
The Short-Term Efficacy of a Three-Week Pulmonary Rehabilitation Program among Patients with Obstructive Lung Diseases
 and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Baseline Data Analysis
3.2. Assessment of the Effectiveness of the PR Program among Patients with Obstructive Lung Disease
3.3. Assessment of the Effectiveness of the PR Program among Patients with Asthma, COPD and COPD-A
3.3.1. Exercise Tolerance Analysis
3.3.2. Spirometry Parameters
3.3.3. Health-Related Quality of Life
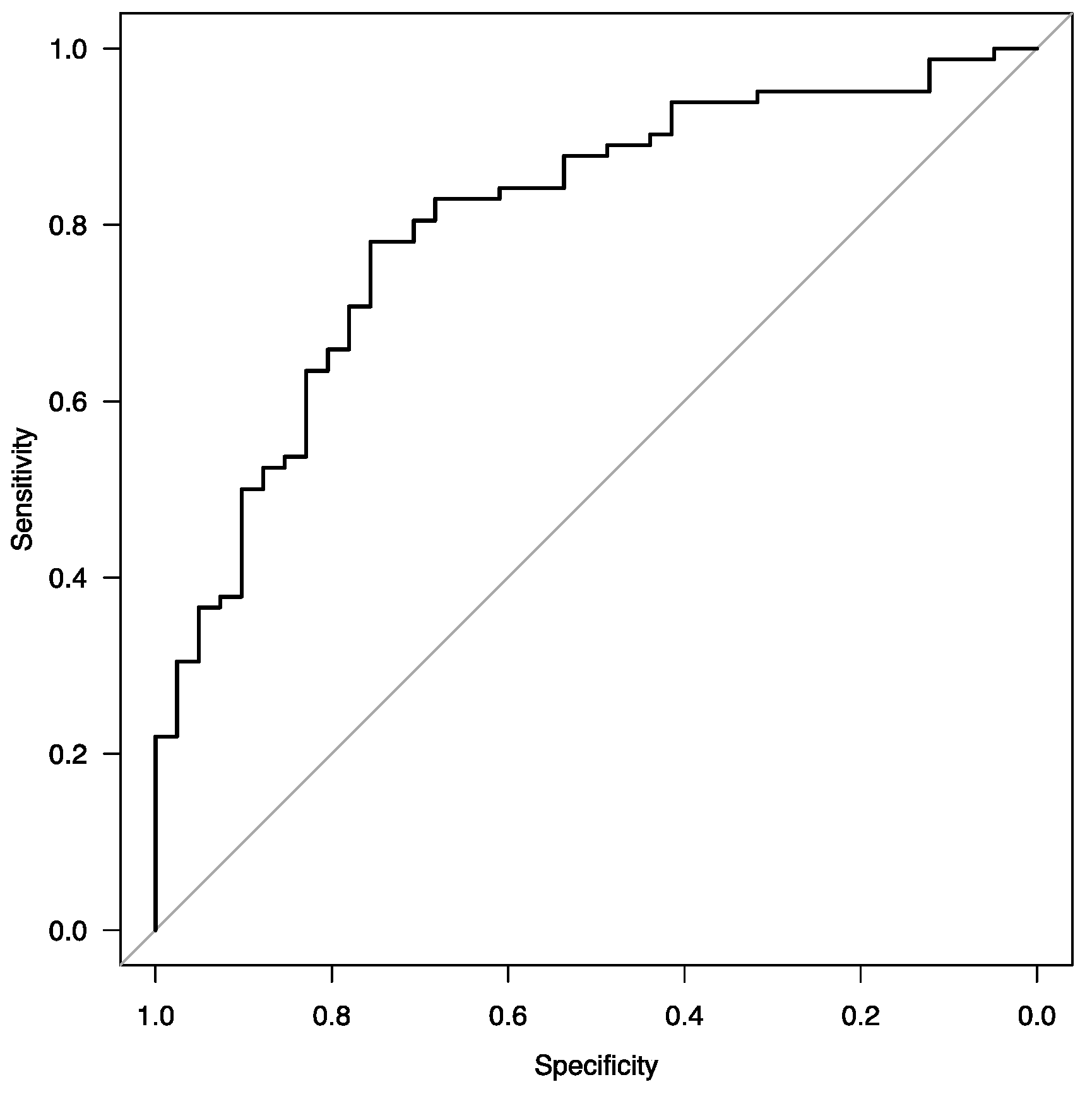
3.3.4. Improvement of Exercise Tolerance Expressed as a Significant Elongation of the Distance in 6 MWT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease, 2024 Report. Available online: www.goldcopd.org (accessed on 23 March 2024).
