
Comparative Outcomes of Open Radical Cystectomy vs. Robot-Assisted Approaches with Intracorporeal and Extracorporeal Urinary Diversion: A Meta-Analysis and Network Meta-Analysis of Perioperative and Quality of Life Outcomes
 , , , , ,
, , , , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Risk of Bias Assessment
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
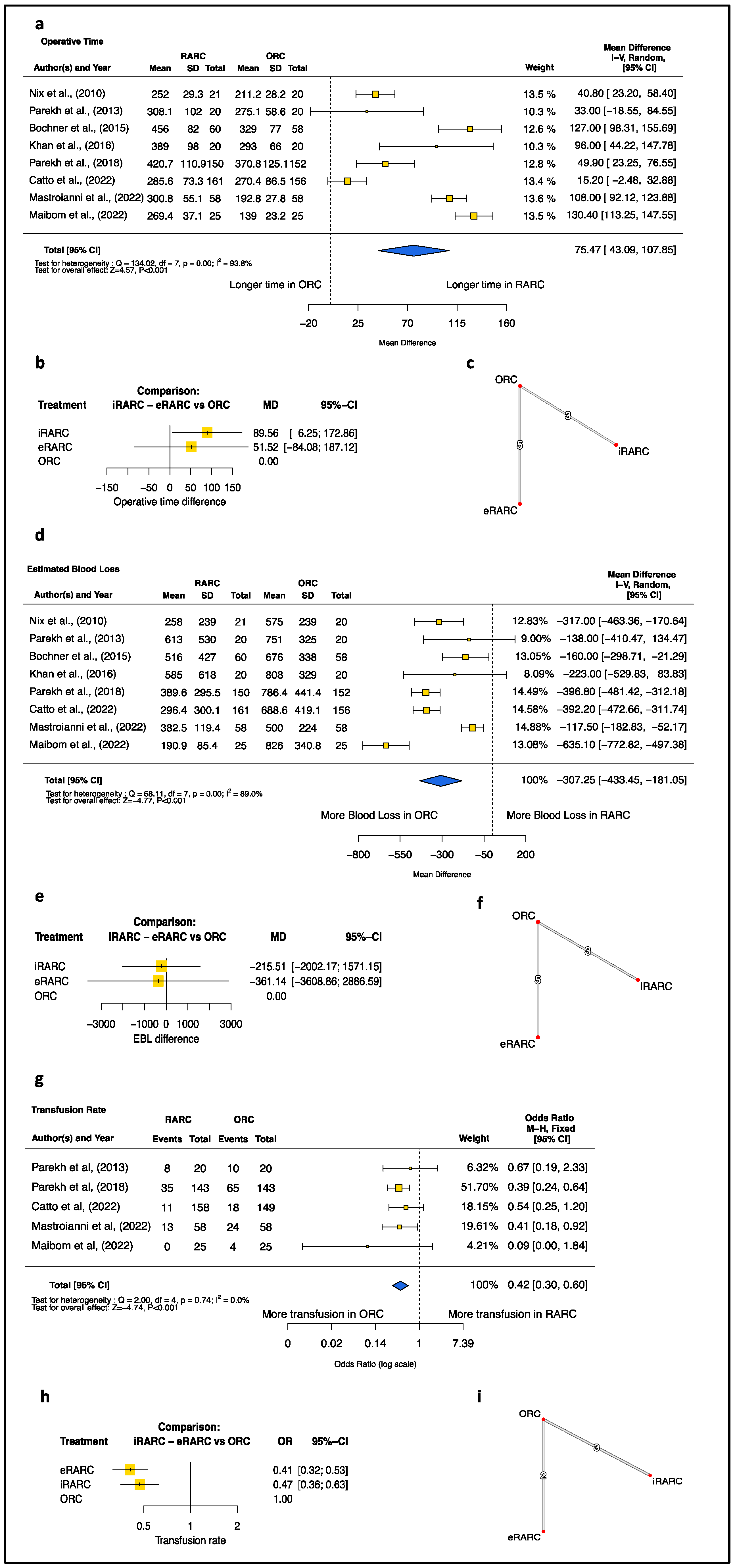
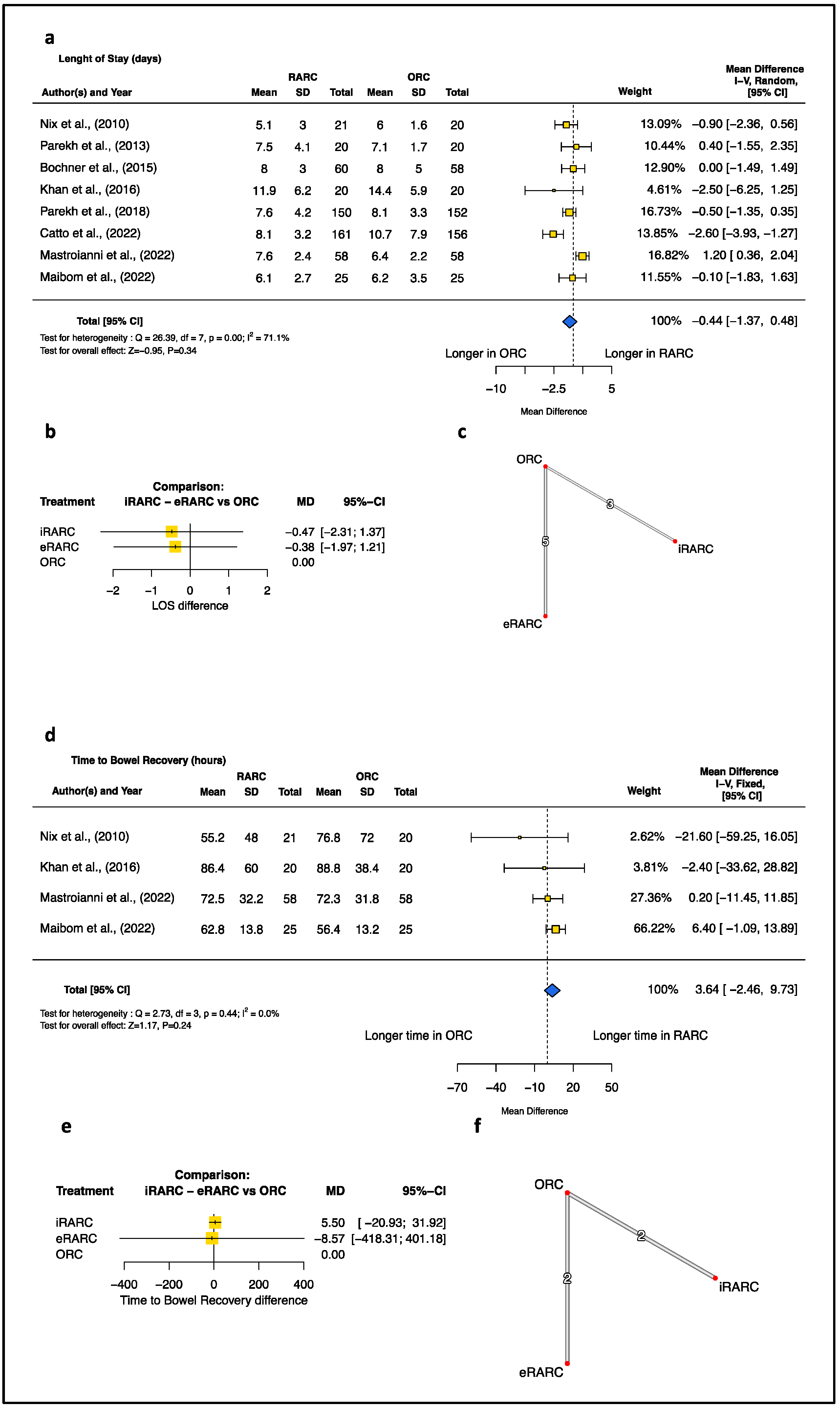
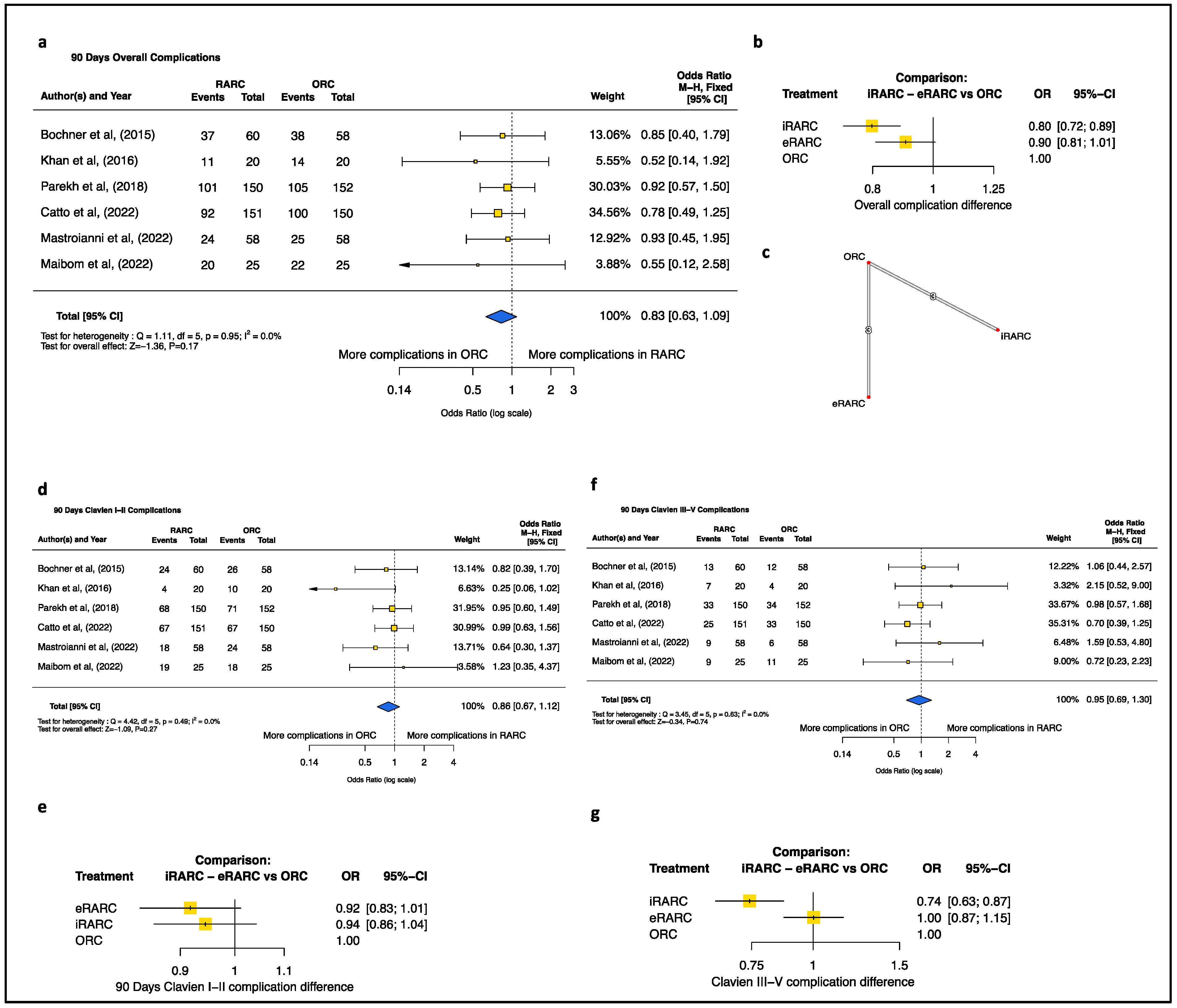
3.2. Perioperative Outcomes: RARC vs. ORC
3.3. Perioperative Outcomes: ECUD vs. ICUD vs. ORC
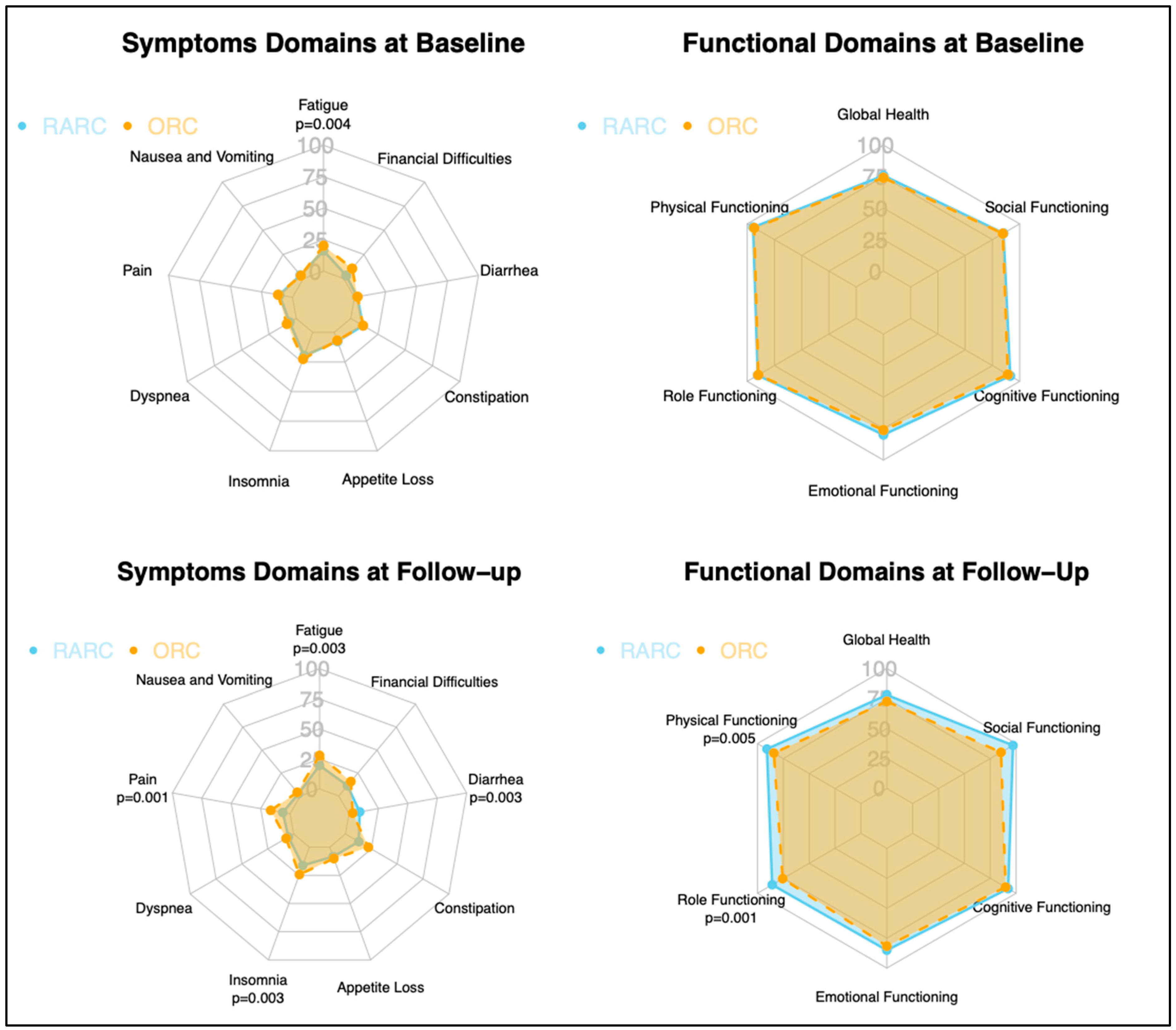
3.4. Quality of Life Assessment: RARC vs. ORC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alfred Witjes, J.; Max Bruins, H.; Carrión, A.; Cathomas, R.; Compérat, E.; Efstathiou, J.A.; Fietkau, R.; Gakis, G.; Lorch, A.; Martini, A.; et al. European Association of Urology Guidelines on Muscle-Invasive and Metastatic Bladder Cancer: Summary of the 2023 Guidelines. Eur. Urol. 2023, 85, 17–31. [Google Scholar] [CrossRef] [PubMed]
- Leonardo, C.; Flammia, R.S.; Lucciola, S.; Proietti, F.; Pecoraro, M.; Bucca, B.; Licari, L.C.; Borrelli, A.; Bologna, E.; Landini, N.; et al. Performance of Node-RADS Scoring System for a Standardized Assessment of Regional Lymph Nodes in Bladder Cancer Patients. Cancers 2023, 15, 580. [Google Scholar] [CrossRef] [PubMed]
- Leow, J.J.; Reese, S.W.; Jiang, W.; Lipsitz, S.R.; Bellmunt, J.; Trinh, Q.-D.; Chung, B.I.; Kibel, A.S.; Chang, S.L. Propensity-Matched Comparison of Morbidity and Costs of Open and Robot-Assisted Radical Cystectomies: A Contemporary Population-Based Analysis in the United States. Eur. Urol. 2014, 66, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Shabsigh, A.; Korets, R.; Vora, K.C.; Brooks, C.M.; Cronin, A.M.; Savage, C.; Raj, G.; Bochner, B.H.; Dalbagni, G.; Herr, H.W.; et al. Defining Early Morbidity of Radical Cystectomy for Patients with Bladder Cancer Using a Standardized Reporting Methodology. Eur. Urol. 2009, 55, 164–176. [Google Scholar] [CrossRef] [PubMed]
- Autorino, R.; Zargar, H.; Kaouk, J.H. Robotic-Assisted Laparoscopic Surgery: Recent Advances in Urology. Fertil Steril. 2014, 102, 939–949. [Google Scholar] [CrossRef] [PubMed]
