
Data on Demodex Ectoparasite Infestation in Patients Attending an Outpatient Clinic in Greece

1
Department of Internal Medicine, Spiliopoulio Agia Eleni Hospital, 11521 Athens, Greece
2
Department of Microbiology, Andreas Syggros General Hospital, 16121 Athens, Greece
3
Unit of Medical Entomology, Laboratory for the Surveillance of Infectious Diseases, Department of Public Health Policy, School of Public Health, University of West Attica, 11521 Athens, Greece
*
Author to whom correspondence should be addressed.
Parasitologia 2024, 4(2), 129-136; https://0-doi-org.brum.beds.ac.uk/10.3390/parasitologia4020011
Submission received: 11 March 2024
/
Revised: 10 April 2024
/
Accepted: 12 April 2024
/
Published: 26 April 2024
Abstract
:Demodex mites are acari, common ectoparasites of humans and other mammalian pilosebaceous units. Demodicosis occurs when mites overpopulate the skin, causing several skin disorders. Our aim was to investigate the prevalence of demodicosis in patients with suspicious clinical features, such as cheek redness, itching, and skin sensitivity, who presented at the outpatient clinic of the Andreas Syggros Dermatology Hospital in Greece. We studied 184 individuals aged between 18 and 97 years and analyzed the content of pilosebaceous units by microscopy to determine the density of Demodex mites. Samples were evaluated as positive when Demodex spp. densities equaled or exceeded 5 mites per square cm. Sixty-six percent of the examined subjects were positive for demodicosis. The age distribution was statistically normal (p = 0.2), and the median age was 51.29 years. Seventy percent of the patients were females, and 30% were males, while 64.46% of the demodicosis-positive individuals were females, and 35.54% were males. We observed a rise in the percentage of males as the age of the patients increased. Demodicosis can be a challenging disease because it presents apart from the typical symptoms, with a variety of nonspecific symptoms mimicking other dermatological skin conditions. Therefore, it is important to investigate Demodex spp. in patients who present with common facial dermatological diseases to improve treatment results. Further studies could contribute to a better understanding of the pathogenic role of Demodex mites and how this role is affected by mite density, host sex and age.
1. Introduction
Demodex mites (Acari: Demodicidae) are among the most common ectoparasites of humans. Among Demodex mites, two species have been described as ubiquitous obligatory ectoparasites of humans: Demodex folliculorum (Simon) and Demodex brevis (Akbulatova) [1]. Although both species are found in the pilosebaceous complex of the skin, Demodex folliculorum mainly inhabits the hair follicles of the face, while Demodex brevis resides in the sebaceous and Meibomian glands [1]. D. folliculorum is larger, approximately 0.3–0.4 mm long, while D. brevis is smaller, approximately 0.2–0.3 mm long, with a spindle shape. D. folliculorum is more commonly localized to the face, while D. brevis is mostly found on the neck and chest [2]. Demodex mites are found on 20–100% of healthy humans of all races without sex preference. When mite density remains low, in most cases, the host is asymptomatic [3,4]. Abnormally high mite densities can be detected on skin samples from patients with papulopustular rosacea, pityriasis folliculorum and perioral dermatitis. When the mite density exceeds the limit of 5 mites/cm2, pathogenic overcolonization is considered to indicate “demodicosis” [5,6,7,8,9]. Recent studies suggest that Demodex mites represent a transitional stage from a host-injuring obligate parasite to an obligate symbiont that has an impact on the genome and physiology of the mite [10].
The term “human demodicosis” refers to skin conditions caused by D. folliculorum and/or D. brevis infestation in humans [11]. In symptomatic cases, Demodex mites can result in skin sensitivity and dryness, cheek redness, rash, exfoliation and erythema [12].