- Venkatesan, P. GOLD COPD Report: 2024 Update. Lancet Respir. Med. 2024, 12, 15–16. [Google Scholar] [CrossRef] [PubMed]
- Celli, B.R.; Wedzicha, J.A. Update on Clinical Aspects of Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2019, 381, 1257–1266. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. 2023. Available online: www.ginasthma.org (accessed on 23 March 2024).
- O’Byrne, P.M.; FitzGerald, J.M.; Bateman, E.D.; Barnes, P.J.; Zheng, J.; Gustafson, P.; Lamarca, R.; Puu, M.; Keen, C.; Alagappan, V.K.T.; et al. Effect of a Single Day of Increased As-Needed Budesonide-Formoterol Use on Short-Term Risk of Severe Exacerbations in Patients with Mild Asthma: A Post-Hoc Analysis of the SYGMA 1 Study. Lancet Respir. Med. 2021, 9, 149–158. [Google Scholar] [CrossRef]
- Patadia, R.; Casale, T.B.; Fowler, J.; Patel, S.; Cardet, J.C. Advancements in Biologic Therapy in Eosinophilic Asthma. Expert Opin. Biol. Ther. 2024. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.E.; Wadell, K.; Spruit, M.A. How to Adapt the Pulmonary Rehabilitation Programme to Patients with Chronic Respiratory Disease Other than COPD. Eur. Respir. Rev. Off. J. Eur. Respir. Soc. 2013, 22, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Zampogna, E.; Zappa, M.; Spanevello, A.; Visca, D. Pulmonary Rehabilitation and Asthma. Front. Pharmacol. 2020, 11, 542. [Google Scholar] [CrossRef] [PubMed]
- Türk, Y.; Theel, W.; van Huisstede, A.; van de Geijn, G.-J.M.; Birnie, E.; Hiemstra, P.S.; Sont, J.K.; Taube, C.; Braunstahl, G.-J. Short-Term and Long-Term Effect of a High-Intensity Pulmonary Rehabilitation Programme in Obese Patients with Asthma: A Randomised Controlled Trial. Eur. Respir. J. 2020, 56, 1901820. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, N.; Senjyu, H.; Tanaka, T.; Asai, M.; Yanagita, Y.; Yano, Y.; Nishinakagawa, T.; Kotaki, K.; Kitagawa, C.; Rikitomi, N.; et al. Pulmonary Rehabilitation Improves Exercise Capacity and Dyspnea in Air Pollution-Related Respiratory Disease. Tohoku J. Exp. Med. 2014, 232, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Salandi, J.; Icks, A.; Gholami, J.; Hummel, S.; Schultz, K.; Apfelbacher, C.; Sheikh, A.; Loerbroks, A. Impact of Pulmonary Rehabilitation on Patients’ Health Care Needs and Asthma Control: A Quasi-Experimental Study. BMC Pulm. Med. 2020, 20, 267. [Google Scholar] [CrossRef] [PubMed]
- Schultz, K.; Seidl, H.; Jelusic, D.; Wagner, R.; Wittmann, M.; Faller, H.; Nowak, D.; Schuler, M. Effectiveness of Pulmonary Rehabilitation for Patients with Asthma: Study Protocol of a Randomized Controlled Trial (EPRA). BMC Pulm. Med. 2017, 17, 49. [Google Scholar] [CrossRef] [PubMed]
