
Advancements and Challenges in Non-Invasive Sensor Technologies for Swallowing Assessment: A Review


Abstract
:1. Introduction
2. Methods
2.1. Data Collection and Search Strategy
2.2. Criteria for Literature Inclusion and Exclusion
- -
- Studies that detail methods of swallowing assessment or introduce devices designed for this purpose.
- -
- Scientific articles that are written in English and accessible for review.
- -
- Research focused on devices or methods not directly related to the assessment of swallowing functionality.
- -
- Studies that are limited to evaluating system performance or clinical trials without providing insight into design methodologies.
3. Results
3.1. Anatomy of Swallowing
Swallowing Muscles
- -
- Lips and Cheeks: Involves orbicularis oris, buccinator, risorius, and muscles responsible for elevating and depressing the lips.
- -
- Tongue: Encompasses superior and inferior longitudinal, transverse, vertical, genioglossus, hyoglossus, styloglossus, and palatoglossus muscles.
- -
- Mandibular Muscles: Includes temporal, masseter, lateral and medial pterygoids.
- -
- Soft Palate: Comprises tensor veli palatini, palatoglossus, palatopharyngeus, levator veli palatini, and musculus uvulae.
- -
- Pharyngeal Musculature: Features anterior digastric, geniohyoid, stylohyoid, superior, middle, and inferior constrictors, along with palatopharyngeus and palatoglossus.
- -
- Upper Esophageal Sphincter: Primarily the cricopharyngeus muscle.
3.2. Physiology of Swallowing
- Oral Preparation and Propulsion Phase: The oral phase involves the manipulation of food by the tongue, preparation of the bolus with saliva, and its propulsion towards the pharynx. This stage varies in complexity based on the texture of the ingested material, requiring meticulous coordination of sensory feedback and muscle action to prevent premature leakage into the pharynx [18,22].
- Pharyngeal Phase: This critical phase encompasses a rapid series of events, including pharyngeal peristalsis, UES relaxation, and glottic closure to ensure safe passage of the bolus into the esophagus while protecting the airway from aspiration. The coordinated lifting of the soft palate, retraction of the tongue base, and sequential constriction of pharyngeal muscles facilitate the downward movement of food.
- Esophageal Phase: The process of food passing through the esophagus involves several steps. Initially, the entry of food prompts peristaltic movements in the esophagus, accompanied by the coordinated opening and closing of the esophageal sphincters, ensuring the smooth transport of the bolus to the stomach. Additionally, the contraction of smooth muscles and the regulation of internal pressure within the esophagus are necessary to facilitate the movement of food.
4. Methods of Swallowing Assessment
4.1. Videofluoroscopic Swallowing Study (VFSS)
4.2. Flexible Endoscopic Evaluation of Swallowing (FEES)
4.3. Electromyography (EMG)
4.3.1. Surface Electromyography (sEMG)
4.3.2. Needle Electrodes
4.4. Pressure
High-Resolution Manometry (HRM)
4.5. Bioimpedance
4.6. Barometric Pressure (BP)
4.7. Accelerometer
4.8. Myotonometer
4.9. Mechanomyography (MMG)
4.10. Cervical Auscultation (Acoustics and Vibration)
4.11. Photoelectric Sensor
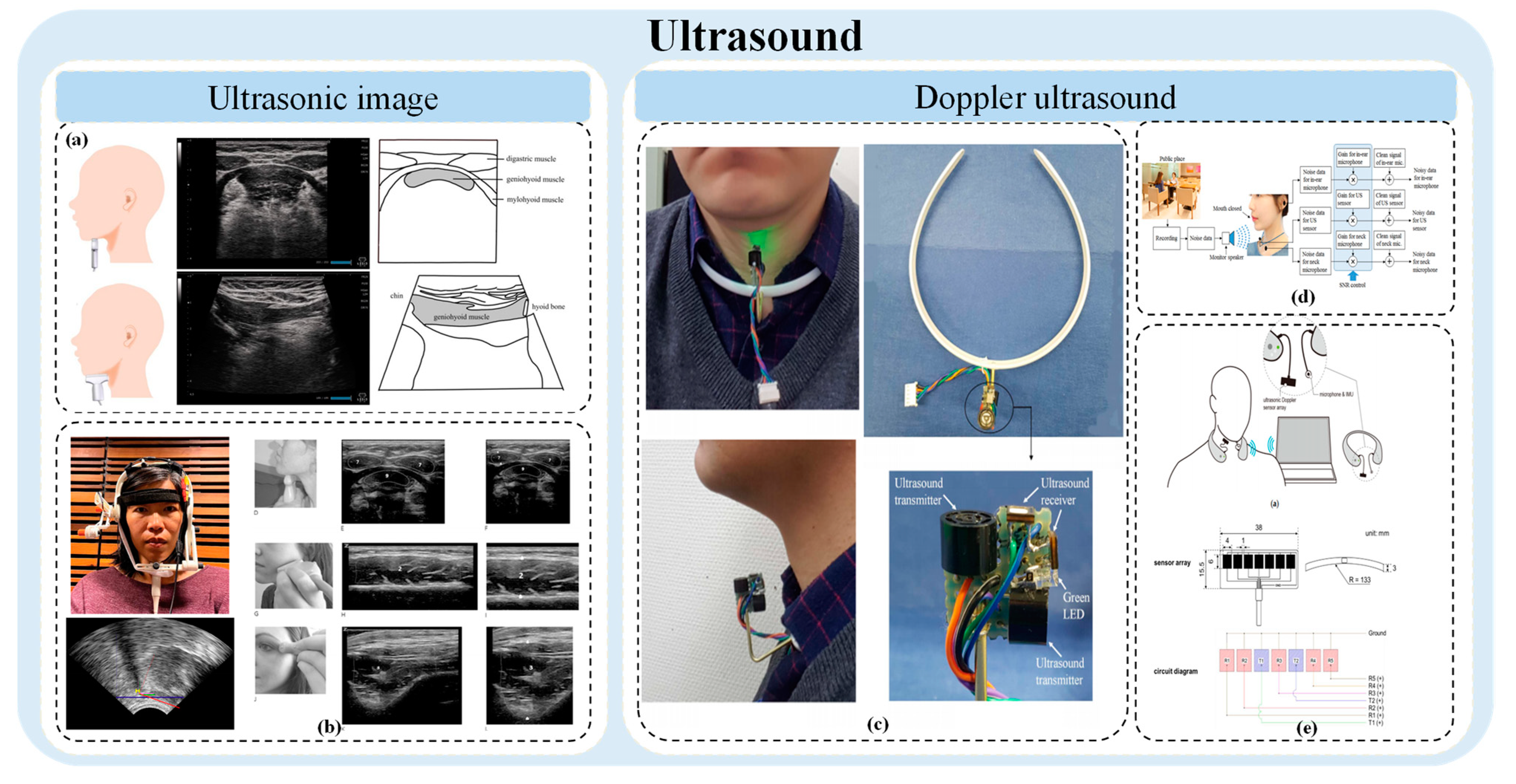
4.12. Ultrasound
4.12.1. Ultrasonic Image
4.12.2. Doppler Ultrasound
4.13. Other Techniques
5. Prospect and Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Adkins, C.; Takakura, W.; Spiegel, B.M.R.; Lu, M.; Vera-Llonch, M.; Williams, J.; Almario, C.V. Prevalence and Characteristics of Dysphagia Based on a Population-Based Survey. Clin. Gastroenterol. Hepatol. 2020, 18, 1970–1979.e2. [Google Scholar] [CrossRef] [PubMed]
- Engh, M.C.N.; Speyer, R. Management of Dysphagia in Nursing Homes: A National Survey. Dysphagia 2021, 37, 266–276. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, H.; Steele, C.; Chau, T. Post-Segmentation Swallowing Accelerometry Signal Trimming and False Positive Reduction. IEEE Signal Process. Lett. 2016, 23, 1221–1225. [Google Scholar] [CrossRef]
- Eslick, G.D.; Talley, N.J. Dysphagia: Epidemiology, risk factors and impact on quality of life--a population-based study. Aliment. Pharmacol. Ther. 2008, 27, 971–979. [Google Scholar] [CrossRef]
- Chiocca, J.C.; Olmos, J.A.; Salis, G.B.; Soifer, L.O.; Higa, R.; Marcolongo, M.; Argentinean Gastro-Oesophageal Reflux Study, G. Prevalence, clinical spectrum and atypical symptoms of gastro-oesophageal reflux in Argentina: A nationwide population-based study. Aliment. Pharmacol. Ther. 2005, 22, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Barczi, S.R.; Sullivan, P.A.; Robbins, J. How should dysphagia care of older adults differ? Establishing optimal practice patterns. Semin. Speech Lang. 2000, 21, 347–361. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.A.; Krishnaswami, S.; Steger, E.; Conover, E.; Vaezi, M.F.; Ciucci, M.R.; Francis, D.O. Economic and survival burden of dysphagia among inpatients in the United States. Dis. Esophagus 2018, 31, dox131. [Google Scholar] [CrossRef]
- Clave, P.; Shaker, R. Dysphagia: Current reality and scope of the problem. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.Y.; Choung, R.S.; Saito, Y.A.; Schleck, C.D.; Zinsmeister, A.R.; Locke, G.R., 3rd; Talley, N.J. Prevalence and risk factors for dysphagia: A USA community study. Neurogastroenterol. Motil. 2015, 27, 212–219. [Google Scholar] [CrossRef]
- Thiyagalingam, S.; Kulinski, A.E.; Thorsteinsdottir, B.; Shindelar, K.L.; Takahashi, P.Y. Dysphagia in Older Adults. Mayo Clin. Proc. 2021, 96, 488–497. [Google Scholar] [CrossRef]
- Allen, J.; Greene, M.; Sabido, I.; Stretton, M.; Miles, A. Economic costs of dysphagia among hospitalized patients. Laryngoscope 2020, 130, 974–979. [Google Scholar] [CrossRef] [PubMed]
- Ekberg, O.; Hamdy, S.; Woisard, V.; Wuttge-Hannig, A.; Ortega, P. Social and psychological burden of dysphagia: Its impact on diagnosis and treatment. Dysphagia 2002, 17, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Warner, H.; Coutinho, J.M.; Young, N. Utilization of Instrumentation in Swallowing Assessment of Surgical Patients during COVID-19. Life 2023, 13, 1471. [Google Scholar] [CrossRef] [PubMed]
