
Blending Behavioural Theory and Narrative Analysis to Explore the Lived Experience of Obesity and Assess Potential Engagement in a UK Weight Management Service: Theory and Narrative Approaches in Weight Management

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Role of the Researcher(s)
2.3. Participants and Procedure
2.4. Data Analysis
2.5. Trustworthiness and Rigor
3. Results
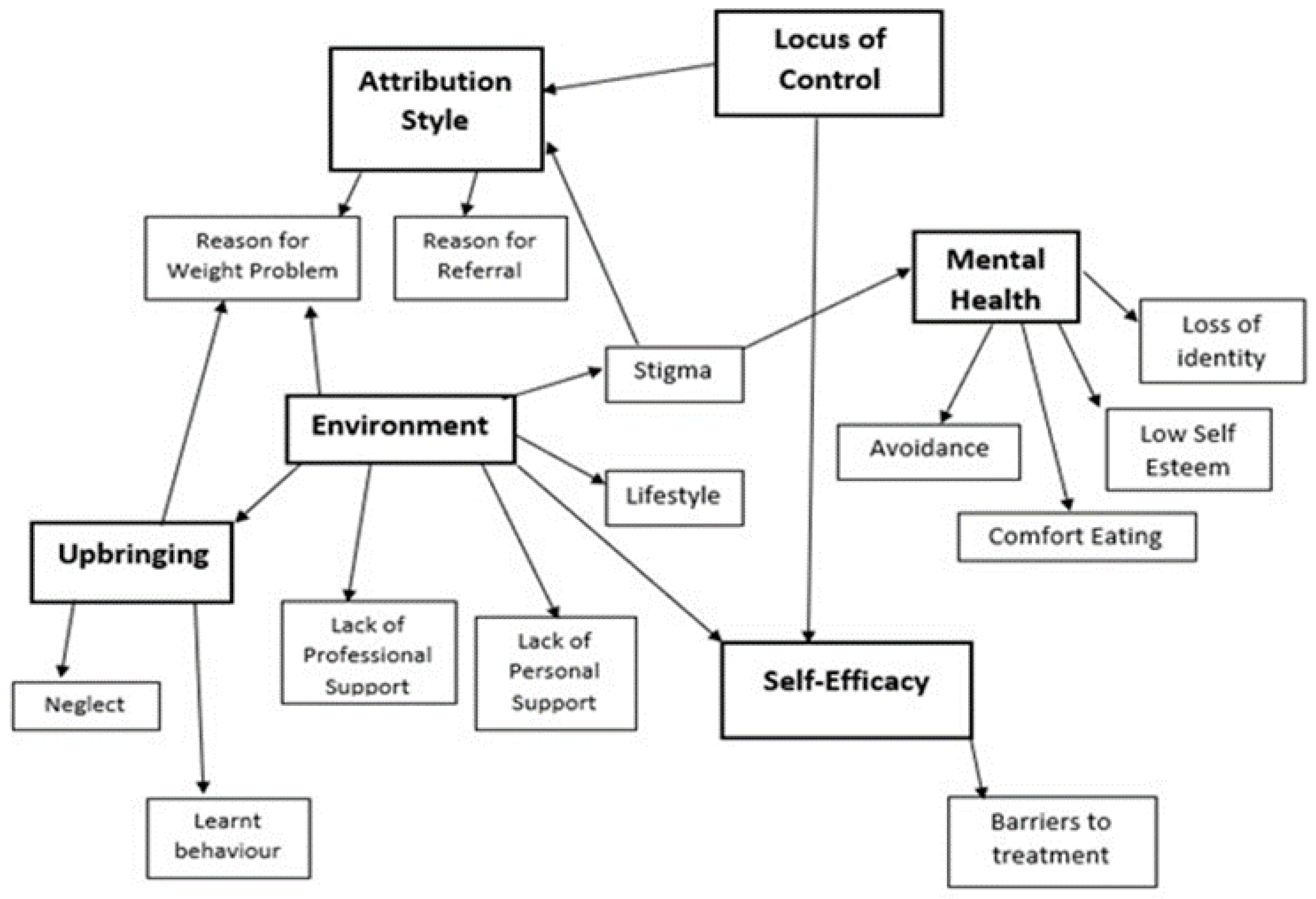
3.1. Theoretical Analysis
3.1.1. Locus of Control
3.1.2. Attribution Style
3.1.3. Self-Efficacy
3.1.4. Environment
3.1.5. Upbringing
3.1.6. Mental Health
3.2. Narrative Analysis: Storylines and Stages of Change
3.2.1. Stages of Change: Contemplation
| Representative Case for Contemplation Phase. |
| Jane—‘There’s nothing I can do, I’m an awkward one.’ Jane attributes the cause of her weight gain to being diagnosed with diabetes and prescribed insulin in her 30s, when ‘the weight walloped on’. She describes a long battle since, trying various avenues to weight loss, such as attending groups, medication, and exercise, all of which have failed. She made these attempts with her son who had success when she did not, contributing to her identification as ‘one of the awkward ones’. Jane’s WMC referral was suggested by her GP. She had reservations because she has tried for so long to lose weight. She attended one group and left feeling angry as the practitioner did not listen to her, and as a result did not attend the second. She is clearly still thinking as to whether she will engage with treatment or not, which places her into the contemplation Stage of Change. |
3.2.2. Stages of Change: Preparation
| Representative Case for Preparation Phase. |
| John—‘Coping with life events through food.’ John was active growing up and injured his knees playing football aged 14. Weight started to become a problem 15 years ago when he discovered his wife was cheating on him and they separated. A two-year period of using alcohol and food to cope with his emotions took place, until he met his current partner. John reports that they currently drink less alcohol, but recognises that his eating habits are still problematic. He did, however, go several weeks without eating takeaways prior to going on holiday recently. John needs knee surgery but has been told he must lose weight before the operation can take place. The nurse and his partner encouraged him to attend the WMC. His goal is to lose weight so he can get surgery for his knee and return to work, something which is important to him. |
3.2.3. Stages of Change: Action
| Representative Case for Participants in Action |
