Development and Implementation of an Ultraviolet-Dye-Based Qualification Procedure for Hand Washing and Disinfection to Improve Quality Assurance of Pharmacy Preparations and Compounding, Especially in Cleanrooms: A Pilot Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Location, and Participants
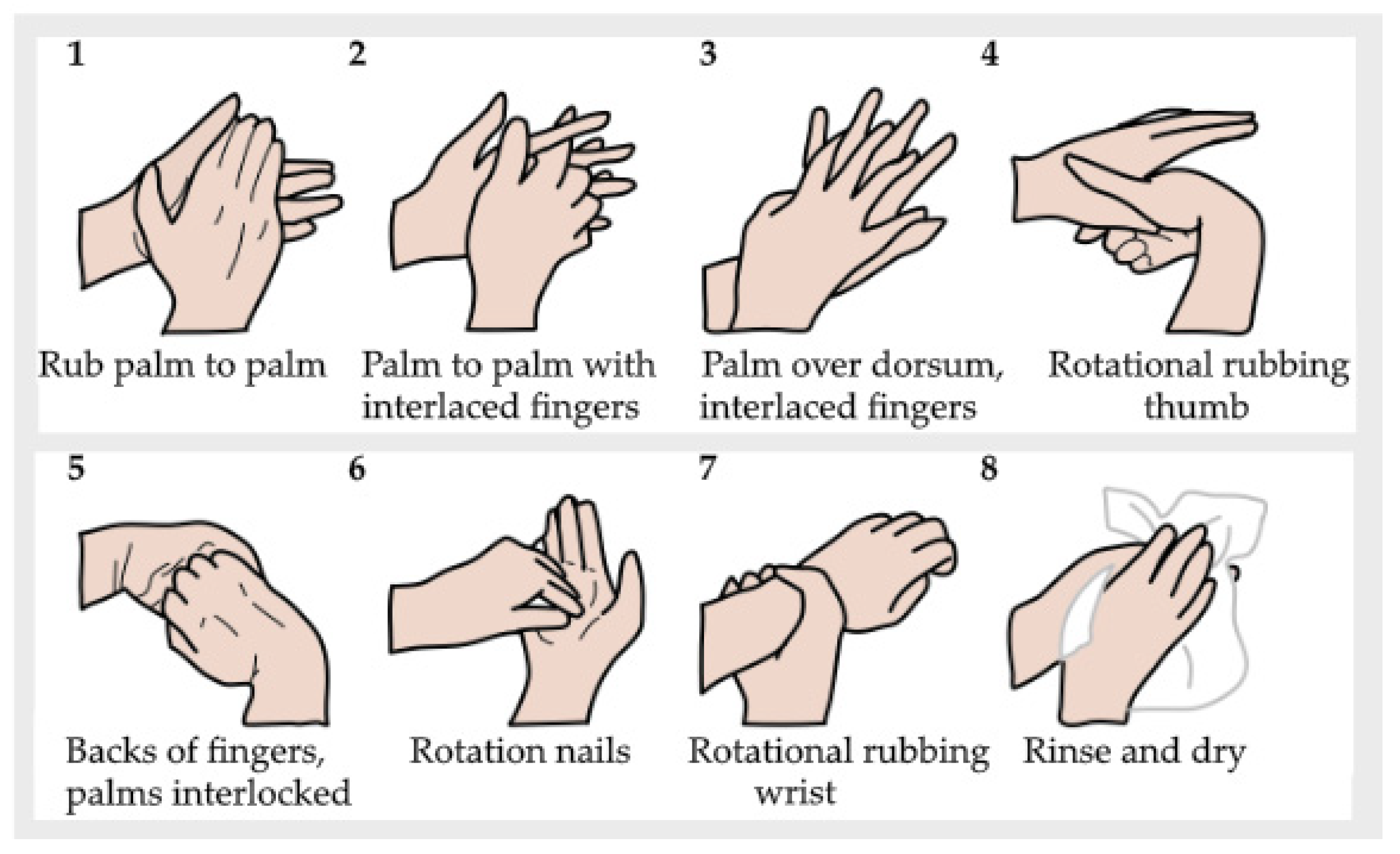
2.2. Hand Washing


2.3. Hand Disinfection
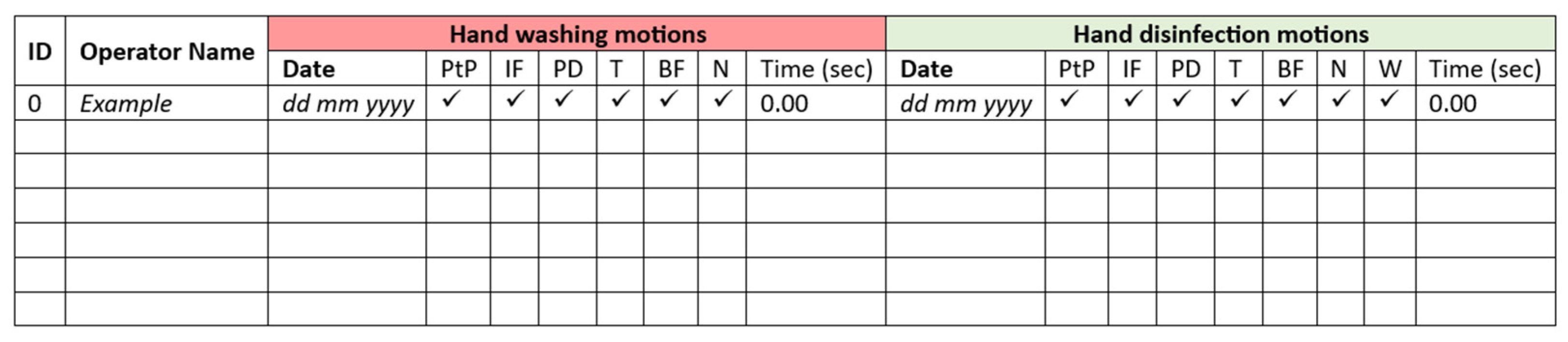
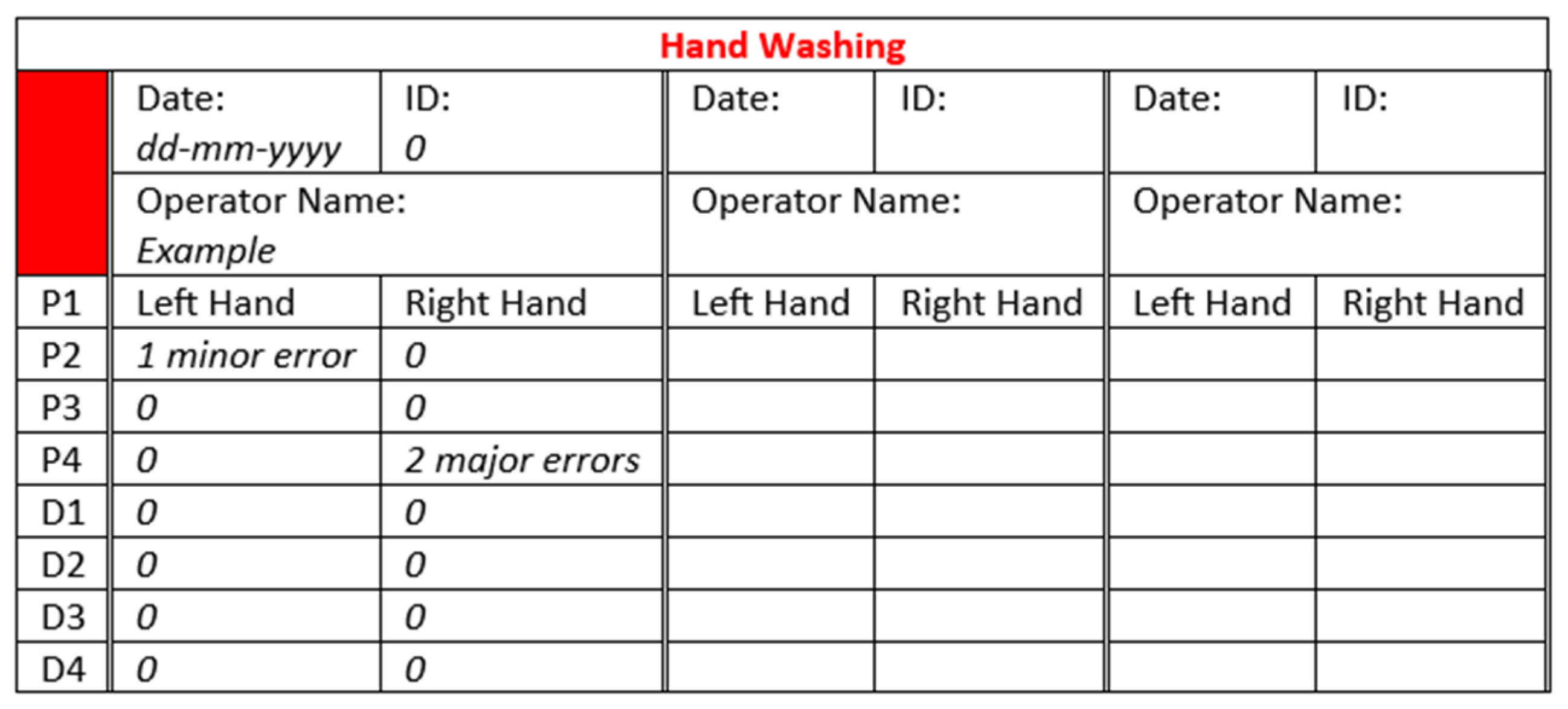
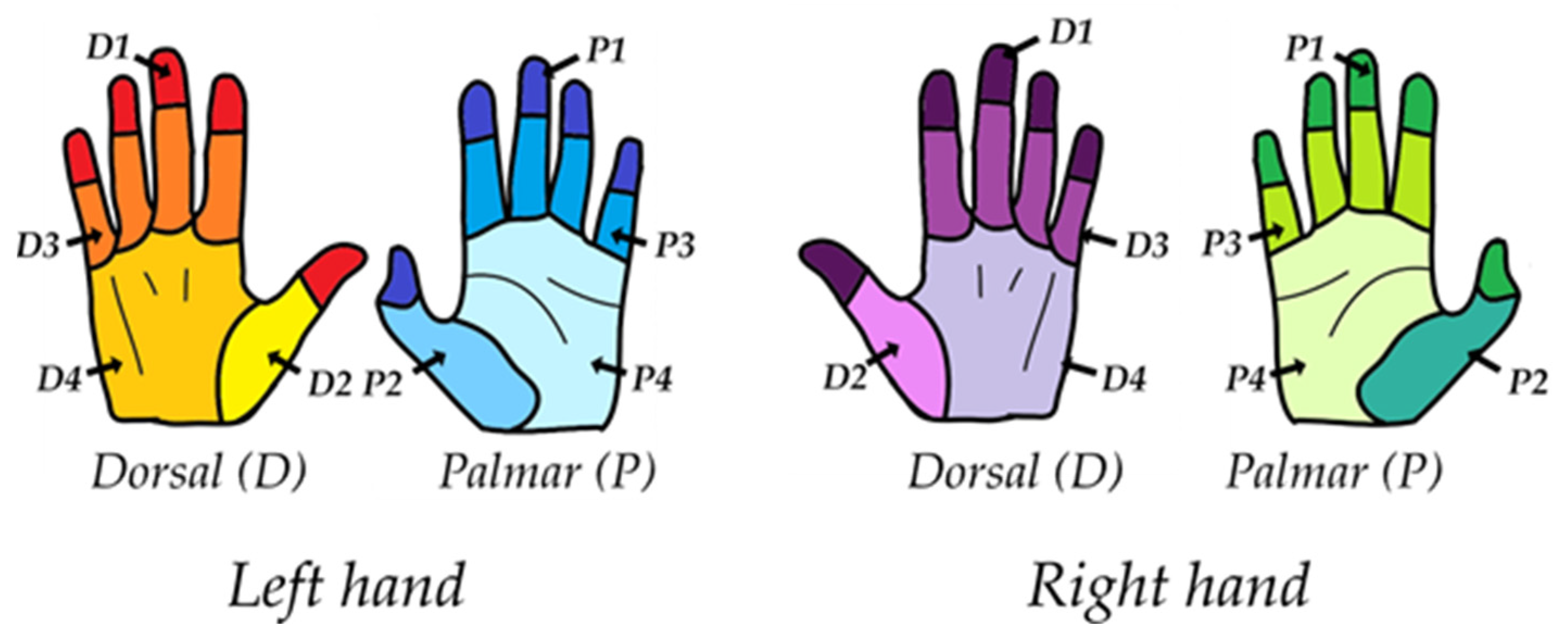
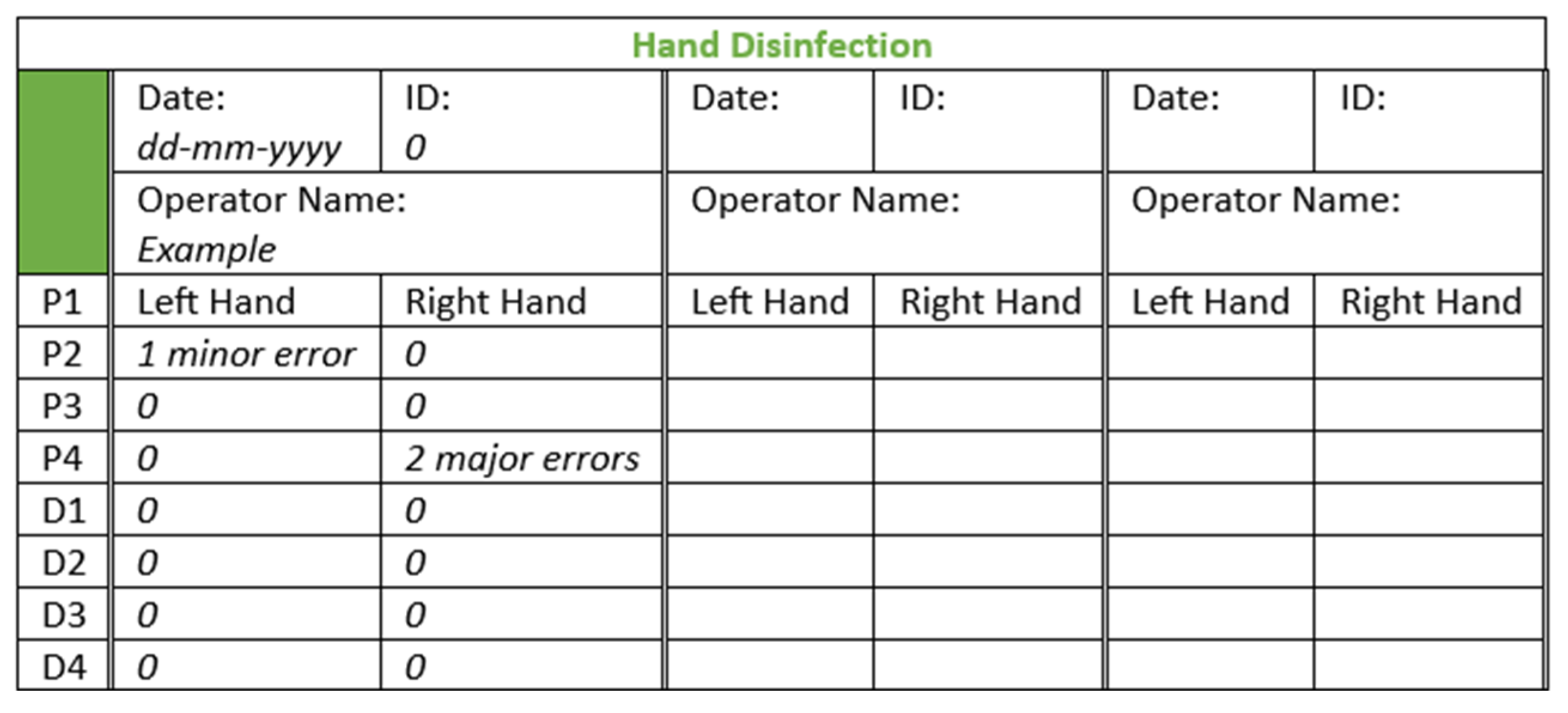
2.4. Analysis of Photographic Material
2.5. Statistics
3. Results