- Teramoto, S.; Fukuchi, Y.; Sasaki, H.; Sato, K.; Sekizawa, K.; Matsuse, T.; Japanese Study Group on Aspiration Pulmonary Disease. High incidence of aspiration pneumonia in community- and hospital-acquired pneumonia in hospitalized patients: A multicenter, prospective study in Japan. J. Am. Geriatr. Soc. 2008, 56, 577–579. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, S.; Nakauma, M.; Funami, T.; Hori, K.; Ono, T. Human physiological responses during swallowing of gel-type foods and its correlation with textural perception. Food Hydrocoll. 2021, 111, 106353. [Google Scholar] [CrossRef]
- Christmas, C.; Rogus-Pulia, N. Swallowing Disorders in the Older Population. J. Am. Geriatr. Soc. 2019, 67, 2643–2649. [Google Scholar] [CrossRef]
- Ney, D.M.; Weiss, J.M.; Kind, A.J.; Robbins, J. Senescent swallowing: Impact, strategies, and interventions. Nutr. Clin. Pract. 2009, 24, 395–413. [Google Scholar] [CrossRef] [PubMed]
- Sasegbon, A.; Hamdy, S. The anatomy and physiology of normal and abnormal swallowing in oropharyngeal dysphagia. Neurogastroenterol. Motil. 2017, 29, e13100. [Google Scholar] [CrossRef]
- Murakami, C.; Sasaki, M.; Shimoda, S.; Tamada, Y. Quantification of the Swallowing Mechanism Through Muscle Synergy Analysis. Dysphagia 2023, 38, 973–989. [Google Scholar] [CrossRef]
- Dodds, W.J.; Stewart, E.T.; Logemann, J.A. Physiology and radiology of the normal oral and pharyngeal phases of swallowing. AJR Am. J. Roentgenol. 1990, 154, 953–963. [Google Scholar] [CrossRef]
- Logemann, J. Evaluation and treatment of swallowing disorders. NSSLHA J. 1984, 12, 38–50. [Google Scholar] [CrossRef]
- Matsuo, K.; Palmer, J.B. Anatomy and Physiology of Feeding and Swallowing: Normal and Abnormal. Phys. Med. Rehabil. Clin. N. Am. 2008, 19, 691–707. [Google Scholar] [CrossRef] [PubMed]
- Cook, I.J.; Dodds, W.J.; Dantas, R.O.; Kern, M.K.; Massey, B.T.; Shaker, R.; Hogan, W.J. Timing of videofluoroscopic, manometric events, and bolus transit during the oral and pharyngeal phases of swallowing. Dysphagia 1989, 4, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Kendall, K.A.; McKenzie, S.; Leonard, R.J.; Goncalves, M.I.; Walker, A. Timing of events in normal swallowing: A videofluoroscopic study. Dysphagia 2000, 15, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Martin-Harris, B.; Brodsky, M.B.; Michel, Y.; Ford, C.L.; Walters, B.; Heffner, J. Breathing and swallowing dynamics across the adult lifespan. Arch. Otolaryngol. Head. Neck Surg. 2005, 131, 762–770. [Google Scholar] [CrossRef] [PubMed]
- Martin-Harris, B.; Brodsky, M.B.; Price, C.C.; Michel, Y.; Walters, B. Temporal coordination of pharyngeal and laryngeal dynamics with breathing during swallowing: Single liquid swallows. J. Appl. Physiol. (1985) 2003, 94, 1735–1743. [Google Scholar] [CrossRef] [PubMed]
- Van Daele, D.J.; McCulloch, T.M.; Palmer, P.M.; Langmore, S.E. Timing of glottic closure during swallowing: A combined electromyographic and endoscopic analysis. Ann. Otol. Rhinol. Laryngol. 2005, 114, 478–487. [Google Scholar] [CrossRef] [PubMed]
- Castell, J.A.; Castell, D.O.; Schultz, A.R.; Georgeson, S. Effect of head position on the dynamics of the upper esophageal sphincter and pharynx. Dysphagia 1993, 8, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Shaker, R.; Ren, J.; Podvrsan, B.; Dodds, W.J.; Hogan, W.J.; Kern, M.; Hoffmann, R.; Hintz, J. Effect of aging and bolus variables on pharyngeal and upper esophageal sphincter motor function. Am. J. Physiol. 1993, 264, G427–G432. [Google Scholar] [CrossRef] [PubMed]
- Steele, C.M.; Huckabee, M.L. The influence of orolingual pressure on the timing of pharyngeal pressure events. Dysphagia 2007, 22, 30–36. [Google Scholar] [CrossRef]
- Green, J.R.; Wang, Y.T. Tongue-surface movement patterns during speech and swallowing. J. Acoust. Soc. Am. 2003, 113, 2820–2833. [Google Scholar] [CrossRef] [PubMed]
- Logemann, J.A.; Pauloski, B.R.; Rademaker, A.W.; Colangelo, L.A.; Kahrilas, P.J.; Smith, C.H. Temporal and biomechanical characteristics of oropharyngeal swallow in younger and older men. J. Speech Lang. Hear. Res. 2000, 43, 1264–1274. [Google Scholar] [CrossRef] [PubMed]
- Logemann, J.A.; Pauloski, B.R.; Rademaker, A.W.; Kahrilas, P.J. Oropharyngeal swallow in younger and older women: Videofluoroscopic analysis. J. Speech Lang. Hear. Res. 2002, 45, 434–445. [Google Scholar] [CrossRef]
- Burkhead, L.M.; Sapienza, C.M.; Rosenbek, J.C. Strength-training exercise in dysphagia rehabilitation: Principles, procedures, and directions for future research. Dysphagia 2007, 22, 251–265. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, C.; Logemann, J.A.; Pauloski, B.R.; Rademaker, A.W.; Helenowski, I.B.; Vonesh, E.F.; Maccracken, E.; Mittal, B.B.; Vokes, E.E.; Haraf, D.J. Effects of radiotherapy with or without chemotherapy on tongue strength and swallowing in patients with oral cancer. Head Neck 2007, 29, 632–637. [Google Scholar] [CrossRef] [PubMed]
- Daniels, S.K.; Schroeder, M.F.; DeGeorge, P.C.; Corey, D.M.; Rosenbek, J.C. Effects of verbal cue on bolus flow during swallowing. Am. J. Speech Lang. Pathol. 2007, 16, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Johnsson, F.; Shaw, D.; Gabb, M.; Dent, J.; Cook, I. Influence of gravity and body position on normal oropharyngeal swallowing. Am. J. Physiol. 1995, 269, G653–G658. [Google Scholar] [CrossRef] [PubMed]
- McConnel, F.M.S.; Guffin, T.N.; Cerenko, D.; Ko, A.S.F. The effects of Bolus Flow on Vertical Pharyngeal Pressure Measurement in the Pharyngoesophageal Segment: Clinical Significance. Otolaryngol.–Head Neck Surg. 1992, 106, 169–174. [Google Scholar] [CrossRef]
- Leow, L.P.; Huckabee, M.L.; Sharma, S.; Tooley, T.P. The influence of taste on swallowing apnea, oral preparation time, and duration and amplitude of submental muscle contraction. Chem. Senses 2007, 32, 119–128. [Google Scholar] [CrossRef]
