
Regional Spondylodiscitis Disparities: Impact on Pathogen Spectrum and Patients
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
Statistics
3. Results
3.1. Admission and Demographic Parameters
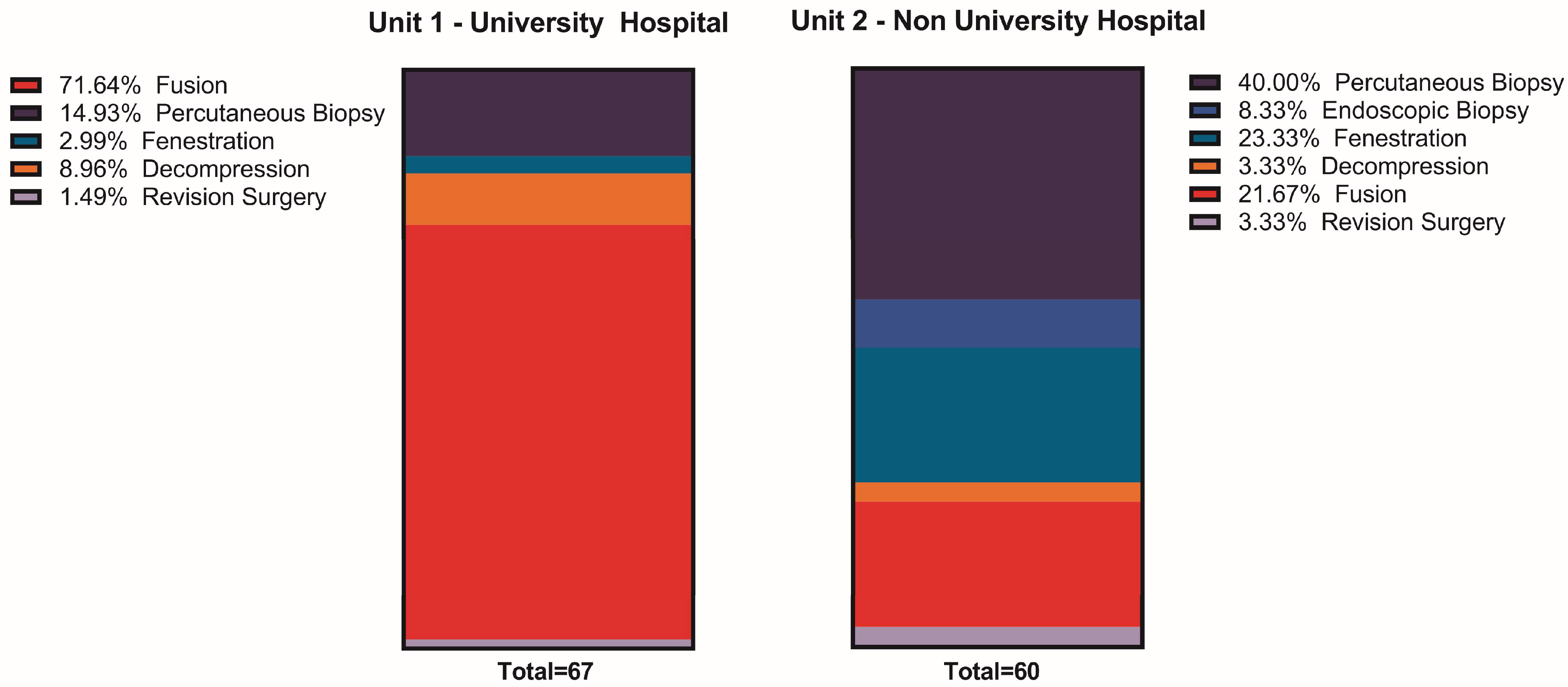
3.2. Surgical Treatment
3.3. Microbiological Parameters
3.4. Antibiotic Treatment
3.5. Resistances
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gouliouris, T.; Aliyu, S.H.; Brown, N.M. Spondylodiscitis: Update on diagnosis and management. J. Antimicrob. Chemother. 2010, 65 (Suppl. 3), iii11–iii24. [Google Scholar] [CrossRef] [PubMed]
- Thavarajasingam, S.G.; Subbiah Ponniah, H.; Philipps, R.; Neuhoff, J.; Kramer, A.; Demetriades, A.K.; Shiban, E.; Ringel, F.; Davies, B. Increasing incidence of spondylodiscitis in England: An analysis of the national health service (NHS) hospital episode statistics from 2012 to 2021. Brain Spine 2023, 3, 101733. [Google Scholar] [CrossRef] [PubMed]
- Pojskic, M.; Carl, B.; Schmockel, V.; Vollger, B.; Nimsky, C.; Sabeta, B. Neurosurgical Management and Outcome Parameters in 237 Patients with Spondylodiscitis. Brain Sci. 2021, 11, 1019. [Google Scholar] [CrossRef]
- Bornemann, R.; Rossler, P.; Jacobs, C.; Randau, T.M.; Rommelspacher, Y.; Wirtz, D.C.; Pflugmacher, R. Spondylitis—Spondylodiscitis—An Update. Z. Orthop. Unfallchirurgie 2019, 157, 132–143. [Google Scholar] [CrossRef]
- Gentile, L.; Benazzo, F.; De Rosa, F.; Boriani, S.; Dallagiacoma, G.; Franceschetti, G.; Gaeta, M.; Cuzzocrea, F. A systematic review: Characteristics, complications and treatment of spondylodiscitis. Eur. Rev. Med. Pharmacol. Sci. 2019, 23 (Suppl. 2), 117–128. [Google Scholar] [CrossRef] [PubMed]
- Baran, A.I.; Celik, M.; Arslan, Y.; Incecik, S.; Binici, I.; Toprak, M.; Sunnetcioglu, M. A comparative perspective on brucellar, pyogenic, and tuberculous spondylodiscitis. Eur. Rev. Med. Pharmacol. Sci. 2024, 28, 2550–2557. [Google Scholar] [CrossRef]
- Mylona, E.; Samarkos, M.; Kakalou, E.; Fanourgiakis, P.; Skoutelis, A. Pyogenic vertebral osteomyelitis: A systematic review of clinical characteristics. Semin. Arthritis Rheum. 2009, 39, 10–17. [Google Scholar] [CrossRef]
- Kramer, A.; Thavarajasingam, S.G.; Neuhoff, J.; Ponniah, H.S.; Ramsay, D.S.C.; Demetriades, A.K.; Davies, B.M.; Shiban, E.; Ringel, F. Epidemiological trends of pyogenic spondylodiscitis in Germany: An EANS Spine Section Study. Sci. Rep. 2023, 13, 20225. [Google Scholar] [CrossRef]
