
An Architectural Solution to a Biological Problem: A Systematic Review of Lighting Designs in Healthcare Environments

 ,
,
Abstract
:1. Introduction
2. Background
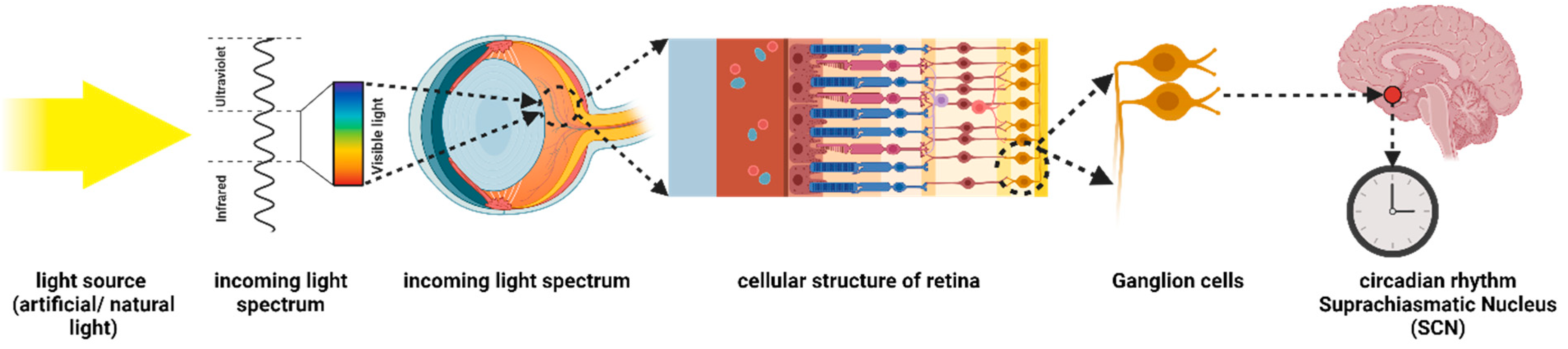
2.1. Circadian Clocks and Rhythms
2.2. Circadian Hygiene in Healthcare Settings
3. Methods
3.1. Information Sources and Study Selection
3.2. Eligibility Criteria
3.3. Screening
3.4. Appraisal of Healthcare Design and Research Studies Based on Levels of Evidence
4. Results
4.1. Study Methodological Characteristics
Interventions and Human Participant Studies
4.2. Sleep-Related Health Outcomes

{kind=link}
{kind=link}
{kind=link}
| Category | Ref. | Setting | Participants | Study Design | Intervention | Mediating Factor | Level |
|---|---|---|---|---|---|---|---|
| Sleep Quality | [32] | Nursing home | Nursing home residents (58 women, 19 men) | Randomized controlled trial | Evening bright light, morning bright light, daytime sleep restriction, evening dim red light | Lighting intensity, timing | 2 |
| [56] | Intensive care units | Patients (n = 19) | Descriptive correlational studies | Cycled lighting environment | Lighting intensity, timing, wavelength | 3a | |
| [25] | Patients’ room | Cardiology ward patients (n = 196) | Controlled clinical trial | Dynamic lighting system | Lighting intensity | 3a | |
| [55] | Patients’ room | Psychiatric patients (n = 54) | Randomized controlled trial | Adjustable lighting | Lighting intensity, CCT, wavelength | 2 | |
| [6] | Patients’ room | Healthy people (n = 12) | Randomized controlled trial | Dynamic lighting system | Blue-depleted light | 2 | |
| [66] | Patients’ room | Psychiatric patients | Randomized controlled trial | Dynamic lighting system | Blue-depleted light | 2 | |
| Sleep- wake Patterns | [64] | Patients’ room | Dementia patients (n = 13) | Pilot study, observations | Biodynamic lighting system | Lighting intensity, CCT | 3a |
| [60] | Patients’ room | Medical inpatients (women = 23; men = 17) | Correlational study or non-experimental study | Dynamic lighting system | Lighting intensity | 2 | |
| Duration | [64] | Patients’ room | Dementia patients (n = 13) | Pilot study, observations | Biodynamic lighting system | Lighting intensity, CCT | 3a |
4.3. Mood and Psychological Outcomes
| Category | Ref. | Setting | Participants | Study Design | Intervention | Mediating Factor | Level |
|---|---|---|---|---|---|---|---|
| Mood Status | [60] | Patients’ room | Medical inpatients (women = 23, men = 17) | Correlational study or non-experimental study | Dynamic lighting system | Light intensity | 2 |
| [25] | Patients’ room | Cardiology ward patients (n = 196) | Controlled clinical trial | Dynamic lighting system | Lighting intensity | 3 | |
| Fatigue Status | [64] | Patients’ room | Dementia patients (n = 13) | Pilot study, observations | Biodynamic lighting system | Lighting intensity, CCT | 3 |
| Anxiety | [25] | Patients’ room | Cardiology ward patients (n = 196) | Controlled clinical trial | Dynamic lighting system | Lighting intensity | 3 |
| [23] | Intermediate acuity unit | Nurses (n = 33), patients (n = 21) | Non-randomized, controlled interventional trial | Blue-depleted lighting at night | Lighting spectrum, intensity | 2 | |
| Depression | [25] | Patients’ room | Cardiology ward patients (n = 196) | Controlled clinical trial | Dynamic lighting system | Lighting intensity | 3 |
| [23] | Intermediate acuity unit | Nurses (n = 33), patients (n = 21) | Non-randomized, controlled interventional trial | Blue-depleted lighting at night | Lighting spectrum, intensity | 2 | |
