
Elasticity of the Cervix in Relation to Uterus Position


1
Teaching Unit of Obstetrics and Gynecology, IRCCS Ospedale San Martino of Genova, 16132 Genova, Italy
2
Department of Neurology, Rehabilitation, Ophthalmology, Genetics, Maternal and Infant Health (DiNOGMI), University of Genova, 16132 Genoa, Italy
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2024, 13(9), 2572; https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092572
Submission received: 31 March 2024
/
Revised: 23 April 2024
/
Accepted: 26 April 2024
/
Published: 27 April 2024
(This article belongs to the Section Obstetrics & Gynecology)
Abstract
:Strain elastography allows the evaluation of tissue elasticity. Background/Objectives: Tissue elasticity depends on the content and distribution of collagen fibers and is shaped by the applied tensile forces that may differ in uteri with a different angle of flexion of the corpus on the cervix. The objective was to investigate whether the angle of uterine flexion is related to cervical tissue elasticity. Methods: The anterior angle between the longitudinal axis of the uterus corpus and that of the cervix was measured in 275 non-pregnant young women by transvaginal ultrasonography and considered both as an absolute value or categorized as ≤150°, between >150° and ≤210°, and >210°. Strain elastography was used to assess tissue elasticity by placing the probe in the anterior vaginal fornix. Tissue elasticity was evaluated in the middle of the anterior cervical compartment (ACC), in the middle of the posterior cervical compartment (PCC), in the middle portion of the cervical canal (MCC), and at the internal cervical os (ICO). In a sagittal plane MCC was evaluated across the cervical canal, and ACC and PCC at a distance equal between the cervical canal and the outer anterior or posterior part of the cervix. MCC, ACC and PCC were evaluated at equal distance between the ICO and the external cervical os. Elasticity was expressed as a color score ranging from 0.1 (low elasticity) to 3 (high elasticity). Results: The angle of uterine flexion show a negative linear relation with the elasticity of the ACC (p = 0.001) and MCC (p = 0.002) and a positive relation with the elasticity of the PCC (p = 0.054). In comparison to uteri with an angle of flexion of <150°, those with an angle of flexion of >210° had lower elasticity of the ACC (p = 0.001) and MCC (p = 0.001) and higher elasticity of the PCC (p = 0.004). The ACC/PCC and PCC/MCC elasticity ratios were also significantly different (p = 0.001). Conclusions: The angle of uterine flexion is associated with changes in cervix elasticity. Retroflexion is associated with stiffer ACC and MCC and a more elastic PCC. Differences in tissue elasticity suggest structural changes of the cervix that may have implication in variate obstetric and gynecological conditions.
Keywords:
retroversion; retroflexion; elastography; cervix; stiffness; cervix structure; uterine flexion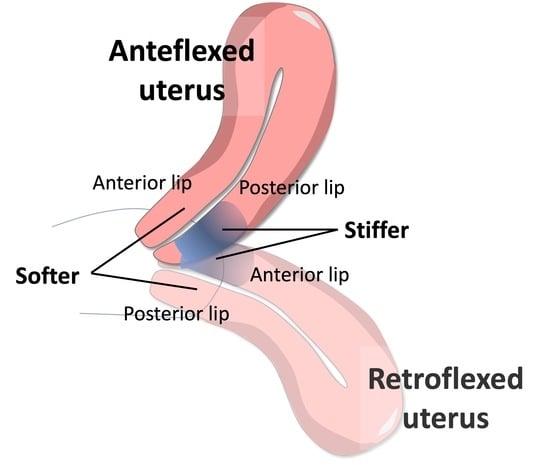
1. Introduction
The uterine cervix comprises collagen fibers, ground matrix, and a substantial amount of muscle at the internal os, which gradually diminishes towards the external os [1,2,3]. According to biochemical data, imaging techniques, and mathematical models, the quantity and direction of collagen fibers change throughout the cervix [4,5], most likely due to the action of various tensile and dilatative forces [6,7]. Fiber distribution characterizes the capability of the cervix to resist to both dilatative and compressive forces [6]. During pregnancy, specific areas, such as the internal cervical os and possibly the upper posterior cervix, receive [8,9] and counteract [5,9] the fetus’s tensile and dilatative forces. Collagen fibers play an essential role in maintaining cervix competence, and when they decrease and disperse, cervix dilation may occur [2,5,10]. Changes in these processes can result in preterm birth or prolonged labor [11,12]. Because of differences in tensile forces exerted by the uterosacral and cardinal ligaments [6,7,11] or by the uterus corpus [13], the direction and quantity of collagen fibers of the cervix may differ in uteri with different positions. Along with ground matrix, the amount and direction of collagen fibers, determine tissue elasticity [2,10,14]. Strain elastography (SE) is an ultrasonographic technique for determining tissue elasticity [12,15,16,17,18], and it has been widely used to assess the elastography characteristics of cervix in both pregnant [16,19,20,21,22] and non-pregnant [23,24] women. In this study we evaluated whether the elastography characteristics of the cervix change with different uterine positions. Ligaments that maintain the uterus within the pelvis are essentially the uterosacral ligaments, and, to less extent, the cardinal ligaments that produce an elastic bounding of the cervix within the pelvis, while the round ligaments create an elastic bounding aimed to maintain the uterus corpus in its position. There are physiological variants of uterine positions, that can be described by uterine version and uterine flexion. Version is defined by the relation between the longitudinal axis of the uterus and that of the vagina, while flexion is defined by the anterior angle between the longitudinal axis of the uterine corpus and the longitudinal axis of the cervix [25,26]. In general, anteversion and retroversion indicate a uterus that forms an anterior angle with the vagina 180° < or > to 180°, respectively. The angle of flexion is in general expressed as a continuous value, and in clinical studies it was also categorized as an angle < 150°, to identify strong anteflexion, between 150 and 210° to identify no marked flexion, and >210°, to indicate a strong retroflexion [25,26]. The different angles of flexion were associated with a different intensity of menstrual pain [25], and a different risk of adenomyosis [26]. Determinants of uterine position are still elusive, but the tensile forces exerted by external ligaments and by the uterine corpus in uteri of different position can possibly determine a different structure of the cervix. This study aimed to evaluate whether the angle of uterine flexion is related to changes in the elastography characteristics of the cervix.