- Zamboni, S.; Soria, F.; Mathieu, R.; Xylinas, E.; Abufaraj, M.; D`Andrea, D.; Tan, W.S.; Kelly, J.D.; Simone, G.; Gallucci, M.; et al. Differences in Trends in the Use of Robot-assisted and Open Radical Cystectomy and Changes over Time in Peri-operative Outcomes among Selected Centres in North America and Europe: An International Multicentre Collaboration. BJU Int. 2019, 124, 656–664. [Google Scholar] [CrossRef] [PubMed]
- Soria, F.; Moschini, M.; D’andrea, D.; Abufaraj, M.; Foerster, B.; Mathiéu, R.; Gust, K.M.; Gontero, P.; Simone, G.; Meraney, A.; et al. Comparative Effectiveness in Perioperative Outcomes of Robotic versus Open Radical Cystectomy: Results from a Multicenter Contemporary Retrospective Cohort Study. Eur. Urol. Focus 2020, 6, 1233–1239. [Google Scholar] [CrossRef] [PubMed]
- Nazzani, S.; Mazzone, E.; Preisser, F.; Bandini, M.; Tian, Z.; Marchioni, M.; Ratti, D.; Motta, G.; Zorn, K.C.; Briganti, A.; et al. Comparison of Perioperative Outcomes Between Open and Robotic Radical Cystectomy: A Population-Based Analysis. J. Endourol. 2018, 32, 701–709. [Google Scholar] [CrossRef]
- Parekh, D.J.; Reis, I.M.; Castle, E.P.; Gonzalgo, M.L.; Woods, M.E.; Svatek, R.S.; Weizer, A.Z.; Konety, B.R.; Tollefson, M.; Krupski, T.L.; et al. Robot-Assisted Radical Cystectomy versus Open Radical Cystectomy in Patients with Bladder Cancer (RAZOR): An Open-Label, Randomised, Phase 3, Non-Inferiority Trial. Lancet 2018, 391, 2525–2536. [Google Scholar] [CrossRef]
- Catto, J.W.F.; Khetrapal, P.; Ricciardi, F.; Ambler, G.; Williams, N.R.; Al-Hammouri, T.; Khan, M.S.; Thurairaja, R.; Nair, R.; Feber, A.; et al. Effect of Robot-Assisted Radical Cystectomy With Intracorporeal Urinary Diversion vs Open Radical Cystectomy on 90-Day Morbidity and Mortality Among Patients With Bladder Cancer. JAMA 2022, 327, 2092. [Google Scholar] [CrossRef]
- Rai, B.P.; Bondad, J.; Vasdev, N.; Adshead, J.; Lane, T.; Ahmed, K.; Khan, M.S.; Dasgupta, P.; Guru, K.; Chlosta, P.L.; et al. Robotic versus Open Radical Cystectomy for Bladder Cancer in Adults. Cochrane Database Syst. Rev. 2019, 4, CD011903. [Google Scholar] [CrossRef] [PubMed]