- Puhan, M.A.; Spaar, A.; Frey, M.; Turk, A.; Brändli, O.; Ritscher, D.; Achermann, E.; Kaelin, R.; Karrer, W. Early versus Late Pulmonary Rehabilitation in Chronic Obstructive Pulmonary Disease Patients with Acute Exacerbations: A Randomized Trial. Respir. Int. Rev. Thorac. Dis. 2012, 83, 499–506. [Google Scholar] [CrossRef]
- Franssen, F.M.E.; Rochester, C.L. Comorbidities in Patients with COPD and Pulmonary Rehabilitation: Do They Matter? Eur. Respir. Rev. 2014, 23, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Hu, D.; Xu, Y.; Wu, L.; Lou, L. Effect of Pulmonary Rehabilitation in Patients with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Ann. Med. 2022, 54, 262–273. [Google Scholar] [CrossRef] [PubMed]
- Gibson, P.G.; McDonald, V.M. Asthma-COPD Overlap 2015: Now We Are Six. Thorax 2015, 70, 683–691. [Google Scholar] [CrossRef]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.-C.; et al. An Official American Thoracic Society/European Respiratory Society Statement: Key Concepts and Advances in Pulmonary Rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef] [PubMed]
- Langhammer, A.; Johannessen, A.; Holmen, T.L.; Melbye, H.; Stanojevic, S.; Lund, M.B.; Melsom, M.N.; Bakke, P.; Quanjer, P.H. Global Lung Function Initiative 2012 Reference Equations for Spirometry in the Norwegian Population. Eur. Respir. J. 2016, 48, 1602–1611. [Google Scholar] [CrossRef] [PubMed]
- Resnik, L.; Borgia, M. Reliability of Outcome Measures for People with Lower-Limb Amputations: Distinguishing True Change from Statistical Error. Phys. Ther. 2011, 91, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An Official European Respiratory Society/American Thoracic Society Technical Standard: Field Walking Tests in Chronic Respiratory Disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef] [PubMed]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories ATS Statement: Guidelines for the Six-Minute Walk Test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [CrossRef] [PubMed]
- Mahler, D.A.; Rosiello, R.A.; Harver, A.; Lentine, T.; McGovern, J.F.; Daubenspeck, J.A. Comparison of Clinical Dyspnea Ratings and Psychophysical Measurements of Respiratory Sensation in Obstructive Airway Disease. Am. Rev. Respir. Dis. 1987, 135, 1229–1233. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.W.; Quirk, F.H.; Baveystock, C.M.; Littlejohns, P. A Self-Complete Measure of Health Status for Chronic Airflow Limitation. The St. George’s Respiratory Questionnaire. Am. Rev. Respir. Dis. 1992, 145, 1321–1327. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria; Available online: https://www.r-project.org/ (accessed on 29 February 2024).
