
Burnout and Quality of Work Life among Physicians during Internships in Public Hospitals in Thailand



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures
2.2.1. Burnout
2.2.2. Quality of Work Life
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
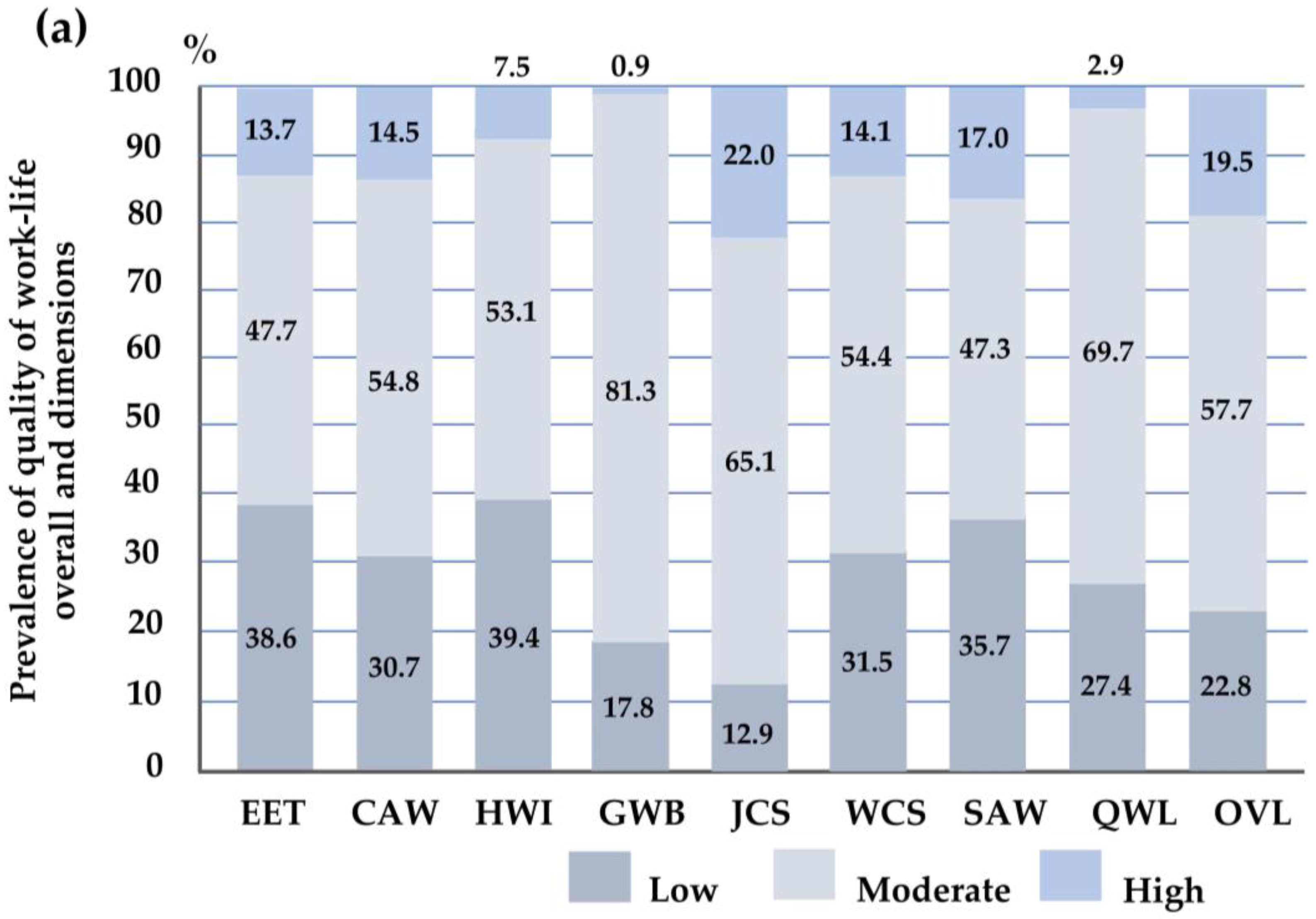
3.1. Descriptive Results on Quality-of-Work-Life Characteristics
3.2. Quality of Work Life among Intern Physicians
3.3. Burnout Subscales among Intern Physicians
3.4. Associations between Burnout and Quality of Work Life among Intern Physicians
3.4.1. Model 1: Associations between Burnout Subscales and Overall QWL

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| QWL (n = 227) | High Emotional Exhaustion (EE) | High Depersonalization (DP) | Low Personal Accomplishment (PA) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| aOR | SE | 95% CI | p | aOR | SE | 95% CI | p | aOR | SE | 95% CI | p | |
| Low QWL a | 1.04 | 0.52 | 0.38 to 2.79 | 0.945 | 2.08 | 0.77 | 1.01 to 4.31 | 0.048 * | 2.74 | 0.94 | 1.40 to 5.39 | 0.003 * |
| Low OVL a | 1.17 | 0.63 | 0.41 to 3.34 | 0.763 | 1.31 | 0.50 | 0.62 to 2.76 | 0.483 | 2.95 | 1.12 | 1.40 to 6.23 | 0.005 * |
3.4.2. Model 2: Associations between Burnout Subscales and QWL Dimensions, Including EET, GWB, and WCS
| QWL Dimensions (n = 227) | High Emotional Exhaustion (EE) | High Depersonalization (DP) | Low Personal Accomplishment (PA) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| aOR | SE | 95% CI | p | aOR | SE | 95% CI | p | aOR | SE | 95% CI | p | |
| Low EET a | 1.71 | 0.78 | 0.70 to 4.17 | 0.238 | 1.37 | 0.44 | 0.73 to 2.56 | 0.327 | 3.24 | 0.99 | 1.78 to 5.88 | <0.001 ** |
| Low GWB a | 2.82 | 1.43 | 1.04 to 7.64 | 0.042 * | 1.81 | 0.58 | 0.97 to 3.38 | 0.062 | 2.30 | 0.68 | 1.28 to 4.12 | 0.005 * |
| Low WCS a | 1.36 | 0.67 | 0.52 to 3.58 | 0.534 | 2.03 | 0.70 | 1.04 to 3.99 | 0.039 * | 2.32 | 0.73 | 1.25 to 4.31 | 0.008 * |
3.4.3. Model 3: Associations between Burnout Subscales and QWL Dimensions Including HWI, SAW, CAW, and JCS
| QWL Dimensions (n = 227) | High Emotional Exhaustion (EE) | High Depersonalization (DP) | Low Personal Accomplishment (PA) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| aOR | SE | p | 95% CI | aOR | SE | p | 95% CI | aOR | SE | p | 95% CI | |
| Low HWI a | 2.32 | 1.06 | 0.067 | 0.94 to 5.69 | 1.03 | 0.31 | 0.930 | 0.56 to 1.87 | 1.01 | 0.29 | 0.974 | 0.58 to 1.76 |
