
Nerve Regeneration after a Nerve Graft in a Rat Model: The Effectiveness of Fibrin Glue

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Walking Track Analysis
2.2. Electroneurophysiological Evaluation
2.3. Muscle Mass Indexes
2.4. Histological Analysis
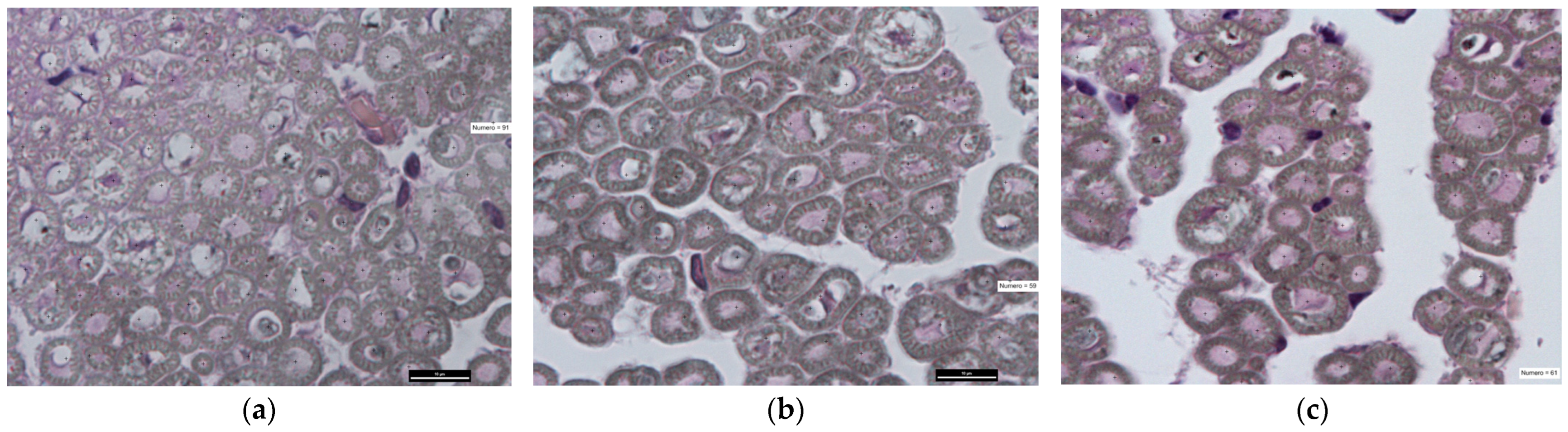
- n = Number of myelinated fibers;
- Fiber Area (FA): Area occupied by nerve fibers (μm2) on an assessed sample area of 5500 μm2;
- Fiber Density (FD): Number of myelinated fibers (n) over the entire area of the sciatic nerve section (μm2).