| [55] | Patients’ room | Psychiatric patients (n = 74) | Randomized controlled groups | Adjustable lighting | Lighting spectrum | 2 |
4.4. Patient-Related Health Outcomes
| Category | Ref. | Setting | Participants | Study Design | Intervention | Mediating Factor | Level |
|---|---|---|---|---|---|---|---|
| Physical Activity | [27] | CCU | Patients (n = 748) | Retrospective cohort study | Dynamic lighting system | CCT | 3 |
| Length of Hospitalization | [26] | Nurse station | Patients (n = 1073) | Field survey | Blue-enriched lighting system | CCT | 3 |
| [27] | CCU | Patient (n = 748) | Retrospective cohort study | Dynamic lighting system | CCT | 2 | |
| [58] | Patient’s room | Depressed patients (n = 30) | Pilot study, observations | Dynamic lighting system | CCT, light intensity | 3 | |
| Delirium | [27] | CCU | Patient (n = 748) | Retrospective cohort study | Dynamic lighting system | CCT | 3 |
| Psychotropic Medication | [32] | Nursing home | Nursing home residents (58 women, 19 men) | Randomized controlled trial | Dynamic lighting system | Light intensity, timing | 2 |
| [61] | Intensive care unit | Patients (n = 183) | Retrospective cohort study | Dynamic lighting system | CCT | 2 | |
| [58] | Patient’s room | Depressed patients (n = 30) | Pilot study, observations | Dynamic lighting system | CCT, light intensity | 2 | |
| Alertness | [32] | Nursing home | Nursing home residents (58 women, 19 men) | Randomized controlled trial | Dynamic lighting system | Light intensity, timing | 2 |
| Pain | [60] | Patients’ room | Medical inpa-tients (women = 23; men = 17) | Correlational study or non-experimental study | Dynamic lighting system | Light intensity | 2 |
4.5. Nurse-Related Health Outcomes
| Category | Ref. | Setting | Participants | Study Design | Intervention | Mediating Factor | Level |
|---|---|---|---|---|---|---|---|
| Medical Errors | [6] | Hospital | Nonpatient (n = 12) | Retrospective cohort study | Dynamic lighting system | Blue-depleted light | 2 |
| Environmental Perception | [62] | Nurse home | Patients (n = 1073) | Case study, observation | Dynamic lighting system | Controlling strategy (intelligent, personalized) | 3 |
| [28] | Nursing home | Staff members (n = 42) | Observation | Tunable lighting systems | CCT, controlling strategy | 2 | |
| Satisfaction | [23] | Intermediate acuity unit | Nurses (n = 33), patients (n= 21) | Non-randomized, controlled interventional trial | Blue-depleted lighting at night | Lighting spectrum, intensity | 2 |
| [65] | Pharmacy | Employee (n = 8) | Case study, observation | Dynamic lighting system | Lighting intensity, CCT | 3 | |
| [28] | Nursing home | Staff members (n = 42) | Observation | Tunable lighting systems | CCT, controlling strategy | 2 |
4.6. Environmental and Psychosocial Outcomes
5. Simulation-Based Studies
| Ref. | Research Setting | Evaluation Metrics | Studies Parameters | Software | Architectural Elements |
|---|---|---|---|---|---|
| [72] | Virtual patient room | Circadian stimulus | Lighting intensity, timing, spectrum | Statistical analysis, DAYSIM, field measurements | Window orientation, WWR, glazing material, shading device |
| [73] | Virtual patient room | Circadian stimulus | Lighting intensity | Statistical analysis, Radiance, field measurements | WWR, glazing materials, latitude |
| [75] | Nursing home | Circadian stimulus, Photopic Lux, EML, CS, plane Lux, M/P | Lighting intensity, timing, spectrum | ALFA | Location, timing, sky condition, materials, luminaires, furniture position |