- Pelletier, C.A.; Dhanaraj, G.E. The effect of taste and palatability on lingual swallowing pressure. Dysphagia 2006, 21, 121–128. [Google Scholar] [CrossRef]
- Kohyama, K.; Ohtsubo, K.; Toyoshima, H.; Shiozawa, K. Electromyographic Study on Cooked Rice with Different Amylose Contents. J. Texture Stud. 2007, 29, 101–113. [Google Scholar] [CrossRef]
- Furuya, J.; Nakamura, S.; Ono, T.; Suzuki, T. Tongue pressure production while swallowing water and pudding and during dry swallow using a sensor sheet system. J. Oral. Rehabil. 2012, 39, 684–691. [Google Scholar] [CrossRef] [PubMed]
- Kohyama, K.; Sasaki, T.; Dan, H. Active stress during compression testing of various foods measured using a multiple-point sheet sensor. Biosci. Biotechnol. Biochem. 2003, 67, 1492–1498. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, S.; Nakauma, M.; Funami, T.; Odake, S.; Nishinari, K. Swallowing profiles of food polysaccharide gels in relation to bolus rheology. Food Hydrocoll. 2011, 25, 1016–1024. [Google Scholar] [CrossRef]
- Hasegawa, A.T.; Otoguro, A.K.; Kumagai, H.I.; Nakazawa, F.U. Velocity of swallowed gel food in the pharynx by ultrasonic method. J. Jpn. Soc. Food Sci. Technol. 2005, 52, 441–447. [Google Scholar] [CrossRef]
- Vaitheeshwari, R.; Yeh, S.-C.; Wu, E.H.-K.; Lin, F.-A. The Swallowing Intelligent Assessment System Based on Tongue Strength and Surface EMG. IEEE Sens. J. 2023, 23, 17310–17318. [Google Scholar] [CrossRef]
- Martin-Harris, B.; Jones, B. The videofluorographic swallowing study. Phys. Med. Rehabil. Clin. N. Am. 2008, 19, 769–785. [Google Scholar] [CrossRef] [PubMed]
- Park, D.; Lee, H.H.; Lee, S.T.; Oh, Y.; Lee, J.C.; Nam, K.W.; Ryu, J.S. Normal contractile algorithm of swallowing related muscles revealed by needle EMG and its comparison to videofluoroscopic swallowing study and high resolution manometry studies: A preliminary study. J. Electromyogr. Kinesiol. 2017, 36, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.J.; Wang, C.C.; Lin, F.Y.; Tseng, K.Y.; Hwu, Y.J. Analysis of Labial and Lingual Strength among Healthy Chinese Adults in Taiwan. Int. J. Environ. Res. Public Health 2020, 17, 7904. [Google Scholar] [CrossRef]
- Jeong, D.M.; Shin, Y.J.; Lee, N.R.; Lim, H.K.; Choung, H.W.; Pang, K.M.; Kim, B.J.; Kim, S.M.; Lee, J.H. Maximal strength and endurance scores of the tongue, lip, and cheek in healthy, normal Koreans. J. Korean Assoc. Oral. Maxillofac. Surg. 2017, 43, 221–228. [Google Scholar] [CrossRef]
- Saraee, E.; Gu, Y.; Pandit, S.; Tran, S.; Shandelman, E.; Singh, S.; Nordahl, T.J.; Ellis, T.; Betke, M. ExerciseCheck. In Proceedings of the 12th ACM International Conference on PErvasive Technologies Related to Assistive Environments, Rhodes, Greece, 5–7 June 2019; pp. 110–118. [Google Scholar]
- Roldan-Vasco, S.; Orozco-Duque, A.; Orozco-Arroyave, J.R. Swallowing disorders analysis using surface EMG biomarkers and classification models. Digit. Signal Process. 2023, 133, 103815. [Google Scholar] [CrossRef]
- Pisegna, J.M.; Murray, J. Clinical Application of Flexible Endoscopic Evaluation of Swallowing in Stroke. Semin. Speech Lang. 2018, 39, 3–14. [Google Scholar] [CrossRef]
- Butler, S.G.; Stuart, A.; Kemp, S. Flexible endoscopic evaluation of swallowing in healthy young and older adults. Ann. Otol. Rhinol. Laryngol. 2009, 118, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Butler, S.G.; Markley, L.; Sanders, B.; Stuart, A. Reliability of the penetration aspiration scale with flexible endoscopic evaluation of swallowing. Ann. Otol. Rhinol. Laryngol. 2015, 124, 480–483. [Google Scholar] [CrossRef] [PubMed]
- Zang, J.; Kiehn, S.; Flugel, T.; Koseki, J.C.; Niessen, A.; Kim, S.H.; Pflug, C.; Nienstedt, J.C. Implementation of Pediatric Flexible-Endoscopic Evaluation of Swallowing: A Systematic Review and Recommendations for Future Research. Dysphagia 2022, 37, 1822–1838. [Google Scholar] [CrossRef]
- Curtis, J.A. A Scoping Review and Tutorial for Developing Standardized and Transparent Protocols for Flexible Endoscopic Evaluation of Swallowing. Perspect. ASHA Spec. Interest Groups 2022, 7, 1960–1971. [Google Scholar] [CrossRef]
- McKeown, M.J.; Torpey, D.C.; Gehm, W.C. Non-invasive monitoring of functionally distinct muscle activations during swallowing. Clin. Neurophysiol. 2002, 113, 354–366. [Google Scholar] [CrossRef] [PubMed]
- Restrepo-Agudelo, S.; Roldan-Vasco, S.; Ramirez-Arbelaez, L.; Cadavid-Arboleda, S.; Perez-Giraldo, E.; Orozco-Duque, A. Improving surface EMG burst detection in infrahyoid muscles during swallowing using digital filters and discrete wavelet analysis. J. Electromyogr. Kinesiol. 2017, 35, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Zaretsky, E.; Pluschinski, P.; Sader, R.; Birkholz, P.; Neuschaefer-Rube, C.; Hey, C. Identification of the most significant electrode positions in electromyographic evaluation of swallowing-related movements in humans. Eur. Arch. Oto-Rhino-Laryngol. 2016, 274, 989–995. [Google Scholar] [CrossRef]
- Zhu, M.; Yu, B.; Yang, W.; Jiang, Y.; Lu, L.; Huang, Z.; Chen, S.; Li, G. Evaluation of normal swallowing functions by using dynamic high-density surface electromyography maps. BioMed. Eng. OnLine 2017, 16, 133. [Google Scholar] [CrossRef]
- Li, Q.; Minagi, Y.; Ono, T.; Chen, Y.; Hori, K.; Fujiwara, S.; Maeda, Y. The biomechanical coordination during oropharyngeal swallowing: An evaluation with a non-invasive sensing system. Sci. Rep. 2017, 7, 15165. [Google Scholar] [CrossRef]
- Shieh, W.Y.; Wang, C.M.; Cheng, H.K.; Wang, C.H. Using Wearable and Non-Invasive Sensors to Measure Swallowing Function: Detection, Verification, and Clinical Application. Sensors 2019, 19, 2624. [Google Scholar] [CrossRef]
- Krishnan, G.; Goswami, S.P. The Effect of Chin-Down Position and Bolus Volume on Swallow-Induced Respiratory Measures in Young Healthy Adults. SN Compr. Clin. Med. 2019, 1, 981–991. [Google Scholar] [CrossRef]