D. folliculorum and D. brevis have been identified and shown to play a role in pathogenic facial conditions [13]. There is no general consensus regarding the degree to which mites cause skin pathology and how they might contribute to the development of demodicosis. Nevertheless, it is very likely that the host immune response has a major impact on determining the degree of mite colonization, affecting the outcome of pathology [14].
As high numbers of Demodex mites have been observed on the skin and eyelashes of patients with infection, several pathogenic mechanisms have been proposed to support the idea that mites alone are able to cause significant damage to their habitat without excluding the pathogenic role of microbial agents potentially associated with Demodex infestation [13,15].
Several recent studies have reported a significant association of Demodex infestation with rosacea, acne vulgaris, seborrheic dermatitis, pityriasis folliculorum, eczema, perioral dermatitis and others [16,17], highlighting the importance of its consideration in patients presenting in the clinic for a prompt diagnosis essential to initiate appropriate antiparasitic treatment when the parasite is detected [18,19].
In the present study, we aimed to examine demodicosis infestation in patients who presented to an outpatient dermatology clinic with cheek redness, itching, skin sensitivity and who were referred for diagnosis; whether there was a difference in demodicosis between males and females; and whether there was an effect of age group on the proportion of patients with demodicosis who presented with the above symptoms.
2. Results
The 184 patients comprised 55 males (29.89%) and 129 females (70.11%). The overall median age was 51.29 years (range 18–97 years) (Figure 1).
Microscopic D. folliculorum infection was detected in 121 subjects (65.76%), while the remaining 63 (34.24%) were negative for demodicosis. In Figure 2a,b, microscopy images of Demodex mites from representative patient samples are presented.
Forty-three (35.54%) of the positive-for-demodicosis samples were male, and 78 (64.46%) were female. The prevalence of demodicosis in male patients was greater than that in female patients (78.18% versus 60.47%).
To more effectively analyze the impact of host age on demodicosis incidence, the sample was divided into age groups as follows: 18–40 years (54 cases, 29.35% of the total sample), 41–60 years (77 cases, 41.8%), 61–80 years (45 cases, 24.45%), and 81–97 years (eight cases, 4.35%).
In the first group (18–40 years), 81.48% were females (44 examinees), and 18.52% were males (10 examinees). Thirty-one (57.41%) subjects were positive; seven (22.58%) were males, and 24 (77.42%) were females. This means that 70% of males and 54.5% of females in this age group were positive for demodicosis.
In the second group (aged 41–60 years), which included 77 patients, 70% (54 individuals) were females, and 30% (23 individuals) were males. Forty-nine examinees (63.63%) in this age group were positive; this percentage was significantly greater than that of the first age group. Fifteen of the positive subjects in this group were males (65.21% of all males in this group), and 34 were females (62.3% of all females aged between 41 and 60 years). A total of 30.6% of the positive subjects in this age group were males, and the remaining 69.4% were females.
In the third age group comprising 45 patients (61–80 years), the percentage of males increased (19 males versus 26 females, 42.22%). The overall prevalence in this age group increased (35 positive cases out of 45, 77.77%). For the first time, there was a gender equilibrium in positive samples in this age group (17 positive males vs. 18 positive females); this means that 89.47% of males and 69.23% of females were positive, so we observed an increase in the prevalence of demodicosis in males in comparison with the previous age group.
In the oldest age group (81–97 years), males outnumbered females (five males out of eight patients, 62.5%). The prevalence of demodicosis was 75% (similar to the previous age group). Four out of the six (66.67%) positive subjects were males, and two (33.33%) were females; thus, the male prevalence was 80%, and the female prevalence was 66.67%.
3. Materials and Methods
A total of 184 individuals who presented at the outpatient dermatological clinic of the Andreas Syggros General Hospital in Athens, Greece, over a 2-year period between 2017 and 2018 with cheek redness, itching, and skin sensitivity were included in the study. All 184 patients with suspicious clinical symptoms of demodicosis were directly referred from the dermatologists to the outpatient microbiology clinic for sample collection. The age of the individuals varied from 18 to 97 years. The Institutional Scientific Board of the A. Syggros Hospital granted approval for the study (Approval no. and date: 2429/9 January 2017). No identifying details of patient records are included in this manuscript.