3.1. Adherence to Hand Washing and Hand Disinfection Procedures
3.2. Missed Hand Areas in Hand Washing and Hand Disinfection Procedures
3.3. Procedure Duration: Influence of Time on Efficacy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Council of Europe. Resolution CM/Res(2016)1 on Quality and Safety Assurance Requirements for Medicinal Products Prepared in Pharmacies for the Special Needs of Patients. Available online: https://search.coe.int/cm/Pages/result_details.aspx?ObjectID=090000168065c132 (accessed on 26 September 2023).
- Le Brun, P.; Crauste-Manciet, S.; Krämer, I.; Smith, J.; Woerdenbag, H. Preface. In Practical Pharmaceutics. An International Guideline for the Preparation, Care and Use of Medicinal Products, 2nd ed.; Le Brun, P., Crauste-Manciet, S., Krämer, I., Smith, J., Woerdenbag, H., Eds.; Springer Nature Switzerland: Cham, Switzerland, 2023; pp. v–vii. [Google Scholar]
- World Health Organization; International Pharmaceutical Federation. WHO Technical Report Series, No. 961, 2011, Annex 8 Joint FIP/WHO Guidelines on Good Pharmacy Practice: Standards for Quality of Pharmacy Services 2011. Available online: https://www.who.int/docs/default-source/medicines/norms-and-standards/guidelines/distribution/trs961-annex8-fipwhoguidelinesgoodpharmacypractice.pdf (accessed on 26 September 2023).
- Watson, C.J.; Whitledge, J.D.; Siani, A.M.; Burns, M.M. Pharmaceutical compounding: A history, regulatory overview, and systematic review of compounding errors. J. Med. Toxicol. 2021, 17, 197–217. [Google Scholar] [CrossRef]
- European Association of Hospital Pharmacists. EAHP Position Paper on Pharmacy Preparations and Compounding, Making a Difference in Medication by Delivering Tailor-Made Medicines for the Benefit of Patients. Adopted October 2020. Available online: https://www.eahp.eu/sites/default/files/eahp_position_paper_on_pharmacy_preparations_and_compounding_october_2020.pdf (accessed on 26 September 2023).
