
Are Babies Born Preterm High-Risk Asthma Candidates?

1
Clinica Pediatrica, Azienda Ospedaliero-Universitaria, Department of Medicine and Surgery, University of Parma, 43126 Parma, Italy
2
Pediatric Unit, San Giuseppe Hospital, 50053 Empoli, Italy
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2023, 12(16), 5400; https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12165400
Submission received: 5 July 2023
/
Revised: 12 August 2023
/
Accepted: 15 August 2023
/
Published: 19 August 2023
(This article belongs to the Special Issue Asthma and Allergic Inflammation: Risks, Mechanisms, and New Treatments: Part II)
Abstract
:Among preterm infants, the risk of developing asthma is a matter of debate. This review discusses the state of the art of poorly understood prematurity-associated asthma. Impaired pulmonary function is common in children born prematurely. Preterm infants are prone to developing viral respiratory tract infections, bronchiolitis in the first year of life, and recurrent viral wheezing in preschool age. All of these conditions may precede asthma development. We also discuss the role of both atopic sensitization and intestinal microbiome and, consequently, immune maturation. Diet and pollution have been considered to better understand how prematurity could be associated with asthma. Understanding the effect of factors involved in asthma onset may pave the way to improve the prediction of this asthma phenotype.
Keywords:
asthma; preterm; allergy; bronchiolitis; lung function; microbiome; atopy; breastfeeding; smoking1. Introduction
Asthma is a heterogeneous disease, usually characterized by chronic airway inflammation, defined according to the GINA recommendations by the history of respiratory symptoms, such as wheezing, shortness of breath, chest tightness, and cough, which vary over time and in intensity, together with variable expiratory airflow limitation [1]. Asthma is the most common chronic disease in childhood and one of the most frequent chronic diseases in all ages, as it is estimated that 358 million people are affected worldwide, with geographical differences gradually narrowing. The Global Asthma Network (GAN) Phase I study determined a prevalence of current wheeze of 11.1% among adolescents and 9.1% in children and asthma ever of 10.5% and 7.5%, respectively [2]. In children, the most common asthma phenotype is type-2 (T2)-high, characterized by eosinophilic airway inflammation. T2-high comprises the allergic phenotype, about 80% of cases, due to sensitization to allergens that elicit a Th2 response with an IgE production. The T2-high non-allergic phenotype is not IgE-mediated. T2-low is distinguished by a neutrophilic infiltrate that is rare in childhood and commonly begins in adulthood. Preterm infants are born before 37 weeks gestational age (wGA) is completed. They can be classified as extreme (<28 wGA), very (28–32 wGA), or moderate to late (32–36 wGA) preterm [3]. It has been estimated that global preterm delivery is growing especially in industrialized countries [4] from about 9.8% of births in 2000 to 14% in 2014, with 81% occurring in Asia and sub-Saharan Africa [5]. Preterm birth is the main cause of mortality under 5 years of age. Most fatalities occur in the neonatal period [6]. However, the advances in neonatal intensive care management have increased survival rates among premature newborns up to more than 95% [7,8], but they have increased morbidity [9]. Preterm birth can be associated with altered development of the lung and morbidity in the respiratory tract, including respiratory infections, wheeze, and asthma [10,11,12,13]. This is a narrative review performed with a literature search of the MEDLINE database using the following keywords: asthma, preterm delivery, prematurity, and gestational age. We aimed to characterize the occurrence of asthma in preterms and identify preterm infants who are at risk of asthma. We identified many factors associated with the development of asthma in preterms; some of them can be present both in preterm and in term children, sometimes more frequent among the former, while others are exclusive to prematurity. They are both environmental and individual factors that can intervene in various moments of the pre- and postnatal life of the preterm (Figure 1). The extent of the effect of these factors is different from each other; for some of them, it is minimal, while others significantly modify the risk of developing asthma (Table 1).
2. Frequency of Asthma in Preterm
The increased susceptibility to asthma in preterm infants has been shown by several studies. Jaakkola, in a systematic review that included 19 studies comparing preterm to term infants, found that preterm infants were 7% more likely to develop asthma according to a fixed-effects model, and the risk reached 36% in a random-effects model [14]. Most studies have focused on the development of asthma at different pediatric ages. In a retrospective cohort study of 7925 infants, late preterm compared to term infants had a 1.7-fold increased risk of persistent asthma at 18 months of age [15]. In the U.S., a large prospective birth cohort study found that preterm birth was associated with a higher prevalence of asthma at ages 0–5 and 6–9 years [16]. An Alaskan population-based study comparing preterm birth <32 wGA to full-term birth revealed that the former was twofold more likely to have asthma at both 0–5 years of age and 6–9 years [17]. These results were confirmed among late preterm infants in a prospective study showing that they were threefold more likely to develop asthma compared to term infants at 7–8 years of age [18] In a retrospective case–control study in 44,173 infants, very preterm infants (<32 wGA) were 3.9-fold more likely to have asthma, and moderate–late preterms (33–36 wGA) were 1.7-fold more likely compared to term infants (39–40 wGA) at 0–19 years of age [19]. A retrospective study on 90,721 children found that preterm infants were 1.64-fold more likely to have asthma compared with term infants at age 0–17 [20]. Furthermore, the increased risk of asthma also persists in adulthood. A Swedish national cohort study, which followed more than 4,000,000 subjects from birth to 46 years of age [21], showed an increased risk of asthma associated with preterm birth in children in each age group (<10, 10–17, 18–46 years).
3. Gestational Age
The immaturity represented by the gestational age is a key factor. The risk of asthma increases with decreasing gestational age, as shown by a large birth cohort study, in which children born <31 wGA were 3.2–6.2 times more likely to develop asthma and those born 32–36 wGA were 1.5–2.5 times more likely when compared to term infants [16]. These findings have been confirmed among adolescents (13–14 years of age), in which those born very preterm compared with those born moderate–late preterm required more respiratory admissions, were more likely to have current asthma (21.6% vs. 9.5%, p = 0.04), and had significantly reduced lung function compared with those born moderate–late preterm [22]. The relative risk of asthma medication prescriptions, indirectly reflecting the asthma severity, for infants with extreme prematurity was 1.92-fold that of infants with moderate–late preterm status [23]. Low birth weight (LBW) (<2500 g) is an additional risk factor for developing asthma [24,25], and the risk rises with weight reduction. Infants with extremely LBW (<1000 g) have a 1.8-fold increased risk of prescription of asthma medications. Very LBW (<1500 g) infants have a 1.43-fold higher risk than LBW infants [23]. Intrauterine growth restriction (IUGR), often associated with preterm birth, represents an additional independent risk factor for future asthma [26]. Most LBW babies also show catch-up growth in infancy, which was associated with lower lung function and an increased risk of childhood asthma [27,28]. A large meta-analysis showed that this increased risk is not explained by preterm birth alone, but high childhood weight gain (>700 g/month) is an independent risk factor for preschool wheezing and school-age asthma [29].
4. Airway Impairment and Asthma Development
Many studies have investigated the mechanisms that lead to the development of asthma in preterm children. Prematurity determines an alteration of the lung development, which consists of five phases: the embryonic period (up to week 6), the pseudoglandular period (weeks 6–16), the canalicular period (weeks 16–24), the saccular period (weeks 24–40), and the alveolarization period (mainly after birth) [30]. In preterm infants, the abnormal maturation of the lung at birth especially before the 32nd week [31] leads to lung function impairments. Mechanical ventilation was associated with bronchial hyperresponsiveness in very LBW infants (<1500 g) who had altered alveolar development and hypertrophy of the bronchial smooth muscle [32]. Preterm infants compared to those born at term had lower lung function in childhood, adolescence, and adulthood [32,33,34,35,36]. The Tasmanian Longitudinal Health Study showed that very-to-moderate prematurity was associated with obstructive lung function deficits including chronic obstructive pulmonary disease (COPD) into the sixth decade of life [37]. These alterations in lung function are independent of lung damage at birth and may represent the result of exposures to maternal smoking, oxygen by a ventilator, and treatment with microbiome-altering therapies [38]. In children born at term, an increased neonatal resistance compared to term controls was associated with wheezing until age 3 years of infancy, while reduced neonatal compliance was associated with wheezing and asthma up to 5 years of life [39]. Furthermore, a lung function deficit and increased bronchial responsiveness to methacholine in infants born at term were risk factors for asthma at 7 to 10 years of age [40,41]. Interestingly, low lung function parameters at the age of six months predicted wheezing and hospitalization for wheezing in schoolchildren born preterm [42]. Children born preterm have more respiratory symptoms, including cough and wheezing than controls before adolescence, irrespective of bronchopulmonary dysplasia (BPD), a chronic lung disease that mainly affects extremely preterm infants, which is the most common complication of prematurity, predisposing the infants to the development of obstructive pulmonary diseases [43,44,45,46,47,48,49,50]. Several studies showed an increased prevalence of asthma in children with a history of BPD [23,51,52], and reduced lung function was less evident in children without BPD than in BPD subjects [36]. However, it is controversial whether the asthma-like symptoms of children with BPD can be diagnosed as asthma or whether BPD and asthma should be considered different entities having different pathogenetic pathways [10,53,54]. In children born preterm, asthma should be differentiated from wheezing due to structural changes in lung parenchymal related to prematurity or poor intrauterine lung growth, leading to fixed airflow obstruction [54,55,56], especially when exhaled nitric oxide levels are low and eosinophilic inflammation is lacking [57,58,59,60]. Intrauterine inflammation to which premature infants are exposed [61] and postnatal factors such as hyperoxia and overdistension [62] can interfere with airway development, which will present a reduced caliber. Neonatal oxygen supplementation is a risk factor for asthma in very LBW infants (<1500 g) [32]. These factors might also trigger an inflammatory process that becomes persistent [56,63]. Along this line, children born <32 wGA, compared to full-term children, have increased lower airways neutrophilic inflammation [64], which is found more often in adult asthma and very rarely in childhood asthma and thus is usually eosinophilic, suggesting a different pathway leading to the development of asthma [65]. It is of note that inflammation linked to asthma in obesity needs to be investigated in premature children [66].
5. Environmental Agents Associated with the Development of Asthma in Preterm Infants
The increased susceptibility to asthma of preterm infants is determined by numerous factors, which could have important clinical consequences already from the fetal stage and in the first periods of life.