| Low SAW a | 8.56 | 5.96 | 0.002 * | 2.19 to 33.51 | 2.12 | 0.69 | 0.021 * | 1.12 to 4.02 | 0.90 | 0.27 | 0.721 | 0.50 to 1.61 |
| Low CAW a | 1.35 | 0.65 | 0.537 | 0.52 to 3.46 | 1.26 | 0.43 | 0.499 | 0.65 to 2.45 | 3.64 | 1.23 | <0.001 ** | 1.88 to 7.05 |
| Low JCS a | 0.31 | 0.19 | 0.059 | 0.09 to 1.04 | 1.97 | 1.12 | 0.232 | 0.65 to 5.97 | 2.72 | 1.49 | 0.066 | 0.94 to 7.93 |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leitão, J.; Pereira, D.; Gonçalves, Â. Quality of Work Life and Organizational Performance: Workers’ Feelings of Contributing, or Not, to the Organization’s Productivity. Int. J. Environ. Res. Public Health 2019, 16, 3803. [Google Scholar] [CrossRef] [PubMed]
- Krueger, P.; Brazil, K.; Lohfeld, L.; Edward, H.G.; Lewis, D.; Tjam, E. Organization specific predictors of job satisfaction: Findings from a Canadian multi-site quality of work life cross-sectional survey. BMC Health Serv. Res. 2002, 2, 6. [Google Scholar] [CrossRef] [PubMed]
- Mosadeghrad, A.M.; Ferlie, E.; Rosenberg, D. A study of relationship between job stress, quality of working life and turnover intention among hospital employees. Health Serv. Manag. Res. 2011, 24, 170–181. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, M.; Zakerian, A.; Akbarzade, A.; Dinarvand, N.; Ghaljahi, M.; Poursadeghiyan, M.; Ebrahimi, M.H. Investigation of the Relationship between Work Ability and Work-related Quality of Life in Nurses. Iran J. Public Health 2017, 46, 1404–1412. [Google Scholar] [PubMed]
- Rastegari, M.; Khani, A.; Ghalriz, P.; Eslamian, J. Evaluation of quality of working life and its association with job performance of the nurses. Iran J. Nurs. Midwifery Res. 2010, 15, 224–228. [Google Scholar]
- de Jong, M.; de Boer, A.G.; Tamminga, S.J.; Frings-Dresen, M.H. Quality of Working Life Issues of Employees with a Chronic Physical Disease: A Systematic Review. J. Occup. Rehabil. 2015, 25, 182–196. [Google Scholar] [CrossRef] [PubMed]
- Skoufi, G.I.; Lialios, G.A.; Papakosta, S.; Constantinidis, T.C.; Galanis, P.; Nena, E. Shift Work and Quality of Personal, Professional, and Family Life among Health Care Workers in a Rehabilitation Center in Greece. Indian J. Occup. Environ. Med. 2017, 21, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Firth-Cozens, J.; Greenhalgh, J. Doctors’ perceptions of the links between stress and lowered clinical care. Soc. Sci. Med. 1997, 44, 1017–1022. [Google Scholar] [CrossRef]
