
Icarifil® in Association with Daily Use of Tadalafil (5 mg) versus Standard Tadalafil Daily Dose (5 mg) or Alone: Results from a Controlled, Randomized Clinical Trial
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
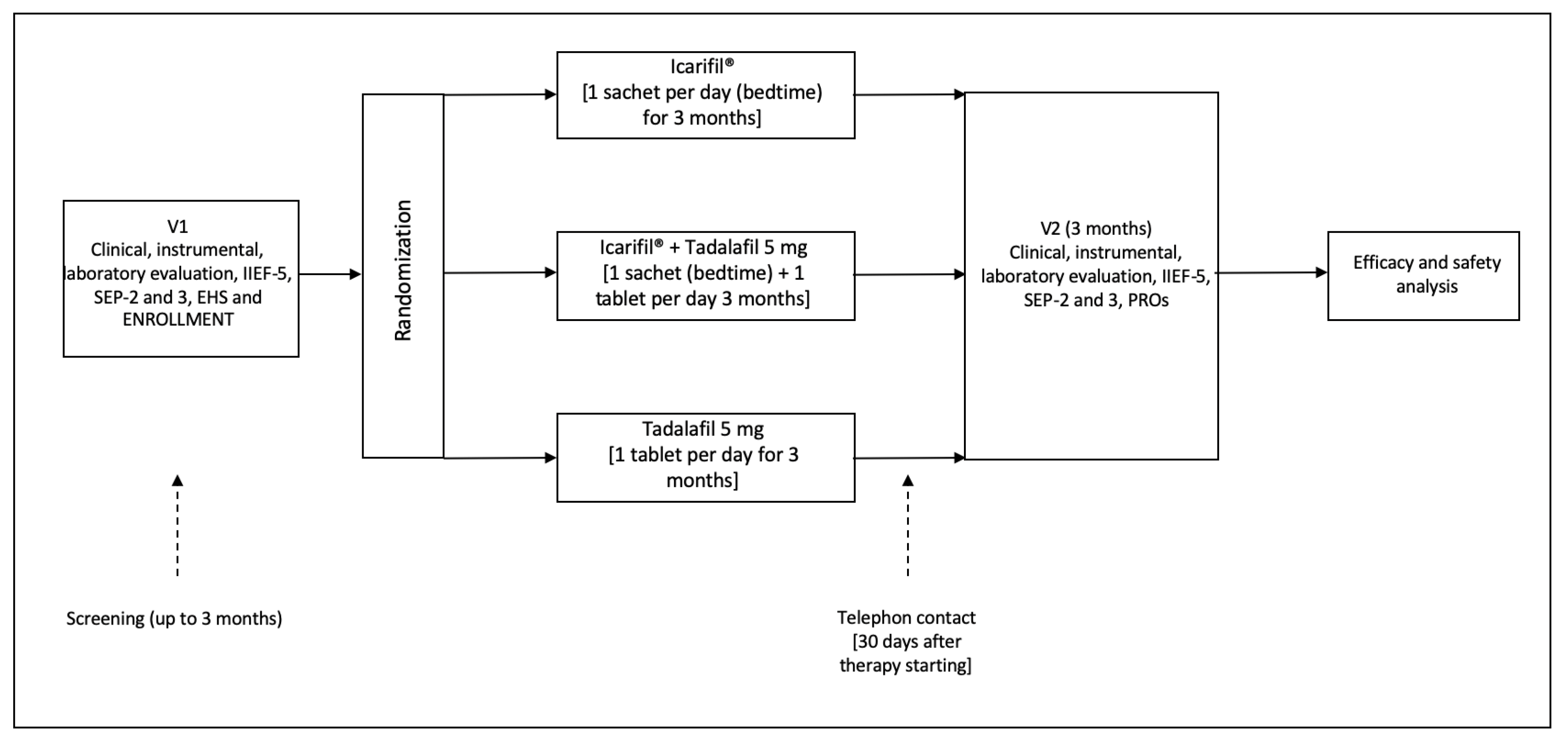
2.1. Study Design and Schedule
2.2. Inclusion and Exclusion Criteria
2.3. Composition and Characterization of the Extracts Used
2.4. Questionnaires
2.5. Statistical Analysis, Outcome Measures and Ethical Considerations
3. Results
3.1. Patients
3.2. Follow-Up Results
3.3. Patients and Their Partners’ Reported Outcomes (PROs)
3.4. Adverse Effects
4. Discussion
4.1. Major Finding
4.2. Results in Comparison with Other Studies
4.3. Strengths and Limitations of the Present Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- La Croce, G.; Schifano, N.; Pescatori, E.; Caraceni, E.; Colombo, F.; Bettocchi, C.; Carrino, M.; Vitarelli, A.; Pozza, D.; Fiordelise, S.; et al. Which patient may benefit the most from penile prosthesis implantation? Andrology 2022, 10, 1567–1574. [Google Scholar] [CrossRef] [PubMed]
- Yafi, F.A.; Jenkins, L.; Albersen, M.; Corona, G.; Isidori, A.M.; Goldfarb, S.; Maggi, M.; Nelson, C.J.; Parish, S.; Salonia, A.; et al. Erectile dysfunction. Nat. Rev. Dis. Primers 2016, 2, 16003. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shamloul, R.; Ghanem, H. Erectile dysfunction. Lancet 2013, 381, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Lewis, R.W.; Fugl-Meyer, K.S.; Corona, G.; Hayes, R.D.; Laumann, E.O.; Moreira, E.D., Jr.; Rellini, A.H.; Segraves, T. Definitions/epidemiology/risk factors for sexual dysfunction. J. Sex. Med. 2010, 7 Pt 2, 1598–1607. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.marketdataforecast.com/market-reports/pde-inhibitors-market-revenue (accessed on 3 February 2024).