- Hussein, A.A.; May, P.R.; Jing, Z.; Ahmed, Y.E.; Wijburg, C.J.; Canda, A.E.; Dasgupta, P.; Shamim Khan, M.; Menon, M.; Peabody, J.O.; et al. Outcomes of Intracorporeal Urinary Diversion after Robot-Assisted Radical Cystectomy: Results from the International Robotic Cystectomy Consortium. J. Urol. 2018, 199, 1302–1311. [Google Scholar] [CrossRef] [PubMed]
- Tan, T.W.; Nair, R.; Saad, S.; Thurairaja, R.; Khan, M.S. Safe Transition from Extracorporeal to Intracorporeal Urinary Diversion Following Robot-Assisted Cystectomy: A Recipe for Reducing Operative Time, Blood Loss and Complication Rates. World J. Urol. 2019, 37, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Canda, A.E.; Atmaca, A.F.; Altinova, S.; Akbulut, Z.; Balbay, M.D. Robot-assisted Nerve-sparing Radical Cystectomy with Bilateral Extended Pelvic Lymph Node Dissection (PLND) and Intracorporeal Urinary Diversion for Bladder Cancer: Initial Experience in 27 Cases. BJU Int. 2012, 110, 434–444. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, K.; Khan, S.A.; Hayn, M.H.; Agarwal, P.K.; Badani, K.K.; Balbay, M.D.; Castle, E.P.; Dasgupta, P.; Ghavamian, R.; Guru, K.A.; et al. Analysis of Intracorporeal Compared with Extracorporeal Urinary Diversion After Robot-Assisted Radical Cystectomy: Results from the International Robotic Cystectomy Consortium. Eur. Urol. 2014, 65, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Katayama, S.; Mori, K.; Pradere, B.; Mostafaei, H.; Schuettfort, V.M.; Quhal, F.; Motlagh, R.S.; Laukhtina, E.; Moschini, M.; Grossmann, N.C.; et al. Intracorporeal versus Extracorporeal Urinary Diversion in Robot-Assisted Radical Cystectomy: A Systematic Review and Meta-Analysis. Int. J. Clin. Oncol. 2021, 26, 1587–1599. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo Classification of Surgical Complications. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Kaasa, S.; Bjordal, K.; Aaronson, N.; Moum, T.; Wist, E.; Hagen, S.; Kvikstad, A. The EORTC Core Quality of Life Questionnaire (QLQ-C30): Validity and Reliability When Analysed with Patients Treated with Palliative Radiotherapy. Eur. J. Cancer 1995, 31, 2260–2263. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- McGrath, S.; Zhao, X.; Steele, R.; Thombs, B.D.; Benedetti, A.; Levis, B.; Riehm, K.E.; Saadat, N.; Levis, A.W.; Azar, M.; et al. Estimating the Sample Mean and Standard Deviation from Commonly Reported Quantiles in Meta-Analysis. Stat. Methods Med. Res. 2020, 29, 2520–2537. [Google Scholar] [CrossRef]
