
Exploring Iodide and Hydrogen Sulfide as ROS Scavengers to Delay Acute Rejection in MHC-Defined Vascularized Composite Allografts


 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
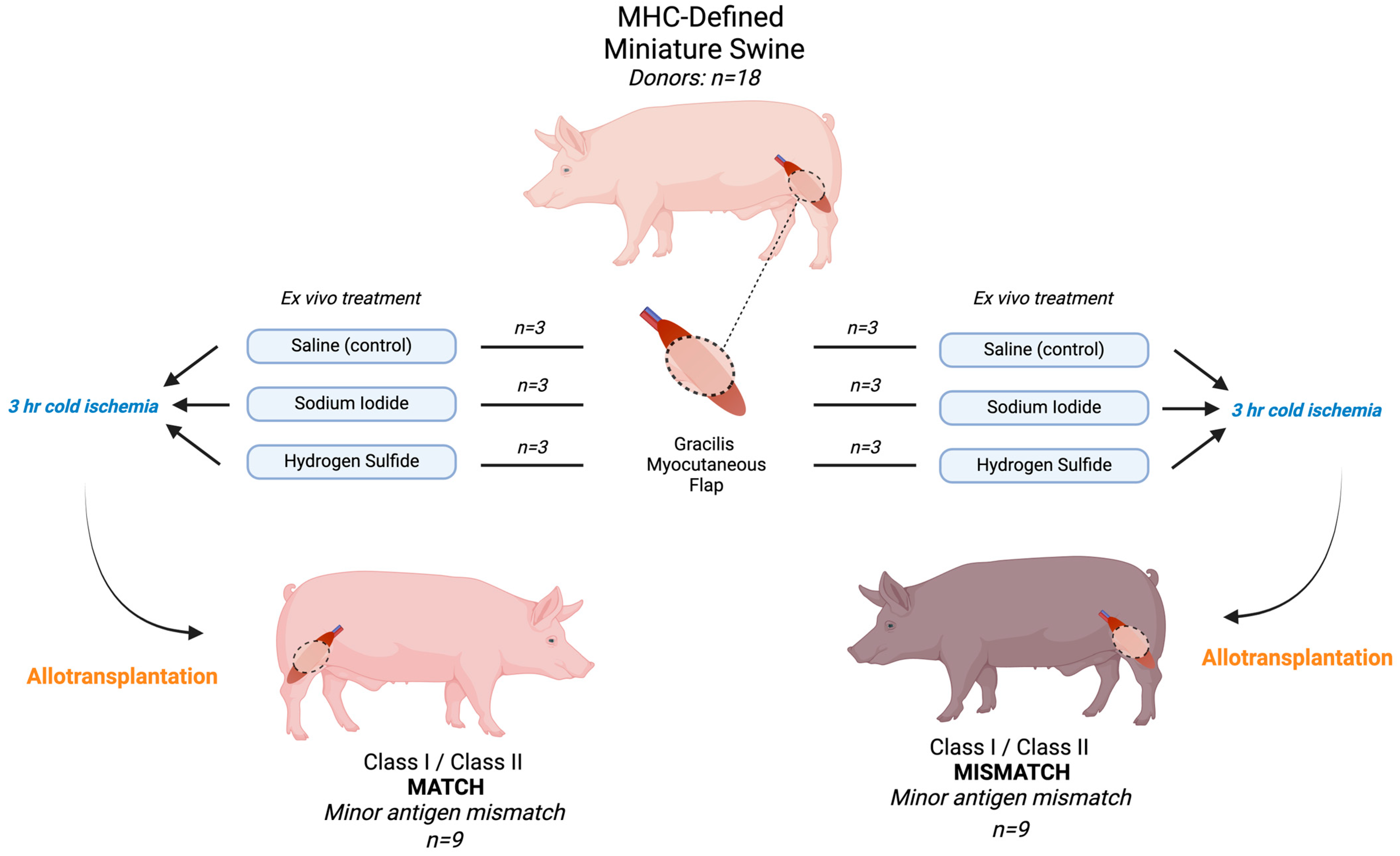
2.1. Animal Use and Experimental Design
2.2. Surgical Model
2.3. Flap Treatment
2.4. Preparation of Oxygen Free Radical Scavengers
- -
- Saline (control): treatment of the flap with 0.9% saline solution.