- Kitchen, M.; Gasslitter, I.; Gisinger, M.; Deeg, J.; Rieger, A.; Sarcletti, M. Pyogenic spondylodiscitis in HIV-positive patients under antiretroviral therapy: A case series. Int. J. STD AIDS 2024, 35, 234–239. [Google Scholar] [CrossRef]
- Herren, C.; von der Höh, N.; Dreimann, M. S2k-Leitlinie Diagnostik und Therapie der Spondylodiszitis; Deutsche Wirbelsäulengesellschaft (DWG); Deutsche Gesellschaft für Orthopädie und Orthopädische Chirurgie e.V. (DGOOC): Berlin, Germany, 2020. [Google Scholar]
- Thavarajasingam, S.G.; Vemulapalli, K.V.; Vishnu, K.S.; Ponniah, H.S.; Vogel, A.S.; Vardanyan, R.; Neuhoff, J.; Kramer, A.; Shiban, E.; Ringel, F.; et al. Conservative versus early surgical treatment in the management of pyogenic spondylodiscitis: A systematic review and meta-analysis. Sci. Rep. 2023, 13, 15647. [Google Scholar] [CrossRef]
- Fleege, C.; Wichelhaus, T.A.; Rauschmann, M. Systemic and local antibiotic therapy of conservative and operative treatment of spondylodiscitis. Orthopade 2012, 41, 727–735. [Google Scholar] [CrossRef] [PubMed]
- Marathe, N.A.; Tedesco, G.; Chiesa, A.M.; Mallepally, A.R.; Di Carlo, M.; Ghermandi, R.; Evangelisti, G.; Girolami, M.; Pipola, V.; Gasbarrini, A. Pyogenic and Non-pyogenic Spinal Infections: Diagnosis and Treatment. Curr. Med. Imaging 2022, 18, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Skaf, G.S.; Domloj, N.T.; Fehlings, M.G.; Bouclaous, C.H.; Sabbagh, A.S.; Kanafani, Z.A.; Kanj, S.S. Pyogenic spondylodiscitis: An overview. J. Infect. Public Health 2010, 3, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Zarghooni, K.; Rollinghoff, M.; Sobottke, R.; Eysel, P. Treatment of spondylodiscitis. Int. Orthop. 2012, 36, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Hadjipavlou, A.G.; Mader, J.T.; Necessary, J.T.; Muffoletto, A.J. Hematogenous Pyogenic Spinal Infections and Their Surgical Management. Spine 2000, 25, 1668–1679. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.G.; Buchholz, A.L.; Sure, D.R.; Buell, T.J.; Nguyen, J.H.; Chen, C.J.; Diamond, J.M.; Washburn, P.A.; Harrop, J.; Shaffrey, C.I.; et al. Presentation and Outcomes After Medical and Surgical Treatment Versus Medical Treatment Alone of Spontaneous Infectious Spondylodiscitis: A Systematic Literature Review and Meta-Analysis. Glob. Spine J. 2018, 8 (Suppl. 4), 49S–58S. [Google Scholar] [CrossRef] [PubMed]
- Grammatico, L.; Baron, S.; Rusch, E.; Lepage, B.; Surer, N.; Desenclos, J.C.; Besnier, J.M. Epidemiology of vertebral osteomyelitis (VO) in France: Analysis of hospital-discharge data 2002–2003. Epidemiol. Infect. 2008, 136, 653–660. [Google Scholar] [CrossRef]