The samples were collected from the patients after compression of the suspicious cheek skin with the fingers and subsequent extraction of the content of the pilosebaceous follicles. Direct microscopic examination (DME) of the samples was subsequently performed [20,21].
Samples were smeared on glass slides, processed with 10% potassium hydroxide solution and then examined under an Olympus light microscope at 10× magnification (Olympus, Tokyo, Japan). Identification was performed using standard methods [1]. The density of visible Demodex mites that appeared as spindle-shaped, transparent forms with stripes across the abdominal area was assessed in each case by calculating the number of mites per visual field. The samples were categorized as positive when the mite density was greater than 5 mites/cm2 [17,18,22].
4. Discussion
In the present study, 65.76% of the examined individuals who presented with symptoms compatible with demodicosis were found to be positive for Demodex mites. Here, the overall prevalence of males who were found to be positive exceeded that of females (78.2% versus 60.5%), while the relative frequencies were 35.54% and 64.46%, respectively, most likely because females, mainly for aesthetic reasons, tend to seek medical assistance, including prompt diagnosis and appropriate treatment earlier, thus presenting with less severe clinical features than males, who are more likely to have already developed demodicosis when they decide to undergo medical examination.
In previous studies in Greek patients, the first involving 74 subjects, similar findings were reported, as eyelash examinations revealed that 78.38% of examinees were positive—78.57% of male subjects and 78.26% of female subjects [23]. In the second study focusing on rosacea patients, D. folliculorum was detected in 90.2% of the subjects examined [24]. In another study on rosacea in northern Greece, the prevalence and mean density of D. folliculorum were significantly increased in rosacea patients, as mites were found on 84% of patients [25].
In the study of Wesolowska et al. [5] in Poland, the group of patients studied consisted of individuals with a high suspicion of demodicosis with respect to their clinical features. Demodex mites were detected on 37.9% of the males and 42.1% of the females.
In our study, the overall Demodex prevalence appeared to increase with increasing age. This finding is consistent with previous literature data, suggesting an increase in the incidence of demodicosis in older individuals, most likely related to alterations in the follicles produced by the mites, skin changes associated with aging, or a combination thereof. Skin changes related to age may favor Demodex mite infestation [26].
In the present study, we observed a clear increasing trend in the relative frequency of demodicosis-positive males in the overall positive samples as age progressed, while the relative frequency of females declined with increasing age [26]. Other studies have shown that older males, in general, were more heavily infested with Demodex mites than females or younger males, probably due to elevated androgenic stimulation of sebaceous glands or due to the increased level of environmental damage to their skin, which promoted mite colonization and survival [26].
Several recent studies have correlated Demodex infestation with several dermatological diseases, such as acne vulgaris, rosacea, seborrheic dermatitis, pityriasis folliculorum and others, suggesting that the investigation of Demodex spp. positivity would be beneficial for prompt diagnosis and treatment of these conditions [16,17,18,27].
An investigation of the prevalence of D. folliculorum mites in patients with polycystic ovary syndrome and an examination of the relationship between Demodex infestation and the presence of acne and oily or dry skin types in patients with polycystic ovary syndrome revealed positivity for D. folliculorum in 53.7% of patients with polycystic ovary syndrome, and it was significantly associated with acne and oily skin [22].
Interestingly, Demodex survival in makeup cosmetics (powder cream, mascara, and lipstick) has been demonstrated; therefore, products used by different individuals at short intervals, from several hours to several days, can be a source of D. folliculorum infection [28].
It is also worth raising awareness and knowledge about demodicosis and its clinical manifestations among aesthetic medicine doctors and cosmetologists, as a possible delayed diagnosis of visible lesions on facial skin could have a negative impact on patients’ well-being and normal functioning [12].