5.1. Allergic Sensitization
Allergic sensitization to aeroallergens may occur less frequently in preterm infants. Siltanen et al. [67] showed that in children born preterm at very LBW, the skin prick test overall and to mugwort and cat but not birch, timothy, dog, and house dust mite and IgE overall and to cat but not birch and timothy were significantly less positive than in full-term infants at 18 to 27 years of age. Asthma and low gestational age, but not atopy, were significantly associated with lower lung function values. Furthermore, it has been shown that the positive skin prick test to inhalants was associated with persisting wheezing but not with lower lung function in children preterm born at 10 years of age [68]. Mitselou et al. [69] studied the frequency of IgE to inhalants in two population-based birth cohorts, BAMSE and STOPPA. He showed that subjects preterm-born compared to those full-term-born had a significantly lower frequency of IgE to inhalants at 16 years of age but not at 4, 8, and 24 years or overall in the BAMSE study and no difference at 9–14 years in the STOPPA cohort. A combined meta-analysis of the results of BAMSE and STOPPA cohorts found that preterm birth was inversely associated with inhalant sensitization. Varying from previous studies, Mai et al. [32] found that very LBW had no impact on sensitization defined as positive skin prick test results in 12-year-old children. Several explanations for reduced sensitization in preterm children may be offered. Early microbial exposure can drive a Th1 immune response instead of a Th2 response. Another possibility might be that a low number of allergens have been investigated [70]. Finally, an immature immune system might not be able to develop a Th2 response. Accordingly, a longer gestation might induce a Th2 over Th1 response with allergic sensitization [71].
5.2. Infections
5.2.1. Viral Respiratory Infections
Children born preterm have an increased rate of airway infections from infancy up to school age, but this susceptibility did not continue in adolescents [72,73]. Infants admitted to the hospital for respiratory infections in the first year of life were at increased risk of asthma. Stratification of the risk of asthma for gestational age showed a significantly higher asthma risk in preterm subjects, especially in those born <28 wGA. This risk persisted until after age 10 but was less pronounced after age 16 [74].
5.2.2. Bronchiolitis and Asthma Development
Bronchiolitis among infants is associated with an increased risk of asthma. Bronchiolitis can be induced by several viruses. Specific organisms are considered important for the development of asthma. The most common infective pathogen is RSV in infants <2 years of age. There is evidence that bronchiolitis caused by RSV is not associated with asthma development both in term and preterm infants. Even if RSV bronchiolitis may lead to a 3.8-fold increased risk of recurrent wheeze and asthma, this association weakened over time, and it was no longer significant by the age of 13 years [75,76,77,78]. Most studies have shown that RSV bronchiolitis was not associated with atopy [75,79,80]. Preterm infants showed comparable figures [81,82]. The causal relationship between severe RSV infection and asthma in preterm infants was analyzed through prospective studies on palivizumab, an anti-RSV monoclonal antibody for preventing RSV infections in infants at risk [83]. Infants aged 1–3 years who received palivizumab experienced a reduction in wheezing days, reported recurrent wheeze, and the use of bronchodilators [84,85,86,87,88], but there was no major effect on lung function or the prevalence of physician-diagnosed asthma at 6 years of age [89,90,91]. Human Rhino Virus (RV) is another pathogen that is often associated with bronchiolitis. Those with bronchiolitis due to RV was four-fold more likely to develop recurrent wheeze than those with RSV bronchiolitis [92]. Moreover, in young children, low respiratory tract infections associated with RV compared to those associated with RSV were associated with more general practitioner attendances, more respiratory-related outpatient attendance, and more wheeze at follow-up [93]. In infants with viral wheezing, RV infections compared to RSV infections are the most significant predictors of asthma at the age of 6 years [94]. At 11 months of age, the risk factors for current atopic asthma at the age of 8 years were allergic sensitization, atopic eczema, and RV wheezing [95]. Atopy was a risk factor not only for asthma in RV bronchiolitis [96,97]. Premature birth is a risk factor not only for RSV disease but also for severe RV disease [98,99]. There are some data showing that in very preterm infants, bronchiolitis is more commonly caused by RV than by RSV [100]. However, studies on the development of asthma following early RV infection in children born preterm are missing. In preterm infants, infections favored a lower production of IFN-α and IFN-γ with a consequent impaired viral clearance [101], a T2 response with increased levels of IL-4 and IL-13 [101,102], eosinophil activation and chemotaxis, and higher levels of IL-17A [103].
5.2.3. Chorioamnionitis
Chorioamnionitis is another independent risk factor for recurrent wheeze and asthma in preterm infants [104,105,106] with the highest risk in the very preterm ones and in African Americans [104,105]. Chorioamnionitis was not associated with pulmonary function impairment [107]. Moreover, in term infants, chorioamnionitis had no effect on the rate of wheeze at 3.5 years and 7 years [108], suggesting that the preterm lung is more susceptible to disruption by inflammation.
6. Breastfeeding
In preterm infants, reduced breastfeeding has been observed [109]. Various studies have found that breastfeeding is a protective factor against the development of recurrent wheeze and asthma. Exclusive breastfeeding during the first 3 months of life was associated with 30% reduced odds of childhood asthma [110]. Breastfeeding for at least 6 months was associated with a 24% reduction in the rate of “recent asthma”, with a 19% reduction in “recent wheeze”, and there was a strong inverse association between breastfeeding and asthma or wheeze up to age 2 [111]. Ever breastfeeding was associated with a 12% reduced risk of asthma in children aged 5–18 [112]. Human milk is a complex mixture with bioactive compounds that include cytokines, immune cells, proteins, oligosaccharides, microbiota, bacterial metabolites (short-chain fatty acids), and mRNA modifications that may prevent prematurity-associated asthma. More studies are needed to elucidate immunological and epigenetic mechanisms involved in asthma prevention [113].
7. Microbioma
Consistent with the hygiene hypothesis, missing microbial exposure in early life leads to immune system development with the onset of allergic diseases [114,115]. Accordingly, a reduced risk of asthma has been shown when there is a highly differentiated gut microbiota in early life [116]. Atopy and the development of asthma at 3 months of life are reduced by a high frequency of Candida and Rhodotorula in the composition of the microbiota profile through a dysfunction in the CD4 T-cell; in contrast, it is promoted by an abundance of Bifodobacteria, Akkermansia, and Faecalibacterium [117]. Furthermore, in the infant gut, the abundance of strains with anti-inflammatory properties (such as Bacteroides, Roseburia, and Coprococcus) may protect from asthma onset [118]. In preterm infants, microbiota colonization in the airways is enriched for RSV/HRV-A, Haemophilus influenzae, Streptococcus pneumoniae, and Moraxella catarrhalis, which are associated with persistent wheeze and asthma [119] at 5 years [120] as well as with the later development of pneumonia or bronchiolitis [121]. In preterm infants, increased asthma development has been linked to a reduced abundance of Bacteroides, Bifidobacterium, Lachnospira, Veillonella, Faecalibacterium, and Akkermansia and a greater abundance of Clostridium difficile, Clostridium neonatale, Staphylococcus, Proteobacteria, and Enterobacteriaceae (Klebsiella, Enterococcus, and Escherichia) in the gut and even in the airway microbiome [122]. This complex led to enhanced eosinophilic and neutrophilic recruitment in the lung, increased IgE levels, bronchial hyper-responsiveness, and decreased IL-10 production and Treg function, which may contribute to asthma occurrence [122,123]. Interestingly, a lower abundance of Proteobacteria, Enterococcus, Lactobacillus, and Acinetobacter and the dominance of Bacteroides and Bifidobacterium in the intestinal microbiota during the first month of life was associated with the development of allergic sensitization [122]. Several factors such as cesarean delivery and the use of antibiotics can explain the different composition and poor diversity of the microbiome in preterm infants compared to term infants. Nutrition can also play a role. Breastfeeding is associated with a dominance of Bifidobacteria in the gut, which is a marker of healthy microbiota development. Gut dysbiosis may negatively affect the immune response [124], predisposing infants to increased susceptibility to infections and asthma development [125,126].
7.1. Delivery
The mode of delivery represents a risk factor for asthma. An increased risk of childhood asthma in children born through cesarean section has been found in several systematic reviews [127,128]. An increased asthma hospitalization risk only among cesarian-delivered preterms has also been shown [129]. There are differences between delivery modes at birth that progressively diminish over the first year of age. Mother-to-infant transmission was compromised in vaginally delivered infants who shared only 72% of gut microbes with their mother, while cesarean-delivered infants shared 41%, with less sharing of Bifidobacterium and Bacteroides (specifically Prevotella), while that of Enterobacteriaceae was maintained [130]. In cesarean-delivered infants, the gut microbiota consists of germs of the maternal skin, mouth, and surrounding environment. There was an abundance of Propionibacterium, Corynebacterium, Haemophilus parainfluenzae/influenzae, and Staphylococcus spp. and also of Clostridium perfringens, Veillonella dispar/V. parvula, and Enterobacteriaceae (Enterobacter cloacae and oxytoca, Klebsiella species, Enterococcus), which significantly differed from the gut microbiota of vaginally delivered infants. They displayed maternal vaginal and gut microbes enriched in Bifidobacterium, Bacteroides (Prevotella), Parabacteroides, Enterobacteriaceae (Escherichia), Sneathia, and Lactobacillus spp. [130].
7.2. Antibiotics
Preterm infants are more frequently exposed to antibiotic therapy [131]. A recent meta-analysis demonstrates that antibiotic treatment during pregnancy is associated with an increased risk of asthma during childhood [132]. A revision of 52 articles [133] showed that exposure to antibiotics was significantly associated with increased odds of childhood asthma in infants. The risk of asthma is increased after postnatal antibiotics but not after prenatal use [134,135,136]. Patrick et al. [137] found that antibiotic use in the first year of life was associated with a two-fold increased risk of asthma at age 5 years. The reduction in the incidence of asthma from 2000 to 2014 was associated with decreasing antibiotic use in infancy. Morata et al. [18] found that antibiotic use in the first 3 years of life was a risk factor for asthma at school age in children born preterm. Antibiotics may act by disrupting gut microbiota, which can predispose children to asthma development by altering the immune response. Maternal antibiotic exposure before or during labor is associated with reduced Bacteroides and Parabacteroides and increased Clostridium and Enterococcus at 3 months of age [138]. Along this line, both asthma and antibiotic exposure are associated with a loss of microbial diversity, a reduction in Bacteroidetes (Rikenellacea), Faecalibacterium, Roseburia, and Ruminococcus bromii, and an increase in Clostridium perfringens [137,139]. The increased risk of asthma does not seem to depend on respiratory infections that require the use of antibiotics; in fact, the results were confirmed even by excluding patients who presented respiratory infections [136].