- Saad Berreta, R.; Zhang, H.; Alsoof, D.; McDonald, C.L.; Diebo, B.G.; Kuris, E.; Daniels, A.H. Beta-lactam-resistant Staphylococcus aureus in spinal osteomyelitis and spondylodiscitis: Current landscape in antibiotic resistance, treatment, and complications. J. Neurosurg. Spine 2023, 38, 758–763. [Google Scholar] [CrossRef]
- Fritzenwanker, M.; Imirzalioglu, C.; Herold, S.; Wagenlehner, F.M.; Zimmer, K.P.; Chakraborty, T. Treatment Options for Carbapenem- Resistant Gram-Negative Infections. Dtsch. Arztebl. Int. 2018, 115, 345–352. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Namvar, A.E.; Bastarahang, S.; Abbasi, N.; Ghehi, G.S.; Farhadbakhtiarian, S.; Arezi, P.; Hosseini, M.; Baravati, S.Z.; Jokar, Z.; Chermahin, S.G. Clinical characteristics of Staphylococcus epidermidis: A systematic review. GMS Hyg. Infect. Control 2014, 9, Doc23. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Grados, F.; Lescure, F.X.; Senneville, E.; Flipo, R.M.; Schmit, J.L.; Fardellone, P. Suggestions for managing pyogenic (non-tuberculous) discitis in adults. Jt. Bone Spine 2007, 74, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Homagk, L.; Homagk, N.; Klauss, J.R.; Roehl, K.; Hofmann, G.O.; Marmelstein, D. Spondylodiscitis severity code: Scoring system for the classification and treatment of non-specific spondylodiscitis. Eur. Spine J. 2016, 25, 1012–1020. [Google Scholar] [CrossRef] [PubMed]
- Pola, E.; Taccari, F.; Autore, G.; Giovannenze, F.; Pambianco, V.; Cauda, R.; Maccauro, G.; Fantoni, M. Multidisciplinary management of pyogenic spondylodiscitis: Epidemiological and clinical features, prognostic factors and long-term outcomes in 207 patients. Eur. Spine J. 2018, 27, 229–236. [Google Scholar] [CrossRef]
- Saini, V.K.; Mammoottil, A.E.; Ora, M.; Gambhir, S.; Nazar, A.H. Contiguous Multilevel Vertebral Metastasis in Carcinoma Breast Mimicking Spondylodiscitis. Indian J. Nucl. Med. 2021, 36, 316–318. [Google Scholar] [CrossRef] [PubMed]
- Hatsuda, Y.; Ishizaka, T.; Koizumi, N.; Yasui, Y.; Saito, T.; Omotani, S.; Maki, S.; Teramachi, H.; Myotoku, M. Monitoring antimicrobial cross-resistance with cross-resistance rate correlation diagrams: Changes in antibiotic susceptibility of Pseudomonas aeruginosa due to hospital relocation. J. Clin. Pharm. Ther. 2021, 46, 395–407. [Google Scholar] [CrossRef]
- Herren, C.; von der Hoeh, N.H.; Zwingenberger, S.; Sauer, D.; Jung, N.; Pieroh, P.; Drange, S.; Pumberger, M.; Scheyerer, M.J.; Spine Section of the German Society for Orthopaedics and Trauma. Spondylodiscitis in Geriatric Patients: What Are the Issues? Glob. Spine J. 2023, 13 (Suppl. 1), 73S–84S. [Google Scholar] [CrossRef]