| [74] | Patient room | EML, photopic lux | Lighting intensity, timing | Statistical analysis, Honeybee, Rhino, field measurements | Materials, orientation, WWR |
| [76] | Patient room | Melanopic EDI, melanopic DER, climate-based metrics | Lighting intensity, timing | ALFA | WWR, orientation, location, sky conditions, materials |
6. Discussion
7. Conclusions and Future Directions
8. Executive Summary
Author Contributions
Funding
Conflicts of Interest
References
- Fonken, L.K.; Nelson, R.J. The Effects of Light at Night on Circadian Clocks and Metabolism. Endocr. Rev. 2014, 35, 648–670. [Google Scholar] [CrossRef]
- Bedrosian, T.A.; Fonken, L.K.; Nelson, R.J. Endocrine Effects of Circadian Disruption. Annu. Rev. Physiol. 2016, 78, 109–131. [Google Scholar] [CrossRef]
- Kyba, C.C.M.; Mohar, A.; Posch, T. How Bright Is Moonlight? Astron. Geophys. 2017, 58, 1.31–1.32. [Google Scholar] [CrossRef]
- Kuijsters, A.; Redi, J.; de Ruyter, B.; Heynderickx, I. Lighting to Make You Feel Better: Improving the Mood of Elderly People with Affective Ambiences. PLoS ONE 2015, 10, e0132732. [Google Scholar] [CrossRef]
- Weil, Z.M.; Fonken, L.K.; Walker, W.H.; Bumgarner, J.R.; Liu, J.A.; Melendez-Fernandez, O.H.; Zhang, N.; DeVries, A.C.; Nelson, R.J. Dim Light at Night Exacerbates Stroke Outcome. Eur. J. Neurosci. 2020, 52, 4139–4146. [Google Scholar] [CrossRef]
- Vethe, D.; Scott, J.; Engstrøm, M.; Salvesen, Ø.; Sand, T.; Olsen, A.; Morken, G.; Heglum, H.S.; Kjørstad, K.; Faaland, P.M.; et al. The Evening Light Environment in Hospitals Can Be Designed to Produce Less Disruptive Effects on the Circadian System and Improve Sleep. Sleep 2021, 44, zsaa194. [Google Scholar] [CrossRef]
- Figueiro, M.G.; Sahin, L.; Wood, B.; Plitnick, B. Light at Night and Measures of Alertness and Performance. Biol. Res. Nurs. 2016, 18, 90–100. [Google Scholar] [CrossRef]
- Navara, K.J.; Nelson, R.J. The Dark Side of Light at Night: Physiological, Epidemiological, and Ecological Consequences. J. Pineal Res. 2007, 43, 215–224. [Google Scholar] [CrossRef]
- Hattar, S.; Liao, H.W.; Takao, M.; Berson, D.M.; Yau, K.W. Melanopsin-Containing Retinal Ganglion Cells: Architecture, Projections, and Intrinsic Photosensitivity. Science 2002, 295, 1065–1070. [Google Scholar] [CrossRef]
- Nelson, R.J.; Bumgarner, J.R.; Liu, J.A.; Love, J.A.; Meléndez-Fernández, O.H.; Becker-Krail, D.D.; Walker, W.H.; Walton, J.C.; DeVries, A.C.; Prendergast, B.J. Time of Day as a Critical Variable in Biology. BMC Biol. 2022, 20, 142. [Google Scholar] [CrossRef]
- Houser, K.W.; Esposito, T. Human-Centric Lighting: Foundational Considerations and a Five-Step Design Process. Front. Neurol. 2021, 12, 630553. [Google Scholar] [CrossRef]
- Vetter, C.; Pattison, P.M.; Houser, K.; Herf, M.; Phillips, A.J.K.; Wright, K.P.; Skene, D.J.; Brainard, G.C.; Boivin, D.B.; Glickman, G. A Review of Human Physiological Responses to Light: Implications for the Development of Integrative Lighting Solutions. LEUKOS 2022, 18, 387–414. [Google Scholar] [CrossRef]
- Rea, M.S.; Nagare, R.; Figueiro, M.G. Modeling Circadian Phototransduction: Retinal Neurophysiology and Neuroanatomy. Front. Neurosci. 2021, 14, 615305. [Google Scholar] [CrossRef]
- Saey, T.H. Seeing the Light: Transforming Nerve Cells into Photoreceptors to Restore Vision. Sci. News 2015, 187, 22–26. [Google Scholar] [CrossRef]
- SOLEMMA. Adaptive Lighting for Alertness A New Circadian Lighting Design Software. Available online: www.solemma.com/alfa (accessed on 26 March 2024).