In children, demodicosis, especially HIV and leukemia, was first reported in immunosuppressed patients. It has also been linked to Langerhans cell histiocytosis, acute lymphoblastic leukemia, and T-cell non-Hodgkin lymphoma. Nevertheless, many healthy children have also been reported [29,30]. Demodicosis should be suspected in all children with papulopustular eruptions on the face or in cases of refractory facial inflammatory disorders, such as periorificial dermatitis and childhood rosacea. In a recent study, either complete clearance of primary demodicosis or control of secondary demodicosis was achieved by decreasing the mite burden [31].
Furthermore, patients with rosacea and primary demodicosis present with a significantly greater rate of Demodex blepharitis and must be evaluated for ocular involvement when they are treated for facial complaints. As the treatment of chronic blepharitis could be rather challenging, the evaluation of patients with facial burning, stinging, itching, and redness complaints in terms of examining both the face and eyelash Demodex will contribute to efficient treatment [32]. The incidence of ocular demodicosis ranges from 29% to 91% across a variety of geographic locations and study populations, increases with age, and is associated with several eyelid disorders [33]. Demodex should be considered in the presence of anterior blepharitis, keratitis, chalazia, or dry eye disease that is unresponsive to conventional treatments. The coexistence of chronic severe rosacea makes diagnosis and treatment even more challenging. Further research is needed to understand Demodex pathogenicity and its association with ocular diseases, specifically the relationships between Demodex and the immune system, which may lead to the identification of new therapeutic targets [34]. Demodex spp. can cause dermatological and ophthalmological problems. Infestation is rather common in adults and elderly individuals, but recently, interest in the presence of Demodex sp. mites in children has increased. Demodex spp. are related to the pathogenesis of numerous dermatoses and common eye dysfunctions. Recently, in addition to bacteriological tests, parasitological analysis has been suggested for both dermatological and eye microbiological diagnostics. Prevention is crucial and mostly relies on thorough hygiene of the skin and the eye area. Therapeutic approaches aim to inhibit the proliferation of parasites, eliminate them and prevent relapses. Antiparasitics (ivermectin, metronidazole) and essential oils are often used. Treatment of patients is a challenging and long-lasting task, thus rendering prompt diagnosis and appropriate therapeutic approach selection of particular significance for successful treatment, especially for younger individuals [35]. We realize that this study has limitations, as it does not concern a case–control study. Our intentions were to document observations related to Demodex infestation, sex and the age of patients who presented to the clinic with cheek redness, itching, and skin sensitivity following referral from dermatologists. Future studies should include a carefully designed study, also involving healthy control individuals and quantification of parasite numbers, to gain deeper insight into this important parasite and its health implications.
5. Conclusions
In conclusion, the association between symptoms such as cheek redness, itching, skin sensitivity and the presence (or absence) of demodicosis is important for the early diagnosis and treatment of several related skin diseases, including rosacea and pityriasis folliculorum. In Greece and many other countries, demodicosis is overlooked. Further studies are needed to better understand the pathogenic role of Demodex mites with respect to the density of the mite population and host characteristics, including sex and age. A more complete determination of high-risk groups and evaluation of patients with skin conditions that favor or are favored by Demodex mite infestation may contribute to the prompt and successful treatment of these pathological conditions.
Author Contributions
Conceptualization, A.K. and E.P.; methodology, A.K. and S.B.; formal analysis, A.K., S.B. and E.P.; investigation, A.K.; writing—original draft preparation, A.K.; writing—review and editing, A.K. and E.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Institutional Scientific Board of the A. Syggros Hospital, Athens, Greece (Approval no and date: 2429/9 January 2017). No identifying details of patient records are included in this manuscript.
Informed Consent Statement
Written informed consent was obtained from the patients.