- Takeuchi, C.; Takei, E.; Ito, K.; Kulvanich, S.; Magara, J.; Tsujimura, T.; Inoue, M. Effects of Carbonation and Temperature on Voluntary Swallowing in Healthy Humans. Dysphagia 2021, 36, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Endo, H.; Ohmori, N.; Chikai, M.; Miwa, H.; Ino, S. Effects of age and gender on swallowing activity assessed by electromyography and laryngeal elevation. J. Oral. Rehabil. 2020, 47, 1358–1367. [Google Scholar] [CrossRef] [PubMed]
- Ofusa, W.; Yamada, Y.; Ishida, R.; Ohkubo, M.; Higashikawa, A.; Kimura, M.; Shibukawa, Y. Use of barometric pressure and electromyography measurement techniques to elucidate the mechanisms by which bolus passes from the oral cavity to the oropharynx during swallowing. Physiol. Behav. 2020, 226, 113115. [Google Scholar] [CrossRef]
- McNulty, J.; de Jager, K.; Lancashire, H.T.; Graveston, J.; Birchall, M.; Vanhoestenberghe, A. Prediction of larynx function using multichannel surface EMG classification. IEEE Trans. Med. Robot. Bionics 2021, 3, 1032–1039. [Google Scholar] [CrossRef] [PubMed]
- Ko, J.Y.; Kim, H.; Jang, J.; Lee, J.C.; Ryu, J.S. Electromyographic activation patterns during swallowing in older adults. Sci. Rep. 2021, 11, 5795. [Google Scholar] [CrossRef]
- Archer, S.K.; Smith, C.H.; Newham, D.J. Surface Electromyographic Biofeedback and the Effortful Swallow Exercise for Stroke-Related Dysphagia and in Healthy Ageing. Dysphagia 2021, 36, 281–292. [Google Scholar] [CrossRef]
- Vacchiano, V.; Di Stasi, V.; Rizzo, G.; Giannoccaro, M.P.; Donadio, V.; Bartolomei, I.; Capellari, S.; Salvi, F.; Avoni, P.; Liguori, R. Prognostic value of EMG genioglossus involvement in amyotrophic lateral sclerosis. Clin. Neurophysiol. 2021, 132, 2416–2421. [Google Scholar] [CrossRef]
- Nicholls, B.; Ang, C.S.; Kanjo, E.; Siriaraya, P.; Mirzaee Bafti, S.; Yeo, W.H.; Tsanas, A. An EMG-based Eating Behaviour Monitoring system with haptic feedback to promote mindful eating. Comput. Biol. Med. 2022, 149, 106068. [Google Scholar] [CrossRef] [PubMed]
- Bahia, M.M.; Lowell, S.Y. Surface Electromyographic Activity of the Masseter Muscle During Regular and Effortful Saliva Swallows: A Preliminary Study. Dysphagia 2024, 39, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Rong, P.; Pattee, G.L. A multidimensional facial surface EMG analysis for objective assessment of bulbar involvement in amyotrophic lateral sclerosis. Clin. Neurophysiol. 2022, 135, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.H.; Chen, M.H.; Liu, J.F.; Chung, W.L.; Chiu, L.L.; Huang, Y.F. Surface Electromyography for Evaluating the Effect of Aging on the Coordination of Swallowing Muscles. Dysphagia 2023, 38, 1430–1439. [Google Scholar] [CrossRef] [PubMed]
- Saito, N.; Ogawa, T.; Shiraishi, N.; Koide, R.; Komine, H.; Yokoyama, M.; Hanawa, S.; Sasaki, K. Difference in the Electromyographic Behavior of the Masticatory and Swallowing Muscles During Cued Versus Spontaneous Swallowing. Dysphagia 2023, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.H.; Pauloski, B.R. Ultrasonography as Biofeedback to Increase Muscle Activation During the Mendelsohn Maneuver in Healthy Adults. Dysphagia 2023, 38, 1156–1168. [Google Scholar] [CrossRef]
- Roldan-Vasco, S.; Restrepo-Uribe, J.P.; Orozco-Duque, A.; Suarez-Escudero, J.C.; Orozco-Arroyave, J.R. Analysis of electrophysiological and mechanical dimensions of swallowing by non-invasive biosignals. Biomed. Signal Process. Control 2023, 82, 104533. [Google Scholar] [CrossRef]
- Alfonsi, E.; Todisco, M.; Fresia, M.; Tassorelli, C.; Cosentino, G. Electrokinesiographic Study of Oropharyngeal Swallowing in Neurogenic Dysphagia. Dysphagia 2023, 38, 543–557. [Google Scholar] [CrossRef]
- Mialland, A.; Atallah, I.; Bonvilain, A. Stylohyoid and Posterior Digastric Recruitment Pattern Evaluation in Swallowing and Non-swallowing Tasks. IRBM 2024, 45, 100823. [Google Scholar] [CrossRef]
- Sukthankar, S.M.; Reddy, N.P.; Canilang, E.P.; Stephenson, L.; Thomas, R. Design and development of portable biofeedback systems for use in oral dysphagia rehabilitation. Med. Eng. Phys. 1994, 16, 430–435. [Google Scholar] [CrossRef]
- Huckabee, M.L.; Cannito, M.P. Outcomes of swallowing rehabilitation in chronic brainstem dysphagia: A retrospective evaluation. Dysphagia 1999, 14, 93–109. [Google Scholar] [CrossRef] [PubMed]
- Alfonsi, E.; Bergamaschi, R.; Cosentino, G.; Ponzio, M.; Montomoli, C.; Restivo, D.A.; Brighina, F.; Ravaglia, S.; Prunetti, P.; Bertino, G.; et al. Electrophysiological patterns of oropharyngeal swallowing in multiple sclerosis. Clin. Neurophysiol. 2013, 124, 1638–1645. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, G.; Tassorelli, C.; Prunetti, P.; Todisco, M.; De Icco, R.; Avenali, M.; Minafra, B.; Zangaglia, R.; Valentino, F.; Pacchetti, C.; et al. Reproducibility and reaction time of swallowing as markers of dysphagia in parkinsonian syndromes. Clin. Neurophysiol. 2020, 131, 2200–2208. [Google Scholar] [CrossRef] [PubMed]
- Kohyama, K.; Hayakawa, F.; Kazami, Y.; Ishihara, S.; Nakao, S.; Funami, T.; Nishinari, K. Electromyographic texture characterization of hydrocolloid gels as model foods with varying mastication and swallowing difficulties. Food Hydrocoll. 2015, 43, 146–152. [Google Scholar] [CrossRef]
- Rafeedi, T.; Abdal, A.; Polat, B.; Hutcheson, K.A.; Shinn, E.H.; Lipomi, D.J. Wearable, epidermal devices for assessment of swallowing function. NPJ Flex. Electron. 2023, 7, 52. [Google Scholar] [CrossRef]
- Ohmori, N.; Watanabe, S.; Momose, H.; Endo, H.; Chikai, M.; Ino, S. Investigation of variation factors in EMG measurement of swallowing: Instruction can improve EMG reproducibility. Med. Biol. Eng. Comput. 2022, 60, 2825–2840. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Valdes, E.; Laine, C.M.; Falla, D.; Mayer, F.; Farina, D. High-density surface electromyography provides reliable estimates of motor unit behavior. Clin. Neurophysiol. 2016, 127, 2534–2541. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Valdes, E.; Negro, F.; Laine, C.M.; Falla, D.; Mayer, F.; Farina, D. Tracking motor units longitudinally across experimental sessions with high-density surface electromyography. J. Physiol. 2017, 595, 1479–1496. [Google Scholar] [CrossRef]
