
Robotic Vascular Resection in Pancreatic Ductal Adenocarcinoma: A Systematic Review

 , , , , , and
, , , , , and
Abstract
:1. Introduction
Historical Development
2. Material and Methods
2.1. Objectives and PICO Process
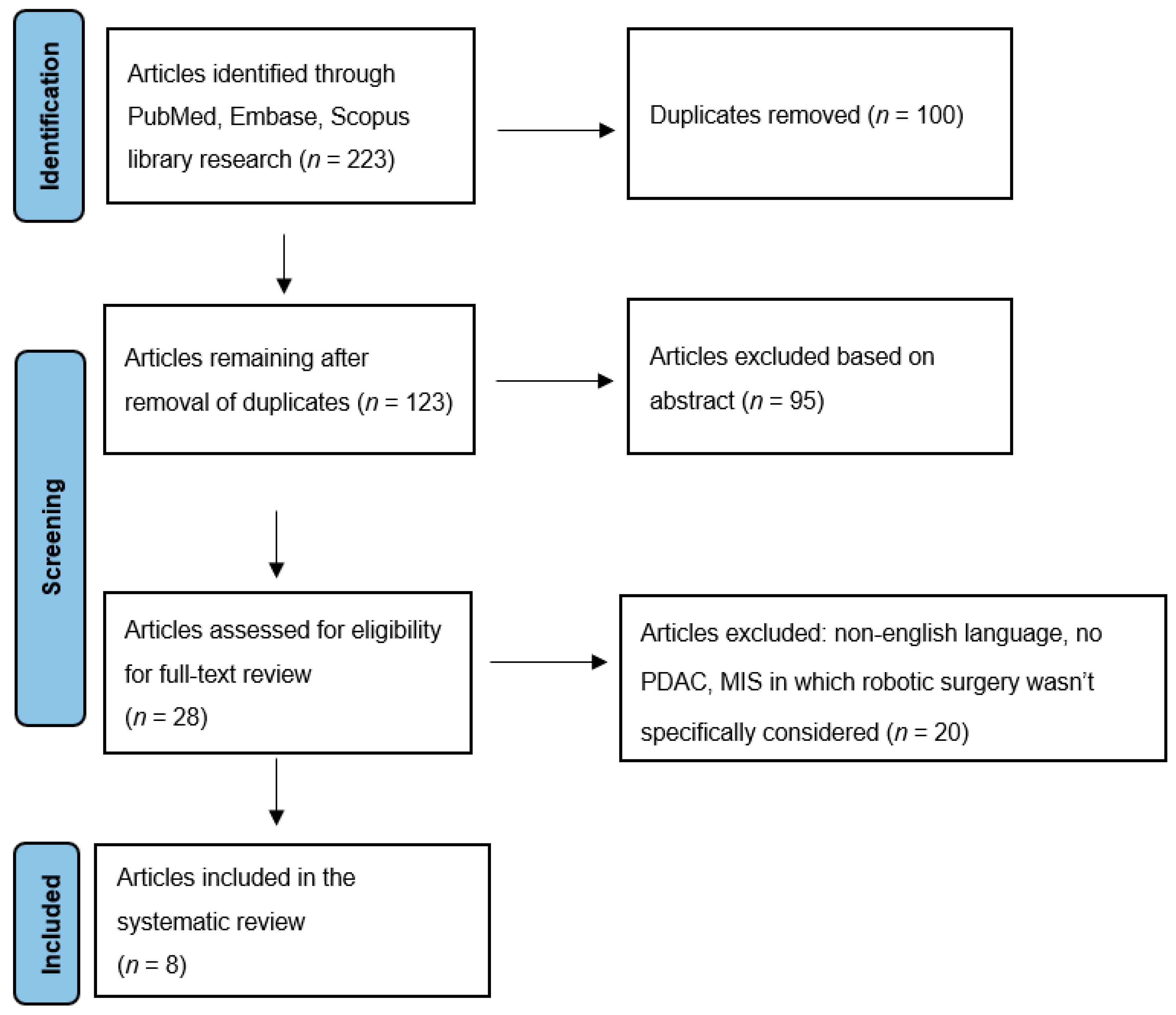
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction
3. Results
3.1. Blood Loss
3.2. Blood Transfusion
3.3. Duration of Surgery
3.4. Complication Rate
3.5. Conversion Rate
3.6. Hospitalization Time
3.7. Postoperative Mortality
3.8. Surgical Margins R0
3.9. Recurrence
3.10. Overall Survival and Disease-Free Survival
4. Discussion
- -
- the bowel cannot be fully mobilized and pushed towards the liver;
- -
- if the surgeon uses a jump graft, he or she must take into consideration that at the conclusion of the procedure the reverse Trendelenburg position will be abolished, which could create vascular kinking if the graft is too long;
- -
- vascular control can be problematic when the SMV is involved near the mesenteric root: it could be quite challenging to reposition the clamp on the SMV after the vein has been separated;
- -
- if the vein segment to be resected includes the splenomesenteric junction, managing the splenic vein presents additional challenges;
- -
- in the event of uncontrolled bleeding, an emergency conversion to open surgery is required.
- -
- In the case of marginal (<25%) circumferential involvement, a small side-wall resection followed by a primary direct venorraphy (Type 1) is performed.
- -
- If <50% of the vein circumference is involved, a larger side-wall resection followed by a patch venorraphy (Type 2) is carried out.
- -
- If a venous involvement > 50% is detected, and the length of the vascular defect is less than 3 cm, a segmental resection with direct repair is performed (Type 3).
- -
- If an encasement of >180° is detected, and the length of post- resection venous defect is more than 3 cm, an interposition graft is used for vascular repair (Type 4).
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
Abbreviations
| PDAC | Pancreatic ductal adenocarcinoma |
| RPS-VR | Robotic pancreatic surgery with vascular resection |
| RPD | Robotic pancreatoduodenectomy |
| LPD | Laparoscopic pancreatoduodenectomy |
| LDP | Laparoscopic distal pancreatectomy |
| OPD | Open pancreatoduodenectomy |
| VR | Vascular resection |
| DP | Distal pancreatectomy |
| RAPR | Robot-assisted pancreatic resection |
References
- Ruarus, A.; Vroomen, L.; Puijk, R.; Scheffer, H.; Meijerink, M. Locally Advanced Pancreatic Cancer: A Review of Local Ablative Therapies. Cancers 2018, 10, 16. [Google Scholar] [CrossRef]