- Cheung, G.Y.C.; Bae, J.S.; Otto, M. Pathogenicity and virulence of Staphylococcus aureus. Virulence 2021, 12, 547–569. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hijazi, M.M.; Siepmann, T.; El-Battrawy, I.; Schrottner, P.; Podlesek, D.; Schackert, G.; Juratli, T.A.; Eyupoglu, I.Y.; Filis, A. The importance of the bacterial spectrum in the clinical diagnostics and management of patients with spontaneous pyogenic spondylodiscitis and isolated spinal epidural empyema: A 20-year cohort study at a single spine center. BMC Infect. Dis. 2024, 24, 39. [Google Scholar] [CrossRef] [PubMed]
- Lagacé-Wiens, P.R.; Adam, H.J.; Low, D.E.; Blondeau, J.M.; Baxter, M.R.; Denisuik, A.J.; Nichol, K.A.; Walkty, A.; Karlowsky, J.A.; Mulvey, M.R.; et al. Trends in antibiotic resistance over time among pathogens from Canadian hospitals: Results of the CANWARD study 2007–11. J. Antimicrob. Chemother. 2013, 68 (Suppl. 1), i23–i29. [Google Scholar] [CrossRef]
- Ntalos, D.; Berger-Groch, J.; Rohde, H.; Grossterlinden, L.G.; Both, A.; Luebke, A.; Hartel, M.J.; Klatte, T.O. Implementation of a multidisciplinary infections conference affects the treatment plan in prosthetic joint infections of the hip: A retrospective study. Arch. Orthop. Trauma Surg. 2019, 139, 467–473. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | UVH | NUH | p-Value |
|---|---|---|---|
| Age (years) | 63.6 ± 13.4 | 69.2 ± 13.4 | 0.020 |
| Female | 35.3% (24) | 40.3% (27) | 0.550 |
| Stay (hospital) | 31.8 ± 22.6 | 18.9 ± 11.6 | 0.002 |
| Stay (ICU) 1 | 8.9 ± 18.8 | 1.6 ± 5.2 | 0.015 |
| Admission | |||
| Acute Onset | 52.9% (36) | 38.5% (20) | 0.115 |
| Pain | 91.9% (57) | 100% (52) | 0.036 |
| -NAS 2 | 4.5 ± 3.0 | 6.6 ± 1.8 | 0.001 |
| Neurological deficit | 19.7% (13) | 11.5% (6) | 0.231 |
| -Myelopathy | 11.8% (8) | 8.2% (4) | 0.597 |
| -Radiculopathy | 7.4% (5) | 4.1% (2) | |
| Fever 3 | 7.5% (5) | 16.1 (10) | 0.125 |
| Leukocytosis | 39.7% (27) | 44.3% (27) | 0.600 |
| CRP-Elevation 4 | 95.6% (65) | 93.9% (62) | 0.668 |
| Feature | UVH | NUH | p-Value |
|---|---|---|---|
| Previous spine surgery | 17.6% (12) | 17.9% (12) | 0.968 |
| Previous infiltration therapy | 7.4% (5) | 7.5% (5) | 0.981 |
| Diabetes | 19.1% (13) | 16.4% (11) | 0.682 |
| Pyogenic infection | 5.9% (4) | 14.9% (10) | 0.085 |
| Intravenous drug abuse | 7.4% (5) | 7.5% (5) | 0.981 |
| Malignancy | 30.9% (21) | 9.0% (6) | 0.001 |
| -Chemotherapy | 4.5% (3) | 0.0% (0) | 0.078 |
| -Port | 1.5% (1) | 3.0% (2) | 0.551 |
