
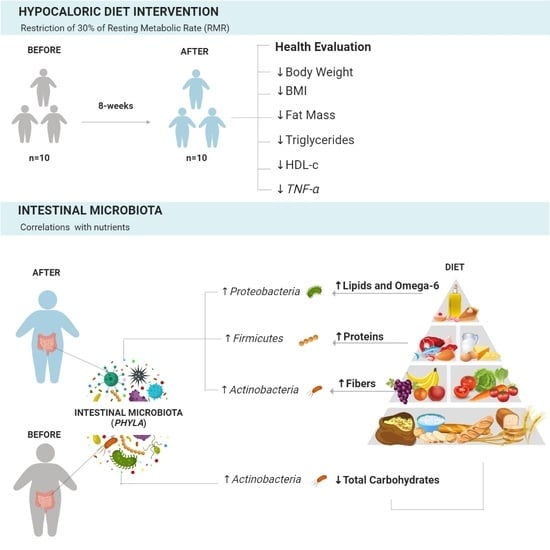
Ability of Hypocaloric Diets to Change Nutrient–Phyla Associations after 8 Weeks of Intervention

 , ,
, ,  ,
,  ,
,  , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
2.3. Hypocaloric Diet Intervention
2.3.1. Food Plan Selection
2.3.2. Food Plan Follow-Up
2.4. Anthropometric Evaluation
2.5. Dietary Intake Assessment
2.6. Biological Sampling and Blood Analysis
2.7. Gut Microbiota Analysis
2.8. Statistical Analysis
3. Results
3.1. Phenotypic Characteristics
3.2. Relationship between Gut Microbiota and Dietary Intake
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pesquisa do IBGE Mostra Aumento da Obesidade Entre Adultos. Available online: https://www.gov.br/pt-br/noticias/saude-e-vigilancia-sanitaria/2020/10/pesquisa-do-ibge-mostra-aumento-da-obesidade-entre-adultos#:~:text=A%20propor%C3%A7%C3%A3o%20de%20obesos%20na,%25%20para%2022%2C8%25 (accessed on 13 January 2023).
- Bernal, R.T.I.; Iser, B.P.M.; Malta, D.C.; Claro, R.M. Sistema de Vigilância de Fatores de Risco e Proteção para Doenças Crônicas por Inquérito Telefônico (Vigitel): Mudança na metodologia de ponderação. Epidemiol. Serviços Saúde 2017, 26, 701–712. [Google Scholar] [CrossRef] [PubMed]
- James, P.T.; Leach, R.; Kalamara, E.; Shayeghi, M. The Worldwide Obesity Epidemic. Obes. Res. 2001, 9, 228S–233S. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.; Versalovic, J. Microbial Metabolism in the Mammalian Gut: Molecular Mechanisms and Clinical Implications. J. Pediatr. Gastroenterol. Nutr. 2018, 66, S72–S79. [Google Scholar] [CrossRef] [PubMed]
- Costello, E.K.; Lauber, C.L.; Hamady, M.; Fierer, N.; Gordon, J.I.; Knight, R. Bacterial Community Variation in Human Body Habitats Across Space and Time. Science 2009, 326, 1694–1697. [Google Scholar] [CrossRef]
- Gomes, A.C.; Hoffmann, C.; Mota, J.F. The human gut microbiota: Metabolism and perspective in obesity. Gut Microbes 2018, 18, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Panel on Energy and Related Compounds. Dietary Reference Intakes for Energy, Carbohydrates, Fibers, Fat, Fat Acids, Cholesterol, Protein and Aminoacids; National Academies Press: Washington, DC, USA, 2000. [Google Scholar]
- Livak, K.J.; Schmittgen, T.D. Analysis of Relative Gene Expression Data Using Real-Time Quantitative PCR and the 2−ΔΔCT Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- Barman, M.; Unold, D.; Shifley, K.; Amir, E.; Hung, K.; Bos, N.; Salzman, N. Enteric Salmonellosis Disrupts the Microbial Ecology of the Murine Gastrointestinal Tract. Infect. Immun. 2008, 76, 907–915. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.W.; Chen, M.K.; Yang, B.Y.; Huang, X.J.; Zhang, X.R.; He, L.Q.; Zhang, J.; Hua, Z.C. Use of 16S rRNA Gene-Targeted Group-Specific Primers for Real-Time PCR Analysis of Predominant Bacteria in Mouse Feces. Appl. Environ. Microbiol. 2015, 81, 6749–6756. [Google Scholar] [CrossRef] [PubMed]