- Zhang, D.; Chen, Z.; Xiao, L.; Zhu, B.; Wu, R.; Ou, C.; Ma, Y.; Xie, L.; Jiang, H. Stretchable and durable HD-sEMG electrodes for accurate recognition of swallowing activities on complex epidermal surfaces. Microsyst. Nanoeng. 2023, 9, 115. [Google Scholar] [CrossRef]
- Zhao, N.; Yang, H.-J.; Shen, G.-C.; Wang, Z.-Z.; Jiang, C.-P.; Yang, B.; Liu, J.-Q. A MEMS-Based Wearable, Flexible Embedded High-Density Sensor With Self-Adhesive PEDOT:PSS Gel for HD-sEMG Monitoring. IEEE Sens. J. 2023, 23, 11016–11024. [Google Scholar] [CrossRef]
- Wang, Y.; Yin, L.; Bai, Y.; Liu, S.; Wang, L.; Zhou, Y.; Hou, C.; Yang, Z.; Wu, H.; Ma, J.; et al. Electrically compensated, tattoo-like electrodes for epidermal electrophysiology at scale. Sci. Adv. 2020, 6, eabd0996. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.; Wang, W.; Zhang, Q. Your Glasses Know Your Diet: Dietary Monitoring Using Electromyography Sensors. IEEE Internet Things J. 2017, 4, 705–712. [Google Scholar] [CrossRef]
- Zhang, R.; Amft, O. Monitoring Chewing and Eating in Free-Living Using Smart Eyeglasses. IEEE J. Biomed. Health Inf. 2018, 22, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Polat, B.; Becerra, L.L.; Hsu, P.-Y.; Kaipu, V.; Mercier, P.P.; Cheng, C.-K.; Lipomi, D.J. Epidermal Graphene Sensors and Machine Learning for Estimating Swallowed Volume. ACS Appl. Nano Mater. 2021, 4, 8126–8134. [Google Scholar] [CrossRef]
- Ramirez, J.; Rodriquez, D.; Qiao, F.; Warchall, J.; Rye, J.; Aklile, E.; Chiang, S.C.A.; Marin, B.C.; Mercier, P.P.; Cheng, C.K.; et al. Metallic Nanoislands on Graphene for Monitoring Swallowing Activity in Head and Neck Cancer Patients. ACS Nano 2018, 12, 5913–5922. [Google Scholar] [CrossRef] [PubMed]
- Burgin, C.; Simmen, P.; Gupta, N.; Suter, L.; Kreuzer, S.; Haeberlin, A.; Schulzke, S.M.; Trachsel, D.; Niederhauser, T.; Jost, K. Multichannel esophageal signals to monitor respiratory rate in preterm infants. Pediatr. Res. 2022, 91, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Katirji, M.B. Electrodiagnosis in Diseases of Nerve and Muscle. Neurology 1990, 40, 869. [Google Scholar] [CrossRef]
- Mu, L.C.; Yang, S.L. A new method of needle-electrode placement in the posterior cricoarytenoid muscle for electromyography. Laryngoscope 1990, 100, 1127–1131. [Google Scholar] [CrossRef]
- Ertekin, C.; Kiylioglu, N.; Tarlaci, S.; Keskin, A.; Aydogdu, I. Effect of mucosal anaesthesia on oropharyngeal swallowing. Neurogastroenterol. Motil. 2000, 12, 567–572. [Google Scholar] [CrossRef]
- Regan, J. Impact of Sensory Stimulation on Pharyngo-esophageal Swallowing Biomechanics in Adults with Dysphagia: A High-Resolution Manometry Study. Dysphagia 2020, 35, 825–833. [Google Scholar] [CrossRef]
- Heslin, N.; Regan, J. Effect of effortful swallow on pharyngeal pressures during swallowing in adults with dysphagia: A pharyngeal high-resolution manometry study. Int. J. Speech Lang. Pathol. 2022, 24, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Mielens, J.D.; Hoffman, M.R.; Ciucci, M.R.; Jiang, J.J.; McCulloch, T.M. Automated analysis of pharyngeal pressure data obtained with high-resolution manometry. Dysphagia 2011, 26, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Kreiser, J.; Hann, A.; Zizer, E.; Ropinski, T. Decision Graph Embedding for High-Resolution Manometry Diagnosis. IEEE Trans. Vis. Comput. Graph. 2018, 24, 873–882. [Google Scholar] [CrossRef] [PubMed]
- Colevas, S.M.; Stalter, L.N.; Jones, C.A.; McCulloch, T.M. The Natural Swallow: Factors Affecting Subject Choice of Bolus Volume and Pharyngeal Swallow Parameters in a Self-selected Swallow. Dysphagia 2022, 37, 1172–1182. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Koyama, S.; Kimura, Y.; Ishiyama, D.; Ohji, S.; Otobe, Y.; Nishio, N.; Kunieda, Y.; Ichikawa, T.; Ito, D.; et al. Relationship between tongue muscle quality and swallowing speed in community-dwelling older women. Aging Clin. Exp. Res. 2020, 32, 2073–2079. [Google Scholar] [CrossRef] [PubMed]
- Natta, L.; Guido, F.; Algieri, L.; Mastronardi, V.M.; Rizzi, F.; Scarpa, E.; Qualtieri, A.; Todaro, M.T.; Sallustio, V.; De Vittorio, M. Conformable AlN Piezoelectric Sensors as a Non-invasive Approach for Swallowing Disorder Assessment. ACS Sens. 2021, 6, 1761–1769. [Google Scholar] [CrossRef] [PubMed]
- Maeda, M.; Kadokura, M.; Aoki, R.; Kawakami, M.; Koyama, Y.; Nishiyama, M.; Watanabe, K. Non-invasive swallowing examination device using hetero-core fiber optic pressure sensor. In Proceedings of the 2021 IEEE 3rd Global Conference on Life Sciences and Technologies (LifeTech), Nara, Japan, 9–11 March 2021; pp. 315–316. [Google Scholar]
- Maeda, M.; Kadokura, M.; Aoki, R.; Komatsu, N.; Kawakami, M.; Koyama, Y.; Watanabe, K.; Nishiyama, M. A Fiber-Optic Non-Invasive Swallowing Assessment Device Based on a Wearable Pressure Sensor. Sensors 2023, 23, 2355. [Google Scholar] [CrossRef] [PubMed]
- Ohashi, M.; Aoyagi, Y.; Ito, S.; Kagaya, H.; Hirata, M.; Nakata, S. Comparison of electromyography, sound, bioimpedance, and high-resolution manometry for differentiating swallowing and vocalization events. Med. Eng. Phys. 2023, 115, 103980. [Google Scholar] [CrossRef] [PubMed]
- Hubl, N.; Riebold, B.; Schramm, D.; Seidl, R.O. Differences in the swallowing process of newborns and healthy preterm infants: First results with a non-invasive bioimpedance and electromyography measurement system. Eur. Arch. Otorhinolaryngol. 2024, 281, 843–854. [Google Scholar] [CrossRef]
- Rosero Salazar, D.H.; Honnlee, S.; Liu, Z.J. Tongue, palatal, hyoid and pharyngeal muscle activity during chewing, swallowing, and respiration. Arch. Oral. Biol. 2024, 157, 105845. [Google Scholar] [CrossRef]
- Sejdic, E.; Steele, C.M.; Chau, T. Classification of Penetration--Aspiration Versus Healthy Swallows Using Dual-Axis Swallowing Accelerometry Signals in Dysphagic Subjects. IEEE Trans. Biomed. Eng. 2013, 60, 1859–1866. [Google Scholar] [CrossRef]