- Salonia, A.; Bettocchi, C.; Boeri, L.; Capogrosso, P.; Carvalho, J.; Cilesiz, N.C.; Cocci, A.; Corona, G.; Dimitropoulos, K.; Gül, M.; et al. European Association of Urology Guidelines on Sexual and Reproductive Health-2021 Update: Male Sexual Dysfunction. Eur. Urol. 2021, 80, 333–357. [Google Scholar] [CrossRef] [PubMed]
- Capece, M.; Montorio, D.; Comune, C.; Aveta, A.; Melchionna, A.; Celentano, G.; Imbimbo, C.; Crocetto, F.; Califano, G.; Cennamo, G. Retinal and Optic Disc Vascular Changes in Patients Using Long-Term Tadalafil: A Prospective Non-Randomized Matched-Pair Study. Diagnostics 2021, 11, 802. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wang, J.; Song, J.; Song, G.; Feng, Y.; Pan, J.; Yang, X.; Xin, Z.; Hu, P.; Sun, T.; Liu, K.; et al. Acetyl-L-carnitine improves erectile function in bilateral cavernous nerve injury rats via promoting cavernous nerve regeneration. Andrology 2022, 10, 984–996. [Google Scholar] [CrossRef] [PubMed]
- Nobili, S.; Lucarini, E.; Murzilli, S.; Vanelli, A.; Di Cesare Mannelli, L.; Ghelardini, C. Efficacy Evaluation of Plant Products in the Treatment of Erectile Dysfunction Related to Diabetes. Nutrients 2021, 13, 4520. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ștefănescu, R.; Farczadi, L.; Huțanu, A.; Ősz, B.E.; Mărușteri, M.; Negroiu, A.; Vari, C.E. Tribulus terrestris Efficacy and Safety Concerns in Diabetes and Erectile Dysfunction, Assessed in an Experimental Model. Plants 2021, 10, 744. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Amante, C.; De Soricellis, C.; Luccheo, G.; Di Vernieri, A.; Luccheo, L.; Falcone, G.; Del Gaudio, P. Icarifil, a Natural Mixture Based on L-Citrulline and L-Carnitine as a Novel Multicomponent Nutraceutical to Modulate ROS and PDE5. Appl. Sci. 2023, 13, 12358. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cappelleri, J.C.; Rosen, R.C.; Smith, M.D.; Mishra, A.; Osterloh, I.H. Diagnostic evaluation of the erectile function domain of the International Index of Erectile Function. Urology 1999, 54, 346–351. [Google Scholar] [CrossRef]
- Tang, Z.; Li, D.; Zhang, X.; Yi, L.; Zhu, X.; Zeng, X.; Tang, Y. Comparison of the simplified International Index of Erectile Function (IIEF-5) in patients of erectile dysfunction with different pathophysiologies. BMC Urol. 2014, 14, 52. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Araujo, A.B.; Allen, K.R.; Ni, X.; Rosen, R.C. Minimal clinically import-ant differences in the vaginal insertion and successful intercourse items of the sexual encounter profile. J. Sex. Med. 2012, 9, 169–179. [Google Scholar] [CrossRef] [PubMed]
- Rosen, R.C.; Riley, A.; Wagner, G.; Osterloh, I.H.; Kirkpatrick, J.; Mishra, A. The international index of erectile function (IIEF): A multidimensional scale for assessment of erectile dysfunction. Urology 1997, 49, 822–830. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, I.; Lue, T.F.; Padma-Nathan, H.; Rosen, R.C.; Steers, W.D.; Wicker, P.A. Oral sildenafil in the treatment of erectile dysfunction. Sildenafil Study Group. N. Engl. J. Med. 1998, 338, 1397–1404. [Google Scholar] [CrossRef] [PubMed]
