
A Nomogram for Predicting ADHD and ASD in Child and Adolescent Mental Health Services (CAMHS)
 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Outcome Variables
2.3. Potential Predictors
2.4. Statistical Analyses
2.5. Graphical Outcomes: Nomograms
3. Results
4. Discussion
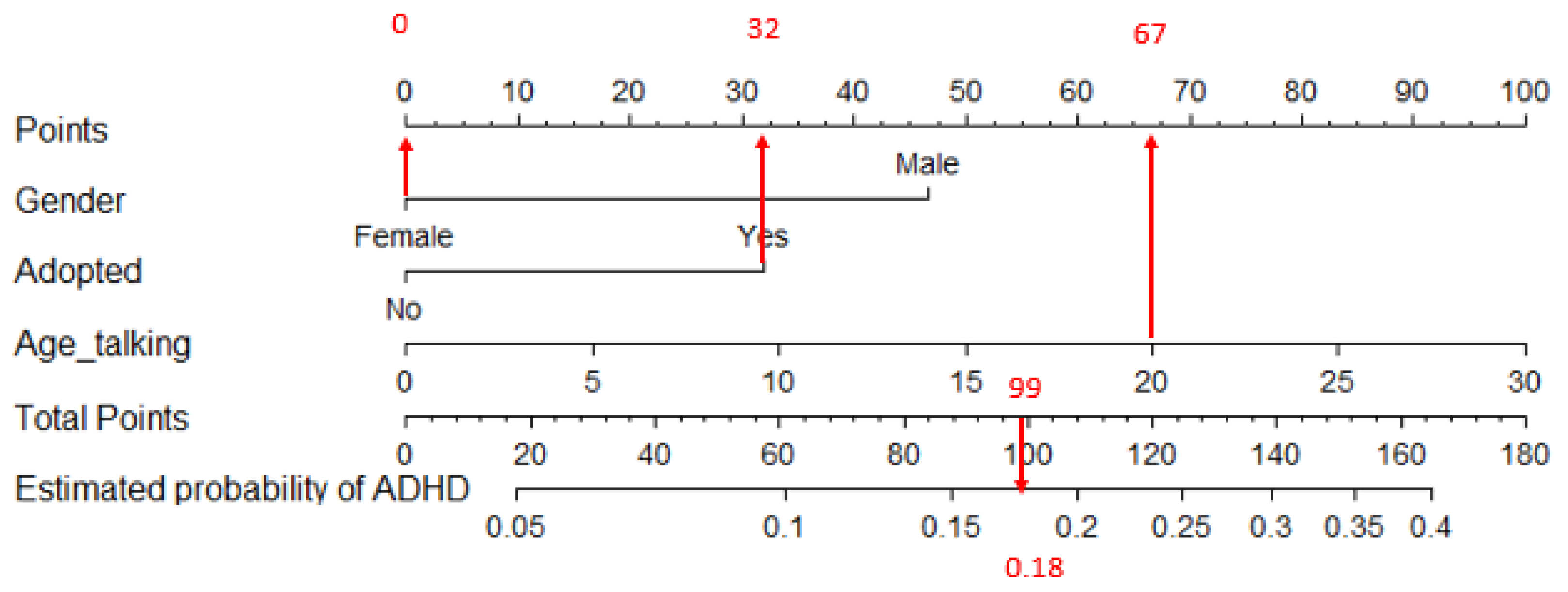
4.1. Predictors of ADHD
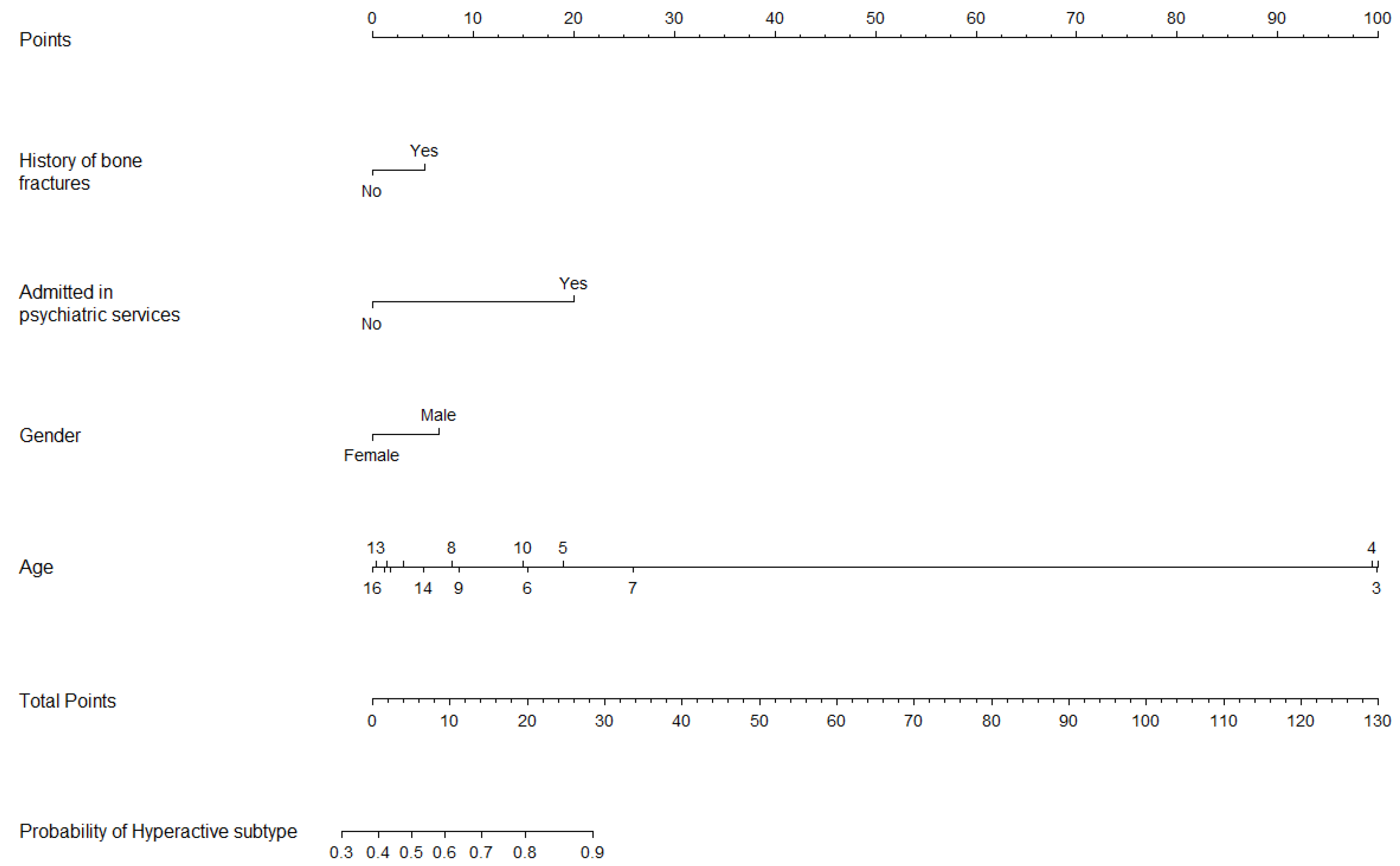
4.2. Predictors of ADHD, Hyperactive/Combined Subtype
4.3. Predictors of ASD
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Polanczyk, G.; De Lima, M.S.; Horta, B.L.; Biederman, J.; Rohde, L.A. The worldwide prevalence of ADHD: A systematic review and metaregression analysis. Am. J. Psychiatry 2007, 164, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Polanczyk, G.V.; Willcutt, E.G.; Salum, G.A.; Kieling, C.; Rohde, L.A. ADHD prevalence estimates across three decades: An updated systematic review and meta-regression analysis. Int. J. Epidemiol. 2014, 43, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Knopf, A. Autism prevalence increases from 1 in 60 to 1 in 54: CDC. Brown Univ. Child Adolesc. Behav. Lett. 2020, 36, 4. [Google Scholar]
- Sciberras, E.; DePetro, A.; Mensah, F.; Hiscock, H. Association between sleep and working memory in children with ADHD: A cross-sectional study. Sleep Med. 2015, 16, 1192–1197. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, J.Y.; Lee, J.; Jeong, G.H.; Lee, E.; Lee, S.; Lee, K.H.; Kronbichler, A.; Stubbs, B.; Solmi, M. Environmental risk factors, protective factors, and peripheral biomarkers for ADHD: An umbrella review. Lancet Psychiatry 2020, 7, 955–970. [Google Scholar] [CrossRef]
- Gurevitz, M.; Geva, R.; Varon, M.; Leitner, Y. Early markers in infants and toddlers for development of ADHD. J. Atten. Disord. 2014, 18, 14–22. [Google Scholar] [CrossRef]
- Modabbernia, A.; Velthorst, E.; Reichenberg, A. Environmental risk factors for autism: An evidence-based review of systematic reviews and meta-analyses. Mol. Autism 2017, 8, 13. [Google Scholar] [CrossRef]
- Lin, Y.; Wang, G.; Yang, Y.; Jin, X.; Huang, H.; Zhang, Y.; Jin, Z. Risk factors for ASD. J. Autism Dev. Disord. 2022, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Association, A.P. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Brower, V. Biomarkers: Portents of malignancy. Nature 2011, 471, S19–S20. [Google Scholar] [CrossRef]
- Lee, D.; Jang, H.I.; Kim, H.J.; Bae, J.; Park, J.H. Development of a Machine-Learning Predictive Model for First-Grade Children at Risk for ADHD. Korean J. Childcare Educ. 2021, 17, 83–103. [Google Scholar]