8. Tobacco Smoke
Prenatal exposure to tobacco smoke increased preterm delivery and the risk of asthma later in life independently from postnatal exposure [29,140,141,142,143,144]. It is unclear whether maternal exposure to secondhand smoke during pregnancy can affect the prevalence of preterm birth [145,146]. The increased risk for asthma is caused by both maternal smoking [147] and exposure to environmental tobacco smoke during pregnancy [148,149]. Nicotine crosses the placental barrier and accumulates in the fetus with serum concentrations higher by 15% than maternal ones [150]. Nicotine induces placental vasoconstriction, which leads to reduced oxygen and nutrient contribution. This impacts alveolar development, breathing actions, the growth and maturation of airways and lungs, and the subsequent development of respiratory diseases [151,152]. Maternal smoking impaired lung development with increasing risk of BPD in preterm [153,154,155]. Regarding mechanisms of asthma onset, nicotine impaired cellular differentiation and airway development, which leads to reduced respiratory function in infants born preterm of smoking mothers compared to those of nonsmokers [156]. Macaubas et al. [157] showed that maternal smoking was associated with an increased risk of asthma and atopy at 6 years of age and with a Th2/Th1 unbalance due to lower levels of serum interleukin 4 and interferon-gamma in cord blood. Furthermore, in mice, maternal smoking during pregnancy induces airway remodeling with hyperplasia of the airway smooth muscle, collagen III deposition, mites-induced mast cell numbers and methacholine responsiveness in house-dust-mite-exposed offspring [158], and significantly exacerbated HDM-induced airway eosinophilic inflammation with increased reactivity, mucus secretion, and T2 cytokine levels in the offspring [159]. Exposure to maternal smoke increases the risk of lower respiratory tract infections in infants, which may trigger asthma. Several studies have shown a transgenerational inheritance of smoking effects [160]. Finally, epigenetic regulations due to the environment pass to the offspring. Prenatal maternal smoking and rising asthma symptoms such as wheezing at age 10 were associated with AXL methylation at birth, measured in bloodspots, in two population study cohorts [161]. Exposure to prenatal maternal tobacco smoke was associated with higher methylation levels in the AHHR gene measured in whole blood and asthma in 8- to 21-year-old Latino children [162]. Smoking cessation before or in the first trimester of pregnancy was associated with a reduction in preterm delivery [163,164,165,166,167,168,169]. This should push more efforts for the timely cessation of smoking in women.
9. Family History
Children with parental asthma have an increased risk of asthma than children without parental asthma, which is 3-fold greater for maternal asthma and 2.4-fold greater for paternal asthma [170]. Familiarity with asthma represents a risk factor for the development of asthma even in preterm infants, as demonstrated by a long-term observational study evaluating preterm infants <32 weeks or weighing <1500 g [171]. Genetic factors certainly favor the development of asthma in children of asthmatic parents, but there is also some evidence that women with asthma have an increased risk of preterm labor [172].
10. Prevention Strategies
Preventive strategies to reduce the risk of asthma are numerous and still being studied. Among interventions for preventing asthma in children born preterm, the administration of daily probiotics seems to have no effect on asthma diagnosis [173]. Other strategies have been studied in full-term babies with mixed results [174,175]. The transplacental passage of vitamin D occurs above all in the third trimester, so preterm infants are often deficient [176], but its supplementation during pregnancy in case of parental atopy had no effect on the development of asthma in the offspring [177]. A systematic review and meta-analysis suggests that bacterial lysates decrease the risk of wheezing episodes and asthma exacerbations [178]. However, further studies in preterm infants that can clarify the actual usefulness of preventive strategies are needed.
11. Conclusions
Many factors contribute to the increased risk of asthma in preterm infants. Intrinsic factors such as structural abnormalities (smaller airways), immune response to viral pathogens or aeroallergens, inflammation, and microbiome diversity play a pathogenetic role. Several risk factors including delivery, pollution exposure, feeding, and drugs influence the development of asthma. These findings may indicate that asthma in preterm babies may be associated with a unique pathway that may be different from those in full-term infants. However, it remains difficult to distinguish the true relationship between causes and effects. This hampers the implementation of practical strategies for mitigating the onset of asthma. Further studies in preterm infants for clarifying asthma endotypes and subgroups at risk of asthma and developing successful prevention strategies are warranted.
Author Contributions
Conceptualization, C.C. and R.B.; data curation and writing, C.C., R.B., S.G., and G.G.; writing—review and editing, C.C. and R.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Acknowledgments
We thank Giulia Carbone, Mandy Ferrocino, and Antonella Rossana Migliarino for technical support in preparing the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2023. Available online: www.ginasthma.org (accessed on 1 July 2023).
- García-Marcos, L.; Asher, M.I.; Pearce, N.; Ellwood, E.; Bissell, K.; Chiang, C.Y.; El Sony, A.; Ellwood, P.; Marks, G.B.; Mortimer, K.; et al. Global Asthma Network Phase I Study Group. The burden of asthma, hay fever and eczema in children in 25 countries: GAN Phase I study. Eur. Respir. J. 2022, 60, 2102866. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Preterm Birth. Available online: https://www.who.int/news-room/fact-sheets/detail/preterm-birth (accessed on 23 June 2023).
- Cao, G.; Liu, J.; Liu, M. Global, regional, and national incidence and mortality of neonatal preterm birth, 1990-2019. JAMA Pediatr. 2022, 176, 787–796. [Google Scholar] [CrossRef] [PubMed]
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef] [PubMed]
- Walani, S.R. Global burden of preterm birth. Int. J. Gynaecol. Obstet. 2020, 150, 31–33. [Google Scholar] [CrossRef]
- Crump, C.; Sundquist, J.; Winkleby, M.A.; Sundquist, K. Gestational age at birth and mortality from infancy into mid-adulthood: A national cohort study. Lancet Child Adolesc. Health 2019, 3, 408–417. [Google Scholar] [CrossRef]
- Crump, C.; Winkleby, M.A.; Sundquist, J.; Sundquist, K. Prevalence of survival without major comorbidities among adults born prematurely. JAMA 2019, 322, 1580–1588. [Google Scholar] [CrossRef] [PubMed]
- Gong, A.; Johnson, Y.R.; Livingston, J.; Matula, K.; Duncan, A.F. Newborn intensive care survivors: A review and a plan for collaboration in Texas. Matern. Health Neonatol. Perinatol. 2015, 1, 24. [Google Scholar] [CrossRef]
- Priante, E.; Moschino, L.; Mardegan, V.; Manzoni, P.; Salvadori, S.; Baraldi, E. Respiratory outcome after preterm birth: A long and difficult journey. Am. J. Perinatol. 2016, 33, 1040–1042. [Google Scholar] [CrossRef]
- Pramana, I.A.; Latzin, P.; Schlapbach, L.J.; Hafen, G.; Kuehni, C.E.; Nelle, M.; Riedel, T.; Frey, U. Respiratory symptoms in preterm infants: Burden of disease in the first year of life. Eur. J. Med. Res. 2011, 16, 223–230. [Google Scholar] [CrossRef]
- Castro-Rodriguez, J.A.; Forno, E.; Rodriguez-Martinez, C.E.; Celedón, J.C. Risk and protective factors for childhood asthma: What is the evidence? J. Allergy Clin. Immunol. Pract. 2016, 4, 1111–1122. [Google Scholar] [CrossRef]
- Anderson, J.; Do, L.A.H.; Wurzel, D.; Licciardi, P.V. Understanding the increased susceptibility to asthma development in preterm infants. Allergy 2023, 78, 928–939. [Google Scholar] [CrossRef] [PubMed]
- Jaakkola, J.J.; Ahmed, P.; Ieromnimon, A.; Goepfert, P.; Laiou, E.; Quansah, R.; Jaakkola, M.S. Preterm delivery and asthma: A systematic review and meta-analysis. J. Allergy Clin. Immunol. 2006, 118, 823–830. [Google Scholar] [CrossRef] [PubMed]
- Goyal, N.K.; Fiks, A.G.; Lorch, S.A. Association of late-preterm birth with asthma in young children: Practice-based study. Pediatrics 2011, 128, e830–e838. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Butz, A.; Keet, C.A.; Minkovitz, C.S.; Hong, X.; Caruso, D.M.; Pearson, C.; Cohen, R.T.; Wills-Karp, M.; Zuckerman, B.S.; et al. Preterm birth with childhood asthma: The role of degree of prematurity and asthma definitions. Am. J. Respir. Crit. Care Med. 2015, 192, 520–523. [Google Scholar] [CrossRef] [PubMed]