- Cai, T.; Palumbo, F.; Liguori, G.; Mondaini, N.; Scroppo, F.I.; Di Trapani, D.; Cocci, A.; Zucchi, A.; Verze, P.; Salonia, A.; et al. The intra-meatal application of alprostadil cream (Vitaros®) improves drug efficacy and patient’s satisfaction: Results from a randomized, two-administration route, cross-over clinical trial. Int. J. Impot. Res. 2019, 31, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Rhim, H.C.; Kim, M.S.; Park, Y.-J.; Choi, W.S.; Park, H.K.; Kim, H.G.; Kim, A.; Paick, S.H. The potential role of arginine supplements on erectile dysfunction: A systemic review and meta-analysis. J. Sex. Med. 2019, 16, 223–234. [Google Scholar] [CrossRef]
- Trinchieri, M.; Perletti, G.; Magri, V.; Stamatiou, K.; Cai, T.; Montanari, E.; Trinchieri, A. Erectile and Ejaculatory Dysfunction Associated with Use of Psychotropic Drugs: A Systematic Review. J. Sex. Med. 2021, 18, 1354–1363. [Google Scholar] [CrossRef] [PubMed]
- Aguayo, E.; Martínez-Sánchez, A.; Fernández-Lobato, B.; Alacid, F. L-Citrulline: A Non-Essential Amino Acid with Important Roles in Human Health. Appl. Sci. 2021, 11, 3293. [Google Scholar] [CrossRef]
- Cormio, L.; De Siati, M.; Lorusso, F.; Selvaggio, O.; Mirabella, L.; Sanguedolce, F.; Carrieri, G. Oral L-citrulline supplementation improves erection hardness in men with mild erectile dysfunction. Urology 2011, 77, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.D.; Park, C.W.; Jang, J.; Kim, S.H.; Jeon, H.Y.; Kim, W.G.; Lee, S.J.; Chung, W.S. Effects of Korean ginseng berry extract on sexual function in men with erectile dysfunction: A multicenter, placebo-controlled, double-blind clinical study. Int. J. Impot. Res. 2013, 25, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Ciccone, V.; Piragine, E.; Gorica, E.; Citi, V.; Testai, L.; Pagnotta, E.; Matteo, R.; Pecchioni, N.; Montanaro, R.; Di Cesare Mannelli, L.; et al. Anti-Inflammatory Effect of the Natural H2S-Donor Erucin in Vascular Endothelium. Int. J. Mol. Sci. 2022, 23, 15593. [Google Scholar] [CrossRef]
- Jupiter, R.C.; Yoo, D.; Pankey, E.A.; Reddy, V.V.; Edward, J.A.; Polhemus, D.J.; Peak, T.C.; Katakam, P.; Kadowitz, P.J. Analysis of erectile responses to H2S donors in the anesthetized rat. Am. J. Physiol. Heart Circ. Physiol. 2015, 309, H835–H843. [Google Scholar] [CrossRef] [PubMed]
- Gauthaman, K.; Ganesan, A.P.; Prasad, R.N.V. Sexual Effects of Puncturevine (Tribulus terrestris) Extract (Protodioscin): An Evaluation Using a Rat Model. J. Altern. Complement. Med. 2003, 9, 257–265. [Google Scholar] [CrossRef]
- Porst, H.; Brock, G.B.; Kula, K.; Moncada, I.; Montorsi, F.; Basson, B.R.; Kinchen, K.; Aversa, A. Effects of once-daily tadalafil on treatment satisfaction, psychosocial outcomes, spontaneous erections, and measures of endothelial function in men with erectile dysfunction but naive to phosphodiesterase type 5 inhibitors. J. Androl. 2012, 33, 1305–1322. [Google Scholar] [CrossRef] [PubMed]
- Mirone, V.; Napolitano, L.; D’Emmanuele di Villa Bianca, R.; Mitidieri, E.; Sorrentino, R.; Vanelli, A.; Vanacore, D.; Turnaturi, C.; La Rocca, R.; Celentano, G.; et al. A new original nutraceutical formulation ameliorates the effect of Tadalafil on clinical score and cGMP accumulation. Arch. Ital. Urol. Androl. 2021, 93, 221–226. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Group 1 | Group 2 | Group 3 | ||