- Beauchamp, M.K.; Janaudis-Ferreira, T.; Goldstein, R.S.; Brooks, D. Optimal Duration of Pulmonary Rehabilitation for Individuals with Chronic Obstructive Pulmonary Disease—A Systematic Review. Chron. Respir. Dis. 2011, 8, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Abramson, M.J.; Crockett, A.J.; Frith, P.A.; McDonald, C.F. COPDX: An Update of Guidelines for the Management of Chronic Obstructive Pulmonary Disease with a Review of Recent Evidence. Med. J. Aust. 2006, 184, 342–345. [Google Scholar] [CrossRef] [PubMed]
- Greulich, T.; Koczulla, A.R.; Nell, C.; Kehr, K.; Vogelmeier, C.F.; Stojanovic, D.; Wittmann, M.; Schultz, K. Effect of a Three-Week Inpatient Rehabilitation Program on 544 Consecutive Patients with Very Severe COPD: A Retrospective Analysis. Respir. Int. Rev. Thorac. Dis. 2015, 90, 287–292. [Google Scholar] [CrossRef] [PubMed]
- von Leupoldt, A.; Hahn, E.; Taube, K.; Schubert-Heukeshoven, S.; Magnussen, H.; Dahme, B. Effects of 3-Week Outpatient Pulmonary Rehabilitation on Exercise Capacity, Dyspnea, and Quality of Life in COPD. Lung 2008, 186, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Szafraniec, R.; Jozefowski, P.; Chojnowska, A. The Effect of 3-Week Sanatorium Rehabilitation on Exercise Capacity and Subjective Perception of Health of Patients with Asthma and COPD. Balt. J. Health Phys. Act. 2016, 8, 20–25. [Google Scholar] [CrossRef]
- Schultz, K.; Wittmann, M.; Wagner, R.; Lehbert, N.; Schwarzkopf, L.; Szentes, B.; Nowak, D.; Faller, H.; Schuler, M. In-Patient Pulmonary Rehabilitation to Improve Asthma Control–A Randomized Controlled Study (EPRA, Effectiveness of Pulmonary Rehabilitation for Patients with Asthma). Dtsch. Arzteblatt Int. 2021, 118, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Schneeberger, T.; Jarosch, I.; Moll, J.; Gloeckl, R.; Boensch, M.; Hitzl, W.; Idzko, M.; Taube, C.; Kenn, K.; Koczulla, A.R. Increased Asthma Control after a 3-Week Inpatient Pulmonary Rehabilitation Program. Respir. Med. 2020, 165, 105930. [Google Scholar] [CrossRef] [PubMed]
- Orooj, M.; Moiz, J.A.; Mujaddadi, A.; Ali, M.S.; Talwar, D. Effect of Pulmonary Rehabilitation in Patients with Asthma COPD Overlap Syndrome: A Randomized Control Trial. Oman Med. J. 2020, 35, e136. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameter | COPD N = 37 | Asthma N = 61 | COPD-A N = 27 | Total N = 125 | p-Value |
|---|---|---|---|---|---|
| Age, years, median [IQR] Male sex, n (%) BMI, kg/m2, median [IQR] | 71 [64–77] 24 (64.86) 24.7 [20.41–29.76] | 69 [63–75] 13 (21.31) 27.9 [24.85–33.3] | 70 [62–77] 11 (40.74) 27.52 [21.97–29.3] | 70 [63–76] 48 (38.4) 26.33 [22.2–30.88] | 0.58 <0.0001 0.02 |
