
Pain Assessment for Individuals with Advanced Dementia in Care Homes: A Systematic Review

 ,
,
Abstract
:1. Introduction
Aims of the Review
- To identify what pain assessment tools have been used to assess pain in advanced dementia care in care home settings globally including their psychometric properties; and
- To explore the implications of using pain assessment tools in practice through the medium of a narrative synthesis.
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Extraction and Critical Appraisal
- Study characteristics: author, date and country;
- Participant characteristics: diagnosed with a dementia, living in a care home setting;
- Aims of the study;
- Sample size, age range;
- Methodology: study collection, data collection process, synthesis of results, risks of bias;
- Pain assessment tool/s used;
- Main findings; and
- Recommendations made.
2.5. Quality Assessment
3. Results
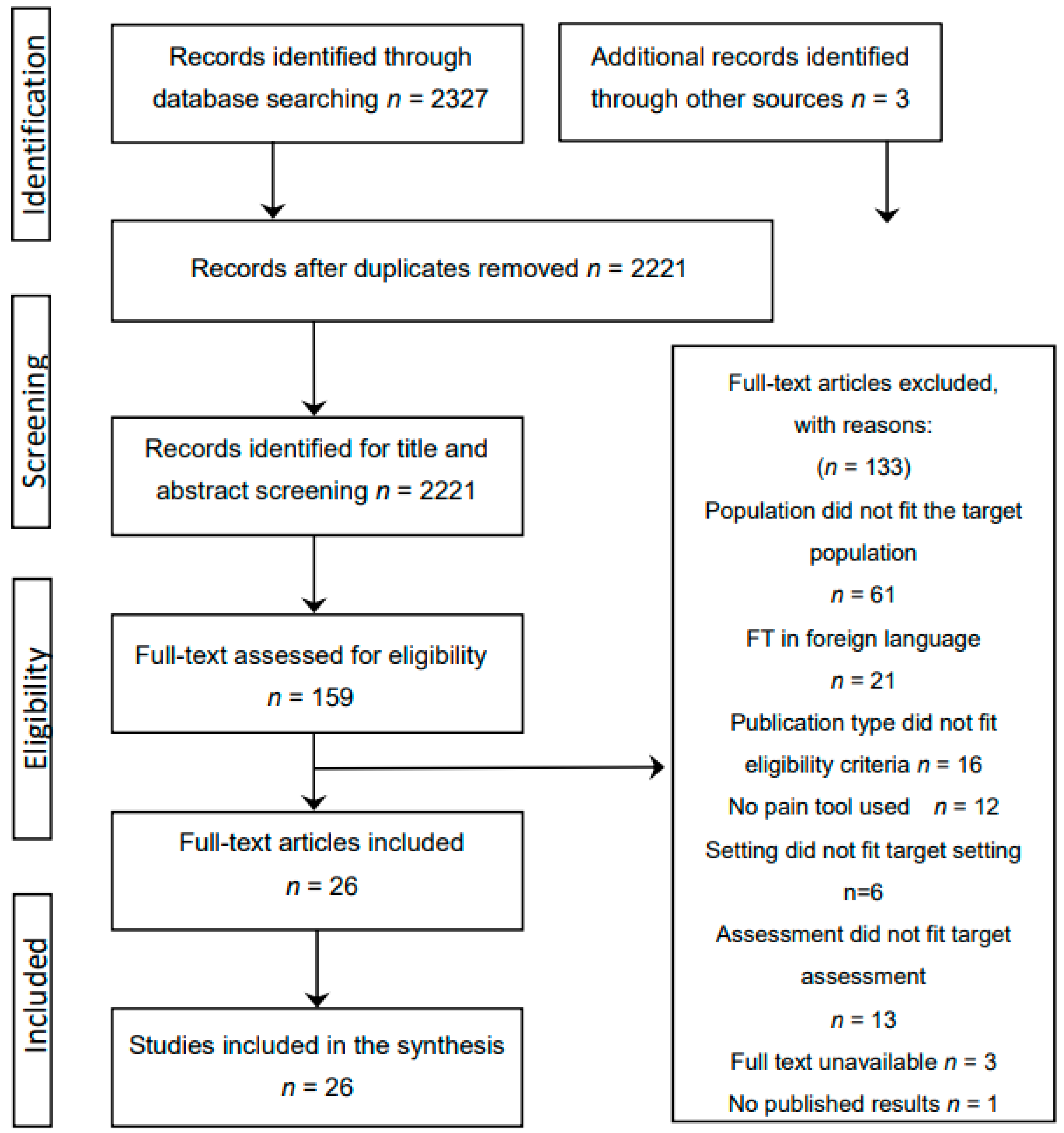
3.1. Search Results
3.2. Summary of the Studies
3.3. Quality Appraisal
3.4. Data Synthesis
3.4.1. Preliminary Synthesis
3.4.2. Primary Themes
Behavioural Indicators
- Facial expressions such as grimacing;
- Verbalisations and vocalisations such as groaning;
- Body movements, such as rocking;
- Changes in interpersonal interactions such as aggression;
- Changes in activity patterns and routines such as sleep; and
- Changes in mental state such as confusion.