Data Availability Statement
All relevant data are reported in the paper.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Desch, C.; Nutting, B.W. Demodex folliculorum (Simon) and D. brevis Akbulatova of Man: Redescription and Reevaluation. J. Parasitol. 1972, 58, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Forton, F. Demodex and perifollicular inflammation in man: Review and report of 69 biopsies. Ann. Dermatol. Venereol. 1986, 113, 1047–1058. [Google Scholar] [PubMed]
- Panopoulou, A.D.; Ieronymaki, A.; Chryssou, S.E. Human Demodex mites (Demodex folliculorum and Demodex brevis) and Demodicosis. Acta Microbilogica Hell. 2017, 62, 7–16. [Google Scholar]
- Wesolowska, M.; Knysz, B.; Reich, A.; Blazejewska, D.; Czarnecki, M.; Gladysz, A.; Pozowski, A.; Misiuk-Hojlo, M. Prevalence of Demodex spp. in eyelash follicles in different populations. Arch. Med. Sci. 2014, 12, 319–324. [Google Scholar] [CrossRef]
- Bonnar, E.; Eustace, P.; Powell, F.C. The Demodex mite population in rosacea. J. Am. Acad. Dermatol. 1993, 28, 443–448. [Google Scholar] [CrossRef]
- Forton, F.; Seys, B. Density of Demodex folliculorum in rosacea: A case-control study using standardized skin surface biopsy. Br. J. Dermatol. 1993, 128, 650–659. [Google Scholar] [CrossRef] [PubMed]
- Forton, F.M. Papulopustular rosacea, skin immunity and Demodex: Pityriasis folliculorum as a missing link. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 19–28. [Google Scholar] [CrossRef]
- Erbağci, Z.; Ozgöztaşi, O. The significance of Demodex folliculorum density in rosacea. Int. J. Dermatol. 1998, 37, 421–425. [Google Scholar] [CrossRef]
- Dolenc- Voljc, M.; Pohar, M.; Lunder, T. Density of Demodex folliculorum in perioral dermatitis. Acta Derm. Venereol. 2005, 85, 211–215. [Google Scholar] [CrossRef]
- Smith, G.; Manzano Marín, A.; Reyes-Prieto, M.; Ribeiro Antunes, C.S.; Ashworth, V.; Goselle, O.N.; Jan, A.A.A.; Moya, A.; Latorre, A.; Perotti, M.A.; et al. Human follicular mites: Ectoparasites becoming symbionts. Mol. Biol. Evol. 2022, 21, 39. [Google Scholar] [CrossRef]
- Plewig, G.; Kligman, A.M. Acne and Rosacea, 3rd ed.; Springer: Berlin/Heidelberg, Germany, 2000; pp. 507–508. [Google Scholar]
- Przydatek-Tyrajska, R.; Sędzikowska, A.; Bartosik, K. Primary facial demodicosis as a health problem and aesthetic challenge: A case report. J. Cosmet. Dermatol. 2021, 20, 420–424. [Google Scholar] [CrossRef]