- -
- Sodium iodide (NaI): solution containing 10 mg/mL. Animals in this group received an additional intravenous dose of 1 mg/mL one minute after the anastomosis was unclamped.
- -
- Hydrogen sulfide (H2S): solution containing 2 mg/kg.
2.5. Drinking Water
2.6. Blood Analysis
2.7. Histopathology
2.8. Statistical Analysis
2.9. Endpoints and Recipient Euthanasia
3. Results
3.1. Postoperative Clinical Observations and Pathology Assessment in the MATCH Group
3.2. Postoperative Clinical Observations and Pathology Assessment in the MISMATCH Group
3.3. Effect of Sodium Iodide (NaI) Treatment on Blood Enzyme Levels in MATCH and MISMATCH Groups
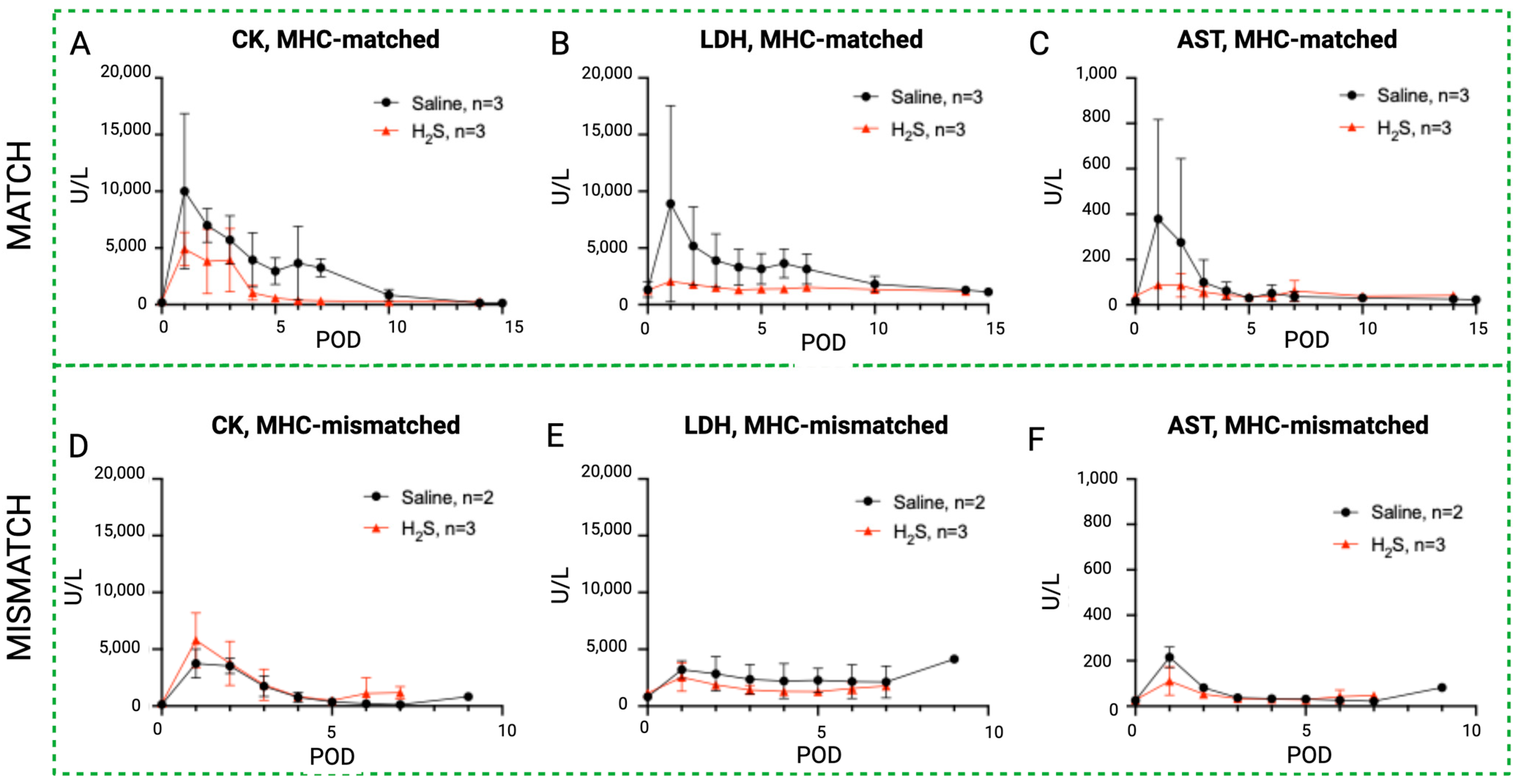
3.4. Effect of Hydrogen Sulfide (H2S) Treatment on Blood Enzyme Levels in MATCH and MISMATCH Groups
3.5. Blood Enzyme Levels in MATCH vs. MISMATCH Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Petruzzo, P.; Lanzetta, M.; Dubernard, J.M.; Landin, L.; Cavadas, P.; Margreiter, R.; Schneeberger, S.; Breidenbach, W.; Kaufman, C.; Jablecki, J.; et al. The International Registry on Hand and Composite Tissue Transplantation. Transplantation 2010, 90, 1590–1594. [Google Scholar] [CrossRef] [PubMed]
- Gok, E.; Kubiak, C.A.; Guy, E.; Kemp, S.W.P.; Ozer, K. Effect of Static Cold Storage on Skeletal Muscle after Vascularized Composite Tissue Allotransplantation. J. Reconstr. Microsurg. 2020, 36, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Gillani, S.; Cao, J.; Suzuki, T.; Hak, D.J. The effect of ischemia reperfusion injury on skeletal muscle. Injury 2012, 43, 670–675. [Google Scholar] [CrossRef]
- Siemionow, M.; Arslan, E. Ischemia/reperfusion injury: A review in relation to free tissue transfers. Microsurgery 2004, 24, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Zelt, R.G.; Olding, M.; Kerrigan, C.L.; Daniel, R.K. Primary and secondary critical ischemia times of myocutaneous flaps. Plast. Reconstr. Surg. 1986, 78, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Toyokuni, S. Reactive oxygen species-induced molecular damage and its application in pathology. Pathol. Int. 1999, 49, 91–102. [Google Scholar] [CrossRef]
- He, J.; Khan, U.Z.; Qing, L.; Wu, P.; Tang, J. Improving the ischemia-reperfusion injury in vascularized composite allotransplantation: Clinical experience and experimental implications. Front. Immunol. 2022, 13, 998952. [Google Scholar] [CrossRef]
- Kruit, A.S.; Smits, L.; Pouwels, A.; Schreinemachers, M.J.M.; Hummelink, S.L.M.; Ulrich, D.J.O. Ex-vivo perfusion as a successful strategy for reduction of ischemia-reperfusion injury in prolonged muscle flap preservation—A gene expression study. Gene 2019, 701, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Kadono, K.; Gruszynski, M.; Azari, K.; Kupiec-Weglinski, J.W. Vascularized composite allotransplantation versus solid organ transplantation: Innate-adaptive immune interphase. Curr. Opin. Organ. Transplant. 2019, 24, 714–720. [Google Scholar] [CrossRef]