Staff Training and Education
Affective Symptoms of Pain
Multi-Dimensional Assessment
4. Discussion
4.1. Summary of Findings
4.2. Methodological Critique
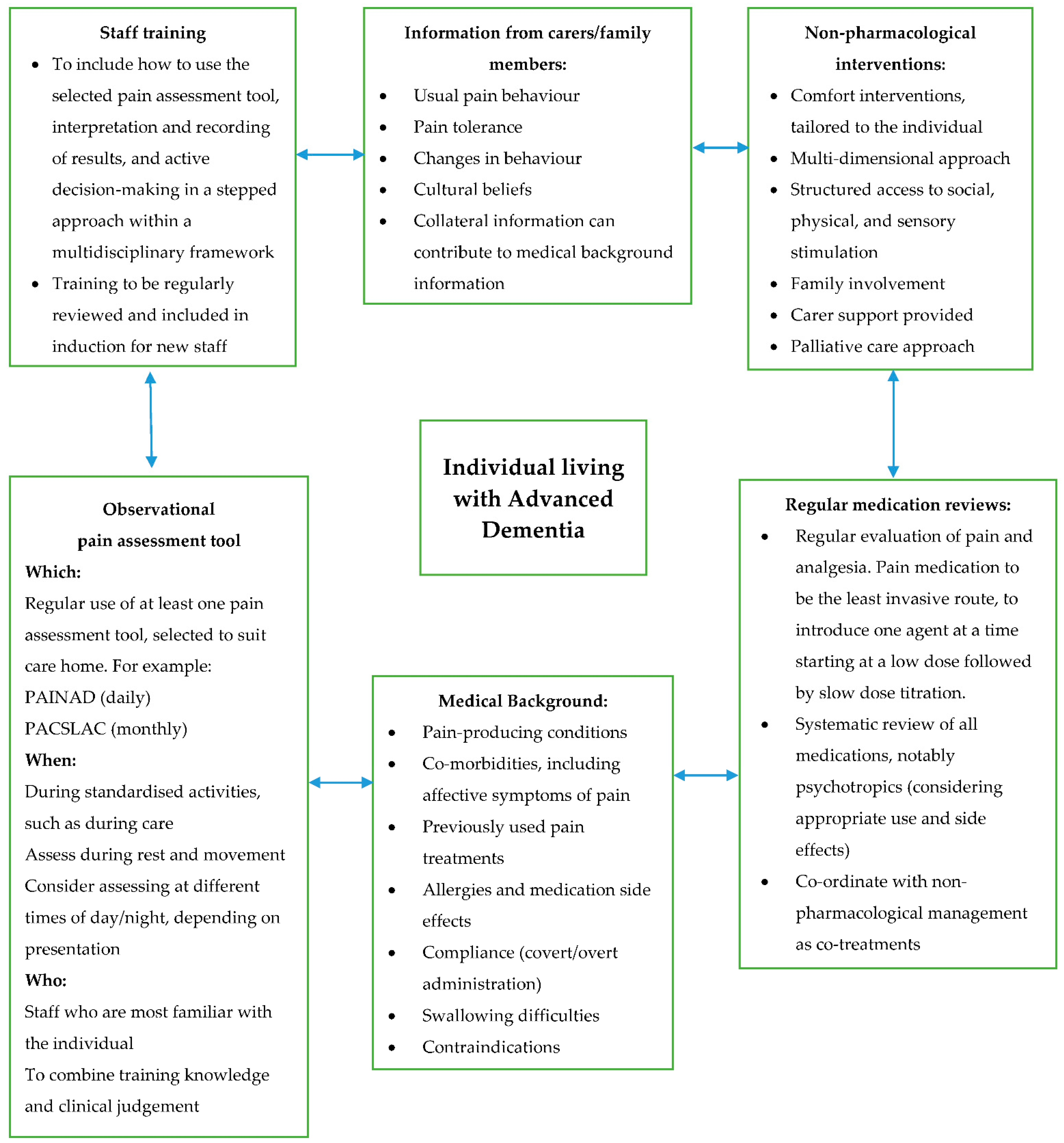
4.3. Implications for Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Closs, S.J.; Dowding, D.; Allcock, N.; Hulme, C.; Keady, J.; Sampson, E.; Briggs, M.; Corbett, A.; Esterhuizen, P.; Holmes, J.; et al. Towards improved decision support in the assessment and management of pain for people with dementia in hospital: A systematic meta-review and observational study. Health Serv. Deliv. Res. 2016, 4, 1–162. [Google Scholar] [CrossRef] [Green Version]
- Geddis-Regan, A.R.; Stewart, M.; Wassall, R.R. Orofacial pain assessment and management for patients with dementia: A meta-ethnography. J. Oral Rehabil. 2018, 46, 189–199. [Google Scholar] [CrossRef]
- Hadjistavropoulos, T.; Fitzgerald, T.D.; Marchildon, G. Practice Guidelines for Assessing Pain in Older Persons with Dementia Residing in Long-Term Care Facilities. Physiother. Can. 2010, 62, 104–113. [Google Scholar] [CrossRef]
- Schofield, P. The Assessment of Pain in Older People: UK National Guidelines. Age Ageing 2018, 47, i1–i22. [Google Scholar] [CrossRef]
- Zwakhalen, S.; Docking, R.E.; Gnass, I.; Sirsch, E.; Stewart, C.; Allcock, N.; Schofield, P. Pain in older adults with dementia: A survey across Europe on current practices, use of assessment tools, guidelines and policies. Schmerz 2018, 32, 364–373. [Google Scholar] [CrossRef] [Green Version]