- Ruotsalainen, J.; Serra, C.; Marine, A.; Verbeek, J. Systematic review of interventions for reducing occupational stress in health care workers. Scand. J. Work Environ. Health 2008, 34, 169–178. [Google Scholar] [CrossRef]
- Michie, S.; Williams, S. Reducing work related psychological ill health and sickness absence: A systematic literature review. Occup. Environ. Med. 2003, 60, 3–9. [Google Scholar] [CrossRef]
- Tomioka, K.; Morita, N.; Saeki, K.; Okamoto, N.; Kurumatani, N. Working hours, occupational stress and depression among physicians. Occup. Med. 2011, 61, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Lee, S.; Choi, Y.H. Relationship between occupational stress and depressive mood among interns and residents in a tertiary hospital, Seoul, Korea. Clin. Exp. Emerg. Med. 2015, 2, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Bernburg, M.; Vitzthum, K.; Groneberg, D.A.; Mache, S. Physicians’ occupational stress, depressive symptoms and work ability in relation to their working environment: A cross-sectional study of differences among medical residents with various specialties working in German hospitals. BMJ Open 2016, 6, e011369. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Liu, X.L.; Wei, T.D.; Lan, Y.J. Relationship of job stress with job burnout and quality of work life in workers for offshore oil platforms. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi 2017, 35, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Bragard, I.; Dupuis, G.; Fleet, R. Quality of work life, burnout, and stress in emergency department physicians: A qualitative review. Eur. J. Emerg. Med. 2015, 22, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Leitão, J.; Pereira, D.; Gonçalves, Â. Quality of Work Life and Contribution to Productivity: Assessing the Moderator Effects of Burnout Syndrome. Int. J. Environ. Res. Public Health 2021, 18, 2425. [Google Scholar] [CrossRef]
- Guerrero-Barona, E.; Guerrero-Molina, M.; García-Gómez, A.; Moreno-Manso, J.M.; García-Baamonde, M.E. Quality of Working Life, Psychosocial Factors, Burnout Syndrome and Emotional Intelligence. Int. J. Environ. Res. Public Health 2020, 17, 9550. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. The Maslach Burnout Inventory Manual. In Evaluating Stress: A Book of Resources, 3rd ed.; Zalaquette, C.P., Wood, R.J., Eds.; The Scarecrow Press: Lanham, MD, USA, 1997; pp. 191–218. [Google Scholar]