- Ochando, J.; Ordikhani, F.; Boros, P.; Jordan, S. The innate immune response to allotransplants: Mechanisms and therapeutic potentials. Cell Mol. Immunol. 2019, 16, 350–356. [Google Scholar] [CrossRef]
- Xu, W.; Chen, J.; Lin, J.; Liu, D.; Mo, L.; Pan, W.; Feng, J.; Wu, W.; Zheng, D. Exogenous H2S protects H9c2 cardiac cells against high glucose-induced injury and inflammation by inhibiting the activation of the NF-κB and IL-1β pathways. Int. J. Mol. Med. 2015, 35, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.; Ji, J.; Li, H.; Zhang, X. H2S alleviates renal ischemia and reperfusion injury by suppressing ERS-induced autophagy. Transpl. Immunol. 2024, 83, 102006. [Google Scholar] [CrossRef] [PubMed]
- Winkler, R.; Griebenow, S.; Wonisch, W. Effect of iodide on total antioxidant status of human serum. Cell Biochem. Funct. 2000, 18, 143–146. [Google Scholar] [CrossRef]
- Villamaria, C.Y.; Fries, C.A.; Spencer, J.R.; Roth, M.; Davis, M.R. Hydrogen sulfide mitigates reperfusion injury in a porcine model of vascularized composite autotransplantation. Ann. Plast. Surg. 2014, 72, 594–598. [Google Scholar] [CrossRef] [PubMed]
- Murphy, B.; Bhattacharya, R.; Mukherjee, P. Hydrogen sulfide signaling in mitochondria and disease. FASEB J. 2019, 33, 13098–13125. [Google Scholar] [CrossRef] [PubMed]
- Pedre, B.; Barayeu, U.; Ezeriņa, D.; Dick, T.P. The mechanism of action of N-acetylcysteine (NAC): The emerging role of H2S and sulfane sulfur species. Pharmacol. Ther. 2021, 228, 107916. [Google Scholar] [CrossRef] [PubMed]
- Scammahorn, J.J.; Nguyen, I.T.N.; Bos, E.M.; Van Goor, H.; Joles, J.A. Fighting Oxidative Stress with Sulfur: Hydrogen Sulfide in the Renal and Cardiovascular Systems. Antioxidants 2021, 10, 373. [Google Scholar] [CrossRef] [PubMed]
- Török, S.; Almási, N.; Veszelka, M.; Börzsei, D.; Szabó, R.; Varga, C. Protective Effects of H2S Donor Treatment in Experimental Colitis: A Focus on Antioxidants. Antioxidants 2023, 12, 1025. [Google Scholar] [CrossRef] [PubMed]
- Cendales, L.C.; Kanitakis, J.; Schneeberger, S.; Burns, C.; Ruiz, P.; Landin, L.; Remmelink, M.; Hewitt, C.W.; Landgren, T.; Lyons, B.; et al. The Banff 2007 working classification of skin-containing composite tissue allograft pathology. Am. J. Transpl. 2008, 8, 1396–1400. [Google Scholar] [CrossRef]
- Leto Barone, A.A.; Leonard, D.A.; Torabi, R.; Mallard, C.; Glor, T.; Scalea, J.R.; Randolph, M.A.; Sachs, D.H.; Cetrulo, C.L., Jr. The gracilis myocutaneous free flap in swine: An advantageous preclinical model for vascularized composite allograft transplantation research. Microsurgery 2013, 33, 51–55. [Google Scholar] [CrossRef]