- Lichtner, V.; Dowding, D.; Esterhuizen, P.; Closs, S.J.; Long, A.F.; Corbett, A.; Briggs, M. Pain assessment for people with dementia: A systematic review of systematic reviews of pain assessment tools. BMC Geriatr. 2014, 14, 1–19. [Google Scholar] [CrossRef]
- Tsai, Y.I.; Browne, G.; Inder, K.J. The effectiveness of interventions to improve pain assessment and management in people living with dementia: A systematic review and meta-analyses. J. Adv. Nurs. 2021, 77, 1127–1140. [Google Scholar] [CrossRef]
- Herr, K.; Bursch, H.; Miller, L.L.; Swafford, K. Use of pain-behavioural assessment tools in the nursing home. J. Gerontol. Nurs. 2010, 36, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Kupeli, N.; Leavey, G.; Harrington, J.; Lord, K.; King, M.; Nazareth, I.; Moore, K.; Sampson, E.; Jones, L. What are the barriers to care integration for those at the advanced stages of dementia living in care homes in the UK? Health care professional perspective. Dementia 2016, 17, 164–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petyaeva, A.; Kajander, M.; Lawrence, V.; Clifton, L.; Thomas, A.J.; Ballard, C.; Leroi, I.; Briggs, M.; Closs, J.; Dening, T.; et al. Feasibility of a staff training and support programme to improve pain assessment and management in people with dementia living in care homes. Int. J. Geriatr. Psychiatry 2017, 33, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Office of National Statistics, Overview of the UK Population 2019. Available online: https://www.ons.gov.uk/releases/overviewoftheukpopulationjuly2019 (accessed on 20 February 2020).