3. Results
3.1. Walking Track Analysis
3.2. Electroneurophysiological Evaluation
3.3. Muscle Mass Indexes
3.3.1. GMWR
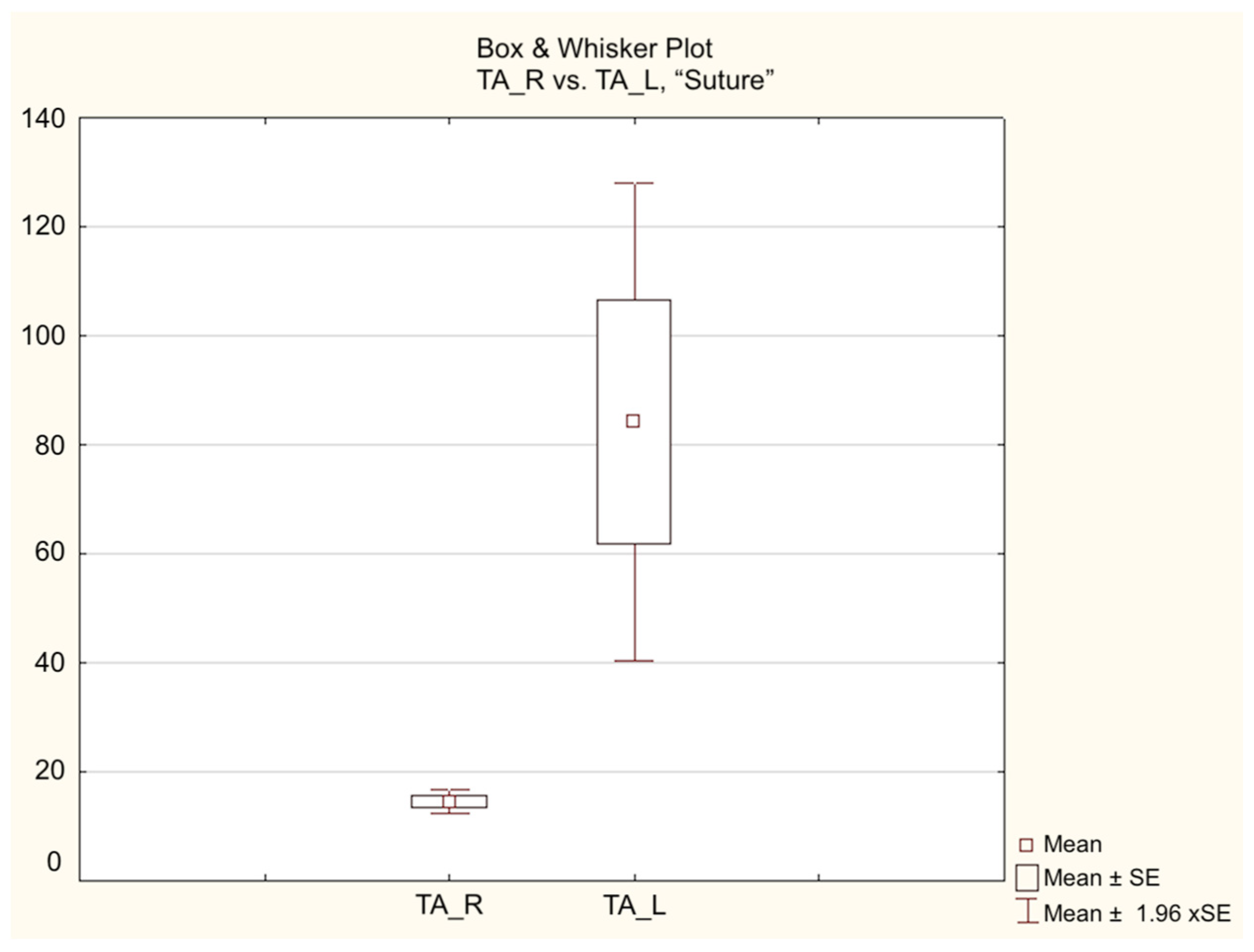
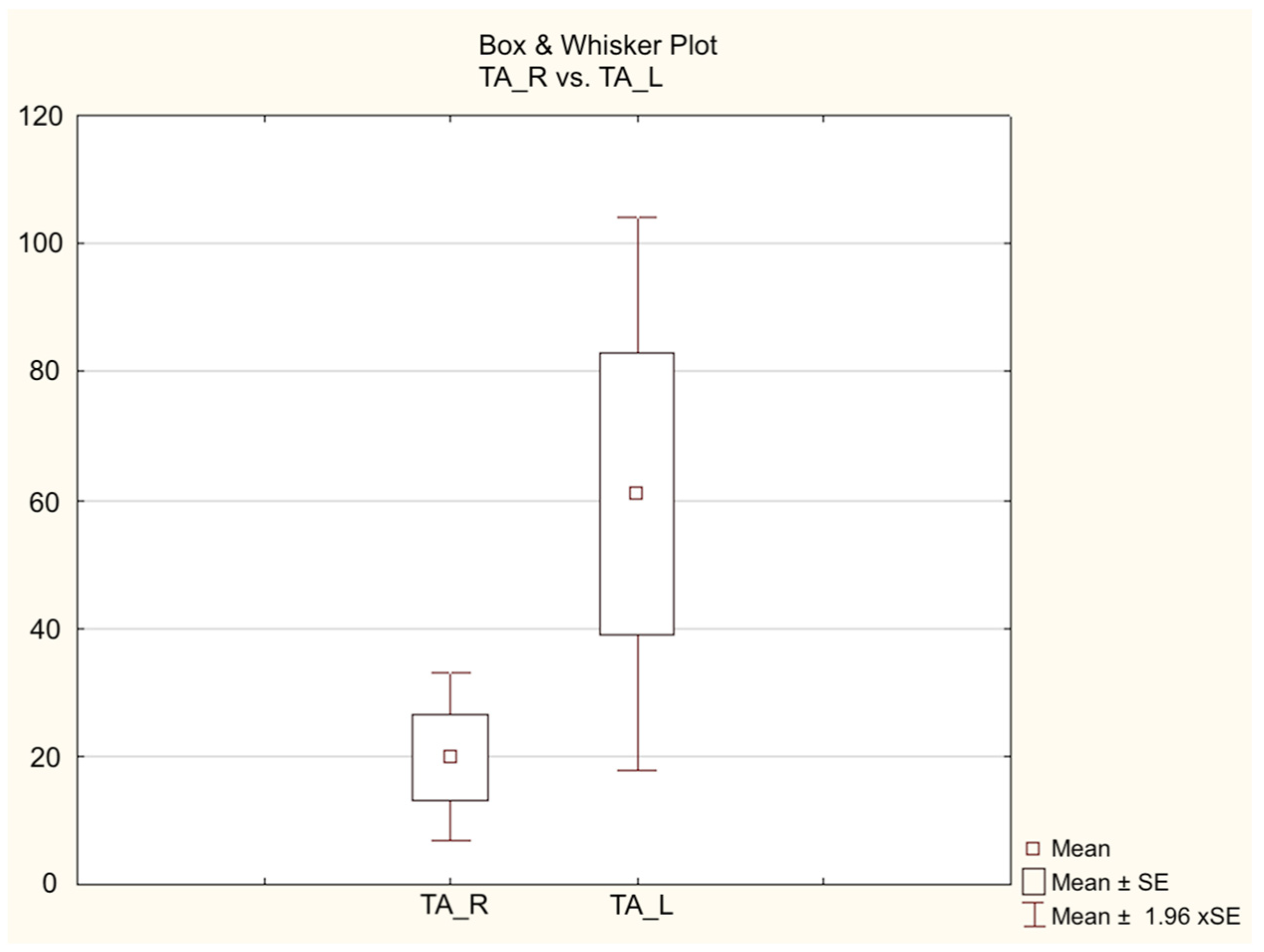
3.3.2. TAMWR
3.4. Histological Analysis
4. Discussion
- -
- Walking Track Analysis for the analysis of the locomotor activity;
- -
- Electroneurography;
- -
- Weight of the muscles (and their ratio);
- -
- Histological examination of the regenerated.