- Morrison, M.L.; Iwata, A.; Keyes, C.C.; Langston, W.; Insko, M.A.; Langdale, L.A.; Roth, M.B. Iodide Improves Outcome After Acute Myocardial Infarction in Rats and Pigs. Crit. Care Med. 2018, 46, e1063–e1069. [Google Scholar] [CrossRef] [PubMed]
- Dubernard, J.M.; Owen, E.; Herzberg, G.; Lanzetta, M.; Martin, X.; Kapila, H.; Dawahra, M.; Hakim, N.S. Human hand allograft: Report on first 6 months. Lancet 1999, 353, 1315–1320. [Google Scholar] [CrossRef]
- Cendales, L.C.; Breidenbach, W.C., 3rd. Hand transplantation. Hand Clin. 2001, 17, 499–510. [Google Scholar] [CrossRef] [PubMed]
- Schneeberger, S.; Kreczy, A.; Brandacher, G.; Steurer, W.; Margreiter, R. Steroid- and ATG-resistant rejection after double forearm transplantation responds to Campath-1H. Am. J. Transplant. 2004, 4, 1372–1374. [Google Scholar] [CrossRef] [PubMed]
- Horváth, T.; Sándor, L.; Baráth, B.; Donka, T.; Baráth, B.; Mohácsi, Á.; Jász, K.D.; Hartmann, P.; Boros, M. Methane Admixture Protects Liver Mitochondria and Improves Graft Function after Static Cold Storage and Reperfusion. Antioxidants 2023, 12, 271. [Google Scholar] [CrossRef] [PubMed]
- Bardallo, R.G.; Company-Marin, I.; Folch-Puy, E.; Roselló-Catafau, J.; Panisello-Rosello, A.; Carbonell, T. PEG35 and Glutathione Improve Mitochondrial Function and Reduce Oxidative Stress in Cold Fatty Liver Graft Preservation. Antioxidants 2022, 11, 158. [Google Scholar] [CrossRef] [PubMed]
- Granata, S.; Votrico, V.; Spadaccino, F.; Catalano, V.; Netti, G.S.; Ranieri, E.; Stallone, G.; Zaza, G. Oxidative Stress and Ischemia/Reperfusion Injury in Kidney Transplantation: Focus on Ferroptosis, Mitophagy and New Antioxidants. Antioxidants 2022, 11, 769. [Google Scholar] [CrossRef] [PubMed]
- Tripatara, P.; SA Patel, N.; Collino, M.; Gallicchio, M.; Kieswich, J.; Castiglia, S.; Benetti, E.; Stewart, K.N.; Brown, P.A.; Yaqoob, M.M. Generation of endogenous hydrogen sulfide by cystathionine γ-lyase limits renal ischemia/reperfusion injury and dysfunction. Lab. Investig. 2008, 88, 1038–1048. [Google Scholar] [CrossRef]
- Tripatara, P.; Patel, N.S.; Brancaleone, V.; Renshaw, D.; Rocha, J.; Sepodes, B.; Mota-Filipe, H.; Perretti, M.; Thiemermann, C. Characterisation of cystathionine gamma-lyase/hydrogen sulphide pathway in ischaemia/reperfusion injury of the mouse kidney: An in vivo study. Eur. J. Pharmacol. 2009, 606, 205–209. [Google Scholar] [CrossRef]
- Han, S.J.; Kim, J.I.; Park, J.W.; Park, K.M. Hydrogen sulfide accelerates the recovery of kidney tubules after renal ischemia/reperfusion injury. Nephrol. Dial. Transplant. 2015, 30, 1497–1506. [Google Scholar] [CrossRef]
- Piko, N.; Bevc, S.; Hojs, R.; Ekart, R. The Role of Oxidative Stress in Kidney Injury. Antioxidants 2023, 12, 1772. [Google Scholar] [CrossRef] [PubMed]