- Chellappa, S.L.; Steiner, R.; Blattner, P.; Oelhafen, P.; Götz, T.; Cajochen, C. Non-Visual Effects of Light on Melatonin, Alertness and Cognitive Performance: Can Blue-Enriched Light Keep Us Alert? PLoS ONE 2011, 6, e16429. [Google Scholar] [CrossRef]
- Moore-Ede, M.; Heitmann, A.; Guttkuhn, R. Circadian Potency Spectrum with Extended Exposure to Polychromatic White LED Light under Workplace Conditions. J. Biol. Rhythm. 2020, 35, 405–415. [Google Scholar] [CrossRef]
- Wang, R.; Yang, B.; Yao, Y.; Bloom, M.S.; Feng, Z.; Yuan, Y.; Zhang, J.; Liu, P.; Wu, W.; Lu, Y.; et al. Residential Greenness, Air Pollution and Psychological Well-Being among Urban Residents in Guangzhou, China. Sci. Total Environ. 2020, 711, 134843. [Google Scholar] [CrossRef]
- Zolfaghari, Z.; R.Jones, J. Study of the Effect of Light Emitting Diode (LED) on the Optimum Window-to-Wall Ratio and Whole-Building Energy Consumption in Open Offices. Ph.D. Dissertation, Virginia Polytechnic Institute and State University, Blacksburg, Virginia, 2022. [Google Scholar] [CrossRef]
- Falchi, F.; Cinzano, P.; Duriscoe, D.; Kyba, C.C.M.; Elvidge, C.D.; Baugh, K.; Portnov, B.A.; Rybnikova, N.A.; Furgoni, R. The New World Atlas of Artificial Night Sky Brightness. Sci. Adv. 2016, 2, e1600377. [Google Scholar] [CrossRef] [PubMed]
- Kyba, C.C.M.; Kuester, T.; Sánchez de Miguel, A.; Baugh, K.; Jechow, A.; Hölker, F.; Bennie, J.; Elvidge, C.D.; Gaston, K.J.; Guanter, L. Artificially Lit Surface of Earth at Night Increasing in Radiance and Extent. Sci. Adv. 2017, 3, e1701528. [Google Scholar] [CrossRef] [PubMed]
- Hansen, J. Night Shift Work and Risk of Breast Cancer. Curr. Environ. Health Rep. 2017, 4, 325–339. [Google Scholar] [CrossRef]
- Albala, L.; Bober, T.; Hale, G.; Warfield, B.; Collins, M.L.; Merritt, Z.; Steimetz, E.; Nadler, S.; Lev, Y.; Hanifin, J. Effect on Nurse and Patient Experience: Overnight Use of Blue-Depleted Illumination. BMJ Open Qual. 2019, 8, e000692. [Google Scholar] [CrossRef] [PubMed]
- Hadi, K.; DuBose, J.R.; Ryherd, E. Lighting and Nurses at Medical–Surgical Units. HERD: Health Environ. Res. Des. J. 2016, 9, 17–30. [Google Scholar] [CrossRef] [PubMed]
- Giménez, M.C.; Geerdinck, L.M.; Versteylen, M.; Leffers, P.; Meekes, G.J.B.M.; Herremans, H.; de Ruyter, B.; Bikker, J.W.; Kuijpers, P.M.J.C.; Schlangen, L.J.M. Patient Room Lighting Influences on Sleep, Appraisal and Mood in Hospitalized People. J. Sleep Res. 2017, 26, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Broman, A.T.; Priest, G.; Landrigan, C.P.; Rahman, S.A.; Lockley, S.W. The Effect of Blue-Enriched Lighting on Medical Error Rate in a University Hospital ICU. Jt. Comm. J. Qual. Patient Saf. 2021, 47, 165–175. [Google Scholar] [CrossRef]
- Pustjens, T.; Schoutens, A.M.; Janssen, L.; Heesen, W.F. Effect of Dynamic Light at the Coronary Care Unit on the Length of Hospital Stay and Development of Delirium: A Retrospective Cohort Study. J. Geriatr. Cardiol. 2018, 15, 567–573. [Google Scholar] [PubMed]
- Schledermann, K.M.; Hansen, T.S.; Bjørner, T. Perceived Visual Comfort and Usefulness of a Circadian Lighting System Implemented at a Nursing Home. Multimed. Tools Appl. 2023, 82, 5253–5269. [Google Scholar] [CrossRef]
- Amirazar, A.; Azarbayjani, M.; Im, O.-K.; Zarrabi, H.; Ashrafi, R.; Cox, R.; Johnson, A. Assessing the Circadian Potential of an Office Building in the Southeastern US. In Proceedings of the 2018 Symposium on Simulation for Architecture and Urban Design—SimAUD, Delft, The Netherlands, 4–7 June 2018. [Google Scholar]
- Griepentrog, J.E.; Labiner, H.E.; Gunn, S.R.; Rosengart, M.R. Bright Environmental Light Improves the Sleepiness of Nightshift ICU Nurses. Crit. Care 2018, 22, 295. [Google Scholar] [CrossRef] [PubMed]
- Lledó, R. Human Centric Lighting, a New Reality in Healthcare Environments; Springer International Publishing: Berlin/Heidelberg, Germany, 2019; pp. 23–26. [Google Scholar] [CrossRef]
- Ancoli-Israel, S.; Martin, J.L.; Kripke, D.F.; Marler, M.; Klauber, M.R. Effect of Light Treatment on Sleep and Circadian Rhythms in Demented Nursing Home Patients. J. Am. Geriatr. Soc. 2002, 50, 282–289. [Google Scholar] [CrossRef]
- Lowry, G. A Comparison of Metrics Proposed for Circadian Lighting and the Criterion Adopted in the WELL Building Standard; CIBSE Technical Symposium: London, UK, 2018; Volume 10. [Google Scholar]