| Joe—‘Health scares and taking responsibility’ Joe had a difficult relationship with his father, so lived with his grandparents who displayed love through cooking Joe desserts, giving him large portions, and offerin sweet treats. As a result, he described being a ‘fat kid’. Whilst employed as a refuse collector, he ‘ran the weight off’. However, he then got a driving job and quit smoking, which led to increased eating, alcohol consumption and weight gain. He describes weight impacting his life as he is not as agile when climbing up and down from his lorry and it stops him from working on cars, which he enjoys. Since having serious heart problems, he has bought smaller plates and cutlery to decrease his portion size and ‘trick his mind’ into eating less. He feels he has lost weight as his clothes are loose. Six months ago, Joe told his nurse he would like help with his weight, so she referred him to the WMC. |
3.2.4. Synthesis of the Labovian Analysis
4. Discussion
Strengths, Limitations, and Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Labovian Category | Description |
|---|---|
| Abstract | A summary of the story—what is the story about? This serves the purpose of introducing the story and occurs at the beginning. |
| Orientation | Provides the setting in which the events of the story will be told. Who, when, where, what? This usually occurs early, but speakers may insert extra background information later. |
| Complicating Action | Sometimes referred to as the ‘skeleton plot’ of the story. Complicating Actions are the events of the story and follow a ‘and then’, pattern. They are generally chronological or in time context. |
| Evaluation | Reveals the speaker’s perspective on what they are telling. It is when they step back from the story to tell the listener its meaning. ‘So what?’ It tells the listener what the point is by conveying the speaker’s experience of the events at the time they took place, and their feelings about the experience at the time of telling. |
| Resolution | Tells the listener how the story ends. The resolution is the story’s outcome. |
| Coda | Signing off the story and returning to the present. It indicates the story is over. Stories do not always have a coda. |
| Constructs/Sub Constructs | N = Transcripts | Illustrative Quotes |
|---|---|---|
| Locus of Control External | 20 | “It’s the insulin, and she said to me “as long as you’re on insulin, you’ll never lose” so I thought, you know, oh well, that’s that”. (P6) |
| Attribution Style Reason for Weight Problems Attributed to Past Life Events Reason for Referral | 20 | “Breaking my ankle was the thing. Yeh”. (P1) |
| 20 | “Well she just said, “I think it would be beneficial for you to go to the classes”. (P6) | |
| Self-Efficacy | 20 | “But I will stick at it, and I will promise you, I will lose weight”. (P7) |
| Barriers to Treatment | 17 | “If it’s peeing down with rain, I ain’t coming out. I guarantee you that I ain’t coming out. I’m not spending seven pound on a taxi to get here and go back home and it’s cost me fourteen quid”. (P3) |
| Environment Lack of Professional Support Lack of Personal Support Lifestyle Stigma | 12 | “And unfortunately, she [nurse] obviously had never had a weight problem because she said, losing weight is so easy, (laughs) I wish I could put it in a bottle and sell it. (Laughs) But that just completely put me off, so I never went back there either”. (P12) |