- Shanafelt, T.D.; Dyrbye, L.N.; Sinsky, C.; Hasan, O.; Satele, D.; Sloan, J.; West, C.P. Relationship between Clerical Burden and Characteristics of the Electronic Environment with Physician Burnout and Professional Satisfaction. Mayo Clin. Procs. 2016, 91, 836–848. [Google Scholar] [CrossRef] [PubMed]
- Wallace, J.E.; Lemaire, J.B.; Ghali, W.A. Physician wellness: A missing quality indicator. Lancet 2009, 374, 1714–1721. [Google Scholar] [CrossRef]
- Tang, C.; Guanm, C.; Liu, C. Quality of working life of medical doctors and associated risk factors: A cross-sectional survey in public hospitals in China. BMJ Open. 2022, 12, e063320. [Google Scholar] [CrossRef]
- Van Laar, D.; Edwards, J.A.; Easton, S. The Work-Related Quality of Life scale for healthcare workers. J. Adv. Nurs. 2007, 60, 325–333. [Google Scholar] [CrossRef]
- Sirisawasd, P.; Chaiear, N.; Johns, N.P.; Khiewyoo, J. Validation of the Thai version of a work-related quality of life scale in the nursing profession. Saf. Health Work 2014, 5, 80–85. [Google Scholar] [CrossRef]
- Quality of Working Life. Translated QoWL Scales and Surveys. Available online: https://bit.ly/30QdH7Y (accessed on 8 April 2024).
- Kongsin, T.; Chaiear, N.; Thanomsieng, N.; Boonjaraspinyo, S. Validation of the Brief Thai Version of the Work-Related Quality of Life Scale (Brief THWRQLS). Int. J. Environ. Res. Public Health 2020, 17, 1503. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Kingdom of Thailand Health System Review: Health Systems in Transition; World Health Organization, Regional Office for the Western Pacific: Manila, Philippines, 2015; pp. 103–105. [Google Scholar]
- Intern training program B.E.2560 (as the curriculum for intern certification B.E.2551). In Handbook for Operating the Intern Training Program; The Medical Council of Thailand: Nonthaburi, Thailand, 2017.
- Letter Notifying the Permanent Secretary of the Ministry of Public Health; The Medical Council of Thailand: Nonthaburi, Thailand, 2023; p. 2.
- Standard for Resident and Fellowship Training Programs; The Medical Council of Thailand: Nonthaburi, Thailand, 2017.
- Ministry of Public Health of Thailand. National Health Security Fund: Report to Report to the Senate’s Special Education Commission’s Draft of the Annual Budget Expenditure Act. 2024. Available online: https://hcrp.nhso.go.th/storage/files/875/nhso_2024/nhso_budgetdefend67/nhso_67budgetdefend08.pdf (accessed on 25 February 2024).