- Kolodziejczyk, A.A.; Zheng, D.; Elinav, E. Diet–microbiota interactions and personalized nutrition. Nat. Rev. Microbiol. 2019, 17, 742–753. [Google Scholar] [CrossRef]
- Sorgente, A.; Pietrabissa, G.; Manzoni, G.M.; Re, F.; Simpson, S.; Perona, S.; Rossi, A.; Cattivelli, R.; Innamorati, M.; Jackson, J.B.; et al. Web-Based Interventions for Weight Loss or Weight Loss Maintenance in Overweight and Obese People: A Systematic Review of Systematic Reviews. J. Med. Internet Res. 2017, 19, e229. [Google Scholar] [CrossRef]
- Hernández-Reyes, A.; Cámara-Martos, F.; Molina-Luque, R.; Romero-Saldaña, M.; Molina-Recio, G.; Moreno-Rojas, R. Changes in body composition with a hypocaloric diet combined with sedentary, moderate and high-intense physical activity: A randomized controlled trial. BMC Womens Health 2019, 19, 167. [Google Scholar] [CrossRef] [PubMed]
- Magkos, F.; Fraterrigo, G.; Yoshino, J.; Luecking, C.; Kirbach, K.; Kelly, S.C.; de Las Fuentes, L.; He, S.; Okunade, A.L.; Patterson, B.W.; et al. Effects of Moderate and Subsequent Progressive Weight Loss on Metabolic Function and Adipose Tissue Biology in Humans with Obesity. Cell Metab. 2016, 23, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Cortes-Oliveira, C.; Nicoletti, C.F.; de Souza Pinhel, M.A.; de Oliveira, B.A.P.; Quinhoneiro, D.C.G.; Noronha, N.Y.; Marchini, J.S.; da Silva Júnior, W.A.; Júnior, W.S.; Nonino, C.B. UCP2 expression is associated with weight loss after hypocaloric diet intervention. Eur. J. Clin. Nutr. 2017, 71, 402–406. [Google Scholar] [CrossRef]
- Johnson, E.L.; Heaver, S.L.; Walters, W.A.; Ley, R.E. Microbiome and metabolic disease: Revisiting the bacterial phylum Bacteroidetes. J. Mol. Med. 2017, 95, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Deehan, E.C.; Zhang, Z.; Riva, A.; Armet, A.M.; Perez-Muñoz, M.E.; Nguyen, N.K.; Krysa, J.A.; Seethaler, B.; Zhao, Y.Y.; Cole, J.; et al. Elucidating the role of the gut microbiota in the physiological effects of dietary fiber. Microbiome 2022, 10, 77. [Google Scholar] [CrossRef] [PubMed]
- Barczynska, R.; Slizewska, K.; Litwin, M.; Szalecki, M.; Zarski, A.; Kapusniak, J. The effect of dietary fiber preparations from potato starch on the growth and activity of bacterial strains belonging to the phyla Firmicutes, Bacteroidetes, and Actino-bacteria. J. Funct. Foods 2015, 19, 661–668. [Google Scholar] [CrossRef]
