRef] [PubMed]

| Variables | Min | Max | Mean | Std. Dev | Skewness | Kurtosis |
|---|---|---|---|---|---|---|
| Internet craving | 5.000 | 25.000 | 20.032 | 4.87852 | −1.128 | 0.772 |
| Internet compulsive disorder | 4.000 | 20.000 | 14.719 | 4.201 | −0.745 | −0.202 |
| Addictive behavior | 4.000 | 20.000 | 15.528 | 3.870 | −0.962 | 0.368 |
| Internet obsession | 4.000 | 20.000 | 14.358 | 4.749 | −0.618 | −0.719 |
| Internet addiction | 17.000 | 85.000 | 64.636 | 13.720 | −1.080 | 1.580 |
| Hope | 6.000 | 36.000 | 23.696 | 7.663 | −0.831 | −0.040 |
| Efficacy | 6.000 | 36.000 | 21.701 | 8.300 | −0.282 | −0.770 |
| Resilience | 6.000 | 36.000 | 22.202 | 7.608 | −0.343 | −0.593 |
| Optimism | 6.000 | 36.000 | 21.423 | 7.749 | −0.385 | −0.720 |
| PsyCap | 24.000 | 144.000 | 89.023 | 25.91 | −0.489 | 0.288 |
| Emotional well-being | 3.00 | 21.00 | 11.615 | 4.105 | −0.786 | −0.494 |
| Psychological well-being | 6.00 | 42.00 | 25.115 | 7.719 | −1.080 | 0.249 |
| Social well-being | 5.00 | 35.00 | 21.139 | 6.472 | −0.489 | 0.241 |
| Mental health | 14.00 | 98.00 | 57.869 | 16.574 | −0.815 | 0.944 |
| Model | Unstandardized Coefficients | Standardized Coefficients | t | Sig. | Collinearity Statistics | |
|---|---|---|---|---|---|---|
| Beta | Beta | Tolerance | VIF | |||
| Internet addiction | −0.265 | −0.219 | −7.697 | 0.000 | 0.920 | 1.086 |
| PsyCap | 0.324 | 0.507 | 17.819 | 0.000 | 0.920 | 1.086 |
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| - | ||||||||||||||||
| −0.006 | - | |||||||||||||||
| 0.096 ** | 00.020 | - | ||||||||||||||
| −0.068 * | −0.013 | −0.006 | - | |||||||||||||
| −0.008 | −0.001 | −0.011 | 0.613 ** | - | ||||||||||||
| −0.047 | 0.021 | −0.012 | 0.540 ** | 0.436 ** | - | |||||||||||
| −0.053 | 0.016 | 0.014 | 0.433 ** | 0.459 ** | 0.305 ** | - | ||||||||||
| −0.111 ** | −0.007 | −0.045 | −0.216 ** | −0.165 ** | −0.083 * | −0.162 ** | - | |||||||||
| −0.018 | 0.024 | −0.026 | −0.271 ** | −0.133 ** | −0.222 ** | −0.135 ** | 0.750 ** | - | ||||||||
| −0.137 ** | 0.006 | 0.011 | −0.269 ** | −0.253 ** | −0.143 ** | −0.248 ** | o.598 ** | o.570 ** | - | |||||||
| −0.033 | −0.014 | 0.058 | −0.226 ** | −0.163 ** | −0.225 ** | 0.028 | 0.515 ** | 0.564 ** | 0.506 ** | - | ||||||
| 0.044 | −0.011 | 0.034 | −0.258 ** | −0.242 ** | −0.190 ** | −0.282 ** | 0.458 ** | 0.457 ** | 0.429 ** | 0.272 ** | - | |||||
| 0.054 | −0.028 | 0.041 | −0.274 ** | −0.262 ** | −0.179 ** | −0.298 ** | 0.479 ** | 0.456 ** | 0.453 ** | 0.293 ** | 0.673 ** | - | ||||
| 0.001 | 0.018 | 0.057 | −0.286 ** | −0.237 ** | −0.208 ** | −0.285 ** | 0.536 ** | 0.499 ** | 0.476 ** | 0.294 ** | 0.715 ** | 0.758 ** | - | |||
| −0.058 | 0.007 | −0.004 | 0.845 ** | 0.806 ** | 0.713 ** | 0.727 ** | −0.207 ** | −0.247 ** | −0.299 ** | −0.184 ** | −0.317 ** | −0.331 ** | −0.332 ** | - | ||
| −0.069 | 0.003 | −0.001 | −0.296 ** | −0.214 ** | −0.204 ** | −0.155 ** | 0.863 ** | 0.874 ** | 0.802 ** | 0.778 ** | 0.487 ** | 0.507 ** | 0.544 ** | −0.282 ** | - | |