2. Materials and Methods
The local ethical committee approved this observational study (CER Liguria 123/2022) that was performed on 275 premenopausal women of the outpatient services of infertility and chronic pelvic pain at a university hospital. Each woman signed an informed consent form authorizing the anonymous use of her clinical data in scientific publications, and she was managed per standard clinical practice. Data were collected in an electronic database and then anonymously retrieved and analyzed.
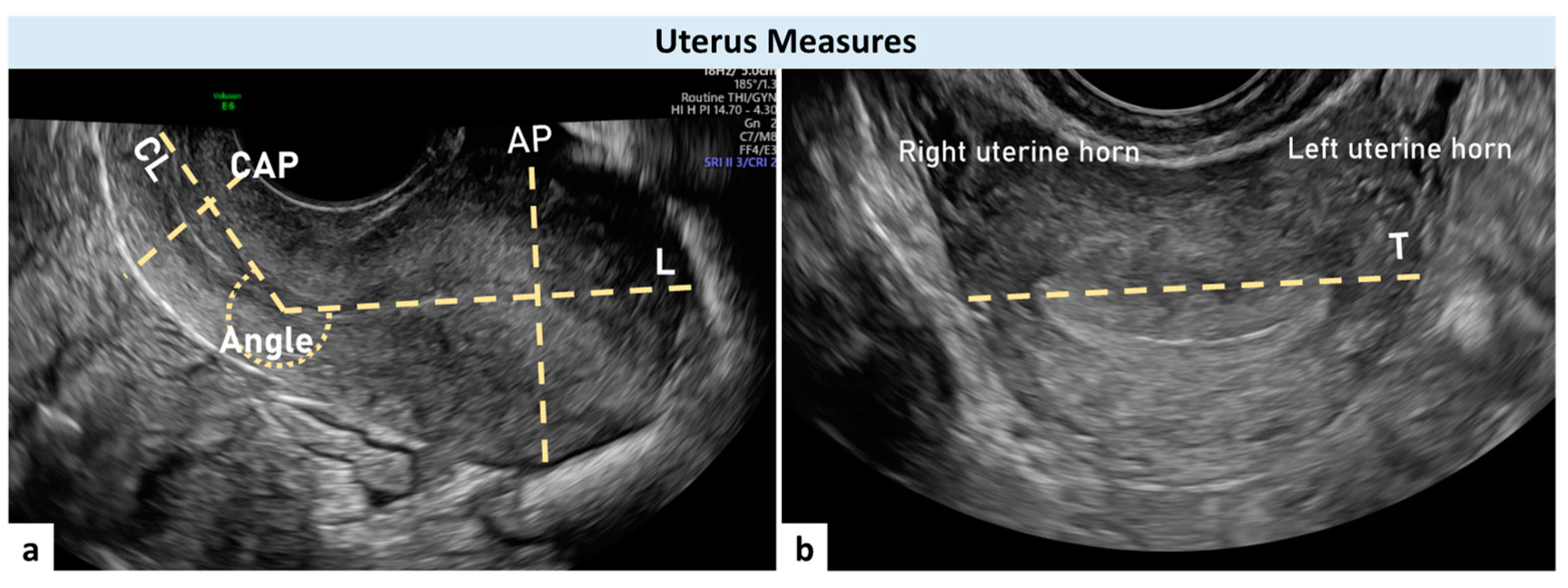
For each woman, we collected general characteristics and clinical data. The presence of gynecological diseases was evaluated by patient history, bimanual examination, and transvaginal ultrasonography. The ultrasound investigation was performed by a single experienced sonographer (A.X.) using a GE E6 (GE Medical Systems, Zipf, Austria) ultrasound machine equipped with a wideband 5–9 MHz intravaginal transducer and proper software for elastography (Voluson E6 BT16, GE Medical System, Zipf, Austria). Longitudinal (L), transverse (T), and antero-posterior (AP) measures of the uterus, length (CL) and diameter (CD) of the cervix, and degrees of the angle of flexion of the uterus on the cervix were obtained during the ultrasound examination. The anterior angle between the cervix’s longitudinal axis and the uterine body’s longitudinal axis was measured with an empty bladder (Figure 1). Three measures were recorded for each patient, and the mean of the three was used in subsequent analyses. The volume of the uterus was calculated by the ultrasound machine based on the formula (L × T × AP × 0.5223) and that of the cervix by the cylinder formula (CL × [CT/2] × 3.14). The uterine L and AP measures were taken in a sagittal plane, with the entire endometrial cavity visible. L was measured between the internal cervical os (ICO) and the more prominent aspect of the fundus; AP measure was estimated perpendicular to L, with the calipers placed at the most prominent parts of the uterus corpus from the anterior to posterior wall serosa. T was measured in a transverse plane (by rotating the vaginal probe 90° and placing the calipers from serosa to serosa at the Fallopian tube insertion) (Figure 1).
The longitudinal cervix diameter was calculated as a line drawn between the ICO and the external cervical os (ECO). The cervix antero-posterior and transverse diameters were calculated as two orthogonal lines drawn at the mid-cervix on their respective planes. For statistical purposes, the mean of the two was used as the cervix diameter (CD) (Figure 1). The ICO was defined as the point at which the endometrium disappears, and the cervical canal begins. SE analysis was performed in a sagittal plane view with the probe directed almost perpendicular to the cervical canal (Figure 2) [16,19,24].