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; The PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [Green Version]
- Hong, Q.N.; Pluye, P.; Fabregues, S.; Bartlett, G.; Broadman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Appraisal Tool (MMAT), 2018, Canadian Intellectual Property Office, Industry Canada. Available online: http://mixedmethodsappraisaltoolpublic.pbworks.com/w/file/fetch/127916259/MMAT_2018_criteria-manual_2018-08-01_ENG.pdf. (accessed on 27 January 2021).
- Zwakhalen, S.M.G.; Hamers, J.P.H.; Abu-Saad, H.H.; Berger, M.P.F. Pain in elderly people with severe dementia: A sys-tematic review of behavioural pain assessment tools. BMC Geriatr. 2006, 6, 3–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coca, S.M.; Zuñiga, R.A.A. Instruments for pain assessment in patients with advanced dementia: A systematic review of the evidence for Latin America. Palliat. Support. Care 2020, 18, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Atee, M.; Hoti, K.; Parsons, R.; Hughes, J.D. A novel pain assessment tool incorporating automated facial analysis: Interrater reliability in advanced dementia. Clin. Interv. Aging 2018, 16, 1245–1258. [Google Scholar] [CrossRef] [Green Version]
- Cheung, G.; Choi, P. The use of the Pain Assessment Checklist for Seniors with Limited Ability to Communicate (PACSLAC) by caregivers in dementia care facilities. N. Z. Med. J. 2008, 121, 21–29. [Google Scholar] [PubMed]
- Cohen-Mansfield, J. Pain assessment in non-communicative elderly persons–PAINE. Clin. J. Pain 2006, 22, 569–575. [Google Scholar] [CrossRef] [Green Version]
- Cohen-Mansfield, J.; Lipson, S. The utility of pain assessment for analgesic use in persons with dementia. Pain 2008, 134, 16–23. [Google Scholar] [CrossRef]
- Ersek, M.; Nash, P.V.; Hilgeman, M.M.; Neradilek, M.B.; Herr, K.; Block, P.; Collins, A. Pain patterns and treatment among nursing home residents with moderate-severe cognitive impairment. Am. Geriatr. Soc. 2019, 68, 794–802. [Google Scholar] [CrossRef]
- Fuchs-Lacelle, S.; Hadjistavropoulos, T.; Lix, L. Pain assessment as intervention: A study of older adults with severe de-mentia. Clin. J. Pain 2008, 24, 697–707. [Google Scholar] [CrossRef]
- Griffioen, C.; Husebo, B.S.; Flo, E.; Caljouw, M.A.; Achterberg, W. Opioid Prescription Use in Nursing Home Residents with Advanced Dementia. Pain Med. 2019, 20, 50–57. [Google Scholar] [CrossRef]
- Hadjistavropoulos, T.; Browne, M.E.; Prkachin, K.M.; Taati, B.; Ashraf, A.; Mihailidis, A. Pain in severe dementia: A compari-son of a fine-grained assessment approach to an observational checklist designed for clinical settings. Eur. J. Pain 2018, 22, 915–925. [Google Scholar] [CrossRef]
- Hoti, K.; Atee, M.; Hughes, J.D. Clinimetric properties of the electronic Pain Assessment Tool (ePAT) for aged-care residents with moderate to severe dementia. J. Pain Res. 2018, 11, 1037–1044. [Google Scholar] [CrossRef] [Green Version]
- Husebo, B.S.; Strand, L.I.; Moe-Nilssen, R.; Husebo, S.B.; Ljunggren, A.E. Pain behaviour and pain intensity in older persons with severe dementia: Reliability of the MOBID Pain Scale by video uptake. Scand. J. Caring Sci. 2009, 23, 180–189. [Google Scholar] [CrossRef]
- Husebo, B.S.; Ostelo, R.; Strand, L.I. The MOBID-2 pain scale: Reliability and responsiveness to pain in patients with demen-tia. Eur. J. Pain 2014, 18, 1419–1430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordan, A.; Hughes, J.; Pakresi, M.; Hepburn, S.; O’Brien, J.T. The utility of PAINAD in assessing pain in a UK population with severe dementia. Int. J. Geriatr. Psychiatry 2011, 26, 118–126. [Google Scholar] [CrossRef]