- Tachmazidis, I.; Chen, T.; Adamou, M.; Antoniou, G. A hybrid AI approach for supporting clinical diagnosis of attention deficit hyperactivity disorder (ADHD) in adults. Health Inf. Sci. Syst. 2021, 9, 1. [Google Scholar] [CrossRef] [PubMed]
- Slobodin, O.; Yahav, I.; Berger, I. A machine-based prediction model of ADHD using CPT data. Front. Hum. Neurosci. 2020, 14, 560021. [Google Scholar] [CrossRef] [PubMed]
- Sen, B.; Borle, N.C.; Greiner, R.; Brown, M.R. A general prediction model for the detection of ADHD and Autism using structural and functional MRI. PLoS ONE 2018, 13, e0194856. [Google Scholar] [CrossRef] [PubMed]
- Maniruzzaman, M.; Shin, J.; Hasan, M.A.M. Predicting Children with ADHD Using Behavioral Activity: A Machine Learning Analysis. Appl. Sci. 2022, 12, 2737. [Google Scholar] [CrossRef]
- Garcia-Argibay, M.; Zhang-James, Y.; Cortese, S.; Lichtenstein, P.; Larsson, H.; Faraone, S.V. Predicting childhood and adolescent attention-deficit/hyperactivity disorder onset: A nationwide deep learning approach. Mol. Psychiatry 2023, 28, 1232–1239. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, M.; Hironaka, L.K.; Feinberg, E.; Sandler, J.; Pellicer, M.; Chen, N.; Cabral, H. Using clinical data to predict accurate ADHD diagnoses among urban children. Clin. Pediatr. 2016, 55, 326–332. [Google Scholar] [CrossRef]
- Caye, A.; Agnew-Blais, J.; Arseneault, L.; Gonçalves, H.; Kieling, C.; Langley, K.; Menezes, A.; Moffitt, T.; Passos, I.; Rocha, T. A risk calculator to predict adult attention-deficit/hyperactivity disorder: Generation and external validation in three birth cohorts and one clinical sample. Epidemiol. Psychiatr. Sci. 2020, 29, e37. [Google Scholar] [CrossRef] [PubMed]
- Jagannatha, S.; Sargsyan, D.; Manyakov, N.V.; Skalkin, A.; Bangerter, A.; Ness, S.; Lewin, D.; Johnson, K.; Durham, K.; Pandina, G. A practical application of data mining methods to build predictive models for autism spectrum disorder based on biosensor data from Janssen Autism Knowledge Engine (JAKE®). Stat. Biopharm. Res. 2019, 11, 111–117. [Google Scholar] [CrossRef]
- Jiao, Y.; Chen, R.; Ke, X.; Chu, K.; Lu, Z.; Herskovits, E.H. Predictive models of autism spectrum disorder based on brain regional cortical thickness. Neuroimage 2010, 50, 589–599. [Google Scholar] [CrossRef]
- Wingfield, B.; Miller, S.; Yogarajah, P.; Kerr, D.; Gardiner, B.; Seneviratne, S.; Samarasinghe, P.; Coleman, S. A predictive model for paediatric autism screening. Health Inform. J. 2020, 26, 2538–2553. [Google Scholar] [CrossRef]
- Association, A.P. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV; American Psychiatric Association: Washington, DC, USA, 1994; Volume 4. [Google Scholar]