- Baima, B.; Sticherling, M. Demodicidosis revisited. Acta Derm. Venereol. 2002, 82, 3–6. [Google Scholar] [CrossRef]
- Ricardo-Gonzalez, R.R.; Kotas, M.E.; O’Leary, C.E.; Singh, K.; Damsky, W.; Liao, C.; Arouge, E.; Tenvooren, I.; Marquez, D.M.; Schroeder, A.W.; et al. Innate type 2 immunity controls hair follicle commensalism by Demodex mites. Immunity 2022, 11, 1891–1908. [Google Scholar] [CrossRef]
- Lacey, N.; Kavanagh, K.; Tseng, S.C. Under the lash: Demodex mites in human diseases. Biochemist 2009, 1, 2–6. [Google Scholar] [CrossRef]
- Karabay, A.E.; Çerman, A.A. Demodex folliculorum infestations in common facial dermatoses: Acne vulgaris, rosacea, seborrheic dermatitis. An. Bras. Dermatol. 2020, 95, 187–193. [Google Scholar] [CrossRef]
- Erdal, B.; Albayrak, H. Investigation of the Prevalence of Demodex spp. in Dermatological Diseases. Turk. Parazitol. Derg. 2022, 1, 54–59. [Google Scholar] [CrossRef]
- Yasak-Guner, R.; Tosun, M.; Akyol, M.; Hayta, S.B. Demodex infestation as a cause of sensitive skin in a dermatology outpatient clinic. J. Cosmet. Dermatol. 2022, 21, 1610–1615. [Google Scholar] [CrossRef]
- Zeytun, E.; Yazıcı, M. Human Demodex Mites (Acari: Demodicidae) as a Possible Etiological Factor in Rosacea—A Cross-Sectional Study from Turkey. Res. Sq. 2023. [Google Scholar] [CrossRef]
- Aşkin, U.; Seçkin, D. Comparison of the two techniques for measurement of the density of Demodex folliculorum: Standardized skin surface biopsy and direct microscopic examination. Br. J. Dermatol. 2010, 162, 1124–1126. [Google Scholar] [CrossRef]
- Forton, F.; Germaux, M.A.; Brasseur, T.; De Liever, A.; Laporte, M.; Mathys, C.; Sass, U.; Stene, J.J.; Thibaut, S.; Tytgat, M.; et al. Demodicosis and rosacea: Epidemiology and significance in daily dermatologic practice. J. Am. Acad. Dermatol. 2005, 52, 74–87. [Google Scholar] [CrossRef]
- Eser, A.; Erpolat, S.; Kaygusuz, I.; Balci, H.; Kosus, A. Investigation of Demodex folliculorum frequency in patients with polycystic ovary syndrome. An. Bras. Dermatol. 2017, 92, 807–810. [Google Scholar] [CrossRef] [PubMed]
- Karapsias, S.; Patelis, A.; Sgourou, A. Demodex Outbreak Causing Palpebra Skin Lesions. J. Pigment. Disord. 2017, 4, 1–2. [Google Scholar]