- Movahedi, F.; Kurosu, A.; Coyle, J.L.; Perera, S.; Sejdic, E. Anatomical Directional Dissimilarities in Tri-axial Swallowing Accelerometry Signals. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 447–458. [Google Scholar] [CrossRef]
- Lee, K.; Ni, X.; Lee, J.Y.; Arafa, H.; Pe, D.J.; Xu, S.; Avila, R.; Irie, M.; Lee, J.H.; Easterlin, R.L.; et al. Mechano-acoustic sensing of physiological processes and body motions via a soft wireless device placed at the suprasternal notch. Nat. Biomed. Eng. 2020, 4, 148–158. [Google Scholar] [CrossRef]
- Xu, H.; Zheng, W.; Zhang, Y.; Zhao, D.; Wang, L.; Zhao, Y.; Wang, W.; Yuan, Y.; Zhang, J.; Huo, Z.; et al. A fully integrated, standalone stretchable device platform with in-sensor adaptive machine learning for rehabilitation. Nat. Commun. 2023, 14, 7769. [Google Scholar] [CrossRef] [PubMed]
- Maden, T.; Usgu, G.; Tuncer, A. Myotonometric comparison of sternocleidomastoideus and masseter muscles in multiple sclerosis patients with swallowing problem and healthy individuals. Mult. Scler. Relat. Disord. 2022, 57, 103387. [Google Scholar] [CrossRef]
- Fukuhara, S.; Ikeno, M.; Oka, H. Basic Characteristics of Submental Mechanomyography and Electromyography Measured Simultaneously During Tongue Lift Using a Novel Muscle Function Measurement Device. J. Med. Biol. Eng. 2023, 43, 612–622. [Google Scholar] [CrossRef]
- Mialland, A.; Kinsiklounon, B.; Tian, G.; Noûs, C.; Bonvilain, A. Submental MechanoMyoGraphy (MMG) to Characterize the Swallowing Signature. IRBM 2022, 43, 414–421. [Google Scholar] [CrossRef]
- He, F.; Hu, X.; Zhu, C.; Li, Y.; Liu, Y. Multi-Scale Spatial and Temporal Speech Associations to Swallowing for Dysphagia Screening. IEEE/ACM Trans. Audio Speech Lang. Process. 2022, 30, 2888–2899. [Google Scholar] [CrossRef]
- Shirazi, S.S.; Moussavi, Z.M. Acoustical modeling of swallowing mechanism. IEEE Trans. Biomed. Eng. 2011, 58, 81–87. [Google Scholar] [CrossRef]
- Dudik, J.M.; Coyle, J.L.; Sejdic, E. Dysphagia Screening: Contributions of Cervical Auscultation Signals and Modern Signal-Processing Techniques. IEEE Trans. Hum. Mach. Syst. 2015, 45, 465–477. [Google Scholar] [CrossRef] [PubMed]
- Donohue, C.; Khalifa, Y.; Perera, S.; Sejdić, E.; Coyle, J.L. Characterizing Effortful Swallows from Healthy Community Dwelling Adults Across the Lifespan Using High-Resolution Cervical Auscultation Signals and MBSImP Scores: A Preliminary Study. Dysphagia 2021, 37, 1103–1111. [Google Scholar] [CrossRef] [PubMed]
- Khalifa, Y.; Donohue, C.; Coyle, J.L.; Sejdic, E. Upper Esophageal Sphincter Opening Segmentation With Convolutional Recurrent Neural Networks in High Resolution Cervical Auscultation. IEEE J. Biomed. Health Inf. 2021, 25, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, R.; Khalifa, Y.; Lucatorto, E.; Perera, S.; Coyle, J.; Sejdic, E. A Preliminary Investigation of Similarities of High Resolution Cervical Auscultation Signals Between Thin Liquid Barium and Water Swallows. IEEE J. Transl. Eng. Health Med. 2022, 10, 4900109. [Google Scholar] [CrossRef] [PubMed]
- He, Q.; Perera, S.; Khalifa, Y.; Zhang, Z.; Mahoney, A.S.; Sabry, A.; Donohue, C.; Coyle, J.L.; Sejdic, E. The Association of High Resolution Cervical Auscultation Signal Features With Hyoid Bone Displacement During Swallowing. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 1810–1816. [Google Scholar] [CrossRef]
- Shu, K.; Mao, S.; Coyle, J.L.; Sejdic, E. Improving Non-Invasive Aspiration Detection With Auxiliary Classifier Wasserstein Generative Adversarial Networks. IEEE J. Biomed. Health Inf. 2022, 26, 1263–1272. [Google Scholar] [CrossRef] [PubMed]
- Wagner, C.; Stappenbeck, L.; Wenzel, H.; Steiner, P.; Lehnert, B.; Birkholz, P. Evaluation of a Non-Personalized Optopalatographic Device for Prospective Use in Functional Post-Stroke Dysphagia Therapy. IEEE Trans. Biomed. Eng. 2022, 69, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Yoshimoto, T.; Taniguchi, K.; Kurose, S.; Kimura, Y. Validation of Earphone-Type Sensors for Non-Invasive and Objective Swallowing Function Assessment. Sensors 2022, 22, 5176. [Google Scholar] [CrossRef]
- Van Den Engel-Hoek, L.; Lagarde, M.; Van Alfen, N. Ultrasound of oral and masticatory muscles: Why every neuromuscular swallow team should have an ultrasound machine. Clin. Anat. 2017, 30, 183–193. [Google Scholar] [CrossRef]
- Ma, J.K.Y.; Wrench, A.A. Automated assessment of hyoid movement during normal swallow using ultrasound. Int. J. Lang. Commun. Disord. 2022, 57, 615–629. [Google Scholar] [CrossRef]
- Maeda, K.; Nagasaka, M.; Nagano, A.; Nagami, S.; Hashimoto, K.; Kamiya, M.; Masuda, Y.; Ozaki, K.; Kawamura, K. Ultrasonography for Eating and Swallowing Assessment: A Narrative Review of Integrated Insights for Noninvasive Clinical Practice. Nutrients 2023, 15, 3560. [Google Scholar] [CrossRef]
- Lee, K.-S. Joint Audio-Ultrasound Food Recognition for Noisy Environments. IEEE J. Biomed. Health Inform. 2020, 24, 1477–1489. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.-S. Food Intake Detection Using Ultrasonic Doppler Sonar. IEEE Sens. J. 2017, 17, 6056–6068. [Google Scholar] [CrossRef]
- Chesney, N.; Khwaounjoo, P.; Huckabee, M.L.; Cakmak, Y.O. Non-Contact Assessment of Swallowing Dysfunction Using Smartphone Captured Skin Displacements. Sensors 2023, 23, 5392. [Google Scholar] [CrossRef]
- Sakai, K.; Gilmour, S.; Hoshino, E.; Nakayama, E.; Momosaki, R.; Sakata, N.; Yoneoka, D. A Machine Learning-Based Screening Test for Sarcopenic Dysphagia Using Image Recognition. Nutrients 2021, 13, 4009. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sensing Modality | Author | Year |
EMG Sensor Location |
Human Subject | Research Purpose |
|---|---|---|---|---|---|
| sEMG | Sebastian Restrepo-Agudelo, Sebastian Roldan-Vasco et al. [59] | 2017 | Laryngeal girdle muscle area (subcervical) | 10 healthy adults | To improve the sEMG detection of infrahyoid muscle during swallowing using digital filtering and discrete wavelet analysis. |
| sEMG | E. Zaretsky, P. Pluschinski, R. Sader et al. [60] | 2017 | In the M. masseter, orbicularis oris, submental, and paralaryngeal regions | 16 healthy subjects | Identify the most significant electrode locations associated with oropharyngeal swallowing activity. |