- Gessner, B.D.; Chimonas, M.A. Asthma is associated with preterm birth but not with small for gestational age status among a population-based cohort of Medicaid-enrolled children < 10 years of age. Thorax 2007, 62, 231–236. [Google Scholar] [CrossRef]
- Morata-Alba, J.; Romero-Rubio, M.T.; Castillo-Corullón, S.; Escribano-Montaner, A. Respiratory morbidity, atopy and asthma at school age in preterm infants aged 32-35 weeks. Eur. J. Pediatr. 2019, 178, 973–982. [Google Scholar] [CrossRef] [PubMed]
- Harju, M.; Keski-Nisula, L.; Georgiadis, L.; Räisänen, S.; Gissler, M.; Heinonen, S. The burden of childhood asthma and late preterm and early term births. J. Pediatr. 2014, 164, 295–299.e1. [Google Scholar] [CrossRef]
- Zhang, J.; Ma, C.; Yang, A.; Zhang, R.; Gong, J.; Mo, F. Is preterm birth associated with asthma among children from birth to 17 years old? -A study based on 2011-2012 US National Survey of Children’s Health. Ital. J. Pediatr. 2018, 44, 151. [Google Scholar] [CrossRef]
- Crump, C.; Sundquist, J.; Sundquist, K. Preterm or early term birth and long-term risk of asthma into midadulthood: A national cohort and cosibling study. Thorax 2023, 78, 653–660. [Google Scholar] [CrossRef]
- Arroyas, M.; Calvo, C.; Rueda, S.; Esquivias, M.; Gonzalez-Menchen, C.; Gonzalez-Carrasco, E.; Garcia-Garcia, M.L. Asthma prevalence, lung and cardiovascular function in adolescents born preterm. Sci. Rep. 2020, 10, 19616. [Google Scholar] [CrossRef]
- Kim, K.; Lee, J.Y.; Kim, Y.M.; Kim, K.; Kim, E.H.; Lee, B.K.; So, H.; Kwon, Y.; Shin, J.; Kim, M. Prevalence of asthma in preterm and associated risk factors based on prescription data from the Korean National Health Insurance database. Sci. Rep. 2023, 13, 4484. [Google Scholar] [CrossRef] [PubMed]
- Matheson, M.C.; D’Olhaberriague, A.L.; Burgess, J.A.; Giles, G.G.; Hopper, J.L.; Johns, D.P.; Abramson, M.J.; Walters, E.H.; Dharmage, S.C. Preterm birth and low birth weight continue to increase the risk of asthma from age 7 to 43. J. Asthma. 2017, 54, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Mu, M.; Ye, S.; Bai, M.J.; Liu, G.L.; Tong, Y.; Wang, S.F.; Sheng, J. Birth weight and subsequent risk of asthma: A systematic review and meta-analysis. Heart Lung Circ. 2014, 23, 511–519. [Google Scholar] [CrossRef]
- Källén, B.; Finnström, O.; Nygren, K.G.; Otterblad Olausson, P. Association between preterm birth and intrauterine growth retardation and child asthma. Eur. Respir. J. 2013, 41, 671–676. [Google Scholar] [CrossRef] [PubMed]
- Pike, K.C.; Crozier, S.R.; Lucas, J.S.; Inskip, H.M.; Robinson, S.; Southampton Women’s Survey Study Group; Roberts, G.; Godfrey, K.M. Patterns of fetal and infant growth are related to atopy and wheezing disorders at age 3 years. Thorax 2010, 65, 1099–1106. [Google Scholar] [CrossRef] [PubMed]
- Sonnenschein-van der Voort, A.M.; Jaddoe, V.W.; Raat, H.; Moll, H.A.; Hofman, A.; de Jongste, J.C.; Duijts, L. Fetal and infant growth and asthma symptoms in preschool children: The Generation R Study. Am. J. Respir. Crit. Care Med. 2012, 185, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Sonnenschein-van der Voort, A.M.; Arends, L.R.; de Jongste, J.C.; Annesi-Maesano, I.; Arshad, S.H.; Barros, H.; Basterrechea, M.; Bisgaard, H.; Chatzi, L.; Corpeleijn, E.; et al. Preterm birth, infant weight gain, and childhood asthma risk: A meta-analysis of 147,000 European children. J. Allergy Clin. Immunol. 2014, 133, 1317–1329. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.J.; McKay, K.O.; van Asperen, P.P.; Selvadurai, H.; Fitzgerald, D.A. Normal development of the lung and premature birth. Paediatr. Respir. Rev. 2010, 11, 135–142. [Google Scholar] [CrossRef]
- Gappa, M.; Stocks, J.; Merkus, P. Lung growth and development after preterm birth: Further evidence. Am. J. Respir. Crit. Care Med. 2003, 168, 399–400. [Google Scholar] [CrossRef]
- Mai, X.M.; Gäddlin, P.O.; Nilsson, L.; Finnström, O.; Björkstén, B.; Jenmalm, M.C.; Leijon, I. Asthma, lung function and allergy in 12-year-old children with very low birth weight: A prospective study. Pediatr. Allergy Immunol. 2003, 14, 184–192. [Google Scholar] [CrossRef]
- Doyle, L.W.; Cheung, M.M.; Ford, G.W.; Olinsky, A.; Davis, M.N.; Callanan, C. BirthWeight <1501 G and respiratory health at age 14. Arch. Dis. Child 2001, 84, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Fawke, J.; Lum, S.; Kirkby, J.; Hennessy, E.; Marlow, N.; Rowell, V.; Thomas, S.; Stocks, J. Lung function and respiratory symptoms at 11 years in children born extremely preterm: The EPICure study. Am. J. Respir. Crit. Care Med. 2010, 182, 237–245. [Google Scholar] [CrossRef] [PubMed]
- den Dekker, H.T.; Sonnenschein-van der Voort, A.M.; de Jongste, J.C.; Anessi-Maesano, I.; Arshad, S.H.; Barros, H.; Beardsmore, C.S.; Bisgaard, H.; Phar, S.C.; Craig, L.; et al. Early growth characteristics and the risk of reduced lung function and asthma: A meta-analysis of 25,000 children. J. Allergy Clin. Immunol. 2016, 137, 1026–1035. [Google Scholar] [CrossRef] [PubMed]
- Kotecha, S.J.; Edwards, M.O.; Watkins, W.J.; Henderson, A.J.; Paranjothy, S.; Dunstan, F.D.; Kotecha, S. Effect of preterm birth on later FEV1: A systematic review and meta-analysis. Thorax 2013, 68, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Bui, D.S.; Perret, J.L.; Walters, E.H.; Abramson, M.J.; Lowe, A.J.; Dharmage, S.C. Association between very to moderate preterm births, lung function deficits, and COPD at age 53 years: Analysis of a prospective cohort study. Lancet Respir. Med. 2022, 10, 478–484. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, C.; Venigalla, S.; Schilling, D.; Clay, N.; Spitale, P.; Nguyen, T. Respiratory function in healthy late preterm infants delivered at 33-36 weeks of gestation. J. Pediatr. 2013, 162, 464–469. [Google Scholar] [CrossRef] [PubMed]
- van der Gugten, A.C.; Uiterwaal, C.S.; van Putte-Katier, N.; Koopman, M.; Verheij, T.J.; van der Ent, C.K. Reduced neonatal lung function and wheezing illnesses during the first 5 years of life. Eur. Respir. J. 2013, 42, 107–115. [Google Scholar] [CrossRef]
- Bisgaard, H.; Jensen, S.M.; Bønnelykke, K. Interaction between asthma and lung function growth in early life. Am. J. Respir. Crit. Care Med. 2012, 185, 1183–1189. [Google Scholar] [CrossRef] [PubMed]
- Håland, G.; Carlsen, K.C.; Sandvik, L.; Devulapalli, C.S.; Munthe-Kaas, M.C.; Pettersen, M.; Carlsen, K.H. ORAACLE. Reduced lung function at birth and the risk of asthma at 10 years of age. N. Engl. J. Med. 2006, 355, 1682–1689. [Google Scholar] [CrossRef]
- Sanchez-Solis, M.; Parra-Carrillo, M.S.; Mondejar-Lopez, P.; Garcia-Marcos, P.W.; Garcia-Marcos, L. Preschool asthma symptoms in children born preterm: The relevance of lung function in infancy. J. Clin. Med. 2020, 9, 3345. [Google Scholar] [CrossRef]
- Narang, I.; Baraldi, E.; Silverman, M.; Bush, A. Airway function measurements and the long-term follow-up of survivors of preterm birth with and without chronic lung disease. Pediatr. Pulmonol. 2006, 41, 497–508. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, A.; McGrath-Morrow, S. Long-term pulmonary outcomes of patients with bronchopulmonary dysplasia. Semin. Perinatol. 2013, 37, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Di Filippo, P.; Giannini, C.; Attanasi, M.; Dodi, G.; Scaparrotta, A.; Petrosino, M.I.; Di Pillo, S.; Chiarelli, F. Pulmonary Outcomes in Children Born Extremely and Very Preterm at 11 Years of Age. Front. Pediatr. 2021, 9, 635503. [Google Scholar] [CrossRef]
- Robin, B.; Kim, Y.J.; Huth, J.; Klocksieben, J.; Torres, M.; Tepper, R.S.; Castile, R.G.; Solway, J.; Hershenson, M.B.; Goldstein-Filbrun, A. Pulmonary function in bronchopulmonary dysplasia. Pediatr. Pulmonol. 2004, 37, 236–242. [Google Scholar] [CrossRef]
- Rona, R.J.; Gulliford, M.C.; Chinn, S. Effects of prematurity and intrauterine growth on respiratory health and lung function in childhood. BMJ 1993, 306, 817–820. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.J.; van Asperen, P.P.; McKay, K.O.; Selvadurai, H.; Fitzgerald, D.A. Reduced exercise capacity in children born very preterm. Pediatrics 2008, 122, e287–e293. [Google Scholar] [CrossRef] [PubMed]
- Verheggen, M.; Wilson, A.C.; Pillow, J.J.; Stick, S.M.; Hall, G.L. Respiratory function and symptoms in young preterm children in the contemporary era. Pediatr. Pulmonol. 2016, 51, 1347–1355. [Google Scholar] [CrossRef] [PubMed]
- Welsh, L.; Kirkby, J.; Lum, S.; Odendaal, D.; Marlow, N.; Derrick, G.; Stocks, J. The EPICure study: Maximal exercise and physicalactivity in school children born extremely preterm. Thorax 2010, 65, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves Eda, S.; Mezzacappa-Filho, F.; Severino, S.D.; Ribeiro, M.Â.; Marson, F.A.; Morcilo, A.M.; Toro, A.A.; Ribeiro, J.D. Association between clinical variables related to asthma in schoolchildren born with very low birth weight with and without bronchopulmonary dysplasia. Rev. Paul. Pediatr. 2016, 34, 271–280. [Google Scholar] [CrossRef]