- Aubé, M.; Roby, J.; Kocifaj, M. Evaluating Potential Spectral Impacts of Various Artificial Lights on Melatonin Suppression, Photosynthesis, and Star Visibility. PLoS ONE 2013, 8, e67798. [Google Scholar] [CrossRef] [PubMed]
- Sano, I.; Tanito, M.; Okuno, T.; Ishiba, Y.; Ohira, A. Estimation of the Melatonin Suppression Index through Clear and Yellow-Tinted Intraocular Lenses. Jpn. J. Ophthalmol. 2014, 58, 320–326. [Google Scholar] [CrossRef]
- Truong, W.; Zandi, B.; Trinh, V.Q.; Khanh, T.Q. Circadian Metric—Computation of Circadian Stimulus Using Illuminance, Correlated Colour Temperature and Colour Rendering Index. Build. Environ. 2020, 184, 107146. [Google Scholar] [CrossRef]
- Rea, M.S.; Nagare, R.; Figueiro, M.G. Corrigendum: Modeling Circadian Phototransduction: Quantitative Predictions of Psychophysical Data (Front. Neurosci., (2021), 15, (615322), 10.3389/Fnins.2021.615322). Front. Neurosci. 2022, 16, 849800. [Google Scholar] [CrossRef]
- Erdem, T.; Demir, H.V. Color-Enrichment Semiconductor Nanocrystals for Biorhythm-Friendly Backlighting. Z. Fur Phys. Chem. 2018, 232, 1457–1468. [Google Scholar] [CrossRef]
- Lucas, R.J.; Peirson, S.N.; Berson, D.M.; Brown, T.M.; Cooper, H.M.; Czeisler, C.A.; Figueiro, M.G.; Gamlin, P.D.; Lockley, S.W.; O’Hagan, J.B.; et al. Measuring and Using Light in the Melanopsin Age. Trends Neurosci. 2014, 37, 1–9. [Google Scholar] [CrossRef]
- Brown, T.M. Melanopic Illuminance Defines the Magnitude of Human Circadian Light Responses under a Wide Range of Conditions. J. Pineal Res. 2020, 69, e12655. [Google Scholar] [CrossRef]
- Shin, J.; Meridew, C.; Athey, A.; Killgore, W.; Gehrels, J.A. Basic and Translational Sleep Science. Sleep 2019, 41, A74. [Google Scholar]
- Oh, J.H.; Yang, S.J.; Do, Y.R. Healthy, Natural, Efficient and Tunable Lighting: Four-Package White LEDs for Optimizing the Circadian Effect, Color Quality and Vision Performance. Light Sci. Appl. 2014, 3, e141. [Google Scholar] [CrossRef]
- Esposito, T.; Houser, K. Correlated Color Temperature Is Not a Suitable Proxy for the Biological Potency of Light. Sci. Rep. 2022, 12, 20223. [Google Scholar] [CrossRef]
- Moore-ede, M.; Heitmann, A. Circadian Potency Spectrum in Light-Adapted Humans. J. Cell Sci. Ther. 2022, 13, 1–6. [Google Scholar] [CrossRef]
- Liu, T. Lighting Evaluation and Design for the Stockholm Metro System Based on Current Models for Non- Visual Responses Lighting Evaluation and Design for the Stockholm Metro System. Master’s Thesis, KTH Royal Institute Of Technology School Of Architecture and the Built Environment, Stockholm, Sweden, 2020. Available online: http://kth.divaportal.org/smash/get/diva2:1463572/FULLTEXT01.pdf (accessed on 26 March 2024).
- Kolberg, E.; Pallesen, S.; Hjetland, G.J.; Nordhus, I.H.; Thun, E.; Flo-Groeneboom, E. Insufficient Melanopic Equivalent Daylight Illuminance in Nursing Home Dementia Units across Seasons and Gaze Directions. Light. Res. Technol. 2022, 54, 163–177. [Google Scholar] [CrossRef]
- Acosta, I.; Campano, M.Á.; Leslie, R.; Radetsky, L. Daylighting Design for Healthy Environments: Analysis of Educational Spaces for Optimal Circadian Stimulus. Sol. Energy 2019, 193, 584–596. [Google Scholar] [CrossRef]
- Reinhart, C.F.; Mardaljevic, J.; Rogers, Z. Dynamic Daylight Performance Metrics for Sustainable Building Design. LEUKOS 2006, 3, 7–31. [Google Scholar] [CrossRef]
- Booth, A.; Papaioannou, D.; Sutton, A. Systematic Approaches to the Literature. Syst. Approaches A Succesful Lit. Rev. 2012. ISBN-13: 978-0857021359. [Google Scholar]
- Pagé, G.; Lavoie, K. Entre Soutien et Contrôle: La Parole Des Actrices et Des Acteurs Sociaux Sur Les Pratiques d’accompagnement Des Familles En Situation de Vulnérabilité. Serv. Soc. 2021, 67, 1. [Google Scholar] [CrossRef]
- van Duijnhoven, J.; Aarts, M.P.J.; Aries, M.B.C.; Rosemann, A.L.P.; Kort, H.S.M. Systematic Review on the Interaction between Office Light Conditions and Occupational Health: Elucidating Gaps and Methodological Issues. Indoor Built Environ. 2019, 28, 152–174. [Google Scholar] [CrossRef]
- Jiang, S. Positive Distractions and Play in the Public Spaces of Pediatric Healthcare Environments: A Literature Review. HERD Health Environ. Res. Des. J. 2020, 13, 171–197. [Google Scholar] [CrossRef] [PubMed]