- Ohgi, K.; Yamamoto, Y.; Sugiura, T.; Okamura, Y.; Ito, T.; Ashida, R.; Aramaki, T.; Uesaka, K. Is Pancreatic Head Cancer with Portal Venous Involvement Really Borderline Resectable? Appraisal of an Upfront Surgery Series. Ann. Surg. Oncol. 2017, 24, 2752–2761. [Google Scholar] [CrossRef]
- Raimondi, S.; Maisonneuve, P.; Lowenfels, A.B. Epidemiology of pancreatic cancer: An overview. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 699–708. [Google Scholar] [CrossRef]
- Ravikumar, R.; Sabin, C.; Hilal, M.A.; Bramhall, S.; White, S.; Wigmore, S.; Imber, C.J.; Fusai, G. Portal Vein Resection in Borderline Resectable Pancreatic Cancer: A United Kingdom Multicenter Study. J. Am. Coll. Surg. 2014, 218, 401–411. [Google Scholar] [CrossRef]
- Kaneoka, Y.; Yamaguchi, A.; Isogai, M. Portal or superior mesenteric vein resection for pancreatic head adenocarcinoma: Prognostic value of the length of venous resection. Surgery 2009, 145, 417–425. [Google Scholar] [CrossRef]
- Satoi, S. Surgical Treatment of Pancreatic Ductal Adenocarcinoma. Cancers 2021, 13, 4015. [Google Scholar] [CrossRef]
- Al-Haddad, M.; Martin, J.K.; Nguyen, J.; Pungpapong, S.; Raimondo, M.; Woodward, T.; Kim, G.; Noh, K.; Wallace, M.B. Vascular Resection and Reconstruction for Pancreatic Malignancy: A Single Center Survival Study. J. Gastrointest. Surg. 2007, 11, 1168–1174. [Google Scholar] [CrossRef]
- Siriwardana, H.P.P.; Siriwardena, A.K. Systematic review of outcome of synchronous portal–superior mesenteric vein resection during pancreatectomy for cancer. Br. J. Surg. 2006, 93, 662–673. [Google Scholar] [CrossRef]
- Allema, J.H.; Reinders, M.E.; Van Gulik, T.M.; Van Leeuwen, D.J.; De Wit, L.T.; Verbeek, P.C.M.; Gouma, D.J. Portal vein resection in patients undergoing pancreatoduodenectomy for carcinoma of the pancreatic head. Br. J. Surg. 2005, 81, 1642–1646. [Google Scholar] [CrossRef]
- Sindelar, W.F. Clinical Experience with Regional Pancreatectomy for Adenocarcinoma of the Pancreas. Arch. Surg. 1989, 124, 127. [Google Scholar] [CrossRef]
- Zureikat, A.H.; Postlewait, L.M.; Liu, Y.; Gillespie, T.W.; Weber, S.M.; Abbott, D.E.; Ahmad, S.A.; Maithel, S.K.; Hogg, M.E.; Zenati, M.; et al. A Multi-Institutional Comparison of Perioperative Outcomes of Robotic and Open Pancreaticoduodenectomy. Ann. Surg. 2016, 264, 640–649. [Google Scholar] [CrossRef]
- King, J.C.; Zeh, H.J.; Zureikat, A.H.; Celebrezze, J.; Holtzman, M.P.; Stang, M.L.; Tsung, A.; Bartlett, D.L.; Hogg, M.E. Safety in Numbers: Progressive Implementation of a Robotics Program in an Academic Surgical Oncology Practice. Surg. Innov. 2016, 23, 407–414. [Google Scholar] [CrossRef]