- Breitkreutz, J.; Boos, J. Pediatric and geriatric drug delivery. Exp. Opin. Drug Deliv. 2007, 4, 37–45. [Google Scholar] [CrossRef]
- Falconer, J.R.; Staedman, K.J. Extemporaneously compounded medicines. Aust. Prescr. 2017, 40, 5–8. [Google Scholar] [CrossRef]
- Ofei, K. The role of compounding pharmacists during drug shortages. Int. J. Pharm. Compd. 2022, 26, 298–301. [Google Scholar] [PubMed]
- Crommelin, D.J.A.; Bouwman-Boer, Y. Pharmacy preparations: Back in the limelight? Pharmacists make up your mind! Int. J. Pharm. 2016, 514, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Hepler, C.D.; Strand, L.M. Opportunities and responsibilities in pharmaceutical care. Am. J. Hosp. Pharm. 1990, 47, 533–543. [Google Scholar] [CrossRef]
- Austin, P.; Elia, M. A systematic review and meta-analysis of the risk of microbial contamination of aseptically prepared doses in different environments. J. Pharm. Pharm. Sci. 2009, 12, 233–242. [Google Scholar] [CrossRef]
- Larmené-Beld, K.H.M.; Frijlink, H.W.; Taxis, K. A systematic review wand meta-analysis of microbial contamination of parenteral medication prepared in a clinical versus pharmacy environment. Eur. J. Clin. Pharmacol. 2019, 75, 609–671. [Google Scholar] [CrossRef] [PubMed]
- Council of Europe. Resolution CM/Res(2016)2 on Good Reconstitution Practices in Health Care Establishments for Medicinal Products for Parenteral Use. Available online: https://www.edqm.eu/en/d/162941 (accessed on 28 November 2023).
- Beancy, A.M.; Le Brun, P.; Ravera, S.; Scheepers, H. Council of Europe Resolution CM/Res(2016)2: A major contribution to patient safety from reconstituted injectable medicines? Eur. J. Hosp. Pharm. 2020, 27, 216–221. [Google Scholar] [CrossRef]
- Resolution CM/Res(2020)3 on the Implementation of Pharmaceutical Care for the Benefit of Patients and Health Services. Available online: https://www.pcne.org/upload/files/400_Council_of_Europe_CM-Res20203_-_Final_-_EN.pdf (accessed on 6 December 2023).
- Centers for Disease Control and Prevention (CDC). Multistate outbreak of fungal infection associated with injection of methylprednisolone acetate solution from a single compounding pharmacy—United states, 2012. Morb. Mortal. Wkly Rep. 2012, 16, 839–842. Available online: https://www.cdc.gov/mmwp/pdf/wk/mm6141.pdf (accessed on 6 December 2023).
- Casadevall, A.; Pirofski, L.A. Exserohilum rostratum fungal meningitis associated with methylprednisolone injections. Future Microbiol. 2013, 8, 135–137. [Google Scholar] [CrossRef]
- Cousins, D.H.; Otero, M.J.; Schmitt, E. Time to review how injectable medicines are prepared and administered in European hospitals. Farm. Hospital. 2021, 45, 204–209. [Google Scholar] [CrossRef]
- United States Food and Drug Administration. FDA’s Human Drug Compounding Progress Report. January 2017. Available online: https://www.fda.gov (accessed on 28 November 2023).
- Lisi, D.M. Pros and cons of pharmacy compounding. US Pharm. 2021, 46, 8–12. Available online: https://www.uspharmacist.com/article/pros-and-cons-of-pharmacy-compounding-1 (accessed on 28 November 2023).
- Siamidi, A.; Pippa, N.; Demetzos, C. Pharmaceutical compounding: Recent advances, lessons learned and future perspectives. Glob. Drugs Therap. 2017, 2, 1–3. [Google Scholar] [CrossRef]
- European Directorate for the Quality of Medicines & HealthCare. Pharmaceutical Preparations. In European Pharmacopoeia (Ph. Eur.), 11.2 ed.; EDQM Council of Europe: Strasbourg, France, 2023; Available online: https://pheur.edqm.eu/home (accessed on 28 April 2023).
- American Society of Health-System Pharmacists (ASHP). ASHP guidelines on compounding sterile preparations. Am. J. Health-Syst. Pharm. 2014, 71, 145–166. [Google Scholar] [CrossRef] [PubMed]
- US Pharmaceutical Convention. United States Pharmacopeia. Monograph <797> Pharmaceutical Compounding—Sterile Preparations; NF-USP: Rockville, MD, USA, 2023. [Google Scholar]
- US Pharmaceutical Convention. United States Pharmacopeia. Monograph <795> Pharmaceutical Compounding—Non-Sterile Preparations; NF-USP: Rockville, MD, USA, 2023. [Google Scholar]
- US Pharmaceutical Convention. United States Pharmacopeia. Monograph <1075> Good Compounding Practices; NF-USP: Rockville, MD, USA, 2023. [Google Scholar]
- European Medicines Agency. Good Manufacturing Practice. Available online: https://www.ema.europa.eu/en/human-regulatory/research-development/compliance/good-manufacturing-practice (accessed on 26 September 2023).