- Georgala, S.; Katoulis, A.C.; Kylafis, G.D.; Koumantaki-Mathioudaki, E.; Georgala, C.; Aroni, K. Increased density of Demodex folliculorum and evidence of delayed hypersensitivity reaction in subjects with papulopustular rosacea. J. Eur. Acad. Dermatol. Venereol. 2001, 15, 441–444. [Google Scholar] [CrossRef]
- Lazaridou, E.; Apalla, Z.; Sotiraki, S.; Ziakas, N.G.; Fotiadou, C.; Ioannides, D. Clinical and laboratory study of rosacea in northern Greece. J. Eur. Acad. Dermatol. Venereol. 2010, 24, 410–414. [Google Scholar] [CrossRef]
- Aylesworth, R.; Vance, C. Demodex folliculorum and Demodex brevis in cutaneous biopsies. J. Am. Acad. Dermatol. 1982, 7, 583–589. [Google Scholar] [CrossRef]
- Paichitrojjana, A.; Chalermchai, T. The Association Between Acne Vulgaris, Acne Vulgaris with Nonspecific Facial Dermatitis, and Demodex Mite Presence. Clin. Cosmet. Investig. Dermatol. 2024, 22, 137–146. [Google Scholar] [CrossRef]
- Sędzikowska, A.; Bartosik, K.; Przydatek-Tyrajska, R.; Dybicz, M. Shared Makeup Cosmetics as a Route of Demodex folliculorum Infections. Acta Parasitol. 2021, 66, 631–637. [Google Scholar] [CrossRef]
- Van Atteveld, J.; Graaf, M.; Grotel, M.; Van den Heuvel-Eibrink, M.M. Demodicosis in Pediatric Cancer. J. Pediatr. Hematol. Oncol. 2017, 39, 402–406. [Google Scholar] [CrossRef]
- Álvarez-Salafranca, M.; Vicente, A.; Prat Torres, C.; Combalia, A.; Monsonís, M.; Celis-Passini, V.P.; González-Enseñat, M.A. Demodicosis in two patients with a previous history of Langerhans cell histiocytosis. Pediatr. Dermatol. 2017, 34, e299–e301. [Google Scholar] [CrossRef]
- Douglas, A.; Zaenglein, A.L. A case series of demodicosis in children. Pediatr. Dermatol. 2019, 36, 651–654. [Google Scholar] [CrossRef]
- Sarac, G.; Cankaya, C.; Ozcan, K.N.; Cenk, H.; Kapicioglu, Y.K. Increased frequency of Demodex blepharitis in rosacea and facial demodicosis patients. J. Cosmet. Dermatol. 2020, 19, 1260–1265. [Google Scholar] [CrossRef]
- Zhang, A.C.; Muntz, A.; Wang, M.T.M.; Craig, J.P.; Downie, L.E. Ocular Demodex: A systematic review of the clinical literature. Ophthalmic Physiol. Opt. 2020, 40, 389–432. [Google Scholar] [CrossRef]
- Cheng, A.M.; Galor, A.; Banoub, R.; Gupta, S.K. The impact of ocular demodicosis on the eyes. Eye 2023, 37, 3061–3062. [Google Scholar] [CrossRef]