- Sun, T.; Yu, H.Y.; Yang, M.; Song, Y.F.; Fu, J.H. Risk of asthma in preterm infants with bronchopulmonary dysplasia: A systematic review and meta-analysis. World J. Pediatr. 2023, 19, 549–556. [Google Scholar] [CrossRef]
- Pérez Tarazona, S.; Solano Galán, P.; Bartoll Alguacil, E.; Alfonso Diego, J. Bronchopulmonary dysplasia as a risk factor for asthma in school children and adolescents: A systematic review. Allergol. Immunopathol. (Madr.) 2018, 46, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Filippone, M.; Carraro, S.; Baraldi, E. The term asthma should be avoided in describing the chronic pulmonary disease of prematurity. Eur. Respir. J. 2013, 42, 1430–1431. [Google Scholar] [CrossRef] [PubMed]
- Suresh, S.; Mamun, A.A.; O’Callaghan, M.; Sly, P.D. The impact of birth weight on peak lung function in young adults. Chest 2012, 142, 1603–1610. [Google Scholar] [CrossRef] [PubMed]
- Lum, S.; Kirkby, J.; Welsh, L.; Marlow, N.; Hennessy, E.; Stocks, J. Nature and severity of lung function abnormalities in extremely pre-term children at 11 years of age. Eur. Respir. J. 2011, 37, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Baraldi, E.; Bonetto, G.; Zacchello, F.; Filippone, M. Low exhaled nitric oxide in school-age children with bronchopulmonary dysplasia and airflow limitation. Am. J. Respir. Crit. Care Med. 2005, 171, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Carraro, S.; Scheltema, N.; Bont, L.; Baraldi, E. Early-life origins of chronic respiratory diseases: Understanding and promoting healthy ageing. Eur. Respir. J. 2014, 44, 1682–1696. [Google Scholar] [CrossRef] [PubMed]
- Riscassi, S.; Corradi, M.; Andreoli, R.; Maccari, C.; Mercolini, F.; Pescollderungg, L.; Caffarelli, C. Nitric oxide products and aldehydes in exhaled breath condensate in children with asthma. Clin. Exp. Allergy 2022, 52, 561–564. [Google Scholar] [CrossRef]
- Manna, A.; Caffarelli, C.; Varini, M.; Povesi Dascola, C.; Montella, S.; Maglione, M.; Sperlì, F.; Santamaria, F. Clinical application of exhaled nitric oxide measurement in pediatric lung diseases. Ital. J. Pediatr. 2012, 31, 38–74. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Hauth, J.C.; Andrews, W.W. Intrauterine infection and preterm delivery. N. Engl. J. Med. 2000, 342, 1500–1507. [Google Scholar] [CrossRef]
- Stocks, J.; Hislop, A.; Sonnappa, S. Early lung development: Lifelong effect on respiratory health and disease. Lancet Respir. Med. 2013, 1, 728–742. [Google Scholar] [CrossRef]
- Barnes, P.J. Immunology of asthma and chronic obstructive pulmonary disease. Nat. Rev. Immunol. 2008, 8, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Teig, N.; Allali, M.; Rieger, C.; Hamelmann, E. Inflammatory markers in induced sputum of school children born before 32 completed weeks of gestation. J. Pediatr. 2012, 161, 1085–1090. [Google Scholar] [CrossRef]
- Caffarelli, C.; Dascola, C.P.; Peroni, D.; Ricò, S.; Stringari, G.; Varini, M.; Folesani, G.; Corradi, M. Airway acidification in childhood asthma exacerbations. Allergy Asthma Proc. 2014, 35, 51–56. [Google Scholar] [CrossRef]
- Di Palmo, E.; Filice, E.; Cavallo, A.; Caffarelli, C.; Maltoni, G.; Miniaci, A.; Ricci, G.; Pession, A. Childhood obesity and respiratory diseases: Which link? Children 2021, 8, 177. [Google Scholar] [CrossRef] [PubMed]
- Siltanen, M.; Wehkalampi, K.; Hovi, P.; Eriksson, J.G.; Strang-Karlsson, S.; Järvenpää, A.L.; Andersson, S.; Kajantie, E. Preterm birth reduces the incidence of atopy in adulthood. J. Allergy Clin. Immunol. 2011, 127, 935–942. [Google Scholar] [CrossRef] [PubMed]
- Siltanen, M.; Savilahti, E.; Pohjavuori, M.; Kajosaari, M. Respiratory symptoms and lung function in relation to atopy in children born preterm. Pediatr. Pulmonol. 2004, 37, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Mitselou, N.; Andersson, N.; Bergström, A.; Kull, I.; Georgelis, A.; van Hage, M.; Hedman, A.M.; Almqvist, C.; Ludvigsson, J.F.; Melén, E. Preterm birth reduces the risk of IgE sensitization up to early adulthood: A population-based birth cohort study. Allergy 2022, 77, 1570–1582. [Google Scholar] [CrossRef]
- Cipriani, F.; Tripodi, S.; Panetta, V.; Perna, S.; Potapova, E.; Dondi, A.; Bernardini, R.; Caffarelli, C.; Casani, A.; Cervone, R.; et al. Early molecular biomarkers predicting the evolution of allergic rhinitis and its comorbidities: A longitudinal multicenter study of a patient cohort. Pediatr. Allergy Immunol. 2019, 30, 325–334. [Google Scholar] [CrossRef]
- Pekkanen, J.; Xu, B.; Järvelin, M.R. Gestational age and occurrence of atopy at age 31—A prospective birth cohort study in Finland. Clin. Exp. Allergy 2001, 31, 95–102. [Google Scholar] [CrossRef]
- Garioud, A.L.B.; Skoven, F.H.; Gregersen, R.; Lange, T.; Buchvald, F.; Greisen, G.T. The increased susceptibility to airway infections after preterm birth does not persist into adolescence. PLoS ONE 2020, 15, e0238382. [Google Scholar] [CrossRef]
- Haataja, P.; Korhonen, P.; Ojala, R.; Hirvonen, M.; Korppi, M.; Gissler, M.; Luukkaala, T.; Tammela, O. Hospital admissions for lower respiratory tract infections in children born moderately/late preterm. Pediatr. Pulmonol. 2018, 53, 209–217. [Google Scholar] [CrossRef]
- Montgomery, S.; Bahmanyar, S.; Brus, O.; Hussein, O.; Kosma, P.; Palme-Kilander, C. Respiratory infections in preterm infants and subsequent asthma: A cohort study. BMJ Open 2013, 3, e004034. [Google Scholar] [CrossRef]
- Sigurs, N.; Aljassim, F.; Kjellman, B.; Robinson, P.D.; Sigurbergsson, F.; Bjarnason, R.; Gustafsson, P.M. Asthma and allergy patterns over 18 years after severe RSV bronchiolitis in the first year of life. Thorax 2010, 65, 1045–1052. [Google Scholar] [CrossRef]
- Hyvärinen, M.K.; Kotaniemi-Syrjänen, A.; Reijonen, T.M.; Korhonen, K.; Korppi, M.O. Lung function and bronchial hyper-responsiveness 11 years after hospitalization for bronchiolitis. Acta Paediatr. 2007, 96, 1464–1469. [Google Scholar] [CrossRef]
- Hasegawa, K.; Mansbach, J.M.; Camargo, C.A., Jr. Infectious pathogens and bronchiolitis outcomes. Exp. Rev. Anti-Infect Ther. 2014, 12, 817–828. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Garcia, M.L.; Gonzalez-Carrasco, E.; Bracamonte, T.; Molinero, M.; Pozo, F.; Casas, I.; Calvo, C. Impact of prematurity and severe viral bronchiolitis on asthma development at 6–9 years. J. Asthma Allergy 2020, 18, 343–353. [Google Scholar] [CrossRef]
- Stein, R.T.; Sherrill, D.; Morgan, W.J.; Holberg, C.J.; Halonen, M.; Taussig, L.M.; Wright, A.L.; Martinez, F.D. Respiratory syncytial virus in early life and risk of wheeze and allergy by age 13 years. Lancet 1999, 14, 541–545. [Google Scholar] [CrossRef]
- Henderson, J.; Hilliard, T.N.; Sherriff, A.; Stalker, D.; Al Shammari, N.; Thomas, H.M. Hospitalization for RSV bronchiolitis before 12 months of age and subsequent asthma, atopy and wheeze: A longitudinal birth cohort study. Pediatr. Allergy Immunol. 2005, 16, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Carbonell-Estrany, X.; Pérez-Yarza, E.G.; García, L.S.; Guzmán Cabañas, J.M.; Bòria, E.V.; Atienza, B.B.; IRIS (Infección Respiratoria Infantil por Virus Respiratorio Sincitial) Study Group. Long-term burden and respiratory effects of respiratory syncytial virus hospitalization in preterm infants-the SPRING study. PLoS ONE 2015, 10, e0125422. [Google Scholar] [CrossRef]
- Anderson, E.J.; Carbonell-Estrany, X.; Blanken, M.; Lanari, M.; Sheridan-Pereira, M.; Rodgers-Gray, B.; Fullarton, J.; Rouffiac, E.; Vo, P.; Notario, G.; et al. Burden of severe respiratory syncytial virus disease among 33-35 weeks’ gestational age infants born during multiple respiratory syncytial virus seasons. Pediatr. Infect. Dis. J. 2017, 36, 160–167. [Google Scholar] [CrossRef]
- Driscoll, A.J.; Arshad, S.H.; Bont, L.; Brunwasser, S.M.; Cherian, T.; Englund, J.A.; Fell, D.B.; Hammitt, L.L.; Hartert, T.V.; Innis, B.L.; et al. Does respiratory syncytial virus lower respiratory illness in early life cause recurrent wheeze of early childhood and asthma? Critical review of the evidence and guidance for future studies from a World Health Organization-sponsored meeting. Vaccine 2020, 38, 2435–2448. [Google Scholar] [CrossRef] [PubMed]
- Blanken, M.O.; Rovers, M.M.; Molenaar, J.M.; Winkler-Seinstra, P.L.; Meijer, A.; Kimpen, J.L.; Bont, L.; Dutch RSV Neonatal Network. Respiratory syncytial virus and recurrent wheeze in healthy preterm infants. N. Engl. J. Med. 2013, 368, 1791–1799. [Google Scholar] [CrossRef] [PubMed]
- Yoshihara, S.; Kusuda, S.; Mochizuki, H.; Okada, K.; Nishima, S.; Simões, E.A. Effect of palivizumab prophylaxis on subsequent recurrent wheezing in preterm infants. Pediatrics 2013, 132, 811–818.e1. [Google Scholar] [CrossRef]