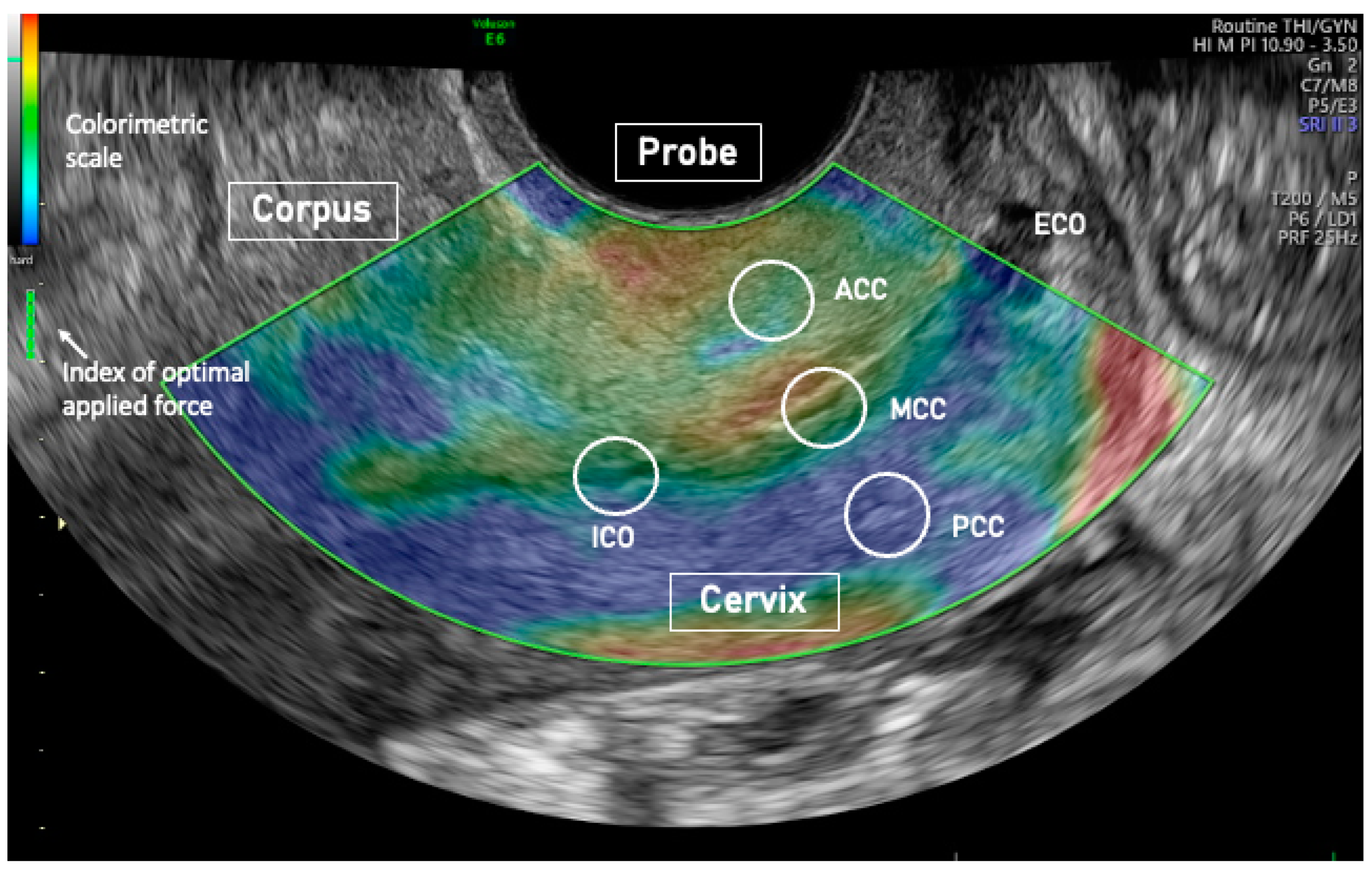
SE was used to evaluate tissue elasticity. SE evaluates differences in elasticity of different regions of interest (ROIs) [13,14] by measuring tissue deformation or displacement generated by the applied pressure. The procedure was already described elsewhere [24]. During image acquisition, vaginal probe was positioned in the anterior vaginal fornix and displayed alongside to facilitate images interpretation [26]. A series of about 5 compression and decompression cycles, using sub-centimetric excursions, were applied perpendicular to the axis of the cervical canal [16,19,24] (Figure 2). Optimal compression force was identified in real time by a control bar of the ultrasound processing program. Analyses were recorded on clips and analyzed afterward. ROIs with a circular area of 19.6 mm2 were placed in the middle of the anterior cervical compartment (ACC), in the middle of the posterior cervical compartment (PCC), in the middle portion of the cervical canal (MCC), and at the ICO of the cervix. In a sagittal plane, ROIs were placed at equal distances from the internal and external cervical os (Figure 2). The MCC ROI was placed across the cervical canal, and the ACC and PCC were seated at a distance equal between the cervical canal and the outer anterior or posterior part of the cervix. Strain results were calculated at optimal compression force defined by the elastography software (General electrics Company, Boston, MA, USA) (Figure 2). Three independent scorers coded tissue elasticity using a colorimetric scale ranging from violet/blue (low elasticity) to red (high elasticity), with yellow/green serving as intermediate values. The scorers assigned values to each ROI analysis across the entire colorimetric spectrum from 0.1 = blue/violet to 3.0 = red. SE analysis inter-operator ICC agreement was 0.93 (95% CI 0.89,0.96). The average of the 3 scorers’ scores was used. We used univariate and multiple linear regression analyses to examine the relationship between the angle of flexion of the uterus on the cervix (dependent variable) and independent variables such as woman age, age at menarche, body mass index (BMI), number of at-term pregnancies and deliveries, uterus and cervix measurements, ROIs elasticity, and the calculated ratio of ROIs elasticities. Only the independent variables that in simple regression analysis were related to the dependent variable (up to a p value of 0.2) were entered into the multiple regression models. In the multiple regression models the variables that were not significantly associated with the dependent variable were gradually eliminated, beginning with the least relevant, to finally preserve only those variables that were independently related to the dependent variable. As previously performed in studies on menstrual pain [25] and adenomyosis [26], the angle of flexion of the uterus on the cervix was also categorized as ≤150°, between >150° and ≤210°, and >210°.
To compare means from different groups, one-way ANOVA (analysis of variance) was used, followed by Fisher’s Least Significant Difference post hoc test. Statview 5.1 was used to conduct statistical analyses (SAS Institute Inc., Cary, NC, USA). The normality of continuous variables was tested with the Kolmogorow-Smirnoff test. The information is presented as a mean and standard deviation (SD), and a p-value < 0.05 was considered statistically significant.
3. Results
Clinical characteristics and measures of the uterus, of the included women, are reported in Table 1.
3.1. Elasticity of the Cervix
Cervical tissue was not homogeneous, and elasticity progressively increased from the ICO, the PCC, the ACC, and the MCC (Table 1). The angle of flexion was positively related to PCC elasticity (p = 0.001), to PCC/MCC elasticity ratio (p = 0.001), and negatively, to ACC elasticity (p = 0.001) and ACC/PCC elasticity ratio (p = 0.001) (Table 2). In addition, the angle of uterine flexion was related to age (p = 0.036), uterus volume (p = 0.009), AP (p = 0.001), T (p = 0.018), and the ratio AP/cervix diameter (p = 0.001) (Table 2).