- Jordan, A.; Regnard, C.; O’Brien, J.; Hughes, J.C. Pain and distress in advanced dementia: Choosing the right tools for the job. Palliat. Med. 2011, 26, 873–878. [Google Scholar] [CrossRef] [PubMed]
- Lints-Martindale, A.C.; Hadjistavropoulos, T.; Lix, L.M.; Thorpe, L. A comparative investigation of observational pain as-sessment tools for older adults with dementia. Clin. J. Pain 2012, 28, 226–237. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, A.E.J.; Peters, L. The Mahoney Pain Scale: Examining Pain and Agitation in Advanced Dementia. Am. J. Alzheimer’s Dis. Other Dementiasr 2008, 23, 250–261. [Google Scholar] [CrossRef] [PubMed]
- Malara, A.; De Biase, G.A.; Bettarini, F.; Ceravolo, F.; Di Cello, S.; Garo, M.; Praino, F.; Settembrini, V.; Sgro, G.; Spadea, F.; et al. Pain assessment in elderly with behavioural and psychological symptoms of dementia. J. Alz-heimer’s Dis. 2016, 50, 1217–1225. [Google Scholar] [CrossRef] [Green Version]
- Monacelli, F.; Nurse, A.V.; Odetti, P.; Traverso, N. Doloplus-2 pain assessment: An effective tool in patients over 85 years with advanced dementia and persistent pain. La Clin. Ter. 2013, 164, 23–25. [Google Scholar]
- Neville, C.; Ostini, R. A Psychometric Evaluation of Three Pain Rating Scales for People with Moderate to Severe Dementia. Pain Manag. Nurs. 2014, 15, 798–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nowak, T.; Neumann-Podczaska, A.; Deskur-Smielecka, E.; Styszynski, A.; Wieczorowska-Tobis, K. Pain as a challenge in nursing home residents with behavioural and psychological symptoms of dementia. Clin. Interv. Aging 2018, 13, 1045–1051. [Google Scholar] [CrossRef] [Green Version]
- Pieper, M.J.C.; van der Steen, J.; Francke, A.L.; Scherder, E.J.A.; Twisk, J.W.R.; Achterberg, W.P. Effects on pain of a stepwise multidisciplinary intervention (STA OP!) that targets pain and behaviour in advanced dementia: A cluster randomised con-trolled trial. Palliat. Med. 2018, 32, 682–692. [Google Scholar] [CrossRef]
- Rostad, H.M.; Utne, I.; Grov, E.K.; Smastuen, M.C.; Puts, M.; Halvorsrud, L. The impact of a pain assessment intervention on pain score and analgesic use in older nursing home residents with severe dementia: A cluster randomised controlled trial. Int. J. Nurs. Stud. 2018, 84, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Van Dalen-Kok, A.H.; Achterberg, W.P.; E Rijkmans, W.; De Vet, H.C.; De Waal, M.W. Pain assessment in impaired cognition: Observer agreement in a long-term care setting in patients with dementia. Pain Manag. 2019, 9, 461–473. [Google Scholar] [CrossRef]
- Van Kooten, J.; Smalbrugge, M.; van der Wouden, J.C.; Stek, M.L.; Hertogh, C.M. Prevalence of Pain in Nursing Home Residents: The Role of Dementia Stage and Dementia Subtypes. J. Am. Med Dir. Assoc. 2017, 18, 522–527. [Google Scholar] [CrossRef]
- Villanueva, M.R. Pain Assessment for the Dementing Elderly (PADE): Reliability and validity of a new measure. J. Am. Med Dir. Assoc. 2003, 4, 1–8. [Google Scholar] [CrossRef]
- Zwakhalen, S.M.; Koopmans, R.T.; Geels, P.J.; Berger, M.P.; Hamers, J.P. The prevalence of pain in nursing home residents with dementia measured using an observational pain scale. Eur. J. Pain 2009, 13, 89–93. [Google Scholar] [CrossRef]
- Zwakhalen, S.M.G.; van’t Hof, C.E.; Hamers, J.P.H. Systematic pain assessment using an observational scale in nursing home residents with dementia: Exploring feasibility and applied interventions. J. Clin. Nurs. 2012, 21, 3009–3017. [Google Scholar] [CrossRef]
- Economic and Social Research Council (ESRC) Guidance on the Conduct of Narrative Synthesis in Systematic Reviews. 2006. Available online: www.lancaster.ac.uk/media/lancaster-university/content-assets/documents/fhm/dhr/chir/NSsynthesisguidanceVersion1-April2006.pdf (accessed on 24 April 2019).