- Somsila, N.; Chaiear, N.; Boonjaraspinyo, S.; Tiamkao, S. Work-Related Quality of Life among Medical Residents at a University Hospital in Northeastern Thailand. J. Med. Assoc. Thai. 2015, 98, 1244–1253. [Google Scholar]
- Soonthornvinit, W.; Chaiear, N. Quality of Working life (QoWL) among Doctors in the University Hospitals in the Northeastern Thailand. J. Med. Assoc. Thai. 2019, 102, S39–S46. [Google Scholar]
- Soonthornvinit, W.; Chaiear, N.; Boonjaraspinyo, S.; Tiamkao, S. Working Hours Related to Good Quality of Work Life (QoWL) Among Doctors Working in Public Hospitals in Northeastern Thailand. J. Med. Assoc. Thai. 2019, 102, S47–S54. [Google Scholar]
- Choon-ngarm, N. Mental health and burnout among physicians in general hospital and community hospital in Nakhon Ratchasima province. J. Ment. Health Thai. 2020, 28, 348–359. [Google Scholar]
- Puranitee, P.; Stevens, F.F.C.J.; Pakakasama, S.; Plitponkarnpim, A.; Vallibhakara, S.A.; Busari, J.O.; Heeneman, S.; van Mook, W.N.K.A. Exploring burnout and the association with the educational climate in pediatric residents in Thailand. BMC Med. Educ. 2019, 19, 245. [Google Scholar] [CrossRef]
- Nimmawitt, N.; Wannarit, K.; Pariwatcharakul, P. Thai psychiatrists and burnout: A national survey. PLoS ONE 2020, 15, e0230204. [Google Scholar] [CrossRef] [PubMed]
- Charoentanyarak, A.; Anothaisintawee, T.; Kanhasing, R.; Poonpetcharat, P. Prevalence of Burnout and Associated Factors among Family Medicine Residency in Thailand. J. Med. Educ. Curric. Dev. 2020, 7, 2382120520944920. [Google Scholar] [CrossRef] [PubMed]
- Thamrongvisava, S.; Pitanupong, J. The Prevalence and Associated Factors of Burnout Syndrome among Residents in Training at Faculty of Medicine, Songklanagarind Hospital. J. Psychiatr. Assoc. Thail. 2018, 63, 309–320. [Google Scholar]
- Na Bangxang, J. Resident Burnout: Prevalence and Associated Factors in Rajavithi Hospital. J. Psychiatr. Assoc. Thail. 2019, 64, 61–76. [Google Scholar]
- Garcia, L.C.; Shanafelt, T.D.; West, C.P.; Sinsky, C.A.; Trockel, M.T.; Nedelec, L.; Maldonado, Y.A.; Tutty, M.; Dyrbye, L.N.; Fassiotto, M. Burnout, Depression, Career Satisfaction, and Work-Life Integration by Physician Race/Ethnicity. JAMA Netw. Open. 2020, 3, e2012762. [Google Scholar] [CrossRef] [PubMed]
- Hall, L.H.; Johnson, J.; Watt, I.; Tsipa, A.; O’Connor, D.B. Healthcare Staff Wellbeing, Burnout, and Patient Safety: A Systematic Review. PLoS ONE 2016, 11, e0159015. [Google Scholar] [CrossRef]
- Rothenberger, D.A. Physician Burnout and Well-Being: A Systematic Review and Framework for Action. Dis. Colon. Rectum 2017, 60, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.D.; West, C.P.; Dyrbye, L.N.; Trockel, M.; Tutty, M.; Wang, H.; Carlasare, L.E.; Sinsky, C. Changes in Burnout and Satisfaction with Work-Life Integration in Physicians during the First 2 Years of the COVID-19 Pandemic. Mayo Clin. Proc. 2022, 97, 2248–2258. [Google Scholar] [CrossRef]
- Olson, K.D. Physician Burnout-A Leading Indicator of Health System Performance? Mayo Clin. Proc. 2017, 92, 1608–1611. [Google Scholar] [CrossRef]
- Tawfik, D.S.; Scheid, A.; Profit, J.; Shanafelt, T.; Trockel, M.; Adair, K.C.; Sexton, J.B.; Ioannidis, J.P.A. Evidence Relating Health Care Provider Burnout and Quality of Care: A Systematic Review and Meta-analysis. Ann. Intern. Med. 2019, 171, 555–567. [Google Scholar] [CrossRef]
- Sammawart, S. Burnout among nurses in Ramathibodi Hospital; Faculty of Medicine Ramathibodi Hospital, Mahidol University: Bangkok, Thailand, 1989. [Google Scholar]
- Ngamjarus, C.; Chongsuvivatwong, V.; McNeilm, E. n4Studies: Sample Size Calculation for an Epidemiological Study on a Smart Device. Siriraj Med. J. 2016, 68, 160–170. [Google Scholar]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard: Thailand Situation. Available online: https://covid19.who.int/region/searo/country/th (accessed on 25 February 2024).