| Comorbidities Arterial hypertension Heart failure, n (%) History of MI, n (%) Diabetes mellitus type 2, n (%) Obesity, n (%) Cachexia, n (%) Chronic kidney disease, n (%) History of malignancy, n (%) History of stroke, n (%) | 24 (64.86) 15 (40.54) 3 (8.11) 11 (29.73) 9 (24.32) 2 (5.41) 1 (2.7) 6 (16.22) 1 (2.7) | 44 (72.13) 23 (37.7) 5 (8.2) 18 (29.51) 22 (36.07) 2 (3.28) 1 (1.63) 3 (4.92) 7 (11.48) | 20 (74.07) 9 (33.33) 5 (18.52) 7 (25.93) 5 (18.52) 2 (7.4) 2 (7.4) 5 (18.52) 0 (0) | 88 (70.4) 47 (37.6) 13 (10.4) 36 (28.8) 36 (28.8) 6 (4.8) 4 (3.2) 14 (11.2) 8 (6.4) | 0.67 0.84 0.32 0.94 0.22 0.65 0.33 0.08 0.09 |
| Disease-specific scales CAT, points, mean (SD) GINA-SCT, points, median [IQR] mMRC, points, median [IQR] | 22.07 (5.11) - 2 [2–3] | - 3 [1–3.25] 2 [1–3] | 25.55 (6.47) 3 [3–4] 3 [2–3] | 23.54 (5.87) 3 [2–4] 2 [2–2] | 0.14 0.07 0.04 |
| 6 MWT Distance, m, mean (SD) Δ SpO2, %, median [IQR] | 330.14 (80.89) 0 [−1–2] | 318.9 (84.31) 0 [−1–2] | 311.11 (89.41) 0 [−1–1.5] | 320.47 (84.07) 0 [−1–2] | 0.66 0.86 |
| Spirometry FEV1, %, median [IQR] FVC, %, mean (SD) FEV1/FVC, median [IQR] | 44 [33–52.5] 69.06 (13.89) 48.18 [44.24–53.82] | 81 [65–94] 80.85 (22.04) 77.29 [70–81.59] | 36 [24.5–48] 62.04 (19.71) 47.19 [40.73–54.56] | 56 [39.75–81] 73.33 (20.87) 61.7 [48.16–77.27] | <0.0001 0.0001 <0.0001 |
| SGRQ total, points, mean (SD) impact, points, mean (SD) symptoms, points, mean (SD) activity, points median [IQR] | 61.59 (14.28) 54.56 (20.02) 63.25 (15.18) 73.02 [59.46–79.67] | 52.95 (17.23) 44.89 (20.89) 54.19 (19.44) 66.19 [59.46–79.67] | 65.29 (15.43) 56.19 (20.87) 61.41 (14.28) 85.82 [78.98–92.51] | 58.09 (16.77) 50.11 (21.13) 58.37 (17.65) 72.44 [59.46–85.87] | 0.002 0.02 0.03 0.0001 |
| Parameter | Kruskal-Wallis Chi-Squared (p-Value) |
|---|---|
| Disease-specific scales Δ CAT, points Δ GINA-SCT, points Δ mMRC, points | 0.53 (p = 0.46) 0.18 (p = 0.67) 1.01 (p = 0.6) |
| 6 MWT Δ Distance, m | 2.98 (p = 0.23) |
| Spirometry Δ FEV1, % Δ FVC, % | 4.68 (p = 0.1) 3.97 (p = 0.14) |
| SGRQ Δ total, points Δ impact, points Δ symptoms, points Δ activity, points | 1.34 (p = 0.51) 0.57 (p = 0.75) 5.13 (p = 0.08) 1.73 (p = 0.42) |
| Parameter | COPD | Asthma | COPD-A | |||
|---|---|---|---|---|---|---|
| Pre-PR | Post-PR | Pre-PR | Post-PR | Pre-PR | Post-PR | |
| Disease-specific scales CAT, points, mean (SD) GINA-SCT, points, median [IQR] mMRC, points, median [IQR] | 22.07 (5.11) - 2 [2–3] | 16.93 *** (5.6) - 1 **** [1–2] | - 3 [1–3.25] 2 [1–3] | - 0.5 ** [0–1.25] 1 **** [0–1] | 25.55 (6.47) 3 [3–4] 3 [2–3] | 18.91 ** (7.94) 2 * [1–3.75] 1 ** [0.5–2] |
| 6 MWT Distance, m, mean (SD) Δ SpO2, %, median [IQR] | 330.14 (80.89) 0 [–1–2] | 388.58 **** (74.92) 1 [−0.25–3] | 318.9 (84.31) 0 [–1–2] | 403.84 **** (98.65) 1 [0–2] | 311.11 (89.41) 0 [−1–1.5] | 378.41 **** (95.12) 1 [−0.5–2.5] |
| Spirometry FEV1, %, median [IQR] FVC, %, mean (SD) FEV1/FVC, median [IQR] | 44 [33–52.5] 69.06 (13.89) 48.18 [44.24–53.82] | 43 [35–56] 71.46 (16.86) 48.57 [42.01–54.49] | 81 [65–94] 80.85 (22.04) 77.29 [70–81.59] | 86 ** [73–98] 87.49 *** (20.65) 76.85 [71.02–81.88] | 36 [24.5–48] 62.04 (19.71) 47.19 [40.73–54.56] | 43 ** [33.5–57.5] 70.52 ** (20.17) 46.23 [42.46–57.41] |