- Simoes, E.A.; Groothuis, J.R.; Carbonell-Estrany, X.; Rieger, C.H.; Mitchell, I.; Fredrick, L.M.; Kimpen, J.L.; Palivizumab Long-Term Respiratory Outcomes Study Group. Palivizumab prophylaxis, respiratory syncytial virus, and subsequent recurrent wheezing. J. Pediatr. 2007, 151, 34–42.e1. [Google Scholar] [CrossRef]
- Moreno-Galdó, A.; Pérez-Yarza, E.G.; Ramilo, O.; Rubí, T.; Escribano, A.; Torres, A.; Sardón, O.; Oliva, C.; Pérez, G.; Cortell, I.; et al. Recurrent wheezing during the first 3 years of life in a birth cohort of moderate-to-late preterm infants. Pediatr. Allergy Immunol. 2020, 31, 124–132. [Google Scholar] [CrossRef]
- Igde, M.; Kabasakal, H.; Ozturk, O.; Karatekin, G.; Aygun, C. Palivizumab prophylaxis, respiratory syncytial virus and subsequent development of asthma. Minerva Pediatr. 2018, 70, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Scheltema, N.M.; Nibbelke, E.E.; Pouw, J.; Blanken, M.O.; Rovers, M.M.; Naaktgeboren, C.A.; Mazur, N.I.; Wildenbeest, J.G.; van der Ent, C.K.; Bont, L.J. Respiratory syncytial virus prevention and asthma in healthy preterm infants: A randomized controlled trial. Lancet Respir. Med. 2018, 6, 257–264. [Google Scholar] [CrossRef]
- Mochizuki, H.; Kusuda, S.; Okada, K.; Yoshihara, S.; Furuya, H.; Simões, E.A.F. Palivizumab prophylaxis in preterm infants and subsequent recurrent wheezing. Six-year follow-up study. Am. J. Respir. Crit. Care Med. 2017, 196, 29–38. [Google Scholar] [CrossRef]
- Quinn, L.A.; Shields, M.D.; Sinha, I.; Groves, H.E. Respiratory syncytial virus prophylaxis for prevention of recurrent childhood wheeze and asthma: A systematic review. Syst. Rev. 2020, 9, 269. [Google Scholar] [CrossRef]
- Makrinioti, H.; Hasegawa, K.; Lakoumentas, J.; Xepapadaki, P.; Tsolia, M.; Castro-Rodriguez, J.A.; Feleszko, W.; Jartti, T.; Johnston, S.L.; Bush, A.; et al. The role of respiratory syncytial virus- and rhinovirus-induced bronchiolitis in recurrent wheeze and asthma-A systematic review and meta-analysis. Pediatr. Allergy Immunol. 2022, 33, e13741. [Google Scholar] [CrossRef]
- Drysdale, S.B.; Alcazar-Paris, M.; Wilson, T.; Smith, M.; Zuckerman, M.; Broughton, S.; Rafferty, G.F.; Peacock, J.L.; Johnston, S.L.; Greenough, A. Rhinovirus infection and healthcare utilization in prematurely born infants. Eur. Respir. J. 2013, 42, 1029–1036. [Google Scholar] [CrossRef]
- Jackson, D.J.; Gangnon, R.E.; Evans, M.D.; Roberg, K.A.; Anderson, E.L.; Pappas, T.E.; Printz, M.C.; Lee, W.M.; Shult, P.A.; Reisdorf, E.; et al. Wheezing rhinovirus illnesses in early life predict asthma development in high-risk children. Am. J. Respir. Crit. Care Med. 2008, 178, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Lukkarinen, M.; Koistinen, A.; Turunen, R.; Lehtinen, P.; Vuorinen, T.; Jartti, T. Rhinovirus-induced first wheezing episode predicts atopic but not nonatopic asthma at school age. J. Allergy Clin. Immunol. 2017, 140, 988–995. [Google Scholar] [CrossRef]
- Kusel, M.M.; de Klerk, N.H.; Kebadze, T.; Vohma, V.; Holt, P.G.; Johnston, S.L.; Sly, P.D. Early-life respiratory viral infections, atopic sensitization, and risk of subsequent development of persistent asthma. J. Allergy Clin. Immunol. 2007, 119, 1105–1110. [Google Scholar] [CrossRef]
- Rubner, F.J.; Jackson, D.J.; Evans, M.D.; Gangnon, R.E.; Tisler, C.J.; Pappas, T.E.; Gern, J.E.; Lemanske, R.F., Jr. Early life rhinovirus wheezing, allergic sensitization, and asthma risk at adolescence. J. Allergy Clin. Immunol. 2017, 139, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Costa, L.F.; Queiróz, D.A.; Lopes da Silveira, H.; Bernardino Neto, M.; de Paula, N.T.; Oliveira, T.F.; Tolardo, A.L.; Yokosawa, J. Human rhinovirus and disease severity in children. Pediatrics 2014, 133, e312–e321. [Google Scholar] [CrossRef] [PubMed]
- van Piggelen, R.O.; van Loon, A.M.; Krediet, T.G.; Verboon-Maciolek, M.A. Human rhinovirus causes severe infection in preterm infants. Pediatr. Infect. Dis. J. 2010, 29, 364–365. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.K.; Bugna, J.; Libster, R.; Shepherd, B.E.; Scalzo, P.M.; Acosta, P.L.; Hijano, D.; Reynoso, N.; Batalle, J.P.; Coviello, S.; et al. Human rhinoviruses in severe respiratory disease in very low birth weight infants. Pediatrics 2012, 129, e60–e67. [Google Scholar] [CrossRef] [PubMed]
- Perez, G.F.; Pancham, K.; Huseni, S.; Jain, A.; Rodriguez-Martinez, C.E.; Preciado, D.; Rose, M.C.; Nino, G. Rhinovirus-induced airway cytokines and respiratory morbidity in severely premature children. Pediatr. Allergy Immunol. 2015, 26, 145–152. [Google Scholar] [CrossRef]
- Vu, L.D.; Siefker, D.; Jones, T.L.; You, D.; Taylor, R.; DeVincenzo, J.; Cormier, S.A. Elevated levels of type 2 respiratory innate lymphoid cells in human infants with severe respiratory syncytial virus bronchiolitis. Am. J. Respir. Crit. Care Med. 2019, 200, 1414–1423. [Google Scholar] [CrossRef] [PubMed]
- Chesné, J.; Braza, F.; Mahay, G.; Brouard, S.; Aronica, M.; Magnan, A. IL-17 in severe asthma. Where do we stand? Am. J. Respir. Crit. Care Med. 2014, 190, 1094–1101. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Yu, Y.; Story, R.E.; Pongracic, J.A.; Gupta, R.; Pearson, C.; Ortiz, K.; Bauchner, H.C.; Wang, X. Prematurity, chorioamnionitis, and the development of recurrent wheezing: A prospective birth cohort study. J. Allergy Clin. Immunol. 2008, 121, 878–884.e6. [Google Scholar] [CrossRef] [PubMed]
- Getahun, D.; Strickland, D.; Zeiger, R.S.; Fassett, M.J.; Chen, W.; Rhoads, G.G.; Jacobsen, S.J. Effect of chorioamnionitis on early childhood asthma. Arch. Pediatr. Adolesc. Med. 2010, 164, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, J.A.; Gallagher, K.; Beck, C.; Kumar, R.; Gernand, A.D. Maternal-fetal inflammation in the placenta and the developmental origins of health and disease. Front. Immunol. 2020, 11, 531543. [Google Scholar] [CrossRef] [PubMed]
- Prendergast, M.; May, C.; Broughton, S.; Pollina, E.; Milner, A.D.; Rafferty, G.F.; Greenough, A. Chorioamnionitis, lung function and bronchopulmonary dysplasia in prematurely born infants. Arch. Dis. Child Fetal. Neonatal. Ed. 2011, 96, F270–F274. [Google Scholar] [CrossRef]
- Becroft, D.M.O.; Thompson, J.M.D.; Mitchell, E.A. Placental chorioamnionitis at term: Epidemiology and follow-up in childhood. Pediatr. Dev. Pathol. 2010, 13, 282–290. [Google Scholar] [CrossRef]
- Bonnet, C.; Blondel, B.; Piedvache, A.; Wilson, E.; Bonamy, A.E.; Gortner, L.; Rodrigues, C.; van Heijst, A.; Draper, E.S.; Cuttini, M.; et al. Low breastfeeding continuation to 6 months for very preterm infants: A European multiregional cohort study. Matern. Child Nutr. 2019, 15, e12657. [Google Scholar] [CrossRef]
- Gdalevich, M.; Mimouni, D.; Mimouni, M. Breast-feeding and the risk of bronchial asthma in childhood: A systematic review with meta-analysis of prospective studies. J. Pediatr. 2001, 139, 261–266. [Google Scholar] [CrossRef]
- Dogaru, C.M.; Nyffenegger, D.; Pescatore, A.M.; Spycher, B.D.; Kuehni, C.E. Breastfeeding and childhood asthma: Systematic review and meta-analysis. Am. J. Epidemiol. 2014, 179, 1153–1167. [Google Scholar] [CrossRef]
- Lodge, C.J.; Tan, D.J.; Lau, M.; Dai, X.; Tham, R.; Lowe, A.J.; Bowatte, G.; Allen, K.J.; Dharmage, S.C. Breastfeeding and asthma and allergies: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 38–53. [Google Scholar] [CrossRef]
- Christian, P.; Smith, E.R.; Lee, S.E.; Vargas, A.J.; Bremer, A.A.; Raiten, D.J. The need to study human milk as a biological system. Am. J. Clin. Nutr. 2021, 113, 1063–1072. [Google Scholar] [CrossRef] [PubMed]
- Strachan, D.P. Hay fever, hygiene, and household size. BMJ 1989, 299, 1259–1260. [Google Scholar] [CrossRef] [PubMed]
- Garn, H.; Potaczek, D.P.; Pfefferle, P.I. The hygiene hypothesis and new perspectives—Current challenges meeting an old postulate. Front. Immunol. 2021, 2, 637087. [Google Scholar] [CrossRef] [PubMed]
- Barcik, W.; Boutin, R.C.T.; Sokolowska, M.; Finlay, B.B. The role of lung and gut microbiota in the pathology of asthma. Immunity 2020, 52, 241–255. [Google Scholar] [CrossRef] [PubMed]
- Fujimura, K.E.; Sitarik, A.R.; Havstad, S.; Lin, D.L.; Levan, S.; Fadrosh, D.; Panzer, A.R.; LaMere, B.; Rackaityte, E.; Lukacs, N.W.; et al. Neonatal gut microbiota associates with childhood multisensitized atopy and T cell differentiation. Nat. Med. 2016, 22, 1187–1191. [Google Scholar] [CrossRef] [PubMed]
- Depner, M.; Taft, D.H.; Kirjavainen, P.V.; Kalanetra, K.M.; Karvonen, A.M.; Peschel, S.; Schmausser-Hechfellner, E.; Roduit, C.; Frei, R.; Lauener, R.; et al. Maturation of the gut microbiome during the first year of life contributes to the protective farm effect on childhood asthma. Nat. Med. 2020, 26, 1766–1775. [Google Scholar] [CrossRef] [PubMed]
- Bisgaard, H.; Hermansen, M.N.; Buchvald, F.; Loland, L.; Halkjaer, L.B.; Bønnelykke, K.; Brasholt, M.; Heltberg, A.; Vissing, N.H.; Thorsen, S.V.; et al. Childhood asthma after bacterial colonization of the airway in neonates. N. Engl. J. Med. 2007, 357, 1487–1495. [Google Scholar] [CrossRef]