- United States Food and Drugs Administration. Current Good Manufacturing Practice. Available online: https://www.fda.gov/drugs/pharmaceutical-quality-resources/current-good-manufacturing-practice-cgmp-regulations (accessed on 26 September 2023).
- World Health Organization. Health Products Policy and Standards, Good Manufacturing Practices. Available online: https://www.who.int/teams/health-product-policy-and-standards/standards-and-specifications/gmp (accessed on 26 September 2023).
- Commission Directive 2003/94/EC. Laying down the principles and guidelines of good manufacturing practice in respect of medicinal products for human use and investigational medicinal products for human use. European Commission: Brussels, Belgium. Off. J. Eur. Union 2003, L262, 22–26. Available online: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2003:262:0022:0026:en:PDF (accessed on 10 March 2023).
- Pharmaceutical Inspection Convention. PIC/S Guide to Good Practices for the Preparation of Medicinal Products in Healthcare Establishments. PE 010-4, 2014. Available online: https://picscheme.org/docview/3443 (accessed on 6 December 2023).
- Yuliani, S.H.; Putri, D.C.A.; Virginia, D.M.; Gani, M.R.; Riswanto, F.D.O. Prevalence, risk, and challenges of extemporaneous preparation for pediatric patients in developing nations: A review. Pharmaceutics 2023, 15, 840. [Google Scholar] [CrossRef]
- Directorate-General for Health and Food Safety. Annex 1. Manufacture of sterile medicinal products. In The Rules Governing Medicinal Products in the European Union Volume 4 EU Guidelines for Good Manufacturing Practice for Medicinal Products for Human and Veterinary Use; European Commission: Brussels, Belgium, 2022. Available online: https://health.ec.europa.eu/latest-updates/revision-manufacture-sterile-medicinal-products-2022-08-25_en (accessed on 10 March 2023).
- Boom, F.; Beaney, A. Aseptic Handling. Chapter 31. In Practical Pharmaceutics an International Guideline for the Preparation, Care and Use of Medicinal Products, 2nd ed.; Le Brun, P., Crauste-Manciet, S., Krämer, I., Smith, J., Woerdenbag, H., Eds.; Springer Nature Switzerland: Cham, Switzerland, 2023; pp. 749–765. [Google Scholar] [CrossRef]
- European Directorate for the Quality of Medicines & HealthCare. Sterility (2.6.1). In European Pharmacopoeia (Ph. Eur.), 11.2 ed.; EDQM Council of Europe: Strasbourg, France, 2023; Available online: https://pheur.edqm.eu/home (accessed on 6 December 2023).
- Jumaa, P.A. Hand hygiene: Simple and complex. Int. J. Infect. Dis. 2005, 9, 3–14. [Google Scholar] [CrossRef]
- World Health Organization; World Alliance for Patient Safety. WHO Guidelines on Hand Hygiene in Health Care; World Health Organization: Geneva, Switzerland, 2009. Available online: https://www.who.int/publications/i/item/9789241597906 (accessed on 10 March 2023).
- Ayliffe, G.A.; Babb, J.R.; Quoraishi, A.H. A test for ‘hygienic’ hand disinfection. J. Clin. Pathol. 1978, 31, 923–928. [Google Scholar] [CrossRef] [PubMed]
- Lacey, G.; Showstark, M.; van Rhee, J. Training to proficiency in the WHO hand hygiene technique. J. Med. Educ. Curric. Dev. 2019, 6, 2382120519867681. [Google Scholar] [CrossRef]
- Stilo, A.; Troiano, G.; Melcarne, L.; Gioffrè, M.E.; Nante, N.; Messina, G.; Laganà, P. Hand washing in operating room: A procedural comparison. Epidemiol. Biostat. Publ. Health 2016, 13, e11734. [Google Scholar] [CrossRef]
- World Health Organization. WHO Best Practices for Injections and Related Procedures Toolkit. Available online: https://www.who.int/publications/i/item/9789241599252 (accessed on 26 September 2023).