- Sodha, N.R.; Clements, R.T.; Feng, J.; Liu, Y.; Bianchi, C.; Horvath, E.M.; Szabo, C.; Sellke, F.W. The effects of therapeutic sulfide on myocardial apoptosis in response to ischemia-reperfusion injury. Eur. J. Cardiothorac. Surg. 2008, 33, 906–913. [Google Scholar] [CrossRef] [PubMed]
- Francisco, J.; Del Re, D.P. Inflammation in Myocardial Ischemia/Reperfusion Injury: Underlying Mechanisms and Therapeutic Potential. Antioxidants 2023, 12, 1944. [Google Scholar] [CrossRef]
- Iwata, A.; Morrison, M.L.; Roth, M.B. Iodide protects heart tissue from reperfusion injury. PLoS ONE 2014, 9, e112458. [Google Scholar] [CrossRef] [PubMed]
- Fries, C.A.; Lawson, S.D.; Wang, L.C.; Spencer, J.R.; Roth, M.; Rickard, R.F.; Gorantla, V.S.; Davis, M.R. Composite Graft Pretreatment With Hydrogen Sulfide Delays the Onset of Acute Rejection. Ann. Plast. Surg. 2019, 82, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Zdichavsky, M.; Jones, J.W.; Ustuner, E.T.; Ren, X.; Edelstein, J.; Maldonado, C.; Breidenbach, W.; Gruber, S.A.; Ray, M.; Barker, J.H. Scoring of skin rejection in a swine composite tissue allograft model. J. Surg. Res. 1999, 85, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.; Davis, M.R.; Roth, M.; Lawson, S.D.; Cindass, R.; Spencer, J.R. 2603: Ex-vivo graft preservation with hydrogen sulfide and hydrogen iodide for suspended animation of non-human primate (macaca mulatta) upper extremity vascularized composite allotransplants (VCA). Vasc. Compos. Allotransplantation 2016, 3, 61. [Google Scholar] [CrossRef]
- Osipov, R.M.; Robich, M.P.; Feng, J.; Liu, Y.; Clements, R.T.; Glazer, H.P.; Sodha, N.R.; Szabo, C.; Bianchi, C.; Sellke, F.W. Effect of Hydrogen Sulfide in a Porcine Model of Myocardial Ischemia-Reperfusion: Comparison of Different Administration Regimens and Characterization of the Cellular Mechanisms of Protection. J. Cardiovasc. Pharmacol. 2009, 54, 287–297. [Google Scholar] [CrossRef] [PubMed]
- Osipov, R.M.; Robich, M.P.; Feng, J.; Chan, V.; Clements, R.T.; Deyo, R.J.; Szabo, C.; Sellke, F.W. Effect of hydrogen sulfide on myocardial protection in the setting of cardioplegia and cardiopulmonary bypass. Interact. Cardiovasc. Thorac. Surg. 2010, 10, 506–512. [Google Scholar] [CrossRef]
- Huelsboemer, L.; Kauke-Navarro, M.; Reuter, S.; Stoegner, V.A.; Feldmann, J.; Hirsch, T.; Kueckelhaus, M.; Dermietzel, A. Tolerance Induction in Vascularized Composite Allotransplantation—A Brief Review of Preclinical Models. Transpl. Int. 2023, 36, 10955. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Subgroup | # | EOS Day | Banff Grade | Skin Scoring | Comment (Muscle) |
|---|---|---|---|---|---|---|
| MATCH | Saline | 1 | 15 | IV | (pc3, pa3, ei3, e2, v2, c2, cav1) | Focal muscle infiltration, necrosis, and calcification consistent with rejection |