- -
- Sciatic Functional Index is a reference parameter used for evaluating the functional restoration in the regeneration of peripheral nerves for the mouse and rat model, but the results of this test can still be influenced by the behavior of the animal;
- -
- Variability in fibrin glue preparation and usage; many fibrin glues exist, so this study’s results could be different using different glues commercially available;
- -
- The sample size was relatively small, but due to ethical reasons was kept adherent to the preventive sample size calculation based on statistical power;
- -
- We did not analyze, through histological staining, the potential to reduce the inflammation response when using fibrin glue compared to neurorrhaphy; we acknowledge that conducting such a study would be beneficial for our future investigations.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khalifeh, J.M.; Dibble, C.F.; Dy, C.J.; Ray, W.Z. Cost-effectiveness analysis of combined dual motor nerve transfers versus alternative surgical and nonsurgical management strategies to restore shoulder function following upper brachial plexus injury. Neurosurgery 2019, 84, 362–377. [Google Scholar] [CrossRef] [PubMed]
- Gaiovych, I.; Savosko, S.; Labunets, I.; Utko, N.; Makarenko, A.; Chaikovsky, Y. Sciatic nerve regeneration after autografting and application of the bone marrow aspirate concentration. Georgian Med. News 2019, 295, 145–152. [Google Scholar]
- Kornfeld, T.; Vogt, P.M.; Radtke, C. Nerve grafting for peripheral nerve injuries with extended defect sizes. Wien. Med. Wochenschr. 2019, 169, 240–251. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.; Wang, L.; Chen, F.; Huang, Y.; Shi, J.; Zhu, X.; Ding, Y.; Zhang, X. Evaluation of artificial nerve conduit and autografts in peripheral nerve repair in the rat model of sciatic nerve injury. Neurol. Res. 2016, 38, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.I.; Wandling, G.D.; Talukder, M.H.; Govindappa, P.K.; Elfar, J.C. A Novel Standardized Peripheral Nerve Transection Method and a Novel Digital Pressure Sensor Device Construction for Peripheral Nerve Crush Injury. Bio-Protocol 2022, 12, e4350. [Google Scholar] [CrossRef]
- Salomone, R.; Bento, R.F.; Costa, H.J.; Azzi-Nogueira, D.; Ovando, P.C.; Da-Silva, C.F.; Zanatta, D.B.; Strauss, B.E.; Haddad, L.A. Bone marrow stem cells in facial nerve regeneration from isolated stumps. Muscle Nerve 2013, 48, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Heaton, J.T.; Sheu, S.H.; Hohman, M.H.; Knox, C.J.; Weinberg, J.S.; Kleiss, I.J.; Hadlock, T.A. Rat whisker movement after facial nerve lesion: Evidence for autonomic contraction of skeletal muscle. Neuroscience 2014, 265, 9–20. [Google Scholar] [CrossRef]
- Turner, N.J.; Johnson, S.A.; Foster, L.J.R.; Badylak, S.F. Sutureless nerve repair with ECM bioscaffolds and laser-activated chitosan adhesive. J. Biomed. Mater. Res. Part B Appl. Biomater. 2018, 106, 1698–1711. [Google Scholar] [CrossRef]
- Ornelas, L.; Padilla, L.; Di Silvio, M.; Schalch, P.; Esperante, S.; Infante, P.L.; Bustamante, J.C.; Avalos, P.; Varela, D.; Lopez, M. Fibrin glue: An alternative technique for nerve coaptation—Part I. Wave amplitude, conduction velocity, and plantar-length factors. J. Reconstr. Microsurg. 2006, 22, 119–122. [Google Scholar] [CrossRef]