- Cohen, J.F.; Chalumeau, M.; Cohen, R.; Korevaar, D.A.; Khoshnood, B.; Bossuyt, P.M.M. Cochran’s Q Test Was Useful to Assess Heterogeneity in Likelihood Ratios in Studies of Diagnostic Accuracy. J. Clin. Epidemiol. 2015, 68, 299–306. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting Meta-Analyses in R with the Metafor Package. J Stat Softw 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Balduzzi, S.; Rücker, G.; Nikolakopoulou, A.; Papakonstantinou, T.; Salanti, G.; Efthimiou, O.; Schwarzer, G. Netmeta: An R Package for Network Meta-Analysis Using Frequentist Methods. J. Stat. Softw. 2023, 106, 1–40. [Google Scholar] [CrossRef]
- Nix, J.; Smith, A.; Kurpad, R.; Nielsen, M.E.; Wallen, E.M.; Pruthi, R.S. Prospective Randomized Controlled Trial of Robotic versus Open Radical Cystectomy for Bladder Cancer: Perioperative and Pathologic Results. Eur. Urol. 2010, 57, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Parekh, D.J.; Messer, J.; Fitzgerald, J.; Ercole, B.; Svatek, R. Perioperative Outcomes and Oncologic Efficacy from a Pilot Prospective Randomized Clinical Trial of Open Versus Robotic Assisted Radical Cystectomy. J. Urol. 2013, 189, 474–479. [Google Scholar] [CrossRef]
- Bochner, B.H.; Dalbagni, G.; Sjoberg, D.D.; Silberstein, J.; Keren Paz, G.E.; Donat, S.M.; Coleman, J.A.; Mathew, S.; Vickers, A.; Schnorr, G.C.; et al. Comparing Open Radical Cystectomy and Robot-Assisted Laparoscopic Radical Cystectomy: A Randomized Clinical Trial. Eur. Urol. 2015, 67, 1042–1050. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.S.; Gan, C.; Ahmed, K.; Ismail, A.F.; Watkins, J.; Summers, J.A.; Peacock, J.L.; Rimington, P.; Dasgupta, P. A Single-Centre Early Phase Randomised Controlled Three-Arm Trial of Open, Robotic, and Laparoscopic Radical Cystectomy (CORAL). Eur. Urol. 2016, 69, 613–621. [Google Scholar] [CrossRef]