- Kim, J.H. Multicollinearity and misleading statistical results. Korean J. Anesthesiol. 2019, 72, 558–569. [Google Scholar] [CrossRef] [PubMed]
- Pencina, M.J.; D’Agostino, R.B. Evaluating discrimination of risk prediction models: The C statistic. JAMA 2015, 314, 1063–1064. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Felix, B.; García-Esquinas, E.; Muriel, A.; Royuela, A.; Zamora, J. Bootstrap internal validation command for predictive logistic regression models. Stata J. 2021, 21, 498–509. [Google Scholar] [CrossRef]
- Harrell, F.E., Jr.; Harrell, M.F.E., Jr.; Hmisc, D. Package ‘rms’. Vanderbilt Univ. 2017, 229, Q8. [Google Scholar]
- Salmerón-Gómez, R.; García-García, C.; García-Pérez, J. A guide to using the r package “multicoll” for detecting multicollinearity. Comput. Econ. 2021, 57, 529–536. [Google Scholar] [CrossRef]
- Pohlabeln, H.; Rach, S.; De Henauw, S.; Eiben, G.; Gwozdz, W.; Hadjigeorgiou, C.; Molnár, D.; Moreno, L.A.; Russo, P.; Veidebaum, T. Further evidence for the role of pregnancy-induced hypertension and other early life influences in the development of ADHD: Results from the IDEFICS study. Eur. Child Adolesc. Psychiatry 2017, 26, 957–967. [Google Scholar] [CrossRef] [PubMed]
- Von Gontard, A.; Equit, M. Comorbidity of ADHD and incontinence in children. Eur. Child Adolesc. Psychiatry 2015, 24, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Baeyens, D.; Roeyers, H.; Demeyere, I.; Verte, S.; Hoebeke, P.; Walle, J.V. Attention-deficit/hyperactivity disorder (ADHD) as a risk factor for persistent nocturnal enuresis in children: A two-year follow-up study. Acta Paediatr. 2005, 94, 1619–1625. [Google Scholar] [CrossRef] [PubMed]
- McKeown, C.; Hisle-Gorman, E.; Eide, M.; Gorman, G.H.; Nylund, C.M. Association of constipation and fecal incontinence with attention-deficit/hyperactivity disorder. Pediatrics 2013, 132, e1210–e1215. [Google Scholar] [CrossRef]
- Niemczyk, J.; Equit, M.; Hoffmann, L.; Von Gontard, A. Incontinence in children with treated attention-deficit/hyperactivity disorder. J. Pediatr. Urol. 2015, 11, 141.e1–141.e6. [Google Scholar] [CrossRef]
- Mellon, M.W.; Natchev, B.E.; Katusic, S.K.; Colligan, R.C.; Weaver, A.L.; Voigt, R.G.; Barbaresi, W.J. Incidence of enuresis and encopresis among children with attention-deficit/hyperactivity disorder in a population-based birth cohort. Acad. Pediatr. 2013, 13, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Seens, H.; Modarresi, S.; MacDermid, J.C.; Walton, D.M.; Grewal, R. Prevalence of bone fractures among children and adolescents with attention-deficit/hyperactivity disorder: A systematic review and meta-analysis. BMC Pediatr. 2021, 21, 354. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.-W.; Shen, D.; Yan, Y.-t. ADHD, stimulant medication use, and the risk of fracture: A systematic review and meta-analysis. Arch. Osteoporos. 2021, 16, 81. [Google Scholar] [CrossRef] [PubMed]