- Ornelas, L.; Padilla, L.; Di Silvio, M.; Schalch, P.; Esperante, S.; Infante, R.L.; Bustamante, J.C.; Avalos, P.; Varela, D.; Lopez, M. Fibrin glue: An alternative technique for nerve coaptation–part II. Nerve regeneration and his-tomorphometric assessment. J. Reconstr. Microsurg. 2006, 22, 123–128. [Google Scholar] [CrossRef]
- Hong, J.P.; Masoodi, Z.; Tzou, C.J. Attributes of a good microsurgeon—A brief counsel to the up-and-coming prospects. Arch. Plast. Surg. 2023, 50, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Koulaxouzidis, G.; Reim, G.; Witzel, C. Fibrin glue repair leads to enhanced axonal elongation during early peripheral nerve regeneration in an in vivo mouse model. Neural Regen. Res. 2015, 10, 1166–1171. [Google Scholar] [CrossRef]
- Wang, W.; Degrugillier, L.; Tremp, M.; Prautsch, K.; Sottaz, L.; Schaefer, D.J.; Madduri, S.; Kalbermatten, D. Nerve repair with fibrin nerve conduit and modified suture placement. Anat. Rec. 2018, 301, 1690–1696. [Google Scholar] [CrossRef] [PubMed]
- Caillaud, M.; Richard, L.; Vallat, J.M.; Desmouliere, A.; Billet, F. Peripheral nerve regeneration and intraneural revascularization. Neural Regen. Res. 2019, 14, 24–33. [Google Scholar] [PubMed]
- Barton, M.J.; Morley, J.W.; Stoodley, M.A.; Lauto, A.; Mahns, D.A. Nerve repair: Toward a sutureless approach. Neurosurg. Rev. 2014, 37, 585–595. [Google Scholar] [CrossRef]
- Rafijah, G.; Bowen, A.J.; Dolores, C.; Vitali, R.; Mozaffar, T.; Gupta, R. The effects of adjuvant fibrin sealant on the surgical repair of segmental nerve defects in an animal model. J. Hand. Surg. 2013, 38, 847–855. [Google Scholar] [CrossRef]
- Maeda, T.; Hori, S.; Sasaki, S.; Maruo, S. Effects of tension at the site of coaptation on recovery of sciatic nerve function after neurorrhaphy: Evaluation by walking-track measurement, electrophysiology, histomorphometry, and electron probe X-ray microanalysis. Microsurgery 1999, 19, 200–207. [Google Scholar] [CrossRef]
- Gordon, T. Nerve regeneration: Understanding biology and its influence on return of function after nerve transfers. Hand Clin. 2016, 32, 103–117. [Google Scholar] [CrossRef]
- Shuchi, A.; Gupta, D.; Sarabahi, S. An Outcome Analysis of Fibrin Sealant versus Staples for Fixation of Split-Thickness Skin Grafts. Indian J. Plast. Surg. 2024, 57, 60–66. [Google Scholar] [CrossRef]
- Beudert, M.; Gutmann, M.; Lühmann, T.; Meinel, L. Fibrin Sealants: Challenges and Solutions. ACS Biomater. Sci. Eng. 2022, 8, 2220–2231. [Google Scholar] [CrossRef]
- Koopman, J.E.; Duraku, L.S.; de Jong, T.; de Vries, R.B.M.; Michiel Zuidam, J.; Hundepool, C.A. A Systematic Review and Meta-Analysis on the Use of Fibrin Glue in Peripheral Nerve Repair: Can We Just Glue It? J. Plast. Reconstr. Aesthet. Surg. 2022, 75, 1018–1033. [Google Scholar] [CrossRef] [PubMed]
- Biscola, N.P.; Cartarozzi, L.P.; Ulian-Benitez, S.; Barbizan, R.; Castro, M.V.; Spejo, A.B.; Ferreira, R.S., Jr.; Barraviera, B.; Oliveira, A.L.R. Multiple uses of fibrin sealant for nervous system treatment following injury and disease. J. Venom. Anim. Toxins Incl. Trop. Dis. 2017, 23, 13. [Google Scholar] [CrossRef] [PubMed]
- Siroya, H.L.; Kumar, V.B.; Bhat, D.I.; Shukla, D.P.; Devi, B.I. Is Popularity of Fibrin Glue a Misrepresentation? A Comparative Study with Fibrin Glue and Suture Anastomosis in Rat Sciatic Nerve Injury Analysing Functional, Histological, Electrophysiological Parameters. Neurol. India 2023, 71, 55–61. [Google Scholar] [PubMed]