- Beane, J.D.; Zenati, M.; Hamad, A.; Hogg, M.E.; Zeh, H.J.; Zureikat, A.H. Robotic pancreatoduodenectomy with vascular resection: Outcomes and learning curve. Surgery 2019, 166, 8–14. [Google Scholar] [CrossRef]
- Wang, X.; Cai, Y.; Zhao, W.; Gao, P.; Li, Y.; Liu, X.; Peng, B. Laparoscopic pancreatoduodenectomy combined with portal-superior mesenteric vein resection and reconstruction with interposition graft: Case series. Medicine 2019, 98, e14204. [Google Scholar] [CrossRef]
- Dokmak, S.; Aussilhou, B.; Calmels, M.; Maghrebi, H.; Ftériche, F.S.; Soubrane, O.; Sauvanet, A. Laparoscopic pancreaticoduodenectomy with reconstruction of the mesentericoportal vein with the parietal peritoneum and the falciform ligament. Surg. Endosc. 2018, 32, 3256–3261. [Google Scholar] [CrossRef]
- Kauffmann, E.F.; Napoli, N.; Menonna, F.; Vistoli, F.; Amorese, G.; Campani, D.; Pollina, L.E.; Funel, N.; Cappelli, C.; Caramella, D.; et al. Robotic pancreatoduodenectomy with vascular resection. Langenbecks Arch. Surg. 2016, 401, 1111–1122. [Google Scholar] [CrossRef]
- Kang, C.M.; Lee, W.J. Is Laparoscopic Pancreaticoduodenectomy Feasible for Pancreatic Ductal Adenocarcinoma? Cancers 2020, 12, 3430. [Google Scholar] [CrossRef]
- Giulianotti, P.C.; Addeo, P.; Buchs, N.C.; Ayloo, S.M.; Bianco, F.M. Robotic Extended Pancreatectomy with Vascular Resection for Locally Advanced Pancreatic Tumors. Pancreas 2011, 40, 1264–1270. [Google Scholar] [CrossRef]
- Allan, B.J.; Novak, S.M.; Hogg, M.E.; Zeh, H.J. Robotic vascular resections during Whipple procedure. J. Vis. Surg. 2018, 4, 13. [Google Scholar] [CrossRef]
- Shyr, B.U.; Chen, S.C.; Shyr, Y.M.; Wang, S.E. Surgical, survival, and oncological outcomes after vascular resection in robotic and open pancreaticoduodenectomy. Surg. Endosc. 2020, 34, 377–383. [Google Scholar] [CrossRef]
- Whipple, A.O. Pancreaticoduodenectomy for Islet Carcinoma: A Five-Year Follow-Up. Ann Surg. 1945, 121, 847–852. [Google Scholar] [CrossRef]
- Salky, B.A.; Edye, M. Laparoscopic Pancreatectomy. Surg. Clin. N. Am. 1996, 76, 539–545. [Google Scholar] [CrossRef]
- Melvin, W.S.; Needleman, B.J.; Krause, K.R.; Ellison, E.C. Robotic Resection of Pancreatic Neuroendocrine Tumor. J. Laparoendosc. Adv. Surg. Tech. 2003, 13, 33–36. [Google Scholar] [CrossRef]
- Asbun, H.J.; Moekotte, A.L.; Vissers, F.L.; Kunzler, F.; Cipriani, F.; Alseidi, A.; D’angelica, M.I.; Balduzzi, A.; Bassi, C.; Björnsson, B.; et al. The Miami International Evidence-based Guidelines on Minimally Invasive Pancreas Resection. Ann. Surg. 2020, 271, 1–14. [Google Scholar] [CrossRef]