- Price, L.; Gozdzielewska, L.; Matuluko, A.; Pittet, D.; Allegranzi, B.; Reilly, J. Comparing the effectiveness of hand hygiene techniques in reducing the microbial load and covering hand surfaces in healthcare workers: Updated systematic review. Am. J. Infect. Control. 2022, 50, 1079–1090. [Google Scholar] [CrossRef]
- Macdonald, D.J.M.; McKillop, E.C.A.; Trotter, S.; Gray, A.J.R. Improving hand-washing performance—A crossover study of hand-washing in the orthopaedic department. Ann. R. Coll. Surg. Engl. 2006, 88, 289–291. [Google Scholar] [CrossRef]
- Kampf, G.; Ostermeyer, C.; Heeg, P.; Paulson, D. Evaluation of two methods of determining the efficacies of two alcohol-based hand rubs for surgical hand antisepsis. Appl. Environ. Microbiol. 2006, 72, 3856–3861. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.S.; Price, L.; Lang, S.; Robertson, C.; Cheater, F.; Skinner, K.; Chow, A. A pragmatic randomized controlled trial of 6-step vs 3-step hand hygiene technique in acute hospital care in the United Kingdom. Infect. Control Hosp. Epidemiol. 2016, 37, 661–666. [Google Scholar] [CrossRef]
- Lucet, J.C.; Rigaud, M.P.; Mentre, F.; Kassis, N.; Deblangy, C.; Andremont, A.; Bouvet, E. Hand contamination before and after different hand hygiene techniques: A randomized clinical trial. J. Hosp. Infect. 2002, 50, 276–280. [Google Scholar] [CrossRef]
- Lehotsky, A.; Szilágyi, L.; Bánsághi, S.; Szerémy, P.; Wéber, G.; Haidegger, T. Towards objective hand hygiene technique assessment: Validation of the ultraviolet-dye-based hand-rubbing quality assessment procedure. J. Hosp. Infect. 2017, 97, 26–29. [Google Scholar] [CrossRef]
- Vanyolos, E.; Peto, K.; Viszlai, A.; Miko, I.; Furka, I.; Nemeth, N.; Orosi, P. Usage of ultraviolet test method for monitoring the efficacy of surgical hand rub technique among medical students. J. Surg. Educ. 2015, 72, 530–535. [Google Scholar] [CrossRef]
- Szilágyi, L.; Haidegger, T.; Lehotsky, Á.; Nagy, M.; Csonka, E.A.; Sun, X.; Ooi, K.L.; Fisher, D. A large-scale assessment of hand hygiene quality and the effectiveness of the “WHO 6-steps”. BMC Infect. Dis. 2013, 13, 249. [Google Scholar] [CrossRef] [PubMed]
- Lehotsky, Á.; Szilágyi, L.; Ferenci, T.; Kovács, L.; Pethes, R.; Wéber, G.; Haidegger, T. Quantitative impact of direct, personal feedback on hand hygiene technique. J. Hosp. Infect. 2015, 91, 81–84. [Google Scholar] [CrossRef]
- Németh, I.A.K.; Nádor, C.; Szilágyi, L.; Lehotsky, Á.; Haidegger, T. Establishing a learning model for correct hand hygiene technique in a NICU. J. Clin. Med. 2022, 11, 4276. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.S.W.; Lee, J.K.F. The common missed handwashing instances and areas after 15 years of hand-hygiene education. J. Environ. Public Health 2019, 2019, 5928924. [Google Scholar] [CrossRef] [PubMed]
- Rotter, M.L. European norms in hand hygiene. J. Hosp. Infect. 2004, 56 (Suppl. 2), 6–9. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.G.; Gauthier, D.K.; Roby, J.R.; Larson, E.; Gauthier, J.J. Use of image analysis to measure handwashing effectiveness. Am. J. Infect. Control. 1994, 22, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Bánsághi, S.; Sári, V.; Szerémy, P.; Lehotsky, A.; Takács, B.; Tóth, B.K.; Haidegger, T. Evidence-based hand hygiene—Can you trust the fluorescent-based assessment methods? Acta Polytech. Hung. 2021, 18, 269–283. [Google Scholar] [CrossRef]
- Lee, J.Y.; Choi, J.W.; Kim, H. Determination of hand surface area by sex and body shape using alginate. J. Physiol. Anthropol. 2007, 26, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Frijlink, H.; Lagarce, F.; Touw, D.; Woerdenbag, H. Biopharmaceutics. Chapter 5. In Practical Pharmaceutics. An International Guideline for the Preparation, Care and Use of Medicinal Products, 2nd ed.; Le Brun, P., Crauste-Manciet, S., Krämer, I., Smith, J., Woerdenbag, H., Eds.; Springer Nature Switzerland: Cham, Switzerland, 2023; pp. 68–91. [Google Scholar] [CrossRef]