- Akbari, H.; Farrokhi, B.; Emami, S.-A.; Akhoondinasab, M.-R.; Akbari, P.; Karimi, H. Comparison of the never repair with fibrin glue and perineural micro-suture in rat model. World J. Plast. Surg. 2020, 9, 44–47. [Google Scholar] [PubMed]
- Braga Silva, J.; Becker, A.S.; Leal, B.L.M.; Busnello, C.V. Advances of Direct Peripheral Nerve Repair Techniques: Do We Already Have Enough Scientific Evidence? Indian J. Orthop. 2022, 57, 189–202. [Google Scholar] [CrossRef]
- Potter, B.K. From Bench to Bedside: No Need to be Nervous about Microsuturing? Clin. Orthop. Relat. Res. 2017, 475, 2165–2167. [Google Scholar] [CrossRef] [PubMed]
- Isaacs, J.E.; McDaniel, C.O.; Owen, J.R.; Wayne, J.S. Comparative analysis of biomechanical performance of available “nerve glues”. J. Hand Surg. Am. 2008, 33, 893–899. [Google Scholar] [CrossRef] [PubMed]
- Matras, H.; Braun, F.; Lassmann, H.; Ammerer, H.P.; Mamoli, B. Plasma clot welding of nerves (experimental report). J. Max Fac. Surg. 1973, 1, 236–247. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.I.; Gurjar, A.A.; Talukder MA, H.; Rodenhouse, A.; Manto, K.; O’Brien, M.; Govindappa, P.K.; Elfar, J.C. A novel nerve transection and repair method in mice: Histomorphometric analysis of nerves, blood vessels, and muscles with functional recovery. Sci. Rep. 2020, 10, 21637. [Google Scholar] [CrossRef]
- Benfield, C.; Isaacs, J.; Mallu, S.; Kurtz, C.; Smith, M. Comparison of nylon suture versus 2 fibrin glue products for delayed nerve coaptation in an animal model. J. Hand Surg. Am. 2021, 46, 119–125. [Google Scholar] [CrossRef]
- Sallam, A.; Eldeeb, M.; Kamel, N. Autologous fibrin glue versus microsuture in the surgical reconstruction of periph- eral nerves: A randomized clinical trial. J. Hand Surg. Am. 2022, 47, 89.e1–89.e11. [Google Scholar] [CrossRef] [PubMed]
- Leite, A.P.S.; Pinto, C.G.; Tibúrcio, F.C.; Sartori, A.A.; Rodrigues, A.d.C.; Barraviera, B.; Ferreira, R.S.; Filadelpho, A.L.; Matheus, S.M.M. Heterologous fibrin sealant potentiates axonal regeneration after peripheral nerve injury with reduction in the number of suture points. Injury 2019, 50, 834–847. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, S.; Shortland, P.; Lauto, A.; Barton, M.; Morley, J.W.; Mahns, D.A. Sensory perturbations using suture and sutureless repair of transected median nerve in rats. Somatosens. Mot. Res. 2016, 33, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Martins, R.S.; Siqueira, M.G.; Silva, C.F.; Godoy, B.O.; Plese, J.P. Electrophysiologic assessment of regeneration in rat sciatic nerve repair using suture, fibrin glue or a combination of both techniques. Arq. Neuropsiquiatr. 2005, 63, 601–604. [Google Scholar] [CrossRef] [PubMed]
- Martins, R.S.; Siqueira, M.G.; Da Silva, C.F.; Plese, J.P. Overall assessment of regeneration in peripheral nerve lesion repair using fibrin glue, suture, or a combination of the 2 techniques in a rat model: Which is the ideal choice? Surg. Neurol. 2005, 64 (Suppl. S1), 10–16; discussion 16. [Google Scholar]
- Fisher, A.H.; Johnsen, P.H.; Simon, A.; Burns, C.J.; Romiyo, V.; Bodofsky, E.B.; Vega, S.L.; Fuller, D.A. Fibrin Glue Acutely Blocks Distal Muscle Contraction after Confirmed Polyethylene Glycol Nerve Fusion: An Animal Study. Plast. Reconstr. Surg. Glob. Open 2024, 12, e5535. [Google Scholar] [CrossRef]