- Khachfe, H.H.; Habib, J.R.; Harthi, S.A.; Suhool, A.; Hallal, A.H.; Jamali, F.R. Robotic pancreas surgery: An overview of history and update on technique, outcomes, and financials. J. Robot. Surg. 2022, 16, 483–494. [Google Scholar] [CrossRef]
- Tempero, M.A.; Malafa, M.P.; Al-Hawary, M.; Asbun, H.; Bain, A.; Behrman, S.W.; Benson, A.B.; Binder, E.; Cardin, D.B.; Cha, C.; et al. Pancreatic Adenocarcinoma, Version 2.2017, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2017, 15, 1028–1061. [Google Scholar] [CrossRef]
- Isaji, S.; Mizuno, S.; Windsor, J.A.; Bassi, C.; Fernández-del Castillo, C.; Hackert, T.; Hayasaki, A.; Katz, M.H.; Kim, S.-W.; Kishiwada, M.; et al. International consensus on definition and criteria of borderline resectable pancreatic ductal adenocarcinoma 2017. Pancreatology 2018, 18, 2–11. [Google Scholar] [CrossRef]
- Zhu, J.; Li, X.; Kou, J.; Ma, J.; Li, L.; Fan, H.; Lang, R.; He, Q. Proposed Chaoyang vascular classification for superior mesenteric-portal vein invasion, resection, and reconstruction in patients with pancreatic head cancer during pancreaticoduodenectomy—A retrospective cohort study. Int. J. Surg. 2018, 53, 292–297. [Google Scholar] [CrossRef]
- Appleby, L.H. The coeliac axis in the expansion of the operation for gastric carcinoma. Cancer 1953, 6, 704–707. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Amir-Behghadami, M.; Janati, A. Population, Intervention, Comparison, Outcomes and Study (PICOS) design as a framework to formulate eligibility criteria in systematic reviews. Emerg. Med. J. 2020, 37, 387. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Jin, J.; Yin, S.-M.; Weng, Y.; Chen, M.; Shi, Y.; Ying, X.; Gemenetzis, G.; Qin, K.; Zhang, J.; Deng, X.; et al. Robotic versus open pancreaticoduodenectomy with vascular resection for pancreatic ductal adenocarcinoma: Surgical and oncological outcomes from pilot experience. Langenbecks Arch. Surg. 2022, 407, 1489–1497. [Google Scholar] [CrossRef]
- Marino, M.V.; Giovinazzo, F.; Podda, M.; Gomez Ruiz, M.; Gomez Fleitas, M.; Pisanu, A.; Latteri, M.A.; Takaori, K. Robotic-assisted pancreaticoduodenectomy with vascular resection. Description of the surgical technique and analysis of early outcomes. Surg. Oncol. 2020, 35, 344–350. [Google Scholar] [CrossRef]
- Kauffmann, E.F.; Napoli, N.; Menonna, F.; Genovese, V.; Cacace, C.; Andrea, C.I.; Daniela, C.; Vistoli, F.; Amorese, G.; Boggi, U. Robot-assisted pancreaticoduodenectomy with vascular resection: Technical details and results from a high-volume center. Laparosc. Surg. 2020, 4, 37. Available online: https://ls.amegroups.org/article/view/6081 (accessed on 1 January 2020). [CrossRef]