3.2. Multiple Regression Models
Three models were calculated by multiple regression analyses (Table 3).
In Model 1, we entered only the variables significantly related to the angle of uterine flexion. In this calculation (R2 = 0.116), an independent negative relation with the angle of uterine flexion were found for ACC elasticity (p = 0.001), and cervix diameter (p = 0.037) and a positive relation with AP measure of the uterus (p = 0.001). In model 2 measures of the uterus and cervix were included as single variable represented by the ratio of the uterus AP measure/cervix diameter. In this model (R2 = 0.124), the angle of flexion was negatively related to the color score of the ACC (p = 0.001), and positively related to the ratio of the uterus AP measure/cervix diameter (p = 0.001). In model 3, we included the ratio of elasticity of different ROIs. The model achieved a slightly higher relation between dependent and independent variables (R2 = 0.163). The angle of uterine flexion remained positively related to the uterus AP measure/cervix diameter (p = 0.001), and the elasticity ratio of the PCC/MCC (p = 0.001).
3.3. Data Stratification by Angle of Uterine Flexion
Among included women 213 (77.4%) had an angle of flexions ≤150°, 21 (7.6%) women an angle of flexion between >150° and ≤210°, and 41 (14.9%) an angle of flexion >210°. Parameters that were significantly different among these groups are reported in Table 4. In comparison to uteri with an angle of flexion ≤150°, those with an angle of flexion >210° had a significantly higher PCC elasticity (p = 0.004) and lower diameter of the cervix (p = 0.009). Conversely, ACC (p = 0.001) and MCC (p = 0.001) elasticities were lower. The elasticity ratio of the ACC/PCC and the PCC/MCC were also significantly different between uteri with an angle of flexion >210° and ≤150° (p = 0.001) (Figure 3 and Figure 4).
4. Discussion
4.1. Principal Findings
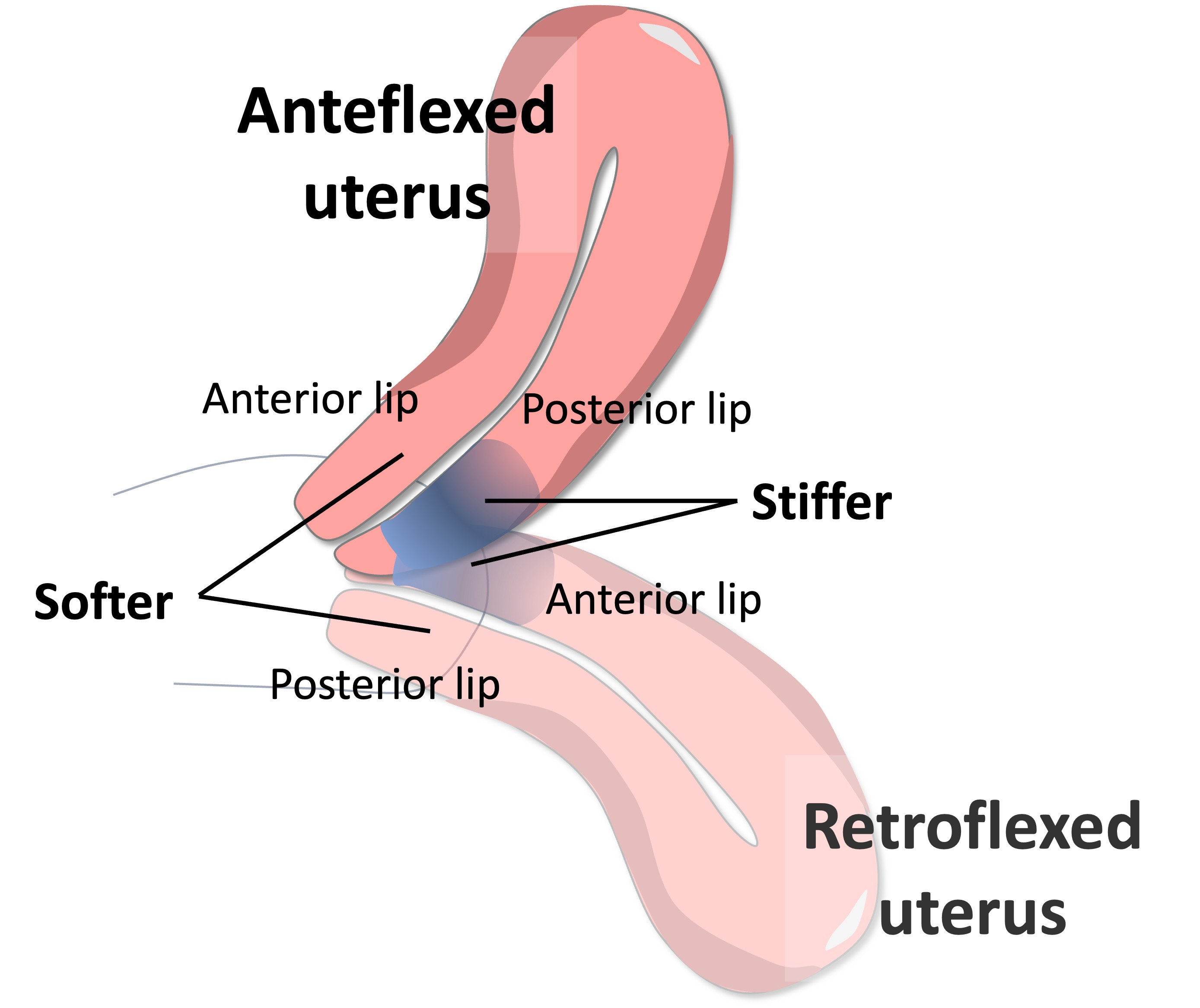
The angle of uterine flexion seems to be related to elasticity changes in some areas of the cervix like the ACC, the PCC, and the MCC. Data stratification clearly shows that in comparison to an anteflexed, a retroflexed uterus has a stiffer ACC and MCC and a softer PCC (Figure 4).
4.2. Results in the Context of What Is Known
Ground matrix, collagen fibers, and their grade of anisotropy determines tissue stiffness [2,10,14]. It is unclear which component is mostly modified in relation to the angle of uterine flexion, but the data strongly suggest that the ACC, the PCC, and the MCC structures are different in uteri with different angles of flexion.