| 0.036 | −0.016 | 0.050 | −0.303 ** | −0.275 ** | −0.212 ** | −0.320 ** | 0.546 ** | 0.520 ** | 0.503 ** | 0.319 ** | 0.840 ** | 0.928 ** | 0.920 ** | −0.362 ** | 0.569 ** | - |
| Internet Addicton Scale (IAS) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Models | α | CR | AVE (>0.50 *) | MSV | Squared correlation | |||
| (>0.70 *) | 1 | 2 | 3 | 4 | ||||
| 1. Internet Craving | 0.883 | 0.883 | 0.658 | 0.44 | - | |||
| 2. Internet Compulsive Disorder | 0.927 | 0.927 | 0.719 | 0.44 | 0.44 | - | ||
| 3. Addictive Behavior | 0.904 | 0.904 | 0.703 | 0.34 | 0.34 | 0.22 | - | |
| 4. Internet Obsession | 0.926 | 0.926 | 0.760 | 0.26 | 0.22 | 0.26 | 0.11 | - |
| Psychological Capital Questionnaire (PCQ-24) | ||||||||
| Models | α | CR | AVE (>0.50 *) | MSV | Squared correlation | |||
| (>0.70 *) | H | E | R | O | ||||
| Hope (H) | 0.958 | 0.958 | 0.791 | 0.59 | - | |||
| Efficacy (E) | 0.950 | 0.951 | 0.764 | 0.59 | 0.59 ** | - | ||
| Resilience (R) | 0.946 | 0.947 | 0.745 | 0.38 | 0.38 ** | 0.34 ** | - | |
| Optimism (O) | 0.957 | 0.957 | 0.788 | 0.34 | 0.29 ** | 0.34 ** | 0.26 ** | - |
| Mental Health Continuum-Short Form (MHC-SF) | ||||||||
| Models | α | CR | AVE (>0.50 *) | MSV | Squared correlation | |||
| EWB | PWB | SWB | ||||||
| Emotional Well-Being (EWB) | 0.934 | 0.934 | 0.825 | 0.62 | - | |||
| Psychological Well-Being (PWB) | 0.964 | 0.964 | 0.818 | 0.59 | 0.50 ** | - | ||
| Social Well-Being (SWB) | 0.959 | 0.960 | 0.826 | 0.62 | 0.62 ** | 0.57 ** | - | |
| Predictors | Outcome Variables | Bootstrap 95% CI | |||
|---|---|---|---|---|---|
| Beta | LBC | UBC | p-Value | ||
| Standardized Direct Effect | |||||
| Internet addiction | PsyCap | −0.327 | −0.414 | −0.248 | 0.001 |
| Internet addiction | Mental Health | −0.211 | −0.277 | −0.140 | 0.003 |
| PsyCap | Mental Health | 0.595 | 0.533 | 0.658 | 0.001 |
| Standardized Indirect Effect | |||||
| Internet addiction → PsyCap → | Mental Health (Figure 5) | −0.195 | −0.252 | −0.146 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zewude, G.T.; Bereded, D.G.; Abera, E.; Tegegne, G.; Goraw, S.; Segon, T. The Impact of Internet Addiction on Mental Health: Exploring the Mediating Effects of Positive Psychological Capital in University Students. Adolescents 2024, 4, 200-221. https://0-doi-org.brum.beds.ac.uk/10.3390/adolescents4020014
Zewude GT, Bereded DG, Abera E, Tegegne G, Goraw S, Segon T. The Impact of Internet Addiction on Mental Health: Exploring the Mediating Effects of Positive Psychological Capital in University Students. Adolescents. 2024; 4(2):200-221. https://0-doi-org.brum.beds.ac.uk/10.3390/adolescents4020014
Chicago/Turabian StyleZewude, Girum Tareke, Derib Gosim Bereded, Endris Abera, Goche Tegegne, Solomon Goraw, and Tesfaye Segon. 2024. "The Impact of Internet Addiction on Mental Health: Exploring the Mediating Effects of Positive Psychological Capital in University Students" Adolescents 4, no. 2: 200-221. https://0-doi-org.brum.beds.ac.uk/10.3390/adolescents4020014