- Mastroianni, R.; Ferriero, M.; Tuderti, G.; Anceschi, U.; Bove, A.M.; Brassetti, A.; Misuraca, L.; Zampa, A.; Torregiani, G.; Ghiani, E.; et al. Open Radical Cystectomy versus Robot-Assisted Radical Cystectomy with Intracorporeal Urinary Diversion: Early Outcomes of a Single-Center Randomized Controlled Trial. J. Urol. 2022, 207, 982–992. [Google Scholar] [CrossRef]
- Maibom, S.L.; Røder, M.A.; Aasvang, E.K.; Rohrsted, M.; Thind, P.O.; Bagi, P.; Kistorp, T.; Poulsen, A.M.; Salling, L.N.; Kehlet, H.; et al. Open vs Robot-assisted Radical Cystectomy (BORARC): A Double-blinded, Randomised Feasibility Study. BJU Int. 2022, 130, 102–113. [Google Scholar] [CrossRef]
- Lenfant, L.; Campi, R.; Parra, J.; Graffeille, V.; Masson-Lecomte, A.; Vordos, D.; de La Taille, A.; Roumiguie, M.; Lesourd, M.; Taksin, L.; et al. Robotic versus Open Radical Cystectomy throughout the Learning Phase: Insights from a Real-Life Multicenter Study. World J. Urol. 2020, 38, 1951–1958. [Google Scholar] [CrossRef]
- Sung, H.H.; Ahn, J.-S.; Seo, S., II; Jeon, S.S.; Choi, H.Y.; Lee, H.M.; Jeong, B.C. A Comparison of Early Complications Between Open and Robot-Assisted Radical Cystectomy. J. Endourol. 2012, 26, 670–675. [Google Scholar] [CrossRef]
- Morozov, A.; Babaevskaya, D.; Taratkin, M.; Inoyatov, J.; Laukhtina, E.; Moschini, M.; Singla, N.; Gomez Rivas, J.; Teoh, J.Y.-C.; Glybochko, P.; et al. Systematic Review: The Learning Curve for Robot-Assisted Radical Cystectomy—What Do We Know? J. Endourol. 2022, 36, 770–784. [Google Scholar] [CrossRef] [PubMed]
- Bertolo, R.; Agudelo, J.; Garisto, J.; Armanyous, S.; Fergany, A.; Kaouk, J. Perioperative Outcomes and Complications after Robotic Radical Cystectomy With Intracorporeal or Extracorporeal Ileal Conduit Urinary Diversion: Head-to-Head Comparison From a Single-Institutional Prospective Study. Urology 2019, 129, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Hanna, N.; Leow, J.J.; Sun, M.; Friedlander, D.F.; Seisen, T.; Abdollah, F.; Lipsitz, S.R.; Menon, M.; Kibel, A.S.; Bellmunt, J.; et al. Comparative Effectiveness of Robot-Assisted vs. Open Radical Cystectomy. Urol. Oncol. Semin. Orig. Investig. 2018, 36, 88.e1–88.e9. [Google Scholar] [CrossRef]