| 2 | 15 | IV | (pc3, pa3, ei3, e2, v3, c2, cav0) | Extensive perivascular inflammation with endothelialitis | ||
| 3 | 14 | IV | (pc3, pa3, ei3, e3, v1, c3, cav3) | Muscle infiltration with focal necrosis | ||
| NaI | 4 | 11 | IV | (pc3, pa3, ei3, e3, v3, ct, cav0) | Extensive inflammation, endarteritis, and focal muscle necrosis | |
| 5 | 12 | IV | (pc3, pa3, ei3, e0, v3, c3, cav0) | Extensive inflammation and necrosis | ||
| 6 | 13 | IV | (pc3, pa3, ei3, e0, v3, c3, cav0) | Frank necrosis, grade IV with muscle involvement | ||
| H2S | 7 | 14 | IV | (pc3, pa3, ei3, e3, v2, c3, cav0) | - | |
| 8 | 14 | IV | (pc3, pa3, ei3, e3, v2, c3, cav0) | Grade IV with muscle involvement | ||
| 9 | 14 | IV | - | Frank necrosis, grade IV with muscle involvement | ||
| MISMATCH | Saline | 10 | 9 | IV | (pc3, pa3, ei3, e2, v3, ct, cav0) | Frank necrosis, subcutaneous tissue and muscle |
| 11 | 7 | III-IV | (pc3, pa3, ei3, e3, v2, c2, cav0) | Diffuse inflammation, focal muscle necrosis | ||
| NaI | 13 | 9 | IV | (pc3, pa3, ei3, e2, v3, c2, cav0) | Frank necrosis, skin, subcutaneous tissue and muscle | |
| 14 | 8 | III | (pc3, pa3, ei3, e2, v3, c2, cav0) | Extensive inflammation and necrosis | ||
| 15 | 6 | IV | (pc3, pa3, ei3, e3, v2, c3, cav0) | Diffuse necrosis | ||
| H2S | 16 | 7 | IV | (pc3, pa3, ei3, e3, v3, c3, cav0) | Grade IV with muscle involvement | |
| 17 | 7 | IV | (pc3, pa3, ei3, e3, v3, c3, cav0) | Extensive necrosis with thrombosis | ||
| 18 | 6 | IV | (pc3, pa3, ei3, e3, v3, c2, cav0) | Diffuse necrosis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tratnig-Frankl, P.; Andrews, A.R.; Berkane, Y.; Guinier, C.; Goutard, M.; Lupon, E.; Lancia, H.H.; Morrison, M.L.; Roth, M.B.; Randolph, M.A.; et al. Exploring Iodide and Hydrogen Sulfide as ROS Scavengers to Delay Acute Rejection in MHC-Defined Vascularized Composite Allografts. Antioxidants 2024, 13, 531. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox13050531
Tratnig-Frankl P, Andrews AR, Berkane Y, Guinier C, Goutard M, Lupon E, Lancia HH, Morrison ML, Roth MB, Randolph MA, et al. Exploring Iodide and Hydrogen Sulfide as ROS Scavengers to Delay Acute Rejection in MHC-Defined Vascularized Composite Allografts. Antioxidants. 2024; 13(5):531. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox13050531
Chicago/Turabian StyleTratnig-Frankl, Philipp, Alec R. Andrews, Yanis Berkane, Claire Guinier, Marion Goutard, Elise Lupon, Hyshem H. Lancia, Michael L. Morrison, Mark B. Roth, Mark A. Randolph, and et al. 2024. "Exploring Iodide and Hydrogen Sulfide as ROS Scavengers to Delay Acute Rejection in MHC-Defined Vascularized Composite Allografts" Antioxidants 13, no. 5: 531. https://0-doi-org.brum.beds.ac.uk/10.3390/antiox13050531