- Machado, M.A.C.; Mattos, B.H.; Lobo Filho, M.M.; Makdissi, F.F. Robotic Resection and Reconstruction of the Superior Mesenteric Vein without Graft During Pancreatoduodenectomy (with Video). J. Gastrointest. Surg. 2021, 25, 3010–3012. [Google Scholar] [CrossRef]
- Kauffmann, E.F.; Napoli, N.; Cacace, C.; Menonna, F.; Vistoli, F.; Amorese, G.; Boggi, U. Resection or repair of large peripancreatic arteries during robotic pancreatectomy. Updates Surg. 2020, 72, 145–153. [Google Scholar] [CrossRef]
- Chen, J.W.; Van Ramshorst, T.M.E.; Lof, S.; Al-Sarireh, B.; Bjornsson, B.; Boggi, U.; Burdio, F.; Butturini, G.; Casadei, R.; Coratti, A.; et al. Robot-Assisted Versus Laparoscopic Distal Pancreatectomy in Patients with Resectable Pancreatic Cancer: An International, Retrospective, Cohort Study. Ann. Surg. Oncol. 2023, 30, 3023–3032. [Google Scholar] [CrossRef]
- Boggi, U.; Del Chiaro, M.; Croce, C.; Vistoli, F.; Signori, S.; Moretto, C.; Amorese, G.; Mazzeo, S.; Cappelli, C.; Campani, D.; et al. Prognostic implications of tumor invasion or adhesion to peripancreatic vessels in resected pancreatic cancer. Surgery 2009, 146, 869–881. [Google Scholar] [CrossRef]
- Zhang, J.; Qian, H.-G.; Leng, J.-H.; Cui, M.; Qiu, H.; Zhou, G.-Q.; Wu, J.-H.; Yang, Y.; Hao, C.-Y. Long Mesentericoportal Vein Resection and End-to-End Anastomosis without Graft in Pancreaticoduodenectomy. J. Gastrointest. Surg. 2009, 13, 1524–1528. [Google Scholar] [CrossRef]
- Kauffmann, E.F.; Napoli, N.; Ginesini, M.; Gianfaldoni, C.; Asta, F.; Salamone, A.; Ripolli, A.; Di Dato, A.; Vistoli, F.; Amorese, G.; et al. Tips and tricks for robotic pancreatoduodenectomy with superior mesenteric/portal vein resection and reconstruction. Surg. Endosc. 2023, 37, 3233–3245. [Google Scholar] [CrossRef] [PubMed]
- Bockhorn, M.; Uzunoglu, F.G.; Adham, M.; Imrie, C.; Milicevic, M.; Sandberg, A.A.; Asbun, H.J.; Bassi, C.; Büchler, M.; Charnley, R.M.; et al. Borderline resectable pancreatic cancer: A consensus statement by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2014, 155, 977–988. [Google Scholar] [CrossRef] [PubMed]
- Stiles, Z.E.; Dickson, P.V.; Deneve, J.L.; Glazer, E.S.; Dong, L.; Wan, J.Y.; Behrman, S.W. The impact of unplanned conversion to an open procedure during minimally invasive pancreatectomy. J. Surg. Res. 2018, 227, 168–177. [Google Scholar] [CrossRef]