- Raita, Y.; Pérez-Losada, M.; Freishtat, R.J.; Hahn, A.; Castro-Nallar, E.; Ramos-Tapia, I.; Stearrett, N.; Bochkov, Y.A.; Gern, J.E.; Mansbach, J.M.; et al. Nasopharyngeal metatranscriptome profiles of infants with bronchiolitis and risk of childhood asthma: A multicentre prospective study. Eur. Respir. J. 2022, 60, 2102293. [Google Scholar] [CrossRef]
- Vissing, N.H.; Chawes, B.L.; Bisgaard, H. Increased risk of pneumonia and bronchiolitis after bacterial colonization of the airways as neonates. Am. J. Respir. Crit. Care Med. 2013, 188, 1246–1252. [Google Scholar] [CrossRef]
- Zimmermann, P.; Messina, N.; Mohn, W.W.; Finlay, B.B.; Curtis, N. Association between the intestinal microbiota and allergic sensitization, eczema, and asthma: A systematic review. J. Allergy Clin. Immunol. 2019, 143, 467–485. [Google Scholar]
- Huang, Y.J.; Nelson, C.E.; Brodie, E.L.; Desantis, T.Z.; Baek, M.S.; Liu, J.; Woyke, T.; Allgaier, M.; Bristow, J.; Wiener-Kronish, J.P.; et al. National Heart, Lung, and Blood Institute’s Asthma Clinical Research Network. Airway microbiota and bronchial hyperresponsiveness in patients with suboptimally controlled asthma. J. Allergy Clin. Immunol. 2011, 127, 372–381.e1–3. [Google Scholar] [CrossRef]
- Olin, A.; Henckel, E.; Chen, Y.; Lakshmikanth, T.; Pou, C.; Mikes, J.; Gustafsson, A.; Bernhardsson, A.K.; Zhang, C.; Bohlin, K.; et al. Stereotypic immune system development in newborn children. Cell 2018, 174, 1277–1292.e14. [Google Scholar] [CrossRef] [PubMed]
- Henrick, B.M.; Rodriguez, L.; Lakshmikanth, T.; Pou, C.; Henckel, E.; Arzoomand, A.; Olin, A.; Wang, J.; Mikes, J.; Tan, Z.; et al. Bifidobacteria-mediated immune system imprinting early in life. Cell 2021, 184, 3884–3898.e11. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, S.; Toh, H.; Hase, K.; Oshima, K.; Nakanishi, Y.; Yoshimura, K.; Tobe, T.; Clarke, J.M.; Topping, D.L.; Suzuki, T.; et al. Bifidobacteria can protect from enteropathogenic infection through production of acetate. Nature 2011, 469, 543–547. [Google Scholar] [CrossRef]
- Thavagnanam, S.; Fleming, J.; Bromley, A.; Shields, M.D.; Cardwell, C.R. A meta-analysis of the association between Caesarean section and childhood asthma. Clin. Exp. Allergy 2008, 38, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Darabi, B.; Rahmati, S.; HafeziAhmadi, M.R.; Badfar, G.; Azami, M. The association between caesarean section and childhood asthma: An updated systematic review and meta-analysis. Allergy Asthma Clin. Immunol. 2019, 15, 62. [Google Scholar] [CrossRef] [PubMed]
- Debley, J.S.; Smith, J.M.; Redding, G.J.; Critchlow, C.W. Childhood asthma hospitalization risk after cesarean delivery in former term and premature infants. Ann. Allergy Asthma Immunol. 2005, 94, 228–233. [Google Scholar] [CrossRef]
- Bäckhed, F.; Roswall, J.; Peng, Y.; Feng, Q.; Jia, H.; Kovatcheva-Datchary, P.; Li, Y.; Xia, Y.; Xie, H.; Zhong, H.; et al. Dynamics and stabilization of the human gut microbiome during the first year of life. Cell Host Microbe 2015, 17, 690–703. [Google Scholar] [CrossRef]
- Zhang, C.; Li, L.; Jin, B.; Xu, X.; Zuo, X.; Li, Y.; Li, Z. The effects of delivery mode on the gut microbiota and health: State of Art. Front. Microbiol. 2021, 12, 724449. [Google Scholar] [CrossRef] [PubMed]
- Bizzarro, M.J. Avoiding unnecessary antibiotic exposure in premature infants: Understanding when (not) to start and when to stop. JAMA Netw. Open 2018, 1, e180165. [Google Scholar] [CrossRef]
- Cait, A.; Wedel, A.; Arntz, J.L.; Duinkerken, J.; Datye, S.; Cait, J.; Alhasan, M.M.; Conrad, M.L. Prenatal antibiotic exposure, asthma, and the atopic march: A systematic review and meta-analysis. Allergy 2022, 77, 3233–3248. [Google Scholar] [CrossRef]
- Strömberg Celind, F.; Wennergren, G.; Vasileiadou, S.; Alm, B.; Goksör, E. Antibiotics in the first week of life were associated with atopic asthma at 12 years of age. Acta Paediatr. 2018, 107, 1798–1804. [Google Scholar] [CrossRef] [PubMed]
- Alm, B.; Erdes, L.; Möllborg, P.; Pettersson, R.; Norvenius, S.G.; Aberg, N.; Wennergren, G. Neonatal antibiotic treatment is a risk factor for early wheezing. Pediatrics 2008, 121, 697–702. [Google Scholar] [CrossRef] [PubMed]
- Kelderer, F.; Mogren, I.; Eriksson, C.; Silfverdal, S.A.; Domellöf, M.; West, C.E. Associations between pre- and postnatal antibiotic exposures and early allergic outcomes: A population-based birth cohort study. Pediatr. Allergy Immunol. 2022, 33, e13848. [Google Scholar] [CrossRef]
- Patrick, D.M.; Sbihi, H.; Dai, D.L.Y.; Al Mamun, A.; Rasali, D.; Rose, C.; Marra, F.; Boutin, R.C.T.; Petersen, C.; Stiemsma, L.T.; et al. Decreasing antibiotic use, the gut microbiota, and asthma incidence in children: Evidence from population-based and prospective cohort studies. Lancet Respir. Med. 2020, 8, 1094–1105. [Google Scholar] [CrossRef]
- Azad, M.B.; Konya, T.; Persaud, R.R.; Guttman, D.S.; Chari, R.S.; Field, C.J.; Sears, M.R.; Mandhane, P.J.; Turvey, S.E.; Subbarao, P.; et al. Impact of maternal intrapartum antibiotics, method of birth and breastfeeding on gut microbiota during the first year of life: A prospective cohort study. Br. J. Obstet. Gynaecol. 2016, 123, 983–993. [Google Scholar] [CrossRef] [PubMed]
- Arrieta, M.C.; Stiemsma, L.T.; Dimitriu, P.A.; Thorson, L.; Russell, S.; Yurist-Doutsch, S.; Kuzeljevic, B.; Gold, M.J.; Britton, H.M.; Lefebvre, D.L.; et al. Early infancy microbial and metabolic alterations affect risk of childhood asthma. Sci. Transl. Med. 2015, 7, 307ra152. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.R.; Bracken, M.B. A systematic review and meta-analysis of prospective studies on the association between maternal cigarette smoking and preterm delivery. Am. J. Obstet. Gynecol. 2000, 182, 465–472. [Google Scholar] [CrossRef]
- Wagijo, M.A.; Sheikh, A.; Duijts, L.; Been, J.V. Reducing tobacco smoking and smoke exposure to prevent preterm birth and its complications. Paediatr. Respir. Rev. 2017, 22, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Lannero, E.; Wickman, M.; Pershagen, G.; Nordvall, L. Maternal smoking during pregnancy increases the risk of recurrent wheezing during the first years of life (BAMSE). Respir. Res. 2006, 7, 3. [Google Scholar] [CrossRef]
- Jaakkola, J.J.; Kosheleva, A.A.; Katsnelson, B.A.; Kuzmin, S.; Privalova, L.; Spengler, J.D. Prenatal and postnatal tobacco smoke exposure and respiratory health in Russian children. Respir. Res. 2006, 7, 48. [Google Scholar] [CrossRef] [PubMed]
- Grabenhenrich, L.B.; Gough, H.; Reich, A.; Eckers, N.; Zepp, F.; Nitsche, O.; Forster, J.; Schuster, A.; Schramm, D.; Bauer, C.P.; et al. Early-life determinants of asthma from birth to age 20 years: A German birth cohort study. J. Allergy Clin. Immunol. 2014, 133, 979–988. [Google Scholar] [CrossRef] [PubMed]
- Leonardi-Bee, J.; Smyth, A.; Britton, J.; Coleman, T. Environmental tobacco smoke and fetal health: Systematic review and meta-analysis. Arch. Dis. Child Fetal. Neonatal. Ed. 2008, 93, F351–F361. [Google Scholar] [CrossRef] [PubMed]
- Salmasi, G.; Grady, R.; Jones, J.; McDonald, S.D.; Knowledge Synthesis Group. Environmental tobacco smoke exposure and perinatal outcomes: A systematic review and meta-analyses. Acta Obstet. Gynecol. Scand. 2010, 89, 423–441. [Google Scholar] [CrossRef]
- Jaakkola, J.J.; Gissler, M. Maternal smoking in pregnancy, fetal development, and childhood asthma. Am. J. Public Health 2004, 94, 136–140. [Google Scholar] [CrossRef]
- Jaakkola, J.J.; Jaakkola, N.; Zahlsen, K. Fetal growth and length of gestation in relation to exposure to environmental tobacco smoke measured by hair nicotine concentration. Environ. Health Perspect. 2001, 109, 557–561. [Google Scholar] [CrossRef]
- Windham, G.C.; Hopkins, B.; Fenster, L.; Swan, S.H. Prenatal active or passive tobacco smoke exposure and the risk of preterm delivery or low birth weight. Epidemiology 2000, 11, 427–433. [Google Scholar] [CrossRef]
- Andres, R.L.; Day, M.C. Perinatal complications associated with maternal tobacco use. Semin. Neonatol. 2000, 5, 231–241. [Google Scholar] [CrossRef]
- Lambers, D.S.; Clark, K.E. The maternal and fetal physiologic effects of nicotine. Semin. Perinatol. 1996, 20, 115–126. [Google Scholar] [CrossRef]
- Maritz, G.S.; Dennis, H. Maternal nicotine exposure during gestation and lactation interferes with alveolar development in the neonatal lung. Reprod. Fertil. Dev. 1998, 10, 255–261. [Google Scholar] [CrossRef]
- Isayama, T.; Shah, P.S.; Ye, X.Y.; Dunn, M.; Da Silva, O.; Alvaro, R.; Lee, S.K. Adverse impact of maternal cigarette smoking on preterm infants: A population-based cohort study. Am. J. Perinatol. 2015, 32, 1105–1111. [Google Scholar] [CrossRef]