4.3. Clinical Implications
It is unknown whether the difference in cervix elasticity is primary or secondary to the angle of flexion. In the first case, it indicates that women may have a primitive difference in the structure of their cervix that influences the angle of flexion of their uterus. Thus, changing this angle artificially through surgery [27,28,29] or possibly during pregnancy may not affect the structure of the cervix. In contrast, whether the cervix structure is secondary to the angle of flexion, i.e., shaped temporarily by differences in external or internal tensile forces, artificial modification of the angle may result in cervical structural changes. A different structure of the cervix may have implications in pregnancy, anteflexed uteri possibly responding differently to dilatative forces than retroflexed uteri. This possibility would deserve dedicated studies to be investigated.
4.4. Research Implications
Published investigations on cervix structure based on histology, imaging techniques, and mathematical models never considered the position of the uterus as a confounding factor [1,2,3,4,5,6,7,8,9,10]. Future studies need to incorporate the angle of flexion of the uterus among the variables that may influence the results. The possible implications of a different composition of the cervix linked to the angle of flexion should be considered in association with different obstetrics and gynecological disturbances and pathologies. It was already reported that a higher variance of ROIs elasticity of the cervix or a different angle of uterine flexion is associated with menstrual pain [24,25] risk of adenomyosis [26,30] and infertility [23]. Furthermore, some evidence indicates that during pregnancy, the angle of flexion may be related to preterm birth [31].
4.5. Strengths and Limitations
The study was conducted on women recruited from outpatient infertility and chronic pelvic pain services at a university hospital. Other researchers must replicate the findings in different settings and populations. A limit of the study is that we have no data on eventual surgeries, performed on the cervix. Surgery may affect cervix elasticity, but there is no reason to suspect a different rate of surgeries in uteri with different uterine flexion. SE is a semiquantitative analysis, and values of tissue elasticity can differ depending on the applied force, on the operator that performs the analysis, and on the interpretation of the color score results. We attempted to overcome some of these limitations by executing the analysis at the optimal compression force suggested by the elastography software and by expressing the data as the ratio between two ROIs that were investigated simultaneously during the same force externally applied by the investigator [18,24]. A single operator performed all ultrasound and elastography evaluations, and three researchers scored the colors of the elastography analysis. Results of tissue elasticity by SE can be influenced by the distance of the tissue from the transducer or by the interposition of the cervical canal, the distant cervical lips receiving a reduced applied force. The consequent reduced tissue compression/decompression may give the false impression of a higher stiffness. In our analysis, as also previously reported [26], the probe was always placed in the anterior cervical fornix thus reducing the possibility that the distance of the anterior and posterior lips differs among ante-flexed and retro-flexed uteri. In linear regression models, tissue elasticity was related to the angle of uterine flexion with the angle of flexion between >150° and ≤210°, showing values intermediate between the marked ante-flexion (≤150°) and the marked retro-flexion (>210°), as to indicate a progression of elasticity changes. Furthermore, the MCC is equidistant from the transducer, independently whether the probe is applied to the anterior or posterior cervical lip, and its elasticity differs among ante- and retro-flexed uteri. Thus, overall, the data indicate that the angle of uterine flexion, more than confounding, is related to the elasticity of cervical tissues evaluated by SE.
5. Conclusions
The current data show that the signal obtained by SE of different areas of the cervix varies with the angle of uterine flexion. These differences may indicate structural differences of the cervix that may have clinical implications in obstetric and gynecological conditions.
Author Contributions
Conceptualization, A.X., A.P.L. and A.C.; methodology, A.X. and U.S.; validation, A.C. and A.P.L.; investigation, A.X. and U.S.; resources, A.X. and U.S.; data curation, A.X., U.S. and A.P.L.; writing—original draft preparation, A.C.; writing—review and editing, A.X., A.P.L., U.S. and A.C.; supervision, A.C.; project administration, A.X. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by Ethics Committee CER Liguria (protocol code 123/2022l).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Due to ethics restriction the data are available from the authors.
Acknowledgments
We acknowledge the administrative and technical support of our unit.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Minamoto, T.; Arai, K.; Hirakawa, S.; Nagai, Y. Immunohistochemical studies on collagen types in the uterine cervix in pregnant and nonpregnant states. Am. J. Obstet. Gynecol. 1987, 156, 138–144. [Google Scholar] [CrossRef]
- Aspden, R.M. Collagen organisation in the cervix and its relation to mechanical function. Coll. Relat. Res. 1988, 8, 103–112. [Google Scholar] [CrossRef]
- Vink, J.Y.; Qin, S.; Brock, C.O.; Zork, N.M.; Feltovich, H.M.; Chen, X.; Urie, P.; Myers, K.M.; Hall, T.J.; Wapner, R.; et al. A new paradigm for the role of smooth muscle cells in the human cervix. Am. J. Obstet. Gynecol. 2016, 215, 478.e1–478.e11. [Google Scholar] [CrossRef]
- Gan, Y.; Yao, W.; Myers, K.M.; Vink, J.Y.; Wapner, R.J.; Hendon, C.P. Analyzing three-dimensional ultrastructure of human cervical tissue using optical coherence tomography. Biomed. Opt. Express 2015, 6, 1090–1108. [Google Scholar] [CrossRef]
- Yao, W.; Gan, Y.; Myers, K.M.; Vink, J.Y.; Wapner, R.J.; Hendon, C.P. Collagen Fiber Orientation and Dispersion in the Upper Cervix of Non-Pregnant and Pregnant Women. PLoS ONE 2016, 11, e0166709. [Google Scholar] [CrossRef] [PubMed]