| 15 | “And I’ve said to him like, when I’ve got the gastric band you know or like when I’m dieting, I need his support fully and he said, “it’s not me on the diet it’s you”. So, I have the funny feeling that I’m still going to have to see extremely greasy beautiful stuff whilst I’m trying to shift a lot of weight”. (P1) | |
| 13 | “I done night work. So, bringing up children, I think me eating the wrong time each time and not eating properly, it just ballooned up me weight, ‘cause I did go up to about 20 odd stone”. (P14) | |
| 16 | “I heard him say the other day, well, he said ‘that fat bastard in the garden’, […] But sometimes I laugh it off but I deep down I do feel a bit, what can you say? I don’t know what the word be? Ashamed of being that weight?” (P7) | |
| Upbringing Neglect Learnt Behaviour | 7 | “…so she [Mum] went out to work and I was left and my brother had to look after me and so my tea everyday was bread and syrup sandwiches, loads and loads of them dipped in tea and there was nobody there to…you know, guide me”. (P4) |
| 9 | “I think it starts in your childhood, you know, because food is a reward…” (P4) | |
| Mental Health Low Self-Esteem Avoidance Loss of Identity Comfort Eating | 17 | “Yeah, you look in the mirror I don’t like it really, I really don’t like what I see, to be honest with you, not at all”. (P15) |
| 12 | “Um, I probably wouldn’t go back to tennis now, the weight I am. Even though it’s probably really good for you”. (P19) | |
| 8 | “I did go through a phase of having counselling and went on anti-depressants, ‘cause I lost everything. In my eyes I had lost everything. You know I had always wanted to teach dance. […] What I was then and what I am now are so different”. (P1) | |
| 12 | “…unfortunately, I’m one of these people that when I get stressed, or down in the dumps, and things like that…I eat”.—(P16) |
References
- Gadde, K.M.; Martin, C.K.; Berthoud, H.R.; Heymsfield, S.B. Obesity: Pathophysiology and Management. J. Am. Coll. Cardiol. 2018, 71, 69–84. [Google Scholar] [CrossRef]
- Withrow, D.; Alter, D.A. The Economic Burden of Obesity Worldwide: A Systematic Review of the Direct Costs of Obesity. Obes. Rev. 2011, 12, 131–141. [Google Scholar] [CrossRef]
- Cai, Q.; Chen, F.; Wang, T.; Luo, F.; Liu, X.; Wu, Q.; He, Q.; Wang, Z.; Liu, Y.; Liu, L.; et al. Obesity and COVID-19 Severity in a Designated Hospital in Shenzhen, China. Diabetes Care 2020, 43, 1392–1398. [Google Scholar] [CrossRef]
- Gao, F.; Zheng, K.I.; Wang, X.B.; Sun, Q.F.; Pan, K.H.; Wang, T.Y.; Chen, Y.P.; Targher, G.; Byrne, C.D.; George, J.; et al. Obesity is a Risk Factor for Greater COVID-19 Severity. Diabetes Care 2020, 43, 72–74. [Google Scholar] [CrossRef]
- Department of Health and Social Care. New Obesity Strategy Unveiled as Country Urged to Lose Weight to Beat Coronavirus (COVID-19) and Protect the NHS. Available online: https://www.gov.uk/government/news/new-obesity-strategy-unveiled-as-country-urged-to-lose-weight-to-beat-coronavirus-covid-19-and-protect-the-nhs (accessed on 21 March 2024).