| Renal insufficiency | 16.2% (11) | 11.9% (8) | 0.479 |
| Microbiological Group Comparison | ||||||
|---|---|---|---|---|---|---|
| UVH | NUH | p-Value | ||||
| Bacteria Groups | S. Aureus | 22 | 37.3% | 10 | 31.3% | 0.13 |
| Coag. Neg. Staph. | 17 | 28.8% | 11 | 34.4% | ||
| Enterobacterales | 4 | 6.8% | 1 | 3.1% | ||
| Streptococcus sp. | 1 | 1.7% | 5 | 15.6% | ||
| Enterococcus sp. | 4 | 6.8% | 3 | 9.4% | ||
| Mycobact. tuberculosis | 3 | 5.1% | 0 | 0.0% | ||
| Miscellaneous | 8 | 13.6% | 2 | 6.3% | ||
| i.v. treatment/days | 29.6 ± 22.9 | 9.8 ± 4.4 | <0.001 | |||
| oral treatment/weeks | 7.2 ± 5.9 | 12.2 ± 3.6 | <0.001 | |||
| Resistances | |||||
|---|---|---|---|---|---|
| UVH | NUH | p-Value | |||
| Penicillin | 36/46 | 78.3% | 17/24 | 70.8% | 0.562 |
| Isoxazolyl-Penicillin | 23/46 | 50.0% | 9/24 | 37.5% | 0.449 |
| Aminopenicillin | 8/46 | 17.4% | 8/24 | 33.3% | 0.147 |
| Cephalosporins | 4/46 | 8.7% | 11/24 | 45.8% | 0.001 |
| Carbapenems | 12/46 | 26.1% | 2/24 | 8.3% | 0.116 |
| Quinolons I–II | 14/46 | 30.4% | 7/24 | 29.2% | 1.000 |
| Quinolons III–IV | 0/46 | 0.00% | 6/24 | 25.00% | 0.001 |
| Macrolides | 18/46 | 39.1% | 10/24 | 41.7% | 1.000 |
| Aminoglycosides | 7/46 | 15.2% | 2/24 | 8.3% | 0.708 |
| Glycopeptides | 4/46 | 8.7% | 0/24 | 0.0% | 0.291 |
| Tetracyclines | 9/46 | 19.6% | 3/24 | 12.5% | 0.526 |
| Lincosamides | 13/46 | 28.3% | 9/24 | 37.5% | 0.433 |
| Nitroimidazoles | 1/46 | 2.2% | 4/24 | 16.7% | 0.044 |
| Sulfonamides | 10/46 | 21.7% | 4/24 | 16.7% | 0.758 |
| Linezolid | 0/46 | 0.00% | 1/24 | 4.2% | 0.343 |
| Rifampicin | 4/46 | 8.7% | 2/24 | 8.3% | 1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pantel, T.; Mende, K.C.; Stangenberg, M.; Mohme, M.; Mohme, T.; Floeth, F.; Eicker, S.O.; Dreimann, M. Regional Spondylodiscitis Disparities: Impact on Pathogen Spectrum and Patients. J. Clin. Med. 2024, 13, 2557. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092557
Pantel T, Mende KC, Stangenberg M, Mohme M, Mohme T, Floeth F, Eicker SO, Dreimann M. Regional Spondylodiscitis Disparities: Impact on Pathogen Spectrum and Patients. Journal of Clinical Medicine. 2024; 13(9):2557. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092557
Chicago/Turabian StylePantel, Tobias, Klaus Christian Mende, Martin Stangenberg, Malte Mohme, Theresa Mohme, Frank Floeth, Sven Oliver Eicker, and Marc Dreimann. 2024. "Regional Spondylodiscitis Disparities: Impact on Pathogen Spectrum and Patients" Journal of Clinical Medicine 13, no. 9: 2557. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13092557