- Khetrapal, P.; Wong, J.K.L.; Tan, W.P.; Rupasinghe, T.; Tan, W.S.; Williams, S.B.; Boorjian, S.A.; Wijburg, C.; Parekh, D.J.; Wiklund, P.; et al. Robot-Assisted Radical Cystectomy Versus Open Radical Cystectomy: A Systematic Review and Meta-Analysis of Perioperative, Oncological, and Quality of Life Outcomes Using Randomized Controlled Trials. Eur. Urol. 2023, 84, 393–405. [Google Scholar] [CrossRef]
- Abou Chawareb, E.; Ayoub, C.H.; Najdi, J.; Ghoubaira, J.; El-Hajj, A. Preoperative Predictors of Prolonged Length of Stay in Radical Cystectomy: A Retrospective Study Using the American College of Surgeons-National Surgical Quality Improvement Program Dataset. Ther. Adv. Urol. 2023, 15, 7562872231191654. [Google Scholar] [CrossRef]
- Patel, H.R.H.; Cerantola, Y.; Valerio, M.; Persson, B.; Jichlinski, P.; Ljungqvist, O.; Hubner, M.; Kassouf, W.; Müller, S.; Baldini, G.; et al. Enhanced Recovery After Surgery: Are We Ready, and Can We Afford Not to Implement These Pathways for Patients Undergoing Radical Cystectomy? Eur. Urol. 2014, 65, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Maffezzini, M.; Campodonico, F.; Canepa, G.; Gerbi, G.; Parodi, D. Current Perioperative Management of Radical Cystectomy with Intestinal Urinary Reconstruction for Muscle-Invasive Bladder Cancer and Reduction of the Incidence of Postoperative Ileus. Surg. Oncol. 2008, 17, 41–48. [Google Scholar] [CrossRef]
- Hussein, A.A.; Elsayed, A.S.; Aldhaam, N.A.; Jing, Z.; Peabody, J.O.; Wijburg, C.J.; Wagner, A.; Canda, A.E.; Khan, M.S.; Scherr, D.; et al. A Comparative Propensity Score-matched Analysis of Perioperative Outcomes of Intracorporeal vs. Extracorporeal Urinary Diversion after Robot-assisted Radical Cystectomy: Results from the International Robotic Cystectomy Consortium. BJU Int. 2020, 126, 265–272. [Google Scholar] [CrossRef]
- Mastroianni, R.; Tuderti, G.; Anceschi, U.; Bove, A.M.; Brassetti, A.; Ferriero, M.; Zampa, A.; Giannarelli, D.; Guaglianone, S.; Gallucci, M.; et al. Comparison of Patient-Reported Health-Related Quality of Life Between Open Radical Cystectomy and Robot-Assisted Radical Cystectomy with Intracorporeal Urinary Diversion: Interim Analysis of a Randomised Controlled Trial. Eur. Urol. Focus 2022, 8, 465–471. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Study Design | Year | Country | N. of Patients per Group (n) | UD | Age (Years) | Male (%) | BMI | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RARC | oRC | RARC | oRC | RARC | oRC | RARC | oRC | |||||