- Chen, V.C.-H.; Yang, Y.-H.; Liao, Y.-T.; Kuo, T.-Y.; Liang, H.-Y.; Huang, K.-Y.; Huang, Y.-C.; Lee, Y.; McIntyre, R.S.; Lin, T.-C. The association between methylphenidate treatment and the risk for fracture among young ADHD patients: A nationwide population-based study in Taiwan. PLoS ONE 2017, 12, e0173762. [Google Scholar]
- Schermann, H.; Gurel, R.; Ankory, R.; Kadar, A.; Yoffe, V.; Snir, N.; Sternheim, A.; Karakis, I. Lower risk of fractures under methylphenidate treatment for ADHD: A dose–response effect. J. Orthop. Res. 2018, 36, 3328–3333. [Google Scholar] [CrossRef] [PubMed]
- Schermann, H.; Ankory, R.; Shlaifer, A.; Dolkart, O.; Rotman, D.; Yoffe, V.; Karakis, I.; Chechik, O. Lower risk of stress fractures in young adults with ADHD under chronic treatment with methylphenidate. Bone 2019, 120, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Mattison, R.E.; Mayes, S.D. Relationships between learning disability, executive function, and psychopathology in children with ADHD. J. Atten. Disord. 2012, 16, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Loyer Carbonneau, M.; Demers, M.; Bigras, M.; Guay, M.-C. Meta-analysis of sex differences in ADHD symptoms and associated cognitive deficits. J. Atten. Disord. 2021, 25, 1640–1656. [Google Scholar] [CrossRef] [PubMed]
- Shilon, Y.; Pollak, Y.; Aran, A.; Shaked, S.; Gross-Tsur, V. Accidental injuries are more common in children with attention deficit hyperactivity disorder compared with their non-affected siblings. Child Care Health Dev. 2012, 38, 366–370. [Google Scholar] [CrossRef]
- Max, J.E.; Schachar, R.J.; Levin, H.S.; Ewing-Cobbs, L.; Chapman, S.B.; Dennis, M.; Saunders, A.; Landis, J. Predictors of attention-deficit/hyperactivity disorder within 6 months after pediatric traumatic brain injury. J. Am. Acad. Child Adolesc. Psychiatry 2005, 44, 1032–1040. [Google Scholar] [CrossRef]
- Sabuncuoglu, O.; Taser, H.; Berkem, M. Relationship between traumatic dental injuries and attention-deficit/hyperactivity disorder in children and adolescents: Proposal of an explanatory model. Dent. Traumatol. 2005, 21, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Nordström, T.; Hurtig, T.; Moilanen, I.; Taanila, A.; Ebeling, H. Disruptive behaviour disorder with and without attention deficit hyperactivity disorder is a risk of psychiatric hospitalization. Acta Paediatr. 2013, 102, 1100–1103. [Google Scholar] [CrossRef] [PubMed]