|---|---|---|---|---|
| p | ||||
| Number of enrolled patients | 51 | 50 | 51 | |
| Age (years) | 0.71 | |||
| Median (IQR †) | 51 (42–67) | 53 (43–66) | 53 (42–69) | |
| BMI (kg/m2) | 0.72 | |||
| Median (IQR †) | 28 (26–30) | 27 (25–30) | 27 (26–31) | |
| Charlson Comorbidity index (CCI) | 0.12 | |||
| 0 | 49 (96.1) | 48 (96.0) | 50 (98.1) | |
| 1 | 2 (3.9) | 2 (4.0) | 1 (1.9) | |
| 2 | 0 (-) | 0 (-) | 0 (-) | |
| Number of sexual partners | 0.37 | |||
| 1 | 41 (80.3) | 39 (76.4) | 40 (78.4) | |
| 2 or more | 10 (19.7) | 11 (23.6) | 11 (22.6) | |
| Sexual partners age | 0.84 | |||
| Median (IQR †) | 48 (39–65) | 48 (38–66) | 49 (39–67) | |
| Duration of erectile dysfunction (months) | 0.91 | |||
| Median (IQR †) | 7 (6–9) | 8 (6–9) | 8 (6–9) | |
| Etiology of the disease | 0.09 | |||
| Organic | 5 (9.8) | 4 (8.0) | 5 (9.8) | |
| Psycogenic | 18 (35.3) | 20 (40.0) | 19 (37.2) | |
| Mixed | 28 (54.9) | 26 (52.0) | 27 (53.0) |
| Group 1 | Group 2 | Group 3 | |||||
|---|---|---|---|---|---|---|---|
| p | |||||||
| Baseline | Follow-Up | Baseline | Follow-Up | Baseline | Follow-Up | ||
| IIEF-5 | <0.001 * 0.82 # | ||||||
| Median (IQR †) | 15 (13–15) | 19 (18–21) | 14 (13–15) | 23 (21–25) | 14 (13–15) | 22 (21–25) | |
| p | <0.003 | <0.001 | <0.001 | ||||
| SEP-2 | <0.001 * <0.001 # | ||||||
| Positive response (%) | 19 (37.2) | 29 (56.9) | 19 (38.0) | 47 (94.0) | 20 (39.2) | 42 (82.3) | |
| p | <0.001 | <0.001 | <0.001 | ||||
| SEP-3 | <0.001 * <0.001 # | ||||||
| Positive response (%) | 11 (21.5) | 30 (58.8) | 13 (26.0) | 47 (94.0) | 12 (23.5) | 43 (84.3) | |
| p | <0.001 | <0.001 | <0.001 | ||||
| EHS | <0.001 * 0.09 # | ||||||
| Median (IQR †) | 2 (1–3) | 3 (3) | 2 (1–3) | 4 (3–4) | 2 (1–3) | 3 (3–4) | |
| p | <0.001 | <0.001 | <0.001 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, T.; Palumbo, F.; Miacola, C.; Ceruti, C.; Rizzo, M.; Liguori, G.; Gallelli, L.; Palmieri, A., on behalf of the Italian Society of Andrology (SIA). Icarifil® in Association with Daily Use of Tadalafil (5 mg) versus Standard Tadalafil Daily Dose (5 mg) or Alone: Results from a Controlled, Randomized Clinical Trial. J. Clin. Med. 2024, 13, 2564. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092564
Cai T, Palumbo F, Miacola C, Ceruti C, Rizzo M, Liguori G, Gallelli L, Palmieri A on behalf of the Italian Society of Andrology (SIA). Icarifil® in Association with Daily Use of Tadalafil (5 mg) versus Standard Tadalafil Daily Dose (5 mg) or Alone: Results from a Controlled, Randomized Clinical Trial. Journal of Clinical Medicine. 2024; 13(9):2564. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092564
Chicago/Turabian StyleCai, Tommaso, Fabrizio Palumbo, Carlos Miacola, Carlo Ceruti, Michele Rizzo, Giovanni Liguori, Luca Gallelli, and Alessandro Palmieri on behalf of the Italian Society of Andrology (SIA). 2024. "Icarifil® in Association with Daily Use of Tadalafil (5 mg) versus Standard Tadalafil Daily Dose (5 mg) or Alone: Results from a Controlled, Randomized Clinical Trial" Journal of Clinical Medicine 13, no. 9: 2564. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092564