- Ateshian, G.A. Anisotropy of fibrous tissues in relation to the distribution of tensed and buckled fibers. J. Biomech. Eng. 2007, 129, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Ateshian, G.A.; Rajan, V.; Chahine, N.O.; Canal, C.E.; Hung, C.T. Modeling the matrix of articular cartilage using a continuous fiber angular distribution predicts many observed phenomena. J. Biomech. Eng. 2009, 131, 061003. [Google Scholar] [CrossRef]
- Fernandez, M.; House, M.; Jambawalikar, S.; Zork, N.; Vink, J.; Wapner, R.; Myers, K. Investigating the mechanical function of the cervix during pregnancy using finite element models derived from high-resolution 3D MRI. Comput. Methods Biomech. Biomed. Eng. 2016, 19, 404–417. [Google Scholar] [CrossRef] [PubMed]
- Louwagie, E.M.; Carlson, L.; Over, V.; Mao, L.; Fang, S.; Westervelt, A.; Vink, J.; Hall, T.; Feltovich, H.; Myers, K. Longitudinal ultrasonic dimensions and parametric solid models of the gravid uterus and cervix. PLoS ONE 2021, 16, e0242118. [Google Scholar] [CrossRef]
- Myers, K.M.; Paskaleva, A.P.; House, M.; Socrate, S. Mechanical and biochemical properties of human cervical tissue. Acta Biomater. 2008, 4, 104–116. [Google Scholar] [CrossRef]
- House, M.; Socrate, S. The cervix as a biomechanical structure. Ultrasound Obstet. Gynecol. 2006, 28, 745–749. [Google Scholar] [CrossRef] [PubMed]
- Myers, K.M.; Feltovich, H.; Mazza, E.; Vink, J.; Bajka, M.; Wapner, R.J.; Hall, T.J.; House, M. The mechanical role of the cervix in pregnancy. J. Biomech. 2015, 48, 1511–1523. [Google Scholar] [CrossRef]
- Huebner, M.; DeLancey, J.O.L. Levels of pelvic floor support: What do they look like on magnetic resonance imaging? Int. Urogynecol. J. 2019, 30, 1593–1595. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Yao, W.; Gan, Y.; Zhao, L.Y.; McKee, W.E.; Vink, J.; Wapner, R.J.; Hendon, C.P.; Myers, K. Anisotropic Material Characterization of Human Cervix Tissue Based on Indentation and Inverse Finite Element Analysis. J. Biomech. Eng. 2019, 141, 0910171–0910173. [Google Scholar] [CrossRef] [PubMed]
- Molina, F.S.; Gómez, L.F.; Florido, J.; Padilla, M.C.; Nicolaides, K.H. Quantification of cervical elastography: A reproducibility study. Ultrasound Obstet. Gynecol. 2012, 39, 685–689. [Google Scholar] [CrossRef] [PubMed]
- Hee, L.; Rasmussen, C.K.; Schlütter, J.M.; Sandager, P.; Uldbjerg, N. Quantitative sonoelastography of the uterine cervix prior to induction of labor as a predictor of cervical dilation time. Acta Obstet. Gynecol. Scand. 2014, 93, 684–690. [Google Scholar] [CrossRef] [PubMed]
- Feltovich, H. Cervical Evaluation: From Ancient Medicine to Precision Medicine. Obstet. Gynecol. 2017, 130, 51–63. [Google Scholar] [CrossRef]
- Ozturk, A.; Grajo, J.R.; Dhyani, M.; Anthony, B.W.; Samir, A.E. Principles of ultrasound elastography. Abdom. Radiol. 2018, 43, 773–785. [Google Scholar] [CrossRef]
- Hernandez-Andrade, E.; Hassan, S.S.; Ahn, H.; Kozzeniewski, S.J.; Yeo, L.; Chaiworapongsa, T.; Romero, R. Evaluation of cervical stiffness during pregnancy using semiquantitative ultrasound elastography. Ultrasound Obstet. Gynecol. 2013, 41, 152–161. [Google Scholar] [CrossRef]
- Fruscalzo, A.; Londero, A.P.; Fröhlich, C.; Möllmann, U.; Schmitz, R. Quantitative elastography for cervical stiffness assessment during pregnancy. Biomed. Res. Int. 2014, 2014, 826535. [Google Scholar] [CrossRef]
- Hernandez-Andrade, E.; Garcia, M.; Ahn, H.; Korzeniewsky, S.J.; Saker, H.; Yeo, L.; Chaiworapongsa, T.; Hassan, S.S.; Romero, R. Strain at the internal cervical os assessed with quasi-static elastography is associated with the risk of spontaneous preterm delivery at ≤34 weeks of gestation. J. Perinat. Med. 2015, 43, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Zhang, Y.; Chen, S.; Xiang, X.; Wen, J.; Yi, M.; He, B.; Hu, B. Diagnostic accuracy of cervical elastography in predicting preterm delivery: A systematic review and meta-analysis. Medicine 2019, 98, e16449. [Google Scholar] [CrossRef] [PubMed]
- Stanziano, A.; Caringella, A.M.; Cantatore, C.; Trojano, G.; Caroppo, E.; D’Amato, G. Evaluation of the cervix tissue homogeneity by ultrasound elastography in infertile women for the prediction of embryo transfer ease: A diagnostic accuracy study. Reprod. Biol. Endocrinol. 2017, 15, 64. [Google Scholar] [CrossRef] [PubMed]
- Xholli, A.; Simoncini, G.; Vujosevic, S.; Trombetta, G.; Chiodini, A.; Ferraro, M.F.; Cagnacci, A. Menstrual Pain and Elasticity of Uterine Cervix. J. Clin. Med. 2021, 10, 1110. [Google Scholar] [CrossRef] [PubMed]
- Cagnacci, A.; Grandi, G.; Cannoletta, M.; Xholli, A.; Piacenti, I.; Volpe, A. Intensity of menstrual pain and estimated angle of uterine flexion. Acta Obstet. Gynecol. Scand. 2014, 93, 58–63. [Google Scholar] [CrossRef]
- Xholli, A.; Scovazzi, U.; Londero, A.P.; Evangelisti, G.; Cavalli, E.; Schiaffino, M.G.; Vacca, I.; Oppedisano, F.; Ferraro, M.F.; Sirito, G.; et al. Angle of Uterine Flexion and Adenomyosis. J. Clin. Med. 2022, 11, 3214. [Google Scholar] [CrossRef] [PubMed]
- Gargiulo, T.; Leo, L.; Gomel, V. Laparoscopic uterine suspension using three-stitch technique. J. Am. Assoc. Gynecol. Laparosc. 2000, 7, 233–236. [Google Scholar] [CrossRef]
- Ott, J.; Nouri, K.; Demmel, M.; Zafraani, S.; Greilberger, U.; Huber, J.C.; Mayerhofer, K. Fourteen-year experience with laparoscopic ventrosuspension in patients with retroverted and retroflected uterus and pelvic pain syndromes. J. Minim. Invasive Gynecol. 2010, 17, 749–753. [Google Scholar] [CrossRef] [PubMed]
- Seracchioli, R.; Zanello, M.; Arena, A.; Costantino, C.; Moro, E.; Zannoni, L.; Raimondo, D. New Laparoscopic Technique of Hysteropexy for Uterine Retrodisplacement: Bologna Technique. J. Minim. Invasive Gynecol. 2016, 23, 675. [Google Scholar] [CrossRef]
- Xholli, A.; Molinari, F.; Oppedisano, F.; Scovazzi, U.; Vacca, I.; Schiaffino, M.G.; Cavalli, E.; Cagnacci, A. Relation between adenomyosis and elastographic characteristics of the cervix. Hum. Reprod. 2023, 38, 621–628. [Google Scholar] [CrossRef]
- Dziadosz, M.; Bennett, T.A.; Dolin, C.; West Honart, A.; Pham, A.; Lee, S.S.; Pivo, S.; Roman, A.S. Uterocervical angle: A novel ultrasound screening tool to predict spontaneous preterm birth. Am. J. Obstet. Gynecol. 2016, 215, 376.e1–376.e7. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Ultrasonographic image of a retroflexed uterus in a sagittal (a) and transverse scan (b). The interrupted lines indicate uterus measures. L: longitudinal uterus measure; AP: anterior-posterior uterus measure; CAP: cervix antero-posterior diameter; CL: cervix length; ICO: internal cervical os; ECO: external cervical os; Angle: angle of uterine flexion; Probe: ultrasound probe; T: transverse uterus measure.