| HD sEMG | Mingxing Zhu, Bin Yu et al. [61] | 2017 | 96 electrodes in the anterior upper neck | 12 healthy subjects | A new technique based on high-density surface electromyography (HD sEMG) is proposed for the assessment of normal swallowing function. |
| Kinematic analysis, HRM, and needle electromyography | Donghwi Park, Hyun Haeng Lee et al. [48] | 2017 | The superior and inferior hyoid muscles | 10 healthy subjects | To investigate the function and importance of the inferior and superior hyoid muscles in the process of swallowing, and to study the swallowing sequence using kinematic analysis, HRM and EMG. |
| Pressure sensors, bending sensors, sEMG, and microphones | Qiang Li, Yoshitomo Minagi et al. [62] | 2017 | Maxillary and mandibular muscles | 15 adult male subjects without any signs of severe malocclusion | Biomechanical coordination during oropharyngeal swallowing was evaluated based on a non-invasive sensing system. |
| sEMG, nasal airflow sensor, and pressure sensing resistance sensor | Wann-Yun Shieh, Chin-Man Wang et al. [63] | 2019 | Mandibular muscle | 45 male participants aged 30–50 years. 26 non-smokers and 19 smokers | A study assessing the coordination between swallowing and breathing was carried out using the proposed detection procedure. |
| SEMG, nasal airflow, and swallowing sounds | Gayathri Krishnan, And S. P. Goswami [64] | 2019 | The inferior submental muscle of the mandible | 30 healthy young volunteers | To study the effects of prone position and gavage volume on swallowing and breathing in healthy young people. |
| sEMG | Chikako Takeuchi, Eri Takei et al. [65] | 2020 | Masticatory muscle and sublingual muscle | 29 healthy volunteers | To investigate how swallowing behavior is affected by water temperature and water bubble content in healthy people. |
| sEMG and pressure sensor | Hiroshi Endo, Nobuyuki Ohmori et al. [66] | 2020 | Mandibular muscle and maxillary muscle | 60 healthy volunteers (divided into 2 age groups: young and old) | To investigate the relationship between the temporal characteristics of muscle activity and laryngeal uplift (LE) during swallowing. |
| Barometric sensor and EMG | Wataru Ofusa, Yoshiaki Yamada et al. [67] | 2020 | The anterior part of the tongue (TA) and the posterior part of the tongue (TP), as well as the superior pharyngeal constrictor muscle (SHy). | 10 healthy volunteers | By recording pressure (BP) and tongue muscle activity, swallowing organs in the mouth and throat swallowing phase of activity time. |
| sEMG | Johnny McNulty, Kylie de Jager et al. [68] | 2021 | Submandibular muscles, intercostal muscles, and diaphragmatic muscles | 10 participants (5 total laryngectomy (TL), 5 control) | Prediction of laryngeal function by multichannel sEMG classification. |
| sEMG | JinYoung Ko, Hayoung Kim, Joonyoung Jang, Jun Chang Lee & Ju Seok Ryu [69] | 2021 | 6 channel surface electrodes were placed on the bilateral suprahyoid muscle (SH), bilateral retro-hyoid muscle (RH), thyrohyoid muscle (TH), and thyrosternal muscle (StH) | 40 healthy participants (20 older adults older than 60 years and 20 younger adults younger than 60 years) | To study the activation pattern of electromyography during swallowing in the elderly. |
| sEMG | Sally K. Archer, Christina H. Smith, Di J. Newham [70] | 2021 | Submentalis | 15 people with dysphagia less than 3 months after stroke and 85 healthy participants | Determine whether age or dysphagia after stroke affects increased submental muscle activity during dysphagia, whether sEMG biofeedback improves the performance of dysphagia, and whether the patient receives sEMG as a supplement to treatment. |
| EMG | Veria Vacchiano, Vitantonio Di Stasi et al. [71] | 2021 | Masticatory muscle and hyoid muscle | 103 people with ALS | To develop a multidimensional facial sEMG analysis for assessing bulbar involvement in amyotrophic lateral sclerosis (ALS). |
| sEMG | Ben Nicholls, Chee Siang Ang et al. [72] | 2022 | Masticatory muscles | 16 participants | To develop an EMG-based eating behavior monitoring system with haptic feedback to facilitate mindful eating. |
| sEMG | Mariana M. Bahia, Soren Y. Lowell [73] | 2022 | M. masseter | 20 healthy young adults | To study the sEMG changes in masseter muscle during regular and forced swallowing of saliva. |
| sEMG | Martin J. McKeown, Dana C. Torpey, Wendy C. Gehm [58] | 2022 | 15 electrodes in the face and throat | 7 healthy subjects | A novel approach based on computing independent components (ICs) of simultaneous sEMG recordings to detect potentially functional muscle activation during swallowing using only sEMG electrodes is described. |
| sEMG | Panying Rong, Gary L. Pattee [74] | 2022 | The stomatognathic, temporalis, and mandibular abdominis muscles | 13 people with ALS and 10 healthy people | To evaluate glossopharyngeal muscle involvement in amyotrophic lateral sclerosis (ALS). |
| Medical imaging, mandibular kinematics, and EMG | Jianqiao Guo, Junpeng Chen, Jing Wang et al. [63] | 2022 | Temporalis and masseter | 7 healthy volunteers | To establish a subject-specific mandibular modeling framework based on clinical measurements. |
| sEMG | Wei-Han Chang, Mei-Hui Chen et al. [75] | 2023 | Anterior temporal muscle, masticatory muscle, and submaxillary muscle | 101 subjects with normal swallowing function | Temporal events observed by sEMG were evaluated to elucidate how aging affects coordination between the masticatory and submaxillary muscles. |
| sEMG | Chiaki Murakami, Makoto Sasaki et al. [19] | 2023 | Musculus hyoideus | 14 healthy young adults and 14 elderly subjects | Based on sEMG through the muscle coordination analysis to quantify the swallowing mechanism. |
| sEMG (self-made spherical electrodes) | Naoya Saito, Toru Ogawa, Naru Shiraishi, Rie Koide et al. [76] | 2023 | Masticatory muscles, bilateral abdominal muscles, and hyoid muscles | 12 healthy adults | sEMG signals were evaluated to investigate differences in the behavior of masticating and swallowing muscles during spontaneous versus cue swallowing. |
