
Soft Robotic Bilateral Rehabilitation System for Hand and Wrist Joints
 ,
,
Abstract
:1. Introduction
- Combination of soft hand-and-wrist exoskeletons for achieving necessary coordinated motion.
- Bilateral therapy of combined hand and wrist joints.
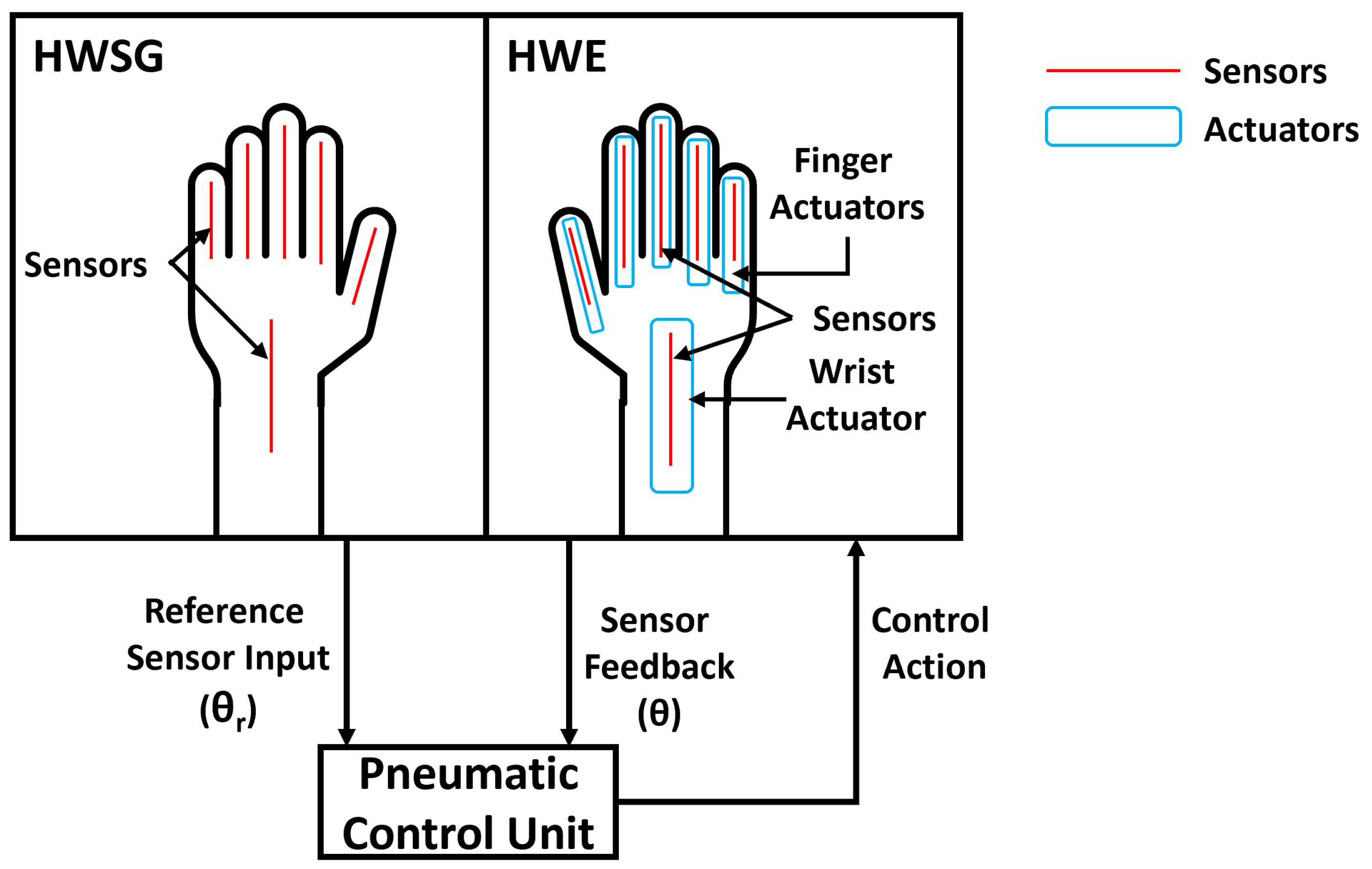
2. Bilateral Therapy System