Figure 1.
Ultrasonographic image of a retroflexed uterus in a sagittal (a) and transverse scan (b). The interrupted lines indicate uterus measures. L: longitudinal uterus measure; AP: anterior-posterior uterus measure; CAP: cervix antero-posterior diameter; CL: cervix length; ICO: internal cervical os; ECO: external cervical os; Angle: angle of uterine flexion; Probe: ultrasound probe; T: transverse uterus measure.

Figure 2.
Elastography image of the cervix of an anteflexed uterus showing a stiffer posterior than anterior (cervical compartment stiffer (blue) than an anterior (cyan/green) cervical compartment. Probe: transvaginal elastography probe; ICO: internal cervical os; ACC: anterior cervical compartment; MCC: middle cervical canal; PCC: posterior cervical compartment; ECO: external cervical os.
Figure 2.
Elastography image of the cervix of an anteflexed uterus showing a stiffer posterior than anterior (cervical compartment stiffer (blue) than an anterior (cyan/green) cervical compartment. Probe: transvaginal elastography probe; ICO: internal cervical os; ACC: anterior cervical compartment; MCC: middle cervical canal; PCC: posterior cervical compartment; ECO: external cervical os.

Figure 3.
Mean (SD) values of tissue elasticity of the anterior cervical compartment (ACC), posterior cervical compartment (PCC), middle cervical canal compartment (MCC), internal cervical os (ICO), and their elasticity ratio, observed in uteri with an angle of flexion ≤150° or >210° * p = 0.004; ** p = 0.001.
Figure 3.
Mean (SD) values of tissue elasticity of the anterior cervical compartment (ACC), posterior cervical compartment (PCC), middle cervical canal compartment (MCC), internal cervical os (ICO), and their elasticity ratio, observed in uteri with an angle of flexion ≤150° or >210° * p = 0.004; ** p = 0.001.

Figure 4.
Schematic representation of the elasticity of different cervical areas observed in anteflexed (left) and retroflexed (right) uteri. ACC: anterior cervical compartment; PCC: posterior cervical compartment; MCC: middle cervical canal compartment; ICO: internal cervical os. Elasticity increases with the intensity from blue up to pink.
Figure 4.
Schematic representation of the elasticity of different cervical areas observed in anteflexed (left) and retroflexed (right) uteri. ACC: anterior cervical compartment; PCC: posterior cervical compartment; MCC: middle cervical canal compartment; ICO: internal cervical os. Elasticity increases with the intensity from blue up to pink.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Demographic information, uterine measurements, and elasticity of four cervical regions of interest, measured by strain elastography in 275 women.
Table 1.
Demographic information, uterine measurements, and elasticity of four cervical regions of interest, measured by strain elastography in 275 women.
| Parameter | Value |
|---|---|
| Age (yrs.) | 36.7 ± 7.5 |
| Menarche (yrs.) | 12.6 ± 1.6 |
| BMI (Kg/m2) | 22.9 ± 4.8 |
| Abortion (%) | 4.1 |
| Parous (%) | 20.5 |
| Caesarean delivery (%) | 4.5 |
| Uterus Volume (mm3) | 61.9 ± 45.3 |
| Uterus L (mm) | 59.5 ± 13.6 |
| Uterus AP (mm) | 39.0 ± 10.4 |
| Uterus T (mm) | 50.9 ± 10.5 |
| Cervix volume (mm3) | 20.1 ± 6.18 |
| Cervix length (mm) | 26.6 ± 5.19 |
| Cervix diameter (mm) | 23.5 ± 4.9 |
| ACC elasticity | 0.94 ± 0.36 |
| PCC elasticity | 0.74 ± 0.29 |
| MCC elasticity | 1.39 ± 0.51 |
| ICO elasticity | 0.63 ± 0.28 |
Data are expressed as mean (SD) or percentage. L: longitudinal measure; AP: antero-posterior measure; T: transverse measure; ACC: anterior cervical compartment; PCC: posterior cervical compartment; MCC: middle cervical canal compartment; ICO Internal cervical os.
Table 2.
Simple linear regression analyses between the angle of uterine of flexion (dependent variable) and significantly related parameters, in 275 women.
Table 2.