- Rosemurgy, A.; Ross, S.; Bourdeau, T.; Craigg, D.; Spence, J.; Alvior, J.; Sucandy, I. Robotic Pancreaticoduodenectomy Is the Future: Here and Now. J. Am. Coll. Surg. 2019, 228, 613–624. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Wang, W.; Qiu, W.; Zhao, S.; Wang, J.; Weng, Y.; Huo, Z.; Jin, J.; Wang, Y.; Deng, X.; et al. Learning Curve From 450 Cases of Robot-Assisted Pancreaticoduocectomy in a High-Volume Pancreatic Center: Optimization of Operative Procedure and a Retrospective Study. Ann. Surg. 2021, 274, e1277–e1283. [Google Scholar] [CrossRef]
- Zhang, T.; Zhao, Z.M.; Gao, Y.X.; Lau, W.Y.; Liu, R. The learning curve for a surgeon in robot-assisted laparoscopic pancreaticoduodenectomy: A retrospective study in a high-volume pancreatic center. Surg. Endosc. 2019, 33, 2927–2933. [Google Scholar] [CrossRef]


{kind=link}
| Author et al. | Year | Type of Study | Number of Patients |
|---|---|---|---|
| Beane J.D. et al. [13] | 2019 | Retroprospective review | ° 380 RPD-VR: 50, RPD: 330 |
| Jin J. et al. [33] | 2022 | Retroprospective review | ° 84 RPD-VR: 14, OPD-VR: 70 |
| Kauffman E. F. et al. [16] | 2016 | systematic review + literature review | ° 130 RPD-VR: 14, RPD: 116 |
| Kauffman E. F. et al. [37] | 2020 | Retroprospective review | ° 361 RAPR-VR: 31, RAPR:330 |
| Marino M. V. et al. [34] | 2020 | Retroprospective review | ° 83 RPD-VR: 10, RPD: 73 |
| Kauffman E. F. et al. [35] | 2020 | Retroprospective review | ° 184 RPD-VR: 22, RPD: 162 |
| Machado M. A. C. et al. [36] | 2021 | Case report | |
| Jeffrey W. C. et al. [38] | 2023 | Retroprospective review | ° 542 RPD: 103, LPD: 439 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zecchin Ferrara, V.; Martinino, A.; Toti, F.; Schilirò, D.; Pinto, F.; Giovinazzo, F.; on behalf of the SMAGEICS Group. Robotic Vascular Resection in Pancreatic Ductal Adenocarcinoma: A Systematic Review. J. Clin. Med. 2024, 13, 2000. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13072000
Zecchin Ferrara V, Martinino A, Toti F, Schilirò D, Pinto F, Giovinazzo F, on behalf of the SMAGEICS Group. Robotic Vascular Resection in Pancreatic Ductal Adenocarcinoma: A Systematic Review. Journal of Clinical Medicine. 2024; 13(7):2000. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13072000
Chicago/Turabian StyleZecchin Ferrara, Victoria, Alessandro Martinino, Francesco Toti, Davide Schilirò, Federico Pinto, Francesco Giovinazzo, and on behalf of the SMAGEICS Group. 2024. "Robotic Vascular Resection in Pancreatic Ductal Adenocarcinoma: A Systematic Review" Journal of Clinical Medicine 13, no. 7: 2000. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm13072000