| SGRQ total, points, mean (SD) impact, points, median [IQR] symptoms, points, median [IQR] activity, points, median [IQR] | 61.59 (14.28) 55.38 [41.41–69.16] 63.12 [53.12–76.01] 73.02 [59.46–79.67] | 49.63 **** (18.11) 39.6 *** [23.04–58.65] 42.24 *** [24.56–59.9] 66.1 * [48.05–79.27] | 52.95 (17.23) 44.36 [28.12–61.49] 52.64 [40.71–68.94] 66.19 [59.46–79.67] | 37.97 **** (21.96) 25.83 *** [11.98–52.35] 34.1 **** [16.76–53.87] 59.3 **** [35.29–66.31] | 65.29 (15.43) 52.18 [44.01–72.13] 60.56 [54.89–72.69] 85.82 [78.98–92.51] | 50.51 *** (21.13) 42.5 ** [23.95–57.78] 43.86 ** [29.19–65.46] 72.76 ** [54.74–85.54] |
| Parameter | Odds Ratio (95%CI) | p-Value |
|---|---|---|
| Univariable Age Sex BMI Overweight Obesity Arterial hypertension Heart failure History of MI Diabetes mellitus type 2 Chronic kidney disease History of malignancy History of stroke CAT GINA-SCT mMRC primary distance in 6 MWT Δ SpO2 in 6 MWT %FEV1 %FVC FEV1/FVC SRGQ—total SRGQ—impact SRGQ—symptoms SRGQ—activity | 0.96 (0.92–1.01) 0.65 (0.31–1.39) 0.93 (0.88–0.99) 2.54 (1.08–6.00) 0.44 (0.2–0.97) 0.54 (0.23–1.27) 0.53 (0.25–1.13) 0.79 (0.24–2.58) 0.72 (0.32–1.61) 0.49 (0.06–3.64) 0.62 (0.2–1.93) 0.83 (0.19–3.67) 1.02 (0.88–1.18) 1.08 (0.62–1.86) 0.85 (0.55–1.32) 1.0 (0.99–1.0) 1.03 (0.9–1.17) 1.01 (1.0–1.03) 1.02 (1.0–1.04) 1.01 (0.98–1.03) 0.99 (0.97–1.01) 0.99 (0.97–1.01) 0.99 (0.97–1.01) 1.01 (0.99–1.02) | 0.08 0.27 0.03 0.03 0.04 0.16 0.1 0.7 0.43 0.49 0.41 0.81 0.81 0.79 0.5 0.18 0.7 0.12 0.03 0.58 0.32 0.22 0.26 0.59 |
| Multivariable primary distance in 6 MWT %FVC Age BMI Overweight Obesity | 0.99 (0.98–0.997) 1.04 (1.01–1.06) 0.92 (0.86–0.97) 0.78 (0.65–0.94) 10.6 (2.18–51.5) 14 (0.96–203) | 0.004 0.004 0.004 0.008 0.003 0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klimczak, M.K.; Krzepkowski, H.A.; Piotrowski, W.J.; Białas, A.J. The Short-Term Efficacy of a Three-Week Pulmonary Rehabilitation Program among Patients with Obstructive Lung Diseases. J. Clin. Med. 2024, 13, 2576. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092576
Klimczak MK, Krzepkowski HA, Piotrowski WJ, Białas AJ. The Short-Term Efficacy of a Three-Week Pulmonary Rehabilitation Program among Patients with Obstructive Lung Diseases. Journal of Clinical Medicine. 2024; 13(9):2576. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092576
Chicago/Turabian StyleKlimczak, Magdalena K., Hubert A. Krzepkowski, Wojciech J. Piotrowski, and Adam J. Białas. 2024. "The Short-Term Efficacy of a Three-Week Pulmonary Rehabilitation Program among Patients with Obstructive Lung Diseases" Journal of Clinical Medicine 13, no. 9: 2576. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092576