Simple linear regression analyses between the angle of uterine of flexion (dependent variable) and significantly related parameters, in 275 women.
| Parameter | R2 | Coefficient of Regression | 95% Confidence Interval | p Value |
|---|---|---|---|---|
| Age (yrs.) | 0.013 | 0.828 | 0.054; 1.601 | 0.036 |
| Uterus Volume (mm3) | 0.021 | 0.173 | 0.042; 0.303 | 0.009 |
| Uterus AP (mm) | 0.040 | 0.970 | 0.421; 1.520 | 0.001 |
| Uterus T (mm) | 0.017 | 0.670 | 0.116; 1.225 | 0.018 |
| Cervix Diameter (mm) | 0.010 | −1.175 | −2.376; 0.002 | 0.059 |
| Uterus AP/Cervix diameter | 0.065 | 23.67 | 13.09; 34.28 | 0.001 |
| ACC elasticity | 0.071 | −36.2 | −51.51; −20.913 | 0.002 |
| PCC elasticity | 0.010 | 19.6 | −0.360; 39.710 | 0.054 |
| MCC elasticity | 0.047 | −26.611 | −32.81; −10.40 | 0.002 |
| ACC/PCC | 0.490 | −11.34 | −17.68; −5.60 | 0.001 |
| PCC/MCC | 0.109 | 28.44 | 18.87; 38.02 | 0.001 |
Data are expressed as mean (SD) or percentage. AP: anterior-posterior measure; T: transverse measure; ACC: anterior cervical compartment; PCC: posterior cervical compartment; MCC: middle cervical canal compartment.
Table 3.
Multiple linear regression models between the angle of uterine flexion and the independently related factors evaluated in 275 women.
Table 3.
Multiple linear regression models between the angle of uterine flexion and the independently related factors evaluated in 275 women.
| Parameter | Coefficient of Regression | 95% Confidence Interval | p Value |
|---|---|---|---|
| Model 1 (R2 = 0.116) | |||
| Uterus AP (mm) | 1.014 | 0.461; 1.567 | 0.001 |
| Cervix Diameter (mm) | −1.24 | −2.401; −0.075 | 0.037 |
| ACC color score | −33.9 | −49.2; −18.65 | 0.001 |
| Model 2 (R2 = 0.124) | |||
| Uterus AP/Cervix diameter | 21.66 | 11.34; 31.89 | 0.001 |
| ACC color score | −33.4 | −48.6; −18.2 | 0.001 |
| Model 3 (R2 = 0.163) | |||
| Uterus AP/Cervix diameter | 21.67 | 11.60; 31.75 | 0.001 |
| PCC/MCC | 26.83 | 17.41; 32.21 | 0.001 |
Data are expressed as mean (SD) or percentage. AP: anterior-posterior measure; ACC: anterior cervical compartment; PCC: posterior cervical compartment; MCC: middle cervical canal compartment.
Table 4.
Demographic, ultrasonographic characteristics and elastography parameters of the cervix of 275 women categorized accordingly to the angle of uterine flexion (A: ≤150°; B: >150°–≤210°; and C: >210°).
Table 4.
Demographic, ultrasonographic characteristics and elastography parameters of the cervix of 275 women categorized accordingly to the angle of uterine flexion (A: ≤150°; B: >150°–≤210°; and C: >210°).
| Parameter | A | B | C | p A vs. B | p A vs. C | p B vs. C |
|---|---|---|---|---|---|---|
| Age (yrs.) | 35.3 ± 7.1 | 41.8 ± 7.1 | 34.7 ± 8.2 | 0.001 | 0.632 | 0.004 |
| Menarche (Yrs.) | 12.5 ± 1.7 | 12.8 ± 1.5 | 12.7 ± 1.2 | 0.723 | 0.718 | 0.907 |
| BMI (Kg/m2) | 22.7 ± 4.8 | 24.6 ± 5.2 | 23.1 ± 4.7 | 0.131 | 0.692 | 0.288 |
| Uterus Volume (mm3) | 56.7 ± 35.40 | 86.1 ± 86.9 | 65.9 ± 51.1 | 0.004 | 0.232 | 0.089 |
| Uterus L (mm) | 54.0 ± 11.4 | 56.8 ± 21.6 | 53.7 ± 14.80 | 0.356 | 0.890 | 0.383 |
| Uterus AP (mm) | 37.7 ± 8.8 | 48.4 ± 16.1 | 40.4 ± 11.8 | 0.001 | 0.132 | 0.004 |
| Uterus T (mm) | 50.2 ± 9.7 | 56.8 ± 16.6 | 51.3 ± 10.1 | 0.007 | 0.520 | 0.060 |
| Cervix volume (mm3) | 19.8 ± 5.8 | 22.0 ± 8.5 | 19.9 ± 6.0 | 0.115 | 0.090 | 0.016 |
| Cervix Diameter (mm) | 23.9 ± 4.6 | 23.4 ± 6.5 | 21.6 ± 5.2 | 0.693 | 0.009 | 0.182 |
| ACC elasticity | 0.98 ± 0.37 | 0.89 ± 0.3 | 0.69 ± 0.26 | 0.239 | 0.001 | 0.044 |
| PCC elasticity | 0.72 ± 0.290 | 0.71 ± 0.25 | 0.86 ± 0.24 | 0.859 | 0.004 | 0.046 |
| MCC elasticity | 1.44 ± 0.51 | 1.44 ± 0.59 | 1.08 ± 0.36 | 0.976 | 0.001 | 0.010 |
| ICO elasticity | 0.62 ± 0.28 | 0.58 ± 0.29 | 0.66 ± 0.23 | 0.442 | 0.425 | 0.246 |
| ACC/PCC | 1.62 ± 1.03 | 1.39 ± 0.77 | 0.90 ± 0.53 | 0.292 | 0.001 | 0.058 |
| PCC/MCC | 0.83 ± 0.49 | 0.89 ± 0.41 | 1.45 ± 0.76 | 0.612 | 0.001 | 0.001 |
L: longitudinal measure; AP: anterior-posterior measure; T: transverse measure; ACC: anterior cervical compartment; PCC: posterior cervical compartment; MCC: middle cervical canal compartment; ICO: internal cervical orifice.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Xholli, A.; Londero, A.P.; Scovazzi, U.; Cagnacci, A. Elasticity of the Cervix in Relation to Uterus Position. J. Clin. Med. 2024, 13, 2572. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092572
AMA Style
Xholli A, Londero AP, Scovazzi U, Cagnacci A. Elasticity of the Cervix in Relation to Uterus Position. Journal of Clinical Medicine. 2024; 13(9):2572. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092572
Chicago/Turabian StyleXholli, Anjeza, Ambrogio Pietro Londero, Umberto Scovazzi, and Angelo Cagnacci. 2024. "Elasticity of the Cervix in Relation to Uterus Position" Journal of Clinical Medicine 13, no. 9: 2572. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092572
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.