- Kalra, S.; Kapoor, N.; Kota, S.; Das, S. Person-Centred Obesity Care—Techniques, Thresholds, Tools and Targets. Eur. Endocrinol. 2020, 16, 11–13. [Google Scholar] [CrossRef]
- Ells, L.J.; Ashton, M.; Li, R.; Logue, J.; Griffiths, C.; Torbahn, G.; Marwood, J.; Stubbs, J.; Clare, K.; Gately, P.J.; et al. Can We Deliver Person-Centred Obesity Care Across the Globe? Curr. Obes. Rep. 2022, 11, 350–355. [Google Scholar] [CrossRef]
- NICE. [CG189]. Obesity: Identification, Assessment and Management. Clinical Guideline (26/7/23). Available online: https://www.nice.org.uk/guidance/cg189/chapter/Recommendations#identifying-and-assessing-overweight-obesity-and-central-adiposity (accessed on 21 March 2024).
- Perriard-Abdoh, S.; Chadwick, P.; Chater, A.M.; Chisolm, A.; Doyle, J.; Gillison, F.B.; Greaves, C.; Liardet, J.; Llewellyn, C.; McKenna, I.; et al. Psychological Perspectives on Obesity—Addressing Policy, Practice, and Research Priorities; British Psychological Society: London, UK, 2019; Available online: http://hdl.handle.net/10547/623942 (accessed on 21 March 2024).
- Sharma, A.M. Obesity and Mental Health—A Complicated and Complex Relation. Can. J. Psychiatry 2012, 57, 3–4. [Google Scholar] [CrossRef]
- Ball, K.; Mishra, G.D.; Crawford, D. Social Factors and Obesity: An Investigation of the Role of Health Behaviours. Int. J. Obes. 2003, 27, 394–403. [Google Scholar] [CrossRef]
- Baker, C. Research Briefing: Obesity; House of Commons Library: London, UK, 2023; Available online: https://commonslibrary.parliament.uk/research-briefings/sn03336/#:~:text=Obesity%20is%20usually%20defined%20as,%2C%2059.0%25%20of%20women (accessed on 21 March 2024).
- McLaren, L. Socioeconomic Status and Obesity. Epidemiol. Rev. 2007, 29, 29–48. [Google Scholar] [CrossRef]
- Graham, D.; Edwards, A. The Psychological Burden of Obesity: The Potential Harmful Impact of Health Promotion and Education Programmes Targeting Obese Individuals. Int. J. Health Promot. Educ. 2013, 51, 124–133. [Google Scholar] [CrossRef]
- Leon, G. A behavioral approach to obesity. Am. J. Clin. Nutr. 1977, 30, 785–789. [Google Scholar] [CrossRef]
- Crawford, D.; Ball, K. Behavioural determinants of the obesity epidemic. Asia Pac. J. Clin. Nutr. 2002, 11, S718–S721. [Google Scholar] [CrossRef]
- Higgs, S. Is there a role for higher cognitive processes in the development of obesity in humans? Phil. Trans. R. Soc. B 2022, 378, 20220208. [Google Scholar] [CrossRef]
- Chadwick, P.; Chater, A.; Gillison, F.; Llewellyn, C.; Moffat, H.; Newsome, L.; Reid, M.; Singh, S.; Snowden-Carr, V. Psychological Perspectives on Obesity: Addressing Policy, Practice and Research Priorities; British Psychological Society: London, UK, 2019; Available online: https://www.bps.org.uk/psychologist/psychological-perspectives-obesity (accessed on 21 March 2024).