- Fordham, L. Pain assessment in people with dementia. In Physiotherapy in Mental Health and Psychiatry: A Scientific and Clinical Based Approach, 1st ed.; Probst, M., Skjaerven, L., Eds.; Elsevier: Warsaw, Poland, 2017; pp. 313–323. [Google Scholar]
- American Geriatrics Society. AGS Panel on persistent pain in older persons. J. Am. Geriatr. Soc. 2002, 50, S205–S224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babicova, I.; Cross, A.; Forman, D.; Hughes, J.; Hoti, K. Evaluation of the Psychometric Properties of PainChek® in UK Aged Care Residents with advanced dementia. BMC Geriatr. 2021, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kitwood, T. Dementia Reconsidered: The Person Comes First; Open University Press: Buckingham, UK, 1997. [Google Scholar]
- Alzheimer’s Disease International. World Alzheimer Report 2016; Improving Healthcare for People Living with Dementia. 2016. Available online: https://www.alzint.org/u/WorldAlzheimerReport2016.pdf (accessed on 23 March 2021).
- Alzheimer’s Society. Optimising Treatment and Care for People with Behavioural and Psychological Symptoms of Dementia: A Best Practice Guide for Health and Social Care Professionals; Alzheimer’s Society: London, UK, 2011. [Google Scholar]
- Taati, B.; Zhao, S.; Ashraf, A.B.; Asgarian, A.; Browne, M.E.; Prkachin, K.M.; Mihailidis, A.; Hadjistavropoulos, T. Algorithmic Bias in Clinical Populations—Evaluating and Improving Facial Analysis Technology in Older Adults with Dementia. IEEE Access 2019, 7, 25527–25534. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study ID | Location | Pain Assessment Tool/s Used | Type of Study | Pain Assessor | |
|---|---|---|---|---|---|
| Clinical Staff | Researcher | ||||
| Atee et al. 2018 [17] | Australia | Electronic Pain Assessment Tool [ePAT] | Observational | √ | |
| Cheung et al. 2008 [18] | New Zealand | Pain Assessment Checklist for Seniors with Limited Ability to Communicate [PACSLAC] | Observational | √ | √ |
| Cohen-Mansfield et al. 2006 [19] | USA | Checklist of Non-verbal Pain Indicators Scale [CNPI] Non-communicative Patient’s Pain Assessment Instrument [NOPAIN] Pain Assessment for the Dementing Elderly [PADE] Pain Assessment in Advanced Dementia [PAINAD] Pain Assessment in Non-communicative Elderly [PAINE] | Evaluation | √ | |
| Cohen-Mansfield et al. 2008 [20] | USA | CNPI PADE PAINAD PAINE | Evaluation | √ | |
| Ersek et al. 2020 [21] | USA | Mobilisation-Observation-Behavioural—Intensity-Dementia [MOBID] Pain Intensity Measure for Persons with Dementia [PIMD] | Evaluation | √ | √ |
| Fuchs-Lacelle et al. 2008 [22] | Canada | PACSLAC | Longitudinal study | √ | |
| Griffioen et al. 2017 [23] | Norway | MOBID-2 | Cross-sectional | Not stated | Not stated |
| Hadjistavropoulos et al. 2018 [24] | Canada | Facial Action Coding System [FACS] PACSLAC-II | Observational | √ | |
| Hoti et al. 2018 [25] | Australia | Abbey Pain Scale [APS] ePAT | Observational | √ | √ |
| Husebo et al. 2009 [26] | Norway | MOBID | Observational | √ | |
| Husebo et al. 2014 [27] | Norway | MOBID-2 | Cluster RCT | √ | |