| sEMG | Sebastian Roldan-Vasco et al. [52] | 2023 | Masticatory muscle and sublingual muscle group | 31 healthy people and 29 people with dysphagia | To study the automatic analysis of sEMG records in healthy people and patients with functional throat dysphagia. |
| sEMG and ultrasonic image | Ching-Hsuan Pen, Barbara R. Pauloski [77] | 2023 | Mandibular muscle | 24 healthy adults | To explore the effect of real-time ultrasound as visual feedback in MM teaching of healthy adults. |
| EMG, acoustic, bioimpedance, and high-resolution manometry | Miho Ohashi, Yoichiro Aoyagi, Satoshi Ito et al. [77] | 2023 | Surface of neck | 6 healthy individuals (4 men, 2 women) participated in this study. | Comparison of EMG, acoustic, bioimpedance and high-resolution manometry for identification of swallowing and vocalization events. |
| sEMG and accelerometer-based neck auscultation (Acc) | Sebastian Roldan-Vasco, Juan Pablo Restrepo-Uribe et al. [78] | 2023 | Superior and inferior thyroid muscles | 30 healthy individuals and 30 patients with functional oropharyngeal dysphagia | A non-invasive, multimodal approach for dysphagia screening using sEMG and accelerometer-based neck auscultation (Acc) was introduced. |
| EKSS, LPM, pressure, and needle electrode | Enrico Alfonsi, Massimiliano Todisco et al. [79] | 2023 | Inferior/submental muscle complex | 15 healthy subjects | To study the electrodynamics of oropharyngeal swallowing in patients with neurogenic dysphagia. |
| sEMG and tongue pressure gauge | R. Vaitheeshwari, Shih-Ching Yeh et al. [46] | 2023 | Laryngeal muscle | 8 subjects. | sEMG and tongue pressure gauges were implemented to assess and improve swallowing function in patients with dysphagia. |
| EMG and sound sensor | Adrien Mialland, Ihab Atallah, Agnès Bonvilain [80] | 2024 | Hyohyoid muscle and posterior submental muscle, submental muscle | 17 participants | Intramuscular electromyography was used to evaluate the hyohyoid and posterior submentalis muscles for feasibility analysis of an implantable active artificial larynx. |
| Method | Advantages | Disadvantages | |
|---|---|---|---|
| Videofluoroscopic Swallowing Study (VFSS) | Provides a clear visual representation of food movement from the mouth to the esophagus, identifies issues like pharyngeal residue and aspiration. | Uses X-rays, posing radiation risks; requires special equipment and technical operation, which are costly. | |
| Flexible Endoscopic Evaluation of Swallowing (FEES) | Directly observes the structure and function of the pharynx, can identify disorders such as vagal nerve dysfunction; does not use radiation. | May cause discomfort to patients; the field of view is limited to the scope of the endoscope. | |
| Electromyography (EMG) | Surface Electromyography (sEMG) | Non-invasive, allows for real-time monitoring of muscle activity during swallowing. | Limited to surface muscles, does not provide information about deep muscle activity. |
| Needle Electrodes | Can record deep muscle electrical activity in detail, helping to diagnose muscle dysfunction. | Invasive, may cause pain or other complications. | |
| High-resolution manometry (HRM) | Non-invasive, by measuring pressure, it can analyze esophageal swallowing function and pressure changes in detail. | Equipment is expensive and requires professional operation and analysis. | |
| Bioimpedance | Non-invasive, by measuring changes in tissue impedance, it indirectly understands swallowing function. | Data interpretation is complex and can be influenced by various physiological and environmental factors. | |
| Barometric Pressure (BP) | Measures changes in pharyngeal and surrounding air pressure, helping to assess air pressure regulation functions. | Relatively limited technical application, limited data interpretation and practical application. | |
| Myotonometer | Measures muscle stiffness and elasticity, which can assess muscle condition. | May not directly correlate with direct swallowing function. | |
| Mechanomyography (MMG) | Non-invasive assessment of muscle activity through sensing muscle vibrations. | Signals may be disrupted by external noise and movement. | |
| Cervical Auscultation (Acoustics and Vibration) | Non-invasively detects acoustic characteristics during swallowing using sound and vibration sensors. | Interpreting sound data may be subjective and limited in accuracy. | |
| Photoelectric Sensor | Monitors swallowing actions through a photoelectric sensor, simple and non-invasive. | Limited information, difficult to provide in-depth physiological data. | |
| Ultrasound | Ultrasonic Image | No radiation, visually displays tissue structures and movements. | Image resolution and quality are limited by the equipment. |
| Doppler Ultrasound | Can accurately identify types of food, have excellent ability to resist environmental noise interference, dynamic monitoring and evaluation can be carried out. | Equipment and operation requirements are high, data interpretation and analysis are complex, and the application range is limited. | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, Y.; Guo, K.; Chu, Y.; Wang, Z.; Yang, H.; Zhang, J. Advancements and Challenges in Non-Invasive Sensor Technologies for Swallowing Assessment: A Review. Bioengineering 2024, 11, 430. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering11050430
Wu Y, Guo K, Chu Y, Wang Z, Yang H, Zhang J. Advancements and Challenges in Non-Invasive Sensor Technologies for Swallowing Assessment: A Review. Bioengineering. 2024; 11(5):430. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering11050430
Chicago/Turabian StyleWu, Yuwen, Kai Guo, Yuyi Chu, Zhisen Wang, Hongbo Yang, and Juzhong Zhang. 2024. "Advancements and Challenges in Non-Invasive Sensor Technologies for Swallowing Assessment: A Review" Bioengineering 11, no. 5: 430. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering11050430