- Deochand, N.; Deochand, M.E. Brief report on hand-hygiene monitoring systems: A pilot study of a computer-assisted image analysis technique. J. Environ. Health 2016, 78, 14–21. [Google Scholar] [PubMed]
- Kampf, G.; Reichel, M.; Feil, Y.; Eggerstedt, S.; Kaulfers, P.M. Influence of rub-in technique on required application time and hand coverage in hygienic hand disinfection. BMC Infect. Dis. 2008, 8, 149. [Google Scholar] [CrossRef] [PubMed]
- Gerace, E.; Mancuso, G.; Midiri, A.; Poidomani, S.; Zummo, S.; Biondo, C. Recent advances in the use of molecular methods for the diagnosis of bacterial infections. Pathogens 2022, 11, 663. [Google Scholar] [CrossRef]
- Goyal, P.A.; Bankar, N.J.; Mishra, V.H.; Borkar, S.K.; Makade, J.G. Revolutionizing medical microbiology: How molecular and genomic approaches are changing diagnostic techniques. Cureus 2023, 15, e47106. [Google Scholar] [CrossRef]
- Banos, S.; Lentendu, G.; Kopf, A.; Wubet, T.; Glöckner, F.O.; Reich, M. A comprehensive fungi-specific 18S rRNA gene sequence primer toolkit suited for diverse research issues and sequencing platforms. BMC Microbiol. 2018, 18, 190. [Google Scholar] [CrossRef] [PubMed]
- Żukowska, M.E. Advanced methods of bacteriological identification in clinical microbiology laboratory. J. Pre-Clin. Clin. Res. 2021, 15, 68–72. [Google Scholar] [CrossRef]
- McCambridge, J.; Witton, J.; Elbourne, D.R. Systematic review of the Hawthorne effect: New concepts are needed to study research participation effects. J. Clin. Epidemiol. 2014, 67, 267–277. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hand Washing | Hand Disinfection | |||||
|---|---|---|---|---|---|---|
| Actions Correctly Executed | Met UV Requirement | Did Not Meet UV Requirement | Total | Met UV Requirement | Did Not Meet UV Requirement | Total |
| Adherent to the WHO 6-step protocol | 19 | 2 | 21 | 19 | 6 | 25 |
| Non-Adherent to the WHO 6-step protocol | 0 | 0 | 0 | 0 | 0 | 0 |
| Total | 19 (90%) | 2 (10%) | 21 (100%) | 19 (76%) | 6 (24%) | 25 (100%) |
| Type of Error | Number of Cleanroom Operators Making an Error | ||
|---|---|---|---|
| Hand Washing | Hand Disinfection | ||
| Met requirements | Zero missed areas | 17 | 17 |
| One minor, missed area (<0.6 cm2) | 1 | 2 | |
| Two minor, missed areas (<0.6 cm2) | 1 | 0 | |
| Did not meet requirements | More than two minor, missed areas (<0.6 cm2) | 1 | 0 |
| One or more major, missed areas (>0.6 cm2) | 1 | 6 | |
| Hand Washing | Hand Disinfection | ||
|---|---|---|---|
| Time (s) | Time (s) | ||
| Met requirements | Average | 101.6 (n = 18 *) | 67.9 (n = 16 *) |
| Median | 98.9 | 65.8 | |
| Minimum | 56.5 | 26.8 | |
| Maximum | 175.7 | 108.6 | |
| Standard deviation | 26.2 | 23.8 | |
| Interquartile range | 22.8 | 32.0 | |
| Did not meet requirements | Average | 123.5 (n = 2) | 67.5 (n = 5 **) |
| Median | - | 65.8 | |
| Minimum | 113.8 | 58.1 | |
| Maximum | 133.3 | 82.4 | |
| Standard deviation | 13.8 | 10.1 | |
| Interquartile range | - | 8.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knol, C.W.J.; Stob, P.H.; Woerdenbag, H.J. Development and Implementation of an Ultraviolet-Dye-Based Qualification Procedure for Hand Washing and Disinfection to Improve Quality Assurance of Pharmacy Preparations and Compounding, Especially in Cleanrooms: A Pilot Study. Pharmacy 2024, 12, 73. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy12030073
Knol CWJ, Stob PH, Woerdenbag HJ. Development and Implementation of an Ultraviolet-Dye-Based Qualification Procedure for Hand Washing and Disinfection to Improve Quality Assurance of Pharmacy Preparations and Compounding, Especially in Cleanrooms: A Pilot Study. Pharmacy. 2024; 12(3):73. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy12030073
Chicago/Turabian StyleKnol, Catharina W. J., Paul H. Stob, and Herman J. Woerdenbag. 2024. "Development and Implementation of an Ultraviolet-Dye-Based Qualification Procedure for Hand Washing and Disinfection to Improve Quality Assurance of Pharmacy Preparations and Compounding, Especially in Cleanrooms: A Pilot Study" Pharmacy 12, no. 3: 73. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy12030073