2.1. Hand-and-Wrist Sensor Glove
2.2. Hand-and-Wrist Exoskeleton
2.3. Pneumatic Control Unit
3. Control Algorithm
4. Experimental Setup
4.1. Materials
4.2. Methods
4.2.1. Wrist Exercise with Dumbbell
4.2.2. Object Pick-and-Place Task
5. Results and Discussion
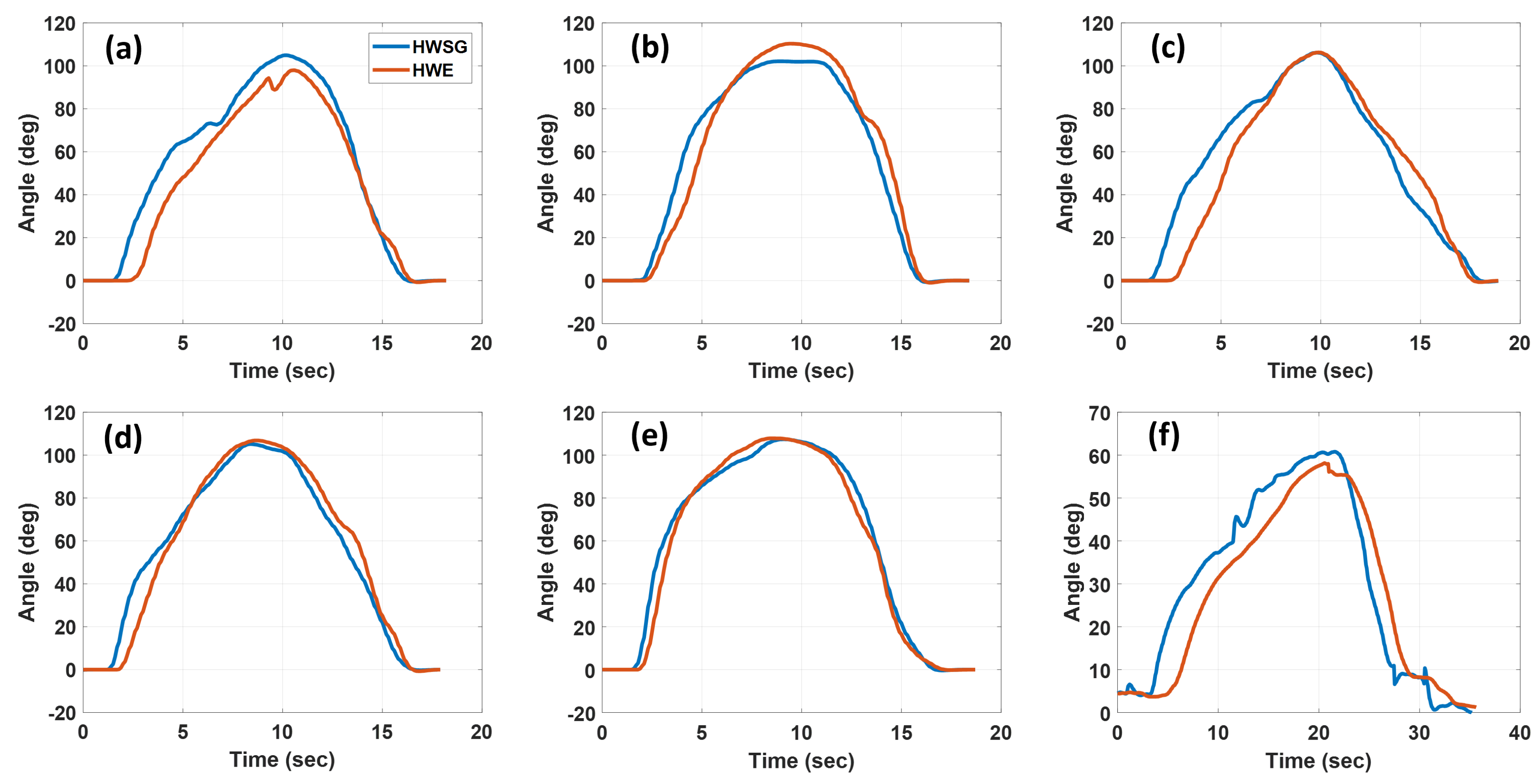
5.1. Wrist Exercise with Dumbbell