- Storman, M.; Storman, D.; Maciąg, J. Quality of work-life among young medical doctors in Poland. Int. J. Occup. Saf. Ergo. 2022, 28, 1611–1617. [Google Scholar] [CrossRef]
- Ofei-Dodoo, S.; Kellerman, R.; Gilchrist, K.; Casey, E.M. Burnout and Quality of Life among Active Member Physicians of the Medical Society of Sedgwick County. Kans J. Med. 2019, 12, 33–39. [Google Scholar] [CrossRef]
- Xiao, Y.; Wang, J.; Chen, S.; Wu, Z.; Cai, J.; Weng, Z.; Li, C.; Zhang, K. Psychological distress, burnout level and job satisfaction in emergency medicine: A cross-sectional study of physicians in China. Emerg. Med. Australas 2014, 26, 538–542. [Google Scholar] [CrossRef] [PubMed]
- Hodkinson, A.; Zhou, A.; Johnson, J.; Geraghty, K.; Riley, R.; Zhou, A.; Panagopoulou, E.; Chew-Graham, C.A.; Peters, D.; Esmail, A.; et al. Associations of physician burnout with career engagement and quality of patient care: Systematic review and meta-analysis. BMJ 2022, 378, e070442. [Google Scholar] [CrossRef]
- Fred, H.L.; Scheid, M.S. Physician Burnout: Causes, Consequences, and (?) Cures. Tex. Heart Inst. J. 2018, 45, 198–202. [Google Scholar] [CrossRef]
- West, C.P.; Huschka, M.M.; Novotny, P.J.; Sloan, J.A.; Kolars, J.C.; Habermann, T.M.; Shanafelt, T.D. Association of Perceived Medical Errors with Resident Distress and EmpathyA Prospective Longitudinal Study. JAMA 2006, 296, 1071–1078. [Google Scholar] [CrossRef]
- Dewa, C.S.; Loong, D.; Bonato, S.; Thanh, N.X.; Jacobs, P. How does burnout affect physician productivity? A systematic literature review. BMC Health Serv. Res. 2014, 14, 325. [Google Scholar] [CrossRef] [PubMed]
- Williams, E.S.; Manwell, L.B.; Konrad, T.R.; Linzer, M. The relationship of organizational culture, stress, satisfaction, and burnout with physician-reported error and suboptimal patient care: Results from the MEMO study. Health Care Manag. Rev. 2007, 32, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.D.; Balch, C.M.; Bechamps, G.; Russell, T.; Dyrbye, L.; Satele, D.; Collicott, P.; Novotny, P.J.; Sloan, J.; Freischlag, J. Burnout and Medical Errors among American Surgeons. Ann. Surg. 2010, 251, 995–1000. [Google Scholar] [CrossRef]
- Knight, C.; Patterson, M.; Dawsonm, J. Building work engagement: A systematic review and meta-analysis investigating the effectiveness of work engagement interventions. J. Organ. Behav. 2017, 38, 792–812. [Google Scholar] [CrossRef]
- Mauno, S.; Kinnunen, U.; Ruokolainen, M. Job Demands and Resources as Antecedents of Work Engagement: A Longitudinal Study. J. Vocat. Behav. 2007, 70, 149–171. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Noseworthy, J.H. Executive Leadership and Physician Well-being: Nine Organizational Strategies to Promote Engagement and Reduce Burnout. Mayo Clin. Proc. 2017, 92, 129–146. [Google Scholar] [CrossRef] [PubMed]