| Nix et al. [25] | Single-center RCT | 2010 | USA | 21 | 20 | ECUD | 67.4 (33–81) a | 69.2 (51–80) a | 66.7 | 85 | 27.5 (−) b | 28.5 (−) b |
| Parekh et al. [26] | Single-center RCT | 2013 | USA | 20 | 20 | ECUD | 69.5 (62.3–74) c | 64.5 (59.8- 72.3) c | 90 | 80 | 27.6 (24.2–29.9) c | 28.3 (26.1–32.3) c |
| Bochner et al. [27] | Single-center RCT | 2015 | USA | 60 | 58 | ECUD | 66 (60–71) c | 65 (58–69) c | 85 | 72 | 27.9 (24.7–31.0) c | 29.0 (26.3–33.7) c |
| Khan et al. [28] | Single-center RCT | 2016 | GB | 20 | 20 | ECUD | 68.6 (6.8) b | 68.6 (9.9) b | 85 | 90 | 27.5 (4.2) b | 27.4 (3.9) b |
| Parekh et al. [9] | Multicenter RCT | 2018 | USA | 150 | 152 | ECUD | 70 (43–90) c | 67 (37–85) c | 84 | 84 | 27.8 (25.0–30.8) c | 28.2 (24.9–31.7) c |
| Catto et al. [10] | Multicenter RCT | 2022 | GB | 161 | 156 | ICUD | 69.3 (8.0) b | 68.7 (8.4) b | 80 | 78 |
|
|
| Mastroianni et al. [29] | Single-center RCT | 2022 | Italy | 58 | 58 | ICUD | 64 (53–70) c | 66 (58–71) c | 76 | 69 | 26 (23–28) c | 26 (24–29) c |
| Maibon et al. [30] | Single-center RCT | 2022 | Denmark | 25 | 25 | ICUD | 70 (63–74) c | 67 (59–74) c | 72 | 80 | 27.3 (23.3–29.4) c | 26.9 (22.9–29.6) c |
| Author | ASA | nCHT (%) | pT (%) | pN (%) | ||||
|---|---|---|---|---|---|---|---|---|
| RARC | oRC | RARC | oRC | RARC | oRC | RARC | oRC | |
| Nix et al. [25] | 2.71 (mean) | 2.70 | - | - | ≤pT2 = 66.6 >pT2 = 14.3 | ≤pT2 = 40 >pT2 = 25 | pN+ = 19 | pN+ = 35 |
| Parekh et al. [26] | 3 (median) | 3 | 30 | 25 | ≤pT2 = 50 >pT2 = 50 | ≤pT2 = 65 >pT2 = 35 | pN+ = 20 | pN+ = 20 |
| Bochner et al. [27] | 2 = 28% 3 = 70% 4 = 1.7% | 2 = 21% 3 = 74% 4 = 5.2% | 31.7 | 44.8 | ≤pT2 = 71.6 >pT2 = 28.4 | ≤pT2 = 67.2 >pT2 = 32.8 | pN+ = 17 | pN+ = 16 |
| Khan et al. [28] | 1 = 20% 2 = 75% 3 = 5% | 1 = 20% 2 = 75% 3 = 5% | 10 | 15 | ≤pT2 = 70 > pT2 = 30 | ≤pT2 = 70 >pT2 = 30 | - | - |