- Chudzicka-Strugała, I.; Gołębiewska, I.; Brudecki, G.; Elamin, W.; Zwoździak, B. Demodicosis in Different Age Groups and Alternative Treatment Options—A Review. J. Clin. Med. 2023, 19, 1649. [Google Scholar] [CrossRef]
Figure 1.
The age distribution of the patients was statistically normal (p = 0.2), and the median age was 51.29 years.
Figure 1.
The age distribution of the patients was statistically normal (p = 0.2), and the median age was 51.29 years.

Figure 2.
Microscopic examination of Demodex mites from patients at (a) ×10 and (b) ×40 magnification.
Figure 2.
Microscopic examination of Demodex mites from patients at (a) ×10 and (b) ×40 magnification.

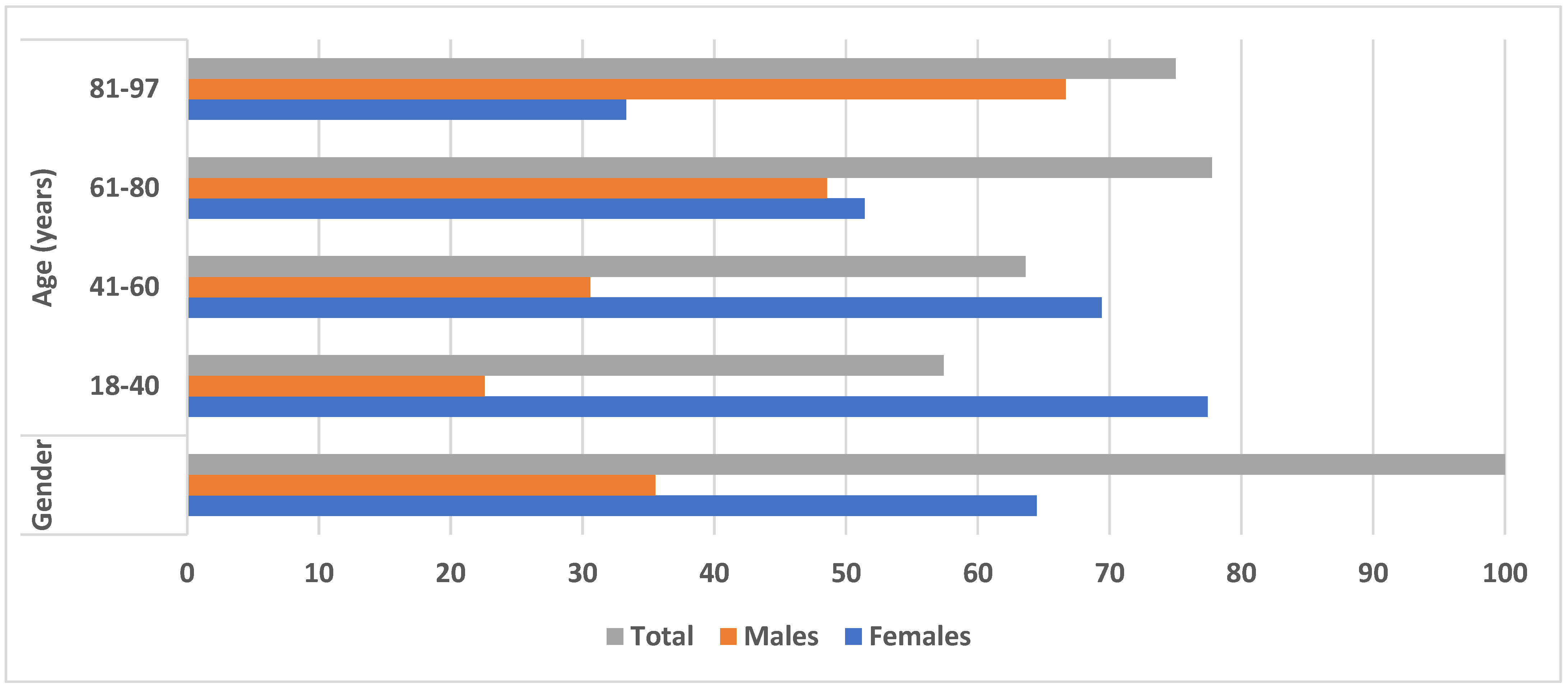
Figure 3.
Prevalence of demodicosis in male and female patients by age group and gender (percentage).
Figure 3.
Prevalence of demodicosis in male and female patients by age group and gender (percentage).


{kind=link}
{kind=link}
{kind=link}
Table 1.
Prevalence of Demodex mite infection in patients according to the studied parameters (gender and age).
Table 1.
Prevalence of Demodex mite infection in patients according to the studied parameters (gender and age).
| Prevalence of Demodex spp. | Parameters | ||||
|---|---|---|---|---|---|
| Gender Number/Percentage | Age (Years) | ||||
| 18–40 | 41–60 | 61–80 | 81–97 | ||
| Female | 78 (64.46%) | 24 (77.42%) | 34 (69.4%) | 18 (51.42%) | 2 (33.33%) |
| Male | 43 (35.54%) | 7 (22.58%) | 15 (30.6%) | 17 (48.57%) | 4 (66.67%) |
| Total | 121 (100%) | 31 (57.41%) | 49 (63.63%) | 35 (77.77%) | 6 (75%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kargadouri, A.; Beleri, S.; Patsoula, E. Data on Demodex Ectoparasite Infestation in Patients Attending an Outpatient Clinic in Greece. Parasitologia 2024, 4, 129-136. https://0-doi-org.brum.beds.ac.uk/10.3390/parasitologia4020011
AMA Style
Kargadouri A, Beleri S, Patsoula E. Data on Demodex Ectoparasite Infestation in Patients Attending an Outpatient Clinic in Greece. Parasitologia. 2024; 4(2):129-136. https://0-doi-org.brum.beds.ac.uk/10.3390/parasitologia4020011
Chicago/Turabian StyleKargadouri, Anastasia, Stavroula Beleri, and Eleni Patsoula. 2024. "Data on Demodex Ectoparasite Infestation in Patients Attending an Outpatient Clinic in Greece" Parasitologia 4, no. 2: 129-136. https://0-doi-org.brum.beds.ac.uk/10.3390/parasitologia4020011