- Simons, G.; Baldwin, D.S. A critical review of the definition of ‘wellbeing’ for doctors and their patients in a post COVID-19 era. Int. J. Soc. Psychiatr. 2021, 67, 984–991. [Google Scholar] [CrossRef] [PubMed]
- Bovier, P.A.; Arigoni, F.; Schneider, M.; Gallacchi, M.B. Relationships between work satisfaction, emotional exhaustion and mental health among Swiss primary care physicians. Eur. J. Public Health 2009, 19, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Elbejjani, M.; Abed, A.l.; Ahad, M.; Simon, M.; Ausserhofer, D.; Dumit, N.; Abu-Saad Huijer, H.; Dhaini, S.R. Work environment-related factors and nurses’ health outcomes: A cross-sectional study in Lebanese hospitals. BMC Nurs. 2020, 19, 95. [Google Scholar] [CrossRef] [PubMed]
- Paskarini, I.; Dwiyanti, E.; Syaiful, D.A.; Syanindita, D. Burnout among nurses: Examining psychosocial work environment causes. J. Public Health Res. 2023, 12, 22799036221147812. [Google Scholar] [CrossRef] [PubMed]
- Yates, S.W. Physician Stress and Burnout. Am. J. Med. 2020, 133, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Tanios, M.; Haberman, D.; Bouchard, J.; Motherwell, M.; Patel, J. Analyses of burn-out among medical professionals and suggested solutions—A narrative review. J. Hosp. Manag. Health Policy 2022, 6, 7. [Google Scholar] [CrossRef]
- Marques-Pinto, A.; Moreira, S.; Costa-Lopes, R.; Zózimo, N.; Vala, J. Predictors of Burnout Among Physicians: Evidence From a National Study in Portugal. Front. Psychol. 2021, 12, 699974. [Google Scholar] [CrossRef]
- NNRoad. 5 Things You Must KNOW about Work Culture in Thailand. Available online: https://nnroad.com/blog/work-culture-in-thailand (accessed on 9 April 2024).




| Quality of Work Life (QWL) Subscales [Number of Items] | Levels of QWL | ||
|---|---|---|---|
| Low (Points) | Moderate (Points) | High (Points) | |
| Employee engagement (EET) [2] | 2 to 4 | 5 to 7 | 8 to 10 |
| Control at work (CAW) [3] | 3 to 6 | 7 to 10 | 11 to 15 |
| Home–work interface (HWI) [3] | 3 to 6 | 7 to 10 | 11 to 15 |
| General well-being (GWB) [4] | 4 to 9 | 10 to 15 | 16 to 20 |
| Job and career satisfaction (JCS) [6] | 6 to 13 | 14 to 21 | 22 to 30 |
| Working conditions (WCS) [3] | 3 to 6 | 7 to 10 | 11 to 15 |
| Stress at work (SAW) [3] | 3 to 6 | 7 to 10 | 11 to 15 |
| Total scores of QWL [24] | 24 to 56 | 57 to 89 | 90 to 120 |
| Overall (OVL) [1] | 1 | 2 to 3 | 4 to 5 |
| Burnout Subscales [Number of Items] | Levels of Burnout | ||
| Low (Points) | Moderate (Points) | High (Points) | |
| Emotional exhaustion (EE) [9] | 0 to 16 | 17 to 26 | >26 |
| Depersonalization (DP) [5] | 0 to 6 | 7 to 12 | >12 |
| Personal accomplishment (PA) [8] | >38 | 32 to 38 | 0 to 31 |
| Characteristics | Total (n = 241) | Quality-of-Work-Life Levels | p-Value | |
|---|---|---|---|---|
| Moderate to High (n = 175, 72.6%) | Low (n = 66, 27.4%) | |||