- Stichler, J.F. Weighing the Evidence. HERD Health Environ. Res. Des. J. 2010, 3, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Marquardt, G.; Motzek, T. How to Rate the Quality of a Research Paper: Introducing a Helpful Algorithm for Architects and Designers. HERD Health Environ. Res. Des. J. 2013, 6, 119–127. [Google Scholar] [CrossRef]
- Okkels, N.; Jensen, L.G.; Skovshoved, L.C.; Arendt, R.; Blicher, A.B.; Vieta, E.; Straszek, S. Lighting as an Aid for Recovery in Hospitalized Psychiatric Patients: A Randomized Controlled Effectiveness Trial. Nord. J. Psychiatry 2020, 74, 105–114. [Google Scholar] [CrossRef]
- Engwall, M.; Fridh, I.; Johansson, L.; Bergbom, I.; Lindahl, B. Lighting, Sleep and Circadian Rhythm: An Intervention Study in the Intensive Care Unit. Intensive Crit. Care Nurs. 2015, 31, 325–335. [Google Scholar] [CrossRef]
- Gleason, J.D.; Oishi, M.; Simkulet, M.; Tuzikas, A.; Brown, L.K.; Brueck, S.R.J.; Karlicek, R.F. A Novel Smart Lighting Clinical Testbed. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju Island, Republic of Korea, 11–15 July 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 4317–4320. [Google Scholar] [CrossRef]
- Canazei, M.; Weninger, J.; Pohl, W.; Marksteiner, J.; Weiss, E.M. Effects of Dynamic Bedroom Lighting on Measures of Sleep and Circadian Rest-Activity Rhythm in Inpatients with Major Depressive Disorder. Sci. Rep. 2022, 12, 6137. [Google Scholar] [CrossRef] [PubMed]
- Soltic, S.; Chalmers, A. Optimization of LED Lighting for Clinical Settings. J. Healthc. Eng. 2019, 2019, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bernhofer, E.I.; Higgins, P.A.; Daly, B.J.; Burant, C.J.; Hornick, T.R. Hospital Lighting and Its Association with Sleep, Mood and Pain in Medical Inpatients. J. Adv. Nurs. 2014, 70, 1164–1173. [Google Scholar] [CrossRef] [PubMed]
- Estrup, S.; Kjer, C.K.W.; Poulsen, L.M.; Gøgenur, I.; Mathiesen, O. Delirium and Effect of Circadian Light in the Intensive Care Unit: A Retrospective Cohort Study. Acta Anaesthesiol. Scand. 2018, 62, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Flyvholm, A.; Sen, S.; Xylakis, E.; Nielsen, L.; Triantafyllidis, G.; Andresen, L.; Pedersen, M.M. A Personalised and Adaptive Intelligent System to Adjust Circadian Lighting for Elderly Housing. In Proceedings of the 15th International Symposium on Ambient Intelligence and Embedded Systems, Heraklion, Greece, 21–23 September 2016. [Google Scholar]
- Pohl, W.; Canazei, M.; Neier, L.M.; Tanzer, K.; Weninger, J. Health Effects of Biodynamic Ligting in Clinics. In Proceedings of the LUX EUROPA, European Lighting Conference, Ljubljana, Slovenia, 18–20 September 2017. [Google Scholar]
- van Lieshout-van Dal, E.; Snaphaan, L.; Bongers, I. Biodynamic Lighting Effects on the Sleep Pattern of People with Dementia. Build. Environ. 2019, 150, 245–253. [Google Scholar] [CrossRef]
- McCunn, L.J.; Wright, J. Hospital Employees’ Perceptions of Circadian Lighting: A Pharmacy Department Case Study. J. Facil. Manag. 2019, 17, 422–437. [Google Scholar] [CrossRef]
- Scott, J.; Langsrud, K.; Goulding, I.R.; Kallestad, H. Let There Be Blue-Depleted Light: In-Patient Dark Therapy, Circadian Rhythms and Length of Stay. BJPsych Adv. 2021, 27, 73–84. [Google Scholar] [CrossRef]
- Rea, M.S.; Figueiro, M.G.; Bierman, A.; Bullough, J.D. Circadian Light. J. Circadian Rhythm. 2010, 8, 2. [Google Scholar] [CrossRef]
- Wilkerson, A.; Safranek, S.; Irvin, L.; Tredinnick, L. Lighting System Control Data to Improve Design and Operation: Tunable Lighting System Data from NICU Patient Rooms. LEUKOS 2023, 19, 94–109. [Google Scholar] [CrossRef]
- Grissinger, M. An Exhausted Workforce Increases the Risk of Errors. P T A Peer-Rev. J. Formul. Manag. 2009, 34, 120–123. [Google Scholar]
- Studer, P.; Brucker, J.M.; Haag, C.; Van Doren, J.; Moll, G.H.; Heinrich, H.; Kratz, O. Effects of Blue- and Red-Enriched Light on Attention and Sleep in Typically Developing Adolescents. Physiol. Behav. 2019, 199, 11–19. [Google Scholar] [CrossRef]
- Graves, E.; Davis, R.G.; DuBose, J.; Campiglia, G.C.; Wilkerson, A.; Zimring, C. Lighting the Patient Room of the Future: Evaluating Different Lighting Conditions for Performing Typical Nursing Tasks. HERD Health Environ. Res. Des. J. 2021, 14, 234–253. [Google Scholar] [CrossRef] [PubMed]
- Pechacek, C.S.; Andersen, M.; Lockley, S.W. Preliminary Method for Prospective Analysis of the Circadian Efficacy of (Day)Light with Applications to Healthcare Architecture. LEUKOS—J. Illum. Eng. Soc. N. Am. 2008, 5, 1–26. [Google Scholar] [CrossRef]