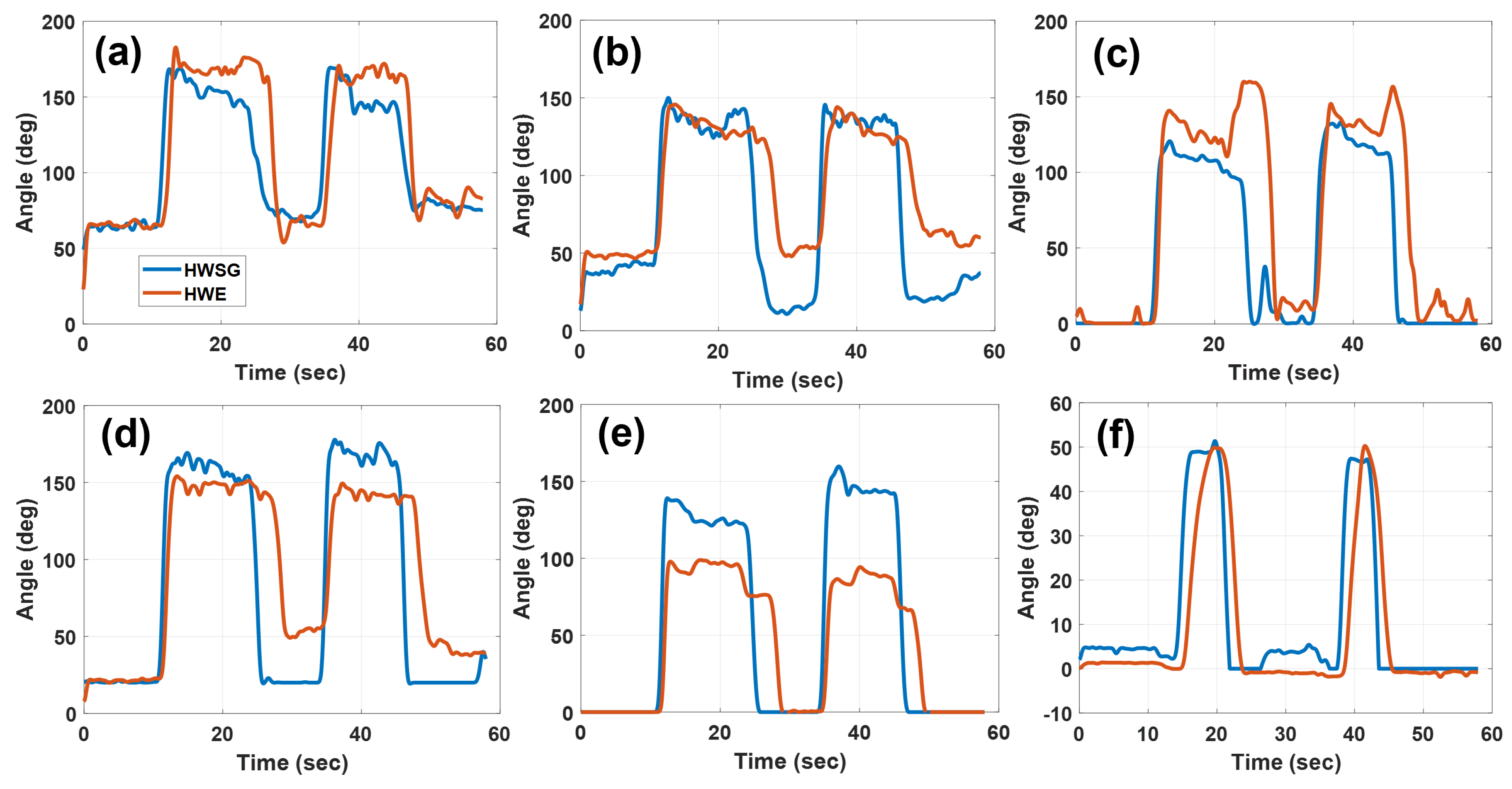
5.2. Object Pick-and-Place Task
5.3. Discussions
- Qualitatively, the graphs demonstrate that the fingers and wrist joints assisted by HWE followed the same trajectories as guided by the HWSG, which verifies the functionality of the bilateral therapy algorithm.