- Erdal, A.I.; Findikçioğlu, K.; Karasu, O.; Özkoçer, S.E.; Elmas, Ç. Use of Erythropoietin and Fibrin Glue Mixture for Peripheral Nerve Repair. Plast. Reconstr. Surg. 2022, 149, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Suri, A.; Mehta, V.S.; Sarkar, C. Microneural anastomosis with fibrin glue: An experimental study. Neurol. India 2002, 50, 23–26. [Google Scholar] [PubMed]
- Adel, M.; Abdo Elgamal, D.; Bakry, R.; Abdelkader, M.; Elshazly, M.; Kamel, A. Suture versus fibrin glue microneural anastomosis of the femoral nerve in Sprague dewly rat model. A comparative experimental assessment of the clinical, histological and statistical features. Acta Chir. Plast. 2017, 59, 65–71. [Google Scholar]
- Akhter, E.T.; Rotterman, T.M.; English, A.W.; Alvarez, F.J. Sciatic nerve cut and repair using fibrin glue in adult mice. Bio Protoc. 2019, 9, e3363. [Google Scholar] [CrossRef] [PubMed]
- Spotnitz, W.D. Fibrin sealant: Past, present, and future: A brief review. World J. Surg. 2010, 34, 632–634. [Google Scholar] [CrossRef]
- Becker, C.M.; Gueuning, C.O.; Graff, G.L. Sutures or fibrin glue for divided rat nerves: Schwann cell and muscle metabolism. Microsurgery 1985, 6, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Sameem, M.; Wood, T.J.; Bain, J.R. A systematic review on the use of fibrin glue for peripheral nerve repair. Plast. Reconstr. Surg. 2011, 127, 2381–2390. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, E.C.; Haddara, M.M.; Wu, K.Y.; Chambers, S.B.; Ferreira, L.M.; Gillis, J.A. Strength comparison of fibrin glue and suture constructs in upper extremity peripheral nerve coaptations: An in vitro study. J. Hand Surg. Am. 2022, 48, 620.e1–620.e6. [Google Scholar] [CrossRef] [PubMed]
- Childe, J.R.; Regal, S.; Schimoler, P.; Kharlamov, A.; Miller, M.C.; Tang, P. Fibrin glue increases the tensile strength of conduit-assisted primary digital nerve repair. Hand 2018, 13, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Menovsky, T.; Beek, J.F. Laser, fibrin glue, or suture repair of peripheral nerves: A comparative functional, histological, and morphometric study in the rat sciatic nerve. J. Neurosurg. 2001, 95, 694–699. [Google Scholar] [CrossRef] [PubMed]
- Inalöz, S.S.; Ak, H.E.; Vayla, V.; Akin, M.; Aslan, A.; Sari, I.; Çelik, Y.; Özkan, Ü. Comparison of microsuturing to the use of tissue adhesives in anastomosing sciatic cuts in rats. Neurosurg. Rev. 1997, 20, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Biazar, E.; Heidari Keshel, S.; Pouya, M. Behavioral evaluation of regenerated rat sciatic nerve by a nanofibrous PHBV conduit filled with Schwann cells as artificial nerve graft. Cell Commun. Adhes. 2013, 20, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Giusti, G.; Willems, W.F.; Kremer, T.; Friedrich, P.F.; Bishop, A.T.; Shin, A.Y. Return of motor function after segmental nerve loss in a rat model: Comparison of autogenous nerve graft, collagen conduit, and processed allograft (AxoGen). J. Bone Joint Surg. Am. 2012, 94, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Summa, P.G.; Kalbermatten, D.F.; Pralong, E.; Raffoul, W.; Kingham, P.J.; Terenghi, G. Long-term in vivo regeneration of peripheral nerves through bioengineered nerve grafts. Neuroscience 2011, 181, 278–291. [Google Scholar] [CrossRef]