- Acosta, I.; Leslie, R.; Figueiro, M. Analysis of Circadian Stimulus Allowed by Daylighting in Hospital Rooms. Light. Res. Technol. 2017, 49, 49–61. [Google Scholar] [CrossRef]
- Song, H.; Jiang, W.; Cui, P. A Study on Nonvisual Effects of Natural Light Environment in a Maternity Ward of a Hospital in Cold Area. BioMed Res. Int. 2022, 2022, 8608892. [Google Scholar] [CrossRef]
- Carmon, D.; Altomonte, S. Lighting for Circadian Well-Being: A Simulation-Based Workflow for the Visual and Non-Visual Lighting Design of a Nursing Home. In Proceedings of the 17th IBPSA Conference, Bruges, Belgium, 1–3 September 2021. [Google Scholar]
- Englezou, M.; Michael, A. Evaluation of Visual and Non-Visual Effects of Daylighting in Healthcare Patient Rooms Using Climate-Based Daylight Metrics and Melanopic Metrics. E3S Web Conf. 2022, 362, 01003. [Google Scholar] [CrossRef]
- Brown, T.M.; Brainard, G.C.; Cajochen, C.; Czeisler, C.A.; Hanifin, J.P.; Lockley, S.W.; Lucas, R.J.; Münch, M.; O’Hagan, J.B.; Peirson, S.N.; et al. Recommendations for Daytime, Evening, and Nighttime Indoor Light Exposure to Best Support Physiology, Sleep, and Wakefulness in Healthy Adults. PLoS Biol. 2022, 20, e3001571. [Google Scholar] [CrossRef]
- Illuminating Engineering Society. ANSI/IES RP-29-22, Recommended Practice: Lighting Hospital and Healthcare Facilities; IES: New York, NY, USA, 2022. [Google Scholar]



| An Architectural Solution to A Biological Problem: A Systematic Review of Lighting Designs That Promote Proper Circadian Alignment in Healthcare Environments | ||||
|---|---|---|---|---|
| Introduction | Methodology | Results | Discussion | |
| Circadian Clock and Rhythms | Lighting and Circadian Rhythms | Eligibility Criteria | (1) Interventional Human Subject | Architectural Solutions for Circadian Alignment Design Guidelines for Healthcare Environments |
| Information Sources | a: Research Methods (experimental studies, quasi-experimental studies, qualitative study/case study) b: Health Outcomes (sleep-related outcomes, mood and psychological outcomes, patient-related health outcomes, nurse-related health outcomes, environmental and psychological outcomes) | ||
| Search Strategy and Study Selection | ||||
| Screening | ||||
| Level of Evidence | (2) Simulation-Based Studies | |||
| Metric | Year | Calculation Method | Architectural Application | Evaluation Methods/Threshold | Ref. |
|---|---|---|---|---|---|
| Melatonin Suppression Index (MSI) | 2001 | Comparing the suppression of melatonin in response to a light source to a reference light source | MSI is related to two other indices: the Induced Photosynthesis Index (IPI) and Star Light Index (SLI) | A higher MSI indicates a greater degree of melatonin suppression. | [33,34,35] |
| Circadian Stimulus (CS) | 2010 | Considering spectral distribution of light source and human eye’s sensitivity at different wavelengths | LEED and WELL Building standards Architectural organizations: IALD, IES | Measured on a scale from 0.1 to 0.7, with higher values representing greater circadian impact. Threshold of 0.3 to 0.4 for maintaining entrainment and promoting healthy circadian rhythms in daytime environments. | [13,36,37] |
| Circadian Effectiveness Factor (CEF) | 2011 | Taking into account both the circadian impact of a light source and the energy efficiency of the light source. Calculating by taking the ratio of the circadian action of a light source to the amount of light energy produced by the light source. | Comparing different lighting systems based on their ability to promote the health and well-being of the occupants while considering energy efficiency | A higher CEF indicates a greater circadian impact on health and well-being. | [35,38] |
| Equivalent Melanopic Lux (EML) | 2013 | Considering melanopsin sensitivity of the human eye by measuring biological influences of light on humans | WELL Building Standard requirement | Measured 1.2 m above floor, assumed to be eye-level for a desk-based worker. At least 200 EML to ensure occupants’ circadian rhythm is adequately supported. | [33,39,40] |
| Circadian Action Factor (CAF) | 2013 | Calculated by taking the ratio of the circadian action of a light source to the circadian action of a reference light source, typically a 3000 K warm-white LED | Allowing them to compare different lighting systems | Higher CAF values are associated with increased alertness and better health outcomes. | [33,35,41,42] |