- In this work, the main focus was to show that the motions of both HWSG and HWE followed a similar trajectory during a rehabilitation task rather than error computation. Regardless, discrepancies between the reference () and measured () angles were observed in some joints and could be attributed to the nature of the experiment. In this work, a human controlled the sensor glove, and object manipulation was involved in the experiments. Therefore, the user had no sense of how much angle to move their fingers in order for the HWE to grab an object. The joint angles in HWSG could move to higher angles than HWE, as there was no object present in the HWSG hand to interfere with the joint motion. However, a similar bilateral soft robotic system for the hand (wrist excluded) was tested in our previous work [16] and showed minimal error between the angular motion of the sensor glove versus the robotic glove while both gloves were attached to artificial hand models.
- It was observed that the gaps (angle difference) between the angles recorded by the HWSG and HWE were greater in the thumb actuators than in all other actuators (Figure 10e and Figure 12e). This was because the user was holding either a dumbbell or an object in the HWE hand, which restricted the movement of the thumb once it touched the object, whereas, in the case of the HWSG hand, there was no object to restrict the movement.
- Results from both applications show that all the finger actuators inflated quicker than the wrist actuator. This was because finger actuators have a very small volume to be filled compared to that of the wrist actuator. This situation can be resolved by using a bigger proportional valve for the wrist actuator.
- In the case of deflation, finger actuators deflated slower than the wrist actuator. This was because the orifice size of the proportional valves used to deflate the finger actuators was small in comparison to the proportional valve used for the wrist actuator. For the fingers and wrist actuators, the orifice sizes of proportional valves were 0.25 mm (Parker-910-000042-030) and 1.02 mm (Parker-910-000045-030), respectively. Conductivity (C) of a pipe under vacuum flow is given as [22],where C, d, l, and p are conductivity, diameter of pipe, length, and air pressure, respectively. From Equation (4) and the diameters of the proportional valves (0.25 mm for fingers and 1.02 mm for wrist actuator), it is clear that flow is approximately times higher for the wrist actuator during deflation.
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| HWSG | Hand-and-wrist sensor glove |
| HWE | Hand-and-wrist exoskeleton |
| PD | Proportional derivative |
| ADC | Analog-to-digital converter |
| ROM | Range of motion |
| PWM | Pulse width modulation |
References
- Nogueira, N.G.D.H.M.; Parma, J.O.; de Assis Leão, S.E.S.; de Souza Sales, I.; Macedo, L.C.; Galvão, A.C.D.R.; de Oliveira, D.C.; Murça, T.M.; Fernandes, L.A.; Junqueira, C.; et al. Mirror therapy in upper limb motor recovery and activities of daily living, and its neural correlates in stroke individuals: A systematic review and meta-analysis. Brain Res. Bull. 2021, 177, 217–238. [Google Scholar] [CrossRef] [PubMed]
- Thieme, H.; Morkisch, N.; Mehrholz, J.; Pohl, M.; Behrens, J.; Borgetto, B.; Dohle, C. Mirror therapy for improving motor function after stroke. Cochrane Database Syst. Rev. 2018, 7, CD008449. [Google Scholar] [CrossRef] [PubMed]
- Yuan, R.; Qiao, X.; Tang, C.; Zhou, T.; Chen, W.; Song, R.; Jiang, Y.; Reinhardt, J.D.; Wang, H. Effects of Uni-vs. Bilateral Upper Limb Robot-Assisted Rehabilitation on Motor Function, Activities of Daily Living, and Electromyography in Hemiplegic Stroke: A Single-Blinded Three-Arm Randomized Controlled Trial. J. Clin. Med. 2023, 12, 2950. [Google Scholar] [CrossRef] [PubMed]