- Ballard, K.D.; Quann, E.E.; Kupchak, B.R.; Volk, B.M.; Kawiecki, D.M.; Fernandez, M.L.; Seip, R.L.; Maresh, C.M.; Kraemer, W.J.; Volek, J.S. Dietary carbohydrate restriction improves insulin sensitivity, blood pressure, microvascular function, and cellular adhesion markers in individuals taking statins. Nutr. Res. 2013, 33, 905–912. [Google Scholar] [CrossRef] [PubMed]
- Schoeler, M.; Caesar, R. Dietary lipids, gut microbiota and lipid metabolism. Rev. Endocr. Metab. Disord. 2019, 20, 461–472. [Google Scholar] [CrossRef] [PubMed]
- Méndez-Salazar, E.O.; Ortiz-López, M.G.; Granados-Silvestre M de los, Á.; Palacios-González, B.; Menjivar, M. Altered Gut Microbiota and Compositional Changes in Firmicutes and Proteobacteria in Mexican Undernourished and Obese Children. Front. Microbiol. 2018, 9, 2494. [Google Scholar]
- Vaughn, A.C.; Cooper, E.M.; DiLorenzo, P.M.; O’Loughlin, L.J.; Konkel, M.E.; Peters, J.H.; Hajnal, A.; Sen, T.; Lee, S.H.; de La Serre, C.B.; et al. Energy-dense diet triggers changes in gut microbiota, reorganization of gut-brain vagal communication and increases body fat accumulation. Acta Neurobiol. Exp. 2017, 77, 18–30. [Google Scholar] [CrossRef]
- He, J.; Zhang, P.; Shen, L.; Niu, L.; Tan, Y.; Chen, L.; Zhao, Y.; Bai, L.; Hao, X.; Li, X.; et al. Short-Chain Fatty Acids and Their Association with Signalling Pathways in Inflammation, Glucose and Lipid Metabolism. Int. J. Mol. Sci. 2020, 21, 6356. [Google Scholar] [CrossRef] [PubMed]
- Albracht-Schulte, K.; Islam, T.; Johnson, P.; Moustaid-Moussa, N. Systematic Review of Beef Protein Effects on Gut Microbiota: Implications for Health. Adv. Nutr. 2021, 12, 102–114. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Phylum | Primer Sequence |
|---|---|
| Firmicutes | F-ATGTGGTTTAATTCGAAGCA R-AGCTGACGACAACCATGCAC |
| Bacteroides | F-GTTTAATTCGATGATACGCGAG R-TTAASCCGACACCTCACGG |
| Actinobacteria | F-TGTAGCGGTGGAATGCGC R-AATTAAGCCACATGCTCCGCT |
| Proteobacteria | F-CATGACGTTACCCGCAGAAGAAG R-CTCTACGAGACTCAAGCTTGC |
| Verrucomicrobia | F-TCAKGTCAGTATGGCCCTTAT R-CAGTTTTYAGGATTTCCTCCGCC |
| rRNA 16S universal | F-AACAGGATTAGATACCCTGGTAG R-GGTTCTTCGCGTTGCATC |
| Parameters | Obese Group (ObG) (n = 10) | |
|---|---|---|
| Before | After | |
| Weight (kg) | 119.5 ± 10.3 | 114.9 ± 10.2 * |
| BMI (kg/m2) | 43.6 ± 2.4 | 41.9 ± 2.6 ± 2.6 * |
| Abdominal circumference (cm) | 123.3 ± 10.8 | 121.4 ± 7.1 |
| Fat mass (kg) | 62.4 ± 7.5 | 58.9 ± 7.7 * |
| Fat mass (%) | 51.9 ± 2.5 | 50.9 ± 2.7 |
| Fat-free mass (kg) | 57.1 ± 3.8 | 55.9 ± 3.6 |
| Fat-free mass (%) | 48.1 ± 2.5 | 49.1 ± 2.7 |
| RMR (kcal/day) | 1976.3 ± 256.1 | 1942.1 ± 288.9 |
| Fasting glucose (mg/dL) | 95.2 ± 18.1 | 91 ± 14.9 |