| Circadian Potency Spectrum (CPS) | 2013 | Consistent results of melatonin levels induced by the light stimulus for extended exposure time to eyes compared to the MSF model. Calculated by taking the ratio of a light source’s spectral power distribution to a reference light source (typically a 3000 K warm-white LED)). | Allowing for comparing different lighting systems | Compared with broad-spectrum light (white light), with a peak at 612 nm, the CPS model is more effective in suppressing melatonin levels and regulating circadian timing. | [17,43,44] |
| Melanopic Equivalent Daylight Illuminance (m-EDI) | 2015 | Considering circadian impact of daylight on the human eye by multiplying the illuminance of a light source by a melanopsin sensitivity function | International Commission on Illumination (CIE) | Melanopic ratio of m-EDI is slightly higher than EML, suggesting that some of the lower recommendations of the WELL Standard may need to be adjusted | [33,40,43,45,46] |
| Circadian Stimulus Weighting Function (CSWF) | 2019 | Takes into account both the circadian effect and the energy efficiency of a light source Calculated by taking the ratio of the circadian action of a light source to the amount of light energy produced by the same source | Allowing them to compare different lighting systems | A higher CSWF indicates a greater circadian impact on health and well-being. | [35,38] |
| Circadian Stimulus Autonomy (CSA) | 2019 | A measure of how many hours throughout the year there is sufficient illumination to promote circadian stimulation (CS) | Identifies effectiveness of window designs and lighting systems for promoting circadian stimulation | Early morning interval should be one or two hours. | [47,48] |
| # | Study Types | Ref. |
|---|---|---|
| 1 | Experimental Studies | |
| • Randomized controlled trial | [25,32,55] | |
| • Intervention study | [26,56] | |
| • Controlled clinical trial | [57] | |
| • Experimental measurements | [57,59] | |
| 2 | Quasi-Experimental Study | |
| • Clinical test bed | [57] | |
| 3 | Observational Study | |
| • Observation | [6,57,58,62,63,64,65,66] | |
| • Field survey | [26,32,59,63] | |
| • Correlational study or non-experimental study | [60] | |
| • Retrospective cohort study | [27,61] | |
| 4 | Qualitative Study/Case Study | |
| • Case study | [62,65] | |
| • Pilot study | [23,58,64] | |
| Category | Ref. | Setting | Participants | Study Design | Intervention | Mediating Factor | Level |
|---|---|---|---|---|---|---|---|
| User Preference | [59] | Patient room | Patient (n = 12) | Field survey, experimental measurements | Dynamic lighting system | Spectral power distribution (SPD) | 2 |
| [71] | Patient room | Patients (n = 45) | Field survey | Dynamic lighting system | CCT, lighting intensity | 3 | |
| Psychosocial Variables (affective organizational commitment, perceived productivity) | [56] | Intensive care units | Patients (n = 19) | Descriptive correlational studies | Cycled lighting environment | Lighting intensity, Timing, wavelength | 3 |
| [58] | Patient’s room | Depressed patients (n = 30) | Pilot study, observations | Dynamic lighting system | CCT, light intensity | 2 | |
| Experience | [65] | Pharmacy | Employee (n = 8) | Case study, observation | Dynamic lighting system | Lighting intensity, CCT | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hosseini, S.N.; Walton, J.C.; SheikhAnsari, I.; Kreidler, N.; Nelson, R.J. An Architectural Solution to a Biological Problem: A Systematic Review of Lighting Designs in Healthcare Environments. Appl. Sci. 2024, 14, 2945. https://0-doi-org.brum.beds.ac.uk/10.3390/app14072945
Hosseini SN, Walton JC, SheikhAnsari I, Kreidler N, Nelson RJ. An Architectural Solution to a Biological Problem: A Systematic Review of Lighting Designs in Healthcare Environments. Applied Sciences. 2024; 14(7):2945. https://0-doi-org.brum.beds.ac.uk/10.3390/app14072945
Chicago/Turabian StyleHosseini, Seyedeh Nazli, James C. Walton, Iman SheikhAnsari, Nicole Kreidler, and Randy J. Nelson. 2024. "An Architectural Solution to a Biological Problem: A Systematic Review of Lighting Designs in Healthcare Environments" Applied Sciences 14, no. 7: 2945. https://0-doi-org.brum.beds.ac.uk/10.3390/app14072945