- Werling, D.M.; Geschwind, D.H. Sex differences in autism spectrum disorders. Curr. Opin. Neurol. 2013, 26, 146. [Google Scholar] [CrossRef] [PubMed]
- Giarelli, E.; Wiggins, L.D.; Rice, C.E.; Levy, S.E.; Kirby, R.S.; Pinto-Martin, J.; Mandell, D. Sex differences in the evaluation and diagnosis of autism spectrum disorders among children. Disabil. Health J. 2010, 3, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.; Smolen, C.; Girirajan, S. Gene discoveries in autism are biased towards comorbidity with intellectual disability. J. Med. Genet. 2020, 57, 647–652. [Google Scholar] [CrossRef] [PubMed]
- Bertelli, M.O. ASD and intellectual disability. In Psychopathology in Adolescents and Adults with Autism Spectrum Disorders; Springer: Berlin/Heidelberg, Germany, 2019; pp. 111–130. [Google Scholar]
- McDonald, C.A.; Donnelly, J.P.; Feldman-Alguire, A.L.; Rodgers, J.D.; Lopata, C.; Thomeer, M.L. Special education service use by children with autism spectrum disorder. J. Autism Dev. Disord. 2019, 49, 2437–2446. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, E.; Daniels, J.; Schieve, L.A.; Christensen, D.L.; Van Naarden Braun, K.; Rice, C.E.; Bakian, A.V.; Durkin, M.S.; Rosenberg, S.A.; Kirby, R.S. Trends in special education eligibility among children with autism spectrum disorder, 2002–2010. Public Health Rep. 2018, 133, 85–92. [Google Scholar] [CrossRef]
- DiGuiseppi, C.; Levy, S.E.; Sabourin, K.R.; Soke, G.N.; Rosenberg, S.; Lee, L.-C.; Moody, E.; Schieve, L.A. Injuries in children with autism spectrum disorder: Study to Explore Early Development (SEED). J. Autism Dev. Disord. 2018, 48, 461–472. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Operationalization | Categories | Frequencies or Mean (sd) * |
|---|---|---|---|
| Age | How old (in years) is the patient? | Continuous variable | 11.1 (3.9) |
| Gender | What is the gender of the patient? | Male (0) or Female (1) | Male = 593 Female = 276 |
| Adopted | Was the child adopted? | Yes (1) or No (0) | No = 798 Yes = 52 |
| Family (first grade) psychiatric antecedents | Does the patient have any first-grade relative formally diagnosed with any mental disorder? | Yes (1) or No (0) | No = 332 Yes = 471 |
| Risky pregnancy | Was the patient’s gestation a risky pregnancy? | Yes (1) or No (0) | No = 608 Yes = 236 |
| Use of toxic substances by the mother during pregnancy | Did the patient’s mother take any toxic substances during pregnancy? | Yes (1) or No (0) | No = 783 Yes = 18 |
| Stress/depression during pregnancy | Did the patient’s mother suffer stress or depression during pregnancy? | Yes (1) or No (0) | No = 644 Yes = 192 |
| Preeclampsia during pregnancy | Did the patient’s mother suffer preeclampsia during pregnancy? | Yes (1) or No (0) | No = 805 Yes = 23 |