| Jordan et al. 2011 [28] | UK | PAINAD | Observational | √ | √ |
| Jordan et al. 2011 [29] | UK | Disability Distress Assessment Tool [DisDAT] PAINAD | Observational | √ | √ |
| Lints-Martindale et al. 2012 [30] | Canada | Assessment of Discomfort in Dementia [ADD] CNPI PACSLAC PADE PAINAD Non-communicative Patients’ Pain Assessment Instrument [NOPAIN] | Observational | √ | |
| Mahoney et al. 2008 [31] | Australia | Mahoney Pain Scale [MPS] | Evaluation | √ | |
| Malara et al. 2016 [32] | Italy | PAINAD | Observational | √ | |
| Monacelli et al. 2013 [33] | Italy | DOLOPLUS-2 | Observational | √ | |
| Neville et al. 2014 [34] | Australia | APS CNPI DOLOPLUS-2 | Observational | √ | |
| Nowak et al. 2018 [35] | Poland | APS | Observational | √ | |
| Pieper et al. 2018 [36] | The Netherlands | Pain Assessment Checklist for Seniors with Limited Ability to Communicate-Dutch version [PACSLAC-D] | Cluster RCT | √ | |
| Rostad et al. 2018 [37] | Norway | DOLOPLUS-2 | Cluster RCT | √ | |
| Van Dalen-Kok et al. 2019 [38] | The Netherlands | Pain Assessment in Impaired Cognition [PAIC] | Observational | √ | |
| Van Kooten et al. 2017 [39] | The Netherlands | PAINAD MOBID-2 | Cross-sectional | n/a | n/a |
| Villanueva et al. 2003 [40] | USA | PADE | Evaluation | √ | |
| Zwakhalen et al. 2008 [41] | The Netherlands | PACSLAC-D | Observational | √ | |
| Zwakhalen et al. 2012 [42] | The Netherlands | PACSLAC-D | Observational | √ | |
| Study ID | PACSLAC (II, D) | PAINAD | MOBID and MOBID2 | CNPI | APS | DOLOPLUS-2 | PADE | e-PAT | ADD | DisDAT | FACS | MPS | NOPAIN | OPBAI | PAIC | PAINE | PIMD |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Atee et al. 2018 [17] | √ | ||||||||||||||||
| Cheung et al. 2008 [18] | √ | ||||||||||||||||
| Cohen-Mansfield et al. 2006 [19] | √ | √ | |||||||||||||||
| Cohen-Mansfield et al. 2008 [20] | √ | √ | √ | √ | √ | ||||||||||||
| Ersek et al. 2020 [21] | √ | √ | |||||||||||||||
| Fuchs-Lacelle et al. 2008 [22] | √ | ||||||||||||||||
| Griffioen et al 2017 [23] | √ | ||||||||||||||||
| Hadjistavropoulos et al. 2018 [24] | √ | √ | |||||||||||||||
| Hoti et al. 2018 [25] | √ | √ | |||||||||||||||
| Husebo et al. 2009 [26] | √ | ||||||||||||||||
| Husebo et al. 2014 [27] | √ | ||||||||||||||||
| Jordan et al. 2011 [28] | √ | ||||||||||||||||
| Jordan et al. 2011 [29] | √ | √ | |||||||||||||||
| Lints-Martindale et al. 2012 [30] | √ | √ | √ | √ | √ | √ | |||||||||||
| Mahoney et al. 2008 [31] | √ | ||||||||||||||||
| Malara et al. 2016 [32] | √ | ||||||||||||||||
| Monacelli et al. 2013 [33] | √ | ||||||||||||||||
| Neville et al. 2014 [34] | √ | √ | √ | ||||||||||||||
| Nowak et al. 2018 [35] | √ | ||||||||||||||||
| Pieper et al. 2018 [36] | √ | ||||||||||||||||
| Rostad et al. 2018 [37] | √ | ||||||||||||||||
| Van Dalen-Kok et al. 2019 [38] | √ | ||||||||||||||||
| Van Kooten et al. 2017 [39] | √ | √ | |||||||||||||||
| Villanueva et al. 2003 [40] | √ | ||||||||||||||||
| Zwakhalen et al. 2008 [41] | √ | ||||||||||||||||
| Zwakhalen et al. 2012 [42] | √ | ||||||||||||||||