- Davis, R.; Campbell, R.; Hildon, Z.; Hobbs, L.; Michie, S. Theories of Behaviour and Behaviour Change Across the Social and Behavioural Sciences: A Scoping Review. Health Psychol. Rev. 2015, 9, 323–344. [Google Scholar] [CrossRef]
- Weiner, B. An Attributional Theory of Achievement Motivation and Emotion. Psychol. Rev. 1985, 92, 548–573. [Google Scholar] [CrossRef]
- Bradley, C. Handbook of Psychology and Diabetes: A Guide to Psychological Measurement in Diabetes Research and Practice, 1st ed.; Routeledge: London, UK, 1994. [Google Scholar]
- Grisolia, J.M.; Longo, A.; Hutchinson, G.; Kee, F. Applying Health Locus of Control and Latent Class Modelling to Food and Physical Activity Choice Affecting CVD Risk. Soc. Sci. Med. 2015, 132, 1–10. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy Mechanism in Human Agency. Am. Psychol. 1982, 37, 122–147. [Google Scholar] [CrossRef]
- Steele, A.L.; Bergin, J.; Wade, T.D. Self-Efficacy as a Robust Predictor of Outcome in Guided Self-Help Treatment for Broadly Defined Bulimia Nervosa. Int. J. Eat. Disord. 2011, 44, 389–396. [Google Scholar] [CrossRef]
- Prochaska, J.O.; DiClemente, C.C. Stages and Processes of Self-Change of Smoking: Toward an Integrative Model of Change. J. Consult. Clin. Psychol. 1983, 51, 390–395. [Google Scholar] [CrossRef]
- Norcross, J.C.; Krebs, P.M.; Prochaska, J.O. Stages of Change. J. Clin. Psychol. 2011, 67, 143–154. [Google Scholar] [CrossRef]
- Andres, A.; Saldana, C.; Gomez-Benito, J. The Transtheoretical Model in Weight Management: Validation of the Processes of Change Questionnaire. Eur. J. Obes. 2011, 4, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Macqueen, C.E.; Brynes, A.E.; Frost, G.S. Treating Obesity: Can the Stages of Change Model Help Predict Outcome Measures? J. Hum. Nutr. Diet. 1999, 12, 229–236. [Google Scholar] [CrossRef]
- Kozica, S.; Lombard, C.; Teede, H.; Ilic, D.; Murphy, K.; Harrison, C. Initiating and Continuing Behaviour Change Within a Weight Gain Prevention Trial: A Qualitative Investigation. PLoS ONE 2015, 10, e0119773. [Google Scholar] [CrossRef] [PubMed]
- Kalitzkus, V.; Matthiessen, P.F. Narrative-Based Medicine: Potential, Pitfalls, and Practice. Perm. J. 2009, 13, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Naldemirci, Ö.; Britten, N.; Lloyd, H.; Wolf, A. The Potential and Pitfalls of Narrative Elicitation in Person-Centred Care. Health Expect. Int. J. Public Particip. Health Care Health Policy 2020, 23, 238–246. [Google Scholar] [CrossRef]
- Zaharias, G. What is Narrative-Based Medicine? Narrative-Based Medicine 1. Can. Fam. Physician Med. De Fam. Can. 2018, 64, 176–180. [Google Scholar]
- Ardito, R.B.; Rabellino, D. Therapeutic Alliance and Outcome of Psychotherapy: Historical Excursus, Measurements, and Prospects for Research. Front. Psychol. 2011, 2, 270. [Google Scholar] [CrossRef]
- Andrews, M.; Squire, C.; Tambouku, M. Doing Narrative Research; SAGE Publications Ltd.: London, UK, 2013. [Google Scholar]
- Greenhalgh, T.; Hurwitz, B. Narrative Based Medicine: Dialogue and Discourse in Clinical Practice; BMJ Publishing Group: London, UK, 1998. [Google Scholar]
- Silver, J. Narrative Psychology. In Introducing Qualitative Research in Psychology, 3rd ed.; Willig, C., Ed.; McGraw Hill Education, Open University Press: Maidenhead, UK, 2013; pp. 143–155. ISBN 978-0-33-524449-2. [Google Scholar]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Labov, W. Language in the Inner City: Studies in the Black English Vernacular; University of Pennsylvania Press: Philadelphia, PA, USA, 1972. [Google Scholar]
- Wong, G.; Breheny, M. Narrative Analysis in Health Psychology: A Guide for Analysis. Adv. Methods Health Psychol. Behav. Med. 2018, 6, 245–261. [Google Scholar] [CrossRef]