| Comorbidity in Axis I (Clinical Disorders) | Does the patient have a second Axis I diagnosis? | Yes (1) or No (0) | No = 245 Yes = 616 |
| Diagnosis in Axis III | Does the patient have a diagnosis of a disorder included in Axis III (general medical condition)? | No = 59 Yes = 809 | |
| Atopy | Did the patient suffer atopy? | Yes (1) or No (0) | No = 485 Yes = 371 |
| History of bone fractures or repetitive injuries evaluated or not at the ER? | Has the patient ever suffered a bone fracture? Has the patient had repetitive injuries evaluated at the ER? | Yes (1) or No (0) | No = 469 Yes = 378 |
| Diagnosis in Axis IV | Does the patient have a diagnosis of a disorder included in Axis IV (psychosocial problems)? | Yes (1) or No (0) | No = 187 Yes = 661 |
| Disability | Does the patient suffer any disability? | Yes (1) or No (0) | No = 717 Yes = 140 |
| Urine control (day and evening) | Does the patient control his/her urine? | Yes (1) or No (0) | No = 112 Yes = 713 |
| Fecal control | Does the patient control his/her feces? | Yes (1) or No (0) | No = 162 Yes = 761 |
| Started walking | Age (in months) at which the patient started walking | Continuous | 15.76 (8.35) |
| Special education needs | Does the patient have any special education needs? | Yes (1) or No (0) | No = 716 Yes = 108 |
| Genetics | Any confirmed genetic disease? | Yes (1) or No (0) | No = 801 Yes = 43 |
| Physically active | Does the patient exercise regularly? | Yes (1) or No (0) | No = 259 Yes = 573 |
| Admitted to the psychiatric acute inpatient unit? | Has the patient ever been admitted to the psychiatric acute inpatient unit? | Yes (1) or No (0) | No = 794 Yes = 50 |
| Admitted (hospitalization) in pediatric services | Has the patient ever been hospitalized in pediatric services? | Yes (1) or No (0) | No = 709 Yes = 130 |
| Medical treatment | Is the patient taking any medication regarding a general medical condition? | Yes (1) or No (0) | No = 399 Yes = 461 |
| Axis V score | Which is the global assessment scale? (0–100) | Continuous | 68.98 (12.16) |
| Total | ADHD (n = 599) | No ADHD (n = 246) | p | Hyperactive/Combined (n = 414) | Inattentive (n = 185) | p | ASD (n = 84) | No ASD (n = 84) | p | |
|---|---|---|---|---|---|---|---|---|---|---|
| Age | 11.1 (3.9) | 11.6 (3.5) 3–18 | 9.8 (4.6) 1.5–22 | <0.001 | 11.1 (3.5) | 12.7 (3.0) | <0.001 | 8.6 (4.4) | 11.3 (3.7) | <0.001 |
| Sex (% Female) | 31.7% | 29.9% | 35.4% | 0.139 | 29.6% | 39.5% | <0.001 | 11.9% | 33.6% | <0.001 |
| Nationality (% Spanish) | 84.9% | 85.0% | 84.5% | 0.9375 | 86.4% | 84.4% | 0.599 | 76.2% | 85.8% | 0.029 |
| Model | Factor | OR (95% CI) | VIF | Condition Number |