| TOTAL | 7 | 7 | 5 | 4 | 3 | 3 | 3 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Study ID | Screen | Quantitative Randomised Controlled Trials | Quantitative Non-Randomised Studies | Total | |||||||||
| S1 | S2 | 2.1 | 2.2 | 2.3 | 2.4 | 2.5 | 3.1 | 3.2 | 3.3 | 3.4 | 3.5 | Y % | |
| Atee et al. 2018 [17] | Y | Y | Y | Y | N | Y | Y | 4 high | |||||
| Cheung et al. 2008 [18] | Y | Y | Y | Y | Y | Y | U | 4 high | |||||
| Cohen-Mansfield et al. 2006 [19] | Y | Y | Y | Y | Y | Y | U | 4 high | |||||
| Cohen-Mansfield et al. 2008 [20] | Y | Y | Y | Y | Y | Y | Y | 5 high | |||||
| Ersek et al. 2020 [21] | Y | Y | Y | Y | Y | Y | U | 4 high | |||||
| Fuchs-Lacelle et al 2008 [22] | Y | Y | Y | Y | Y | Y | Y | 5 high | |||||
| Griffioen et al. 2017 [23] | Y | Y | Y | Y | Y | Y | U | 4 high | |||||
| Hadjistavropoulos, et al. 2018 [24] | Y | Y | Y | Y | U | Y | Y | 4 high | |||||
| Hoti et al. 2018 [25] | Y | Y | Y | Y | Y | Y | Y | 5 high | |||||
| Husebo et al. 2009 [26] | Y | Y | Y | Y | N | Y | Y | 4 high | |||||
| Jordan et al. 2011 [28] | Y | Y | Y | Y | Y | N | Y | 4 high | |||||
| Jordan et al. 2011 [29] | Y | Y | Y | Y | Y | N | Y | 4 high | |||||
| Lints-Martindale et al. 2012 [30] | Y | Y | Y | Y | N | Y | Y | 4 high | |||||
| Mahoney et al. 2008 [31] | Y | Y | Y | Y | N | N | U | 2 low | |||||
| Malara et al. 2016 [32] | Y | Y | Y | Y | Y | Y | U | 4 high | |||||
| Monacelli et al. 2013 [33] | Y | Y | Y | Y | U | N | U | 2 low | |||||
| Neville et al. 2014 [34] | Y | Y | Y | Y | Y | Y | U | 4 high | |||||
| Nowak et al. 2018 [35] | Y | Y | Y | Y | Y | Y | Y | 5 high | |||||
| Van Dalen-Kok et al. 2019 [38] | Y | Y | Y | Y | N | Y | Y | 4 high | |||||
| Van Kooten et al. 2017 [39] | Y | Y | Y | Y | Y | Y | Y | 5 high | |||||
| Villanueva et al. 2003 [40] | Y | Y | Y | Y | Y | N | Y | 4 high | |||||
| Zwakhalen et al. 2008 [41] | Y | Y | Y | Y | Y | Y | N | 4 high | |||||
| Zwakhalen et al. 2012 [42] | Y | Y | Y | Y | N | Y | Y | 4 high | |||||
| Husebo et al. 2014 [27] | Y | Y | Y | Y | Y | Y | U | 4 high | |||||
| Pieperet et al. 2018 [36] | Y | Y | Y | Y | N | Y | Y | 4 high | |||||
| Rostad et al. 2018 [37] | Y | Y | Y | U | Y | Y | U | 3 moderate | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Felton, N.; Lewis, J.S.; Cockburn, S.-J.; Hodgson, M.; Dawson, S. Pain Assessment for Individuals with Advanced Dementia in Care Homes: A Systematic Review. Geriatrics 2021, 6, 101. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics6040101
Felton N, Lewis JS, Cockburn S-J, Hodgson M, Dawson S. Pain Assessment for Individuals with Advanced Dementia in Care Homes: A Systematic Review. Geriatrics. 2021; 6(4):101. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics6040101
Chicago/Turabian StyleFelton, Nansi, Jennifer S. Lewis, Sarah-Jane Cockburn, Margot Hodgson, and Shoba Dawson. 2021. "Pain Assessment for Individuals with Advanced Dementia in Care Homes: A Systematic Review" Geriatrics 6, no. 4: 101. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics6040101