| Sex | ||||
| Female | 108 (44.8) | 77 (44.0) | 31 (47.0) | 0.772 a |
| Male | 133 (55.2) | 98 (56.0) | 35 (53.0) | |
| Age (years) | 25.52 (2.01) | 25.54 (1.93) | 25.55 (2.18) | 0.960 b |
| Income per month (Baht), mean ± SD | 60,937.89 ±17,054.66 | 62,482.56 ±17,762.72 | 60,000 ±13,017.08 | 0.340 b |
| Underlying diseases | ||||
| Yes | 113 (46.9) | 82 (46.9) | 31 (47.0) | 0.988 a |
| No | 128 (53.1) | 93 (53.1) | 35 (53.0) | |
| Taking medication (n = 113) | ||||
| Yes | 62 (54.9) | 47 (75.8) | 15 (24.2) | 0.513 a |
| No | 51 (45.1) | 35 (68.6) | 16 (31.4) | |
| Region of hospital location | ||||
| Central | 68 (28.2) | 44 (25.1) | 24 (36.4) | 0.015 a,* |
| East | 24 (10.0) | 23 (13.1) | 1 (1.5) | |
| West | 17 (7.1) | 10 (5.7) | 7 (10.6) | |
| North | 34 (14.1) | 29 (16.6) | 5 (7.6) | |
| Northeast | 65 (27.0) | 44 (25.1) | 21 (31.8) | |
| South | 33 (13.7) | 25 (14.3) | 8 (12.1) | |
| Hospital affiliation | ||||
| Ministry of Public Health | 200 (83.0) | 145 (82.9) | 55 (83.3) | 0.930 b |
| Others | 41 (17.0) | 30 (17.1) | 11 (16.7) | |
| Quality of Work Life and Its Dimensions in Thai Physicians, % | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Low Levels | Moderate Levels | High Levels | |||||||
| Residents (2015) a | University Physicians (2019) b | Interns (2022) c | Residents (2015) a | University Physicians (2019) b | Interns (2022) c | Residents (2015) a | University Physicians (2019) b | Interns (2022) c | |
| QWL ≠ | 1.5 | 3.0 | 27.4 | 76.6 | 58.6 | 69.7 | 21.9 | 38.4 | 2.9 |
| EET | 0.8 | 3.5 | 38.6 | 55.5 | 42.1 | 47.7 | 43.8 | 54.5 | 13.7 |
| CAW | 15.9 | 3.5 | 30.7 | 56.2 | 51.8 | 54.8 | 27.3 | 44.7 | 14.5 |
| HWI | 23.4 | 6.1 | 39.4 | 52.7 | 54.5 | 53.1 | 23.4 | 39.5 | 7.5 |
| GWB | 5.9 | 5.6 | 17.8 | 73.4 | 46.4 | 81.3 | 20.7 | 47.9 | 0.9 |
| JSC | 0.0 | 0.9 | 12.9 | 36.7 | 22.1 | 65.1 | 63.3 | 77.0 | 22.0 |
| WCS | 9.8 | 3.0 | 31.5 | 69.5 | 54.2 | 54.4 | 20.7 | 42.7 | 14.1 |
| SAW | 35.9 | 20.2 | 35.7 | 54.7 | 67.7 | 47.3 | 9.4 | 12.2 | 17.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Surawattanasakul, V.; Kiratipaisarl, W.; Siviroj, P. Burnout and Quality of Work Life among Physicians during Internships in Public Hospitals in Thailand. Behav. Sci. 2024, 14, 361. https://0-doi-org.brum.beds.ac.uk/10.3390/bs14050361
Surawattanasakul V, Kiratipaisarl W, Siviroj P. Burnout and Quality of Work Life among Physicians during Internships in Public Hospitals in Thailand. Behavioral Sciences. 2024; 14(5):361. https://0-doi-org.brum.beds.ac.uk/10.3390/bs14050361
Chicago/Turabian StyleSurawattanasakul, Vithawat, Wuttipat Kiratipaisarl, and Penprapa Siviroj. 2024. "Burnout and Quality of Work Life among Physicians during Internships in Public Hospitals in Thailand" Behavioral Sciences 14, no. 5: 361. https://0-doi-org.brum.beds.ac.uk/10.3390/bs14050361