- Brochu, P.M.; Gawronski, B.; Esses, V.M. The Integrative Prejudice Framework Different Forms of Weight Prejudice: An Analysis and Expansion. Group Process. Intergroup Relat. 2011, 14, 429–444. [Google Scholar] [CrossRef]
- Bury, M. Chronic Illness as Biographical Disruption. Sociol. Health Illn. 1982, 4, 167–182. [Google Scholar] [CrossRef] [PubMed]
- Pawson, R. Theorizing the Interview. Br. J. Sociol. 1996, 47, 295–314. [Google Scholar] [CrossRef]
- Mattingly, C. Healing Dramas and Clinical Plots: The Narrative Structure of Experience, 2nd ed.; Cambridge University Press: Cambridge, UK, 1998. [Google Scholar] [CrossRef]
- Wolf, A.; Moore, L.; Lyda, D.; Naldemirci, Ö.; Elam, M.; Britten, N. The Realities of Partnership in Person-Centred Care: A qualitative Interview Study with Patients and Professionals. BMJ Open 2017, 7, e016491. [Google Scholar] [CrossRef] [PubMed]
- Fors, A.; Ekman, I.; Taft, C.; Björkelund, C.; Frid, K.; Larsson, M.E.H.; Thorn, J.; Ulin, K.; Wolf, A.; Swedberg, K. Person-Centred Care After Acute Coronary Syndrome, from Hospital to Primary Care—A Randomised Controlled Trial. Int. J. Cardiol. 2015, 187, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, L. Psychological Formulation as an Alternative to Psychiatric Diagnosis. J. Humanist. Psychol. 2018, 58, 30–46. [Google Scholar] [CrossRef]
- Mason, S.M.; Austin, S.B.; Bakalar, J.L.; Boynton-Jarrett, R.; Field, A.E.; Gooding, H.C.; Holsen, L.M.; Jackson, B.; Neumark-Sztainer, D.; Sanchez, M.; et al. Child Maltreatment’s Heavy Toll: The Need for Trauma-Informed Obesity Prevention. Am. J. Prev. Med. 2016, 50, 646–649. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.M.; Heuer, C.A. The Stigma of Obesity: A Review and Update. Obesity 2009, 17, 941–964. [Google Scholar] [CrossRef] [PubMed]
- Fricker, M. Epistemic Injustice: Power and the Ethics of Knowing; Oxford University Press: Oxford, UK, 2007. [Google Scholar] [CrossRef]
- Rice, C. Becoming the “Fat Girl”: Acquisition of an Unfit Identity. Women’s Stud. Int. Forum 2007, 30, 158–174. [Google Scholar] [CrossRef]
- Bradby, H.; Lindenmeyer, A.; Phillimore, J.; Padilla, B.; Brand, T. ‘If there were Doctors who could understand our problems, I would be already better’: Dissatisfactory Health Care and Marginalisation in Superdiverse Neighborhoods. Sociol. Health Illn. 2020, 42, 739–757. [Google Scholar] [CrossRef]
- Lyons, E.; Coyle, A. Analysing Qualitative Data in Psychology, 2nd ed.; SAGE Publications: London, UK, 2016. [Google Scholar]
- Miller, W.R.; Rollnick, S. Motivational Interviewing: Helping People Change, 3rd ed.; The Guildford Press: New York, NY, USA, 2012. [Google Scholar]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gillespie, J.; Wright, H.; Pinkney, J.; Lloyd, H. Blending Behavioural Theory and Narrative Analysis to Explore the Lived Experience of Obesity and Assess Potential Engagement in a UK Weight Management Service: Theory and Narrative Approaches in Weight Management. Healthcare 2024, 12, 747. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare12070747
Gillespie J, Wright H, Pinkney J, Lloyd H. Blending Behavioural Theory and Narrative Analysis to Explore the Lived Experience of Obesity and Assess Potential Engagement in a UK Weight Management Service: Theory and Narrative Approaches in Weight Management. Healthcare. 2024; 12(7):747. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare12070747
Chicago/Turabian StyleGillespie, Jessica, Hannah Wright, Jonathan Pinkney, and Helen Lloyd. 2024. "Blending Behavioural Theory and Narrative Analysis to Explore the Lived Experience of Obesity and Assess Potential Engagement in a UK Weight Management Service: Theory and Narrative Approaches in Weight Management" Healthcare 12, no. 7: 747. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare12070747