|---|---|---|---|---|
| ADHD (n = 632) | Constant | 11.68 | ||
| Risky pregnancy (No = 0, Yes = 1) | 1.85 (1.14, 3.00) | 1.063 | ||
| Age of first words (in months) | 0.86 (0.73, 1.02) | 1.125 | ||
| Urine control (No = 0, Yes = 1) | 0.32 (0.13, 0.88) | 1.630 | ||
| Fecal control (No = 0, Yes = 1) | 7.14 (2.56, 19.23) | 1.623 | ||
| Special educational needs (No = 0, Yes = 1) | 0.29 (0.13, 0.63) | 1.445 | ||
| Disability (No = 0, Yes = 1) | 0.34 (0.18, 0.67) | 1.425 | ||
| Physically active (No = 0, Yes = 1) | 1.63 (1.05, 2.52) | 1.052 | ||
| History of bone fractures (No = 0, Yes = 1) | 2.20 (1.44, 3.37) | 1.036 | ||
| Medical treatment (No = 0, Yes = 1) | 3.33 (2.17, 5.05) | 1.065 | ||
| Pediatric admission (No = 0, Yes = 1) | 0.44 (0.26, 0.74) | 1.023 | ||
| Psychiatric admission (No = 0, Yes = 1) | 0.29 (0.12, 0.70) | 1.023 | ||
| Comorbidity with Axis I diagnose (No = 0, Yes = 1) | 3.70 (2.32, 5.54) | 1.070 | ||
| ADHD subtype: Hyperactive/Combined (n = 551) | Constant | 2.79 | ||
| History of bone fractures (No = 0, Yes = 1) | 1.66 (1.14, 2.54) | 1.020 | ||
| Psychiatric admission (No = 0, Yes = 1) | 6.43 (1.36, 28.31) | 1.007 | ||
| Sex (Male = 0, Female = 1) | 0.60 (0.41, 0.89) | 1.058 | ||
| Age (in years) | 0.86 (0.81, 0.91) | 2.896 * | ||
| ASD (n = 634) | Constant | 3.02 | ||
| Special educational needs (No = 0, Yes = 1) | 2.78 (1.25, 6.20) | 1.685 | ||
| History of bone fractures (No = 0, Yes = 1) | 0.47 (0.24, 0.93) | 1.013 | ||
| Disability (No = 0, Yes = 1) | 8.90 (3.91, 20.28) | 1.723 | ||
| Sex (Male = 0, Female = 1) | 0.21 (0.09, 0.48) | 1.026 | ||
| Diagnostic in Axis V (No = 0, Yes = 1) | 0.66 (0.50, 0.89) | 1.751 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blasco-Fontecilla, H.; Li, C.; Vizcaino, M.; Fernández-Fernández, R.; Royuela, A.; Bella-Fernández, M. A Nomogram for Predicting ADHD and ASD in Child and Adolescent Mental Health Services (CAMHS). J. Clin. Med. 2024, 13, 2397. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13082397
Blasco-Fontecilla H, Li C, Vizcaino M, Fernández-Fernández R, Royuela A, Bella-Fernández M. A Nomogram for Predicting ADHD and ASD in Child and Adolescent Mental Health Services (CAMHS). Journal of Clinical Medicine. 2024; 13(8):2397. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13082397
Chicago/Turabian StyleBlasco-Fontecilla, Hilario, Chao Li, Miguel Vizcaino, Roberto Fernández-Fernández, Ana Royuela, and Marcos Bella-Fernández. 2024. "A Nomogram for Predicting ADHD and ASD in Child and Adolescent Mental Health Services (CAMHS)" Journal of Clinical Medicine 13, no. 8: 2397. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13082397