- Antonucci, R.; Contu, P.; Porcella, A.; Atzeni, C.; Chiappe, S. Intrauterine smoke exposure: A new risk factor for bronchopulmonary dysplasia? J. Perinat. Med. 2004, 32, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Spiegler, J.; Jensen, R.; Segerer, H.; Ehlers, S.; Kühn, T.; Jenke, A.; Gebauer, C.; Möller, J.; Orlikowsky, T.; Heitmann, F.; et al. Influence of smoking and alcohol during pregnancy on outcome of VLBW infants. Z. Geburtshilfe Neonatol. 2013, 217, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Hoo, A.F.; Henschen, M.; Dezateux, C.; Costeloe, K.; Stocks, J. Respiratory function among preterm infants whose mothers smoked during pregnancy. Am. J. Respir. Crit. Care Med. 1998, 158, 700–705. [Google Scholar] [CrossRef] [PubMed]
- Macaubas, C.; de Klerk, N.H.; Holt, B.J.; Wee, C.; Kendall, G.; Firth, M.; Sly, P.D.; Holt, P.G. Association between antenatal cytokine production and the development of atopy and asthma at age 6 years. Lancet 2003, 362, 1192–1197. [Google Scholar] [CrossRef] [PubMed]
- Blacquiere, M.J.; Timens, W.; Melgert, B.N.; Geerlings, M.; Postma, D.S.; Hylkema, M.N. Maternal smoking during pregnancy induces airway remodelling in mice offspring. Eur. Respir. J. 2009, 33, 1133–1140. [Google Scholar] [CrossRef]
- Ferrini, M.; Carvalho, S.; Cho, Y.H.; Postma, B.; Miranda Marques, L.; Pinkerton, K.; Roberts, K.; Jaffar, Z. Prenatal tobacco smoke exposure predisposes offspring mice to exacerbated allergic airway inflammation associated with altered innate effector function. Part. Fibre Toxicol. 2017, 14, 30. [Google Scholar] [CrossRef]
- Kurihara, C.; Kuniyoshi, K.M.; Rehan, V.K. Preterm birth, developmental smoke/nicotine exposure, and life-long pulmonary sequelae. Children 2023, 10, 608. [Google Scholar] [CrossRef]
- Gao, L.; Liu, X.; Millstein, J.; Siegmund, K.D.; Dubeau, L.; Maguire, R.L.; Jim Zhang, J.; Fuemmeler, B.F.; Kollins, S.H.; Hoyo, C.; et al. Self-reported prenatal tobacco smoke exposure, AXL gene-body methylation, and childhood asthma phenotypes. Clin. Epigenetics 2018, 20, 98. [Google Scholar] [CrossRef]
- Neophytou, A.M.; Oh, S.S.; Hu, D.; Huntsman, S.; Eng, C.; Rodríguez-Santana, J.R.; Kumar, R.; Balmes, J.R.; Eisen, E.A.; Burchard, E.G. In utero tobacco smoke exposure, DNA methylation, and asthma in Latino children. Environ. Epidemiol. 2019, 19, e048. [Google Scholar] [CrossRef]
- Cnattingius, S.; Granath, F.; Petersson, G.; Harlow, B.L. The influence of gestational age and smoking habits on the risk of subsequent preterm deliveries. N. Engl. J. Med. 1999, 341, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Räisänen, S.; Sankilampi, U.; Gissler, M.; Kramer, M.R.; Hakulinen-Viitanen, T.; Saari, J.; Heinonen, S. Smoking cessation in the first trimester reduces most obstetric risks, but not the risks of major congenital anomalies and admission to neonatal care: A population-based cohort study of 1,164,953 singleton pregnancies in Finland. J. Epidemiol. Community Health 2014, 68, 159–164. [Google Scholar] [CrossRef]
- Hodyl, N.A.; Stark, M.J.; Scheil, W.; Grzeskowiak, L.E.; Clifton, V.L. Perinatal outcomes following maternal asthma and cigarette smoking during pregnancy. Eur. Respir. J. 2014, 43, 704–716. [Google Scholar] [CrossRef] [PubMed]
- McCowan, L.M.; Dekker, G.A.; Chan, E.; Stewart, A.; Chappell, L.C.; Hunter, M.; Moss-Morris, R. Spontaneous preterm birth and small for gestational age infants in women who stop smoking early in pregnancy: Prospective cohort study. BMJ 2009, 338, b1081. [Google Scholar] [CrossRef] [PubMed]
- Miyake, Y.; Tanaka, K.; Arakawa, M. Active and passive maternal smoking during pregnancy and birth outcomes: The Kyushu Okinawa maternal and child health study. BMC Pregnancy Childbirth 2013, 13, 157. [Google Scholar] [CrossRef]
- Nkansah-Amankra, S. Neighborhood contextual factors, maternal smoking, and birth outcomes: Multilevel analysis of the South Carolina PRAMS survey, 2000–2003. J. Women’s Health 2010, 19, 1543–1552. [Google Scholar] [CrossRef] [PubMed]
- Soneji, S.; Beltrán-Sánchez, H. Association of Maternal Cigarette Smoking and Smoking Cessation With Preterm Birth. JAMA Netw. Open 2019, 2, e192514. [Google Scholar] [CrossRef] [PubMed]
- Lim, R.H.; Kobzik, L.; Dahl, M. Risk for asthma in offspring of asthmatic mothers versus fathers: A meta-analysis. PLoS ONE 2010, 5, e10134. [Google Scholar] [CrossRef] [PubMed]
- Pagano, F.; Conti, M.G.; Boscarino, G.; Pannucci, C.; Dito, L.; Regoli, D.; Di Chiara, M.; Battaglia, G.; Prota, R.; Cinicola, B.; et al. Atopic Manifestations in Children Born Preterm: A Long-Term Observational Study. Children 2021, 8, 843. [Google Scholar] [CrossRef]
- Bravo-Solarte, D.C.; Garcia-Guaqueta, D.P.; Chiarella, S.E. Asthma in pregnancy. Allergy Asthma Proc. 2023, 44, 24–34. [Google Scholar] [CrossRef]
- Plummer, E.L.; Chebar Lozinsky, A.; Tobin, J.M.; Uebergang, J.B.; Axelrad, C.; Garland, S.M.; Jacobs, S.E.; Tang, M.L.K.; ProPrems Study Group. Postnatal probiotics and allergic disease in very preterm infants: Sub-study to the ProPrems randomized trial. Allergy 2020, 75, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Caffarelli, C.; Cardinale, F.; Povesi-Dascola, C.; Dodi, I.; Mastrorilli, V.; Ricci, G. Use of probiotics in pediatric infectious diseases. Expert Rev. Anti Infect Ther. 2015, 13, 1517–1535. [Google Scholar] [CrossRef] [PubMed]
- Mennini, M.; Dahdah, L.; Artesani, M.C.; Fiocchi, A.; Martelli, A. Probiotics in Asthma and Allergy Prevention. Front. Pediatr. 2017, 5, 165. [Google Scholar] [CrossRef] [PubMed]
- Adnan, M.; Wu, S.Y.; Khilfeh, M.; Davis, V. Vitamin D status in very low birth weight infants and response to vitamin D intake during their NICU stays: A prospective cohort study. J. Perinatol. 2022, 42, 209–216. [Google Scholar] [CrossRef]
- Litonjua, A.A.; Carey, V.J.; Laranjo, N.; Stubbs, B.J.; Mirzakhani, H.; O’Connor, G.T.; Sandel, M.; Beigelman, A.; Bacharier, L.B.; Zeiger, R.S.; et al. Six-year follow-up of a trial of antenatal vitamin D for asthma reduction. N. Engl. J. Med. 2020, 382, 525–533. [Google Scholar] [CrossRef] [PubMed]
- de Boer, G.M.; Żółkiewicz, J.; Strzelec, K.P.; Ruszczyński, M.; Hendriks, R.W.; Braunstahl, G.J.; Feleszko, W.; Tramper-Stranders, G.A. Bacterial lysate therapy for the prevention of wheezing episodes and asthma exacerbations: A systematic review and meta-analysis. Eur. Respir. Rev. 2020, 29, 190175. [Google Scholar] [CrossRef]
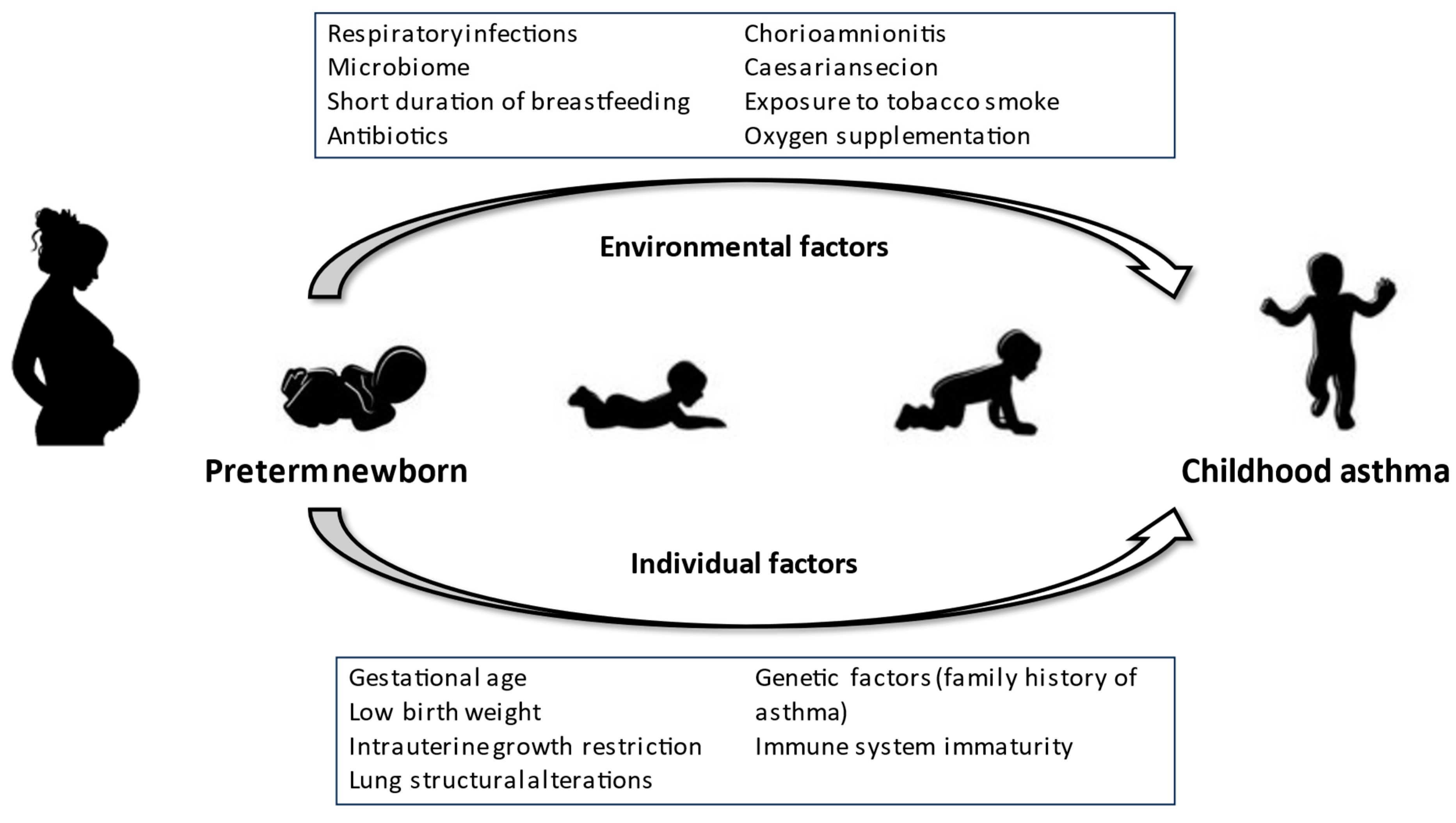
Figure 1.
The effects of environmental and individual factors leading the preterm newborn to the development of childhood asthma.
Figure 1.
The effects of environmental and individual factors leading the preterm newborn to the development of childhood asthma.


{kind=link}
Table 1.
Risk factors associated with the development of childhood asthma in preterm babies vs. full-term babies without the risk factors (if not otherwise specified).
Table 1.
Risk factors associated with the development of childhood asthma in preterm babies vs. full-term babies without the risk factors (if not otherwise specified).
| Risk Factor | Risk of Asthma (Odds Ratio/Relative Risk and 95% Confidence Intervals) * |
|---|---|
| Very preterm (<32 wGA) | 3.9 (3.2–4.8) |
| Moderate–late preterm (33–36 wGA) | 1.7 (1.4–2.0) |
| Extremely low birth weight (<1000 g) | 1.8 (1.1–1.4) |
| Very low birth weight (<1500 g) | 1.43 (1.34–1.54) (compared to LBW) |
| Childhood weight gain >700 g/month | 4.47 (2.58–7.76) |
| Oxygen supplementation in VLBW | 4.3 (1.3–14.0) |
| Respiratory infections in <28 wGA | 2.2 (1.59–3.09) (compared to <28 wGA without respiratory infections) |
| RSV bronchiolitis | 3.8 (3.23–4.58) (no effects of palivizumab) |
| RV wheezing | 25.6 (8.2–79.6) |
| Chorioamnionitis in preterms | 2.9 (2.6–3.3) (compared to chorioamnionitis in full-terms) |
| Airway bacterial colonization | 4.57 (2.18–9.57) |
| Delivery by caesarian section | 1.2 (1.04–1.39) |
| Early antibiotic exposure | 2.2 (1.2–4.2) |
| Maternal smoking in pregnancy | 1.35 (1.13–1.62) |
* According to the data cited in the paper. VLBW, very low birth weught; RSV, respiratory syncytial virus; RV, rhinovirus.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Caffarelli, C.; Gracci, S.; Giannì, G.; Bernardini, R. Are Babies Born Preterm High-Risk Asthma Candidates? J. Clin. Med. 2023, 12, 5400. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12165400
AMA Style
Caffarelli C, Gracci S, Giannì G, Bernardini R. Are Babies Born Preterm High-Risk Asthma Candidates? Journal of Clinical Medicine. 2023; 12(16):5400. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12165400
Chicago/Turabian StyleCaffarelli, Carlo, Serena Gracci, Giuliana Giannì, and Roberto Bernardini. 2023. "Are Babies Born Preterm High-Risk Asthma Candidates?" Journal of Clinical Medicine 12, no. 16: 5400. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm12165400
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.