| Total cholesterol (mg/dL) | 196.0 ±25.7 | 184.0 ± 41.7 |
| HDL-cholesterol (mg/dL) | 45.9 ± 6.8 | 41.2 ± 8.0 * |
| LDL-cholesterol (mg/dL) | 121.4 ± 27.8 | 119.4 ± 23.9 |
| Triglycerides (mg/dL) | 143.2 ±60.9 | 117.94 ± 48.3 * |
| Nutrients | Obese Group (ObG) (n = 10) | |
|---|---|---|
| Before | After | |
| Energy (kcal/day) | 1679.9 ± 279.0 | 1140.5 ± 196.1 * |
| Carbohydrate (g/day) | 196.4 ± 43.7 | 127.6 ± 23.1 * |
| Carbohydrate (%TEI) | 47.2 ± 4.7 | 46.2 ± 10.6 |
| Protein (g/day) | 78.4 ± 15.7 | 63.0 ± 10.4 * |
| Protein (%TEI) | 18.8 ± 2.5 | 22.7 ± 4.7 |
| Total Lipids (g/day) | 62.1 ± 9.1 | 41.3 ± 23.7 |
| Total Lipids (%TEI) | 32.2 ± 6.9 | 30.7 ± 13.1 |
| Fibers (g/day) | 9.3 ± 3.5 | 11.4 ± 2.5 |
| Cholesterol (mg/day) | 269.5 ± 64.5 | 240.7 ± 110.3 |
| SFAs (g/day) | 22.4 ± 5.2 | 13.7 ± 8.4 * |
| MUFAs (g/day) | 19.9 ± 5.2 | 15.9 ± 12.01 |
| PUFAs (g/day) | 9.9 ± 3.1 | 6.0 ± 2.2 * |
| Phyla | Firmicutes | Actinobacteria | Proteobacteria | |||
|---|---|---|---|---|---|---|
| Before Intervention | ||||||
| Correlation | r | p | r | p | r | p |
| CHO (%) | 0.017 | 0.966 | −0.929 | 0.001 * | 0.36 | 0.342 |
| After Intervention | ||||||
| Correlation | r | p | r | p | r | p |
| Fibers (g) | 0.586 | 0.097 | 0.787 | 0.012 * | 0.218 | 0.574 |
| Protein (%) | 0.736 | 0.024 * | 0.285 | 0.485 | −0.435 | 0.242 |
| Total Lipids (%) | 0.469 | 0.203 | −0.117 | 0.764 | 0.669 | 0.049 * |
| Omega-6 (g) | 0.485 | 0.185 | 0.201 | 0.604 | 0.680 | 0.045 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noronha, N.Y.; Martins, L.d.S.; Watanabe, L.M.; de Souza Pinhel, M.A.; Rodrigues, G.d.S.; Schneider, I.M.; Nicoletti, C.F.; Delfino, H.B.P.; Carlos, D.; Nonino, C.B. Ability of Hypocaloric Diets to Change Nutrient–Phyla Associations after 8 Weeks of Intervention. Obesities 2024, 4, 45-54. https://0-doi-org.brum.beds.ac.uk/10.3390/obesities4020005
Noronha NY, Martins LdS, Watanabe LM, de Souza Pinhel MA, Rodrigues GdS, Schneider IM, Nicoletti CF, Delfino HBP, Carlos D, Nonino CB. Ability of Hypocaloric Diets to Change Nutrient–Phyla Associations after 8 Weeks of Intervention. Obesities. 2024; 4(2):45-54. https://0-doi-org.brum.beds.ac.uk/10.3390/obesities4020005
Chicago/Turabian StyleNoronha, Natália Yumi, Luzânia dos Santos Martins, Lígia Moriguchi Watanabe, Marcela Augusta de Souza Pinhel, Guilherme da Silva Rodrigues, Isabelle Mello Schneider, Carolina Ferreira Nicoletti, Heitor Bernardes Pereira Delfino, Daniela Carlos, and Carla Barbosa Nonino. 2024. "Ability of Hypocaloric Diets to Change Nutrient–Phyla Associations after 8 Weeks of Intervention" Obesities 4, no. 2: 45-54. https://0-doi-org.brum.beds.ac.uk/10.3390/obesities4020005