- Saltzman, E.B.; Villa, J.C.; Doty, S.B.; Feinberg, J.H.; Lee, S.K.; Wolfe, S.W. A Comparison Between Two Collagen Nerve Conduits and Nerve Autograft: A Rat Model of Motor Nerve Regeneration. J. Hand Surg. Am. 2019, 44, 700.e1–700.e9. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 16 Weeks Control Group | 21 Weeks Control Group | 16 Weeks Study Group | 21 Weeks Study Group | |
|---|---|---|---|---|
| Average SFI | −47.6 range −35/−60 | −38 range −48/−19 | −45.8 range −40/−68 | −40 range −52/−20 |
| 16 Weeks Control Group | 21 Weeks Control Group | 16 Weeks Study Group | 21 Weeks Study Group | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Gastrocnemius muscles | Average weight | Operated Limb | Healthy Limb | Operated Limb | Healthy Limb | Operated Limb | Healthy Limb | Operated Limb | Healthy Limb |
| 1.008 g range: 0.41–1.38 g | 1.712 g range: 1.06–2.2 g | 0.7620 g range: 0.59–0.86 g | 1.266 g range: 1.01–1.43 g | 0.93 g range: 0.33–1.32 g | 1.768 g range: 1.01–2.5 g | 0.6460 g range: 0.31–0.84 g | 1.2320 g range: 0.92–1.59 g | ||
| Average GMWR | 0.6041 range: 0.262820513–0.90566037 | 0.6368 range: 0.495798319–0.851485149 | 0.5027 range: 0.326732673–0.601990049 | 0.5253 range: 0.336956522–0.762376238 | |||||
| Tibialis Anterior muscles | Average weight | OPERATED LIMB | HEALTHY LIMB | OPERATED LIMB | HEALTHY LIMB | OPERATED LIMB | HEALTHY LIMB | OPERATED LIMB | HEALTHY LIMB |
| 0.63 g range: 0.35–1.08 g | 1.188 g range: 0.67–1.48 g | 0.3720 g range: 0.31–0.46 g | 0.71 g range: 0.55–0.78 g | 0.6160 g range: 0.11–1.11 g | 1.2420 g range: 0.55–1.99 g | 0.2480 g range: 0.15–0.37 g | 0.56 g range: 0.45–0.66 g | ||
| Average TAMWR | 0.5519 range: 0.357142857–0.729729729 | 0.5316 range: 0.397435897–0.63 | 0.4534 range: 0.2–0.6094674556 | 0.4458 range: 0.2878787878–0.6086956521 | |||||
| 16 Weeks Control Group | 21 Weeks Control Group | 16 Weeks Study Group | 21 Weeks Study Group | |
|---|---|---|---|---|
| Average number of regenerated nervous fibers | 59 ± 5 | 65 ± 3.9 | 61 ± 3 | 67 ± 2.6 |
| Fiber area | 4410 ± 150 μm2 | 4854 ± 150 μm2 | 4586 ± 148 μm2 | 5044 ± 130 μm2 |
| Fiber density | 0.0109 ± 0.0004 fibers/μm2 | 0.012 ± 0.0004 fibers/μm2 | 0.0112 ± 0.0005 fibers/μm2 | 0.0123 ± 0.0005 fibers/μm2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zabbia, G.; Toia, F.; Coppola, F.; Cassata, G.; Cicero, L.; Giglia, G.; Puleio, R.; Cordova, A. Nerve Regeneration after a Nerve Graft in a Rat Model: The Effectiveness of Fibrin Glue. J. Pers. Med. 2024, 14, 445. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm14050445
Zabbia G, Toia F, Coppola F, Cassata G, Cicero L, Giglia G, Puleio R, Cordova A. Nerve Regeneration after a Nerve Graft in a Rat Model: The Effectiveness of Fibrin Glue. Journal of Personalized Medicine. 2024; 14(5):445. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm14050445
Chicago/Turabian StyleZabbia, Giovanni, Francesca Toia, Federico Coppola, Giovanni Cassata, Luca Cicero, Giuseppe Giglia, Roberto Puleio, and Adriana Cordova. 2024. "Nerve Regeneration after a Nerve Graft in a Rat Model: The Effectiveness of Fibrin Glue" Journal of Personalized Medicine 14, no. 5: 445. https://0-doi-org.brum.beds.ac.uk/10.3390/jpm14050445