| Parekh et al. [9] | ECOG 0 = 78% ECOG 1 = 19% ECOG 2–3 = 3% | ECOG 0 = 72% ECOG 1 = 26% ECOG 2–3 = 3% | 27.3 | 36.2 | ≤pT2 = 69.3 >pT2 = 30.7 | ≤pT2 = 68.4 >pT2 = 31.6 | pN+ = 23 | pN+ = 24 |
| Catto et al. [10] | ECOG 0 = 81% ECOG 1 = 15% ECOG 2–3 = 3% | ECOG 0 = 81% ECOG 1 = 17% ECOG 2–3 = 2% | 33.5 | 33.9 | ≤pT2 = 70 >pT2 = 30 | ≤pT2 = 75 >pT2 = 25 | pN+ = 18 | pN+ = 17 |
| Mastroianni et al. [29] | 1 = 3% 2 = 74% 3 = 22% | 1 = 3% 2 = 86% 3 = 10% | 39.6 | 37.9 | ≤pT2 = 63 >pT2 = 37 | ≤pT2 = 67 >pT2 = 33 | pN+ = 13 | pN+ = 14 |
| Maibon et al. [30] | 1 = 8% 2 = 72% 3 = 20% | 1 = 12% 2 = 76% 3 = 12% | 36 | 40 | ≤pT2 = 88 >pT2 = 12 | ≤pT2 = 84 >pT2 = 16 | pN+ = 12 | pN+ = 28 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flammia, R.S.; Licari, L.C.; Bologna, E.; Mastroianni, R.; Proietti, F.; Tuderti, G.; Anceschi, U.; Brassetti, A.; Franco, A.; De Nunzio, C.; et al. Comparative Outcomes of Open Radical Cystectomy vs. Robot-Assisted Approaches with Intracorporeal and Extracorporeal Urinary Diversion: A Meta-Analysis and Network Meta-Analysis of Perioperative and Quality of Life Outcomes. J. Clin. Med. 2024, 13, 2421. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13082421
Flammia RS, Licari LC, Bologna E, Mastroianni R, Proietti F, Tuderti G, Anceschi U, Brassetti A, Franco A, De Nunzio C, et al. Comparative Outcomes of Open Radical Cystectomy vs. Robot-Assisted Approaches with Intracorporeal and Extracorporeal Urinary Diversion: A Meta-Analysis and Network Meta-Analysis of Perioperative and Quality of Life Outcomes. Journal of Clinical Medicine. 2024; 13(8):2421. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13082421
Chicago/Turabian StyleFlammia, Rocco Simone, Leslie Claire Licari, Eugenio Bologna, Riccardo Mastroianni, Flavia Proietti, Gabriele Tuderti, Umberto Anceschi, Aldo Brassetti, Antonio Franco, Cosimo De Nunzio, and et al. 2024. "Comparative Outcomes of Open Radical Cystectomy vs. Robot-Assisted Approaches with Intracorporeal and Extracorporeal Urinary Diversion: A Meta-Analysis and Network Meta-Analysis of Perioperative and Quality of Life Outcomes" Journal of Clinical Medicine 13, no. 8: 2421. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13082421