- Winstein, C.; Varghese, R. Been there, done that, so what’s next for arm and hand rehabilitation in stroke? NeuroRehabilitation 2018, 43, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Lo, A.C.; Guarino, P.D.; Richards, L.G.; Haselkorn, J.K.; Wittenberg, G.F.; Federman, D.G.; Ringer, R.J.; Wagner, T.H.; Krebs, H.I.; Volpe, B.T.; et al. Robot-assisted therapy for long-term upper-limb impairment after stroke. N. Engl. J. Med. 2010, 362, 1772–1783. [Google Scholar] [CrossRef] [PubMed]
- Beom, J.; Koh, S.; Nam, H.S.; Kim, W.; Kim, Y.; Seo, H.G.; Oh, B.M.; Chung, S.G.; Kim, S. Robotic mirror therapy system for functional recovery of hemiplegic arms. JoVE (J. Vis. Exp.) 2016, 114, e54521. [Google Scholar]
- Nam, H.S.; Koh, S.; Beom, J.; Kim, Y.J.; Park, J.W.; Koh, E.S.; Chung, S.G.; Kim, S. Recovery of proprioception in the upper extremity by robotic mirror therapy: A clinical pilot study for proof of concept. J. Korean Med. Sci. 2017, 32, 1568–1575. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.Y.; Yang, C.L.; Chen, M.D.; Lin, K.C.; Wu, L.L. Unilateral versus bilateral robot-assisted rehabilitation on arm-trunk control and functions post stroke: A randomized controlled trial. J. Neuroeng. Rehabil. 2013, 10, 35. [Google Scholar] [CrossRef] [PubMed]
- Moggio, L.; de Sire, A.; Marotta, N.; Demeco, A.; Ammendolia, A. Exoskeleton versus end-effector robot-assisted therapy for finger-hand motor recovery in stroke survivors: Systematic review and meta-analysis. Top. Stroke Rehabil. 2022, 29, 539–550. [Google Scholar] [CrossRef] [PubMed]
- Gassert, R.; Dietz, V. Rehabilitation robots for the treatment of sensorimotor deficits: A neurophysiological perspective. J. Neuroeng. Rehabil. 2018, 15, 46. [Google Scholar] [CrossRef] [PubMed]
- Ueki, S.; Kawasaki, H.; Ito, S.; Nishimoto, Y.; Abe, M.; Aoki, T.; Ishigure, Y.; Ojika, T.; Mouri, T. Development of a hand-assist robot with multi-degrees-of-freedom for rehabilitation therapy. IEEE/ASME Trans. Mechatron. 2010, 17, 136–146. [Google Scholar] [CrossRef]
- De la Cruz-Sánchez, B.A.; Arias-Montiel, M.; Lugo-González, E. EMG-controlled hand exoskeleton for assisted bilateral rehabilitation. Biocybern. Biomed. Eng. 2022, 42, 596–614. [Google Scholar] [CrossRef]
- Maciejasz, P.; Eschweiler, J.; Gerlach-Hahn, K.; Jansen-Troy, A.; Leonhardt, S. A survey on robotic devices for upper limb rehabilitation. J. Neuroeng. Rehabil. 2014, 11, 3. [Google Scholar] [CrossRef] [PubMed]
- Polygerinos, P.; Wang, Z.; Galloway, K.C.; Wood, R.J.; Walsh, C.J. Soft robotic glove for combined assistance and at-home rehabilitation. Robot. Auton. Syst. 2015, 73, 135–143. [Google Scholar] [CrossRef]
- Haghshenas-Jaryani, M.; Patterson, R.M.; Bugnariu, N.; Wijesundara, M.B. A pilot study on the design and validation of a hybrid exoskeleton robotic device for hand rehabilitation. J. Hand Ther. 2020, 33, 198–208. [Google Scholar] [CrossRef] [PubMed]
- Haghshenas-Jaryani, M.; Pande, C.; Wijesundara, B.M. Soft robotic bilateral hand rehabilitation system for fine motor learning. In Proceedings of the 2019 IEEE 16th International Conference on Rehabilitation Robotics (ICORR), Toronto, ON, Canada, 24–28 June 2019; pp. 337–342. [Google Scholar]
- Ma, D.; Li, X.; Xu, Q.; Yang, F.; Feng, Y.; Wang, W.; Huang, J.J.; Pei, Y.C.; Pan, Y. Robot-Assisted Bimanual Training Improves Hand Function in Patients with Subacute Stroke: A Randomized Controlled Pilot Study. Front. Neurol. 2022, 13, 884261. [Google Scholar] [CrossRef] [PubMed]
- Haghshenas-Jaryani, M.; Nothnagle, C.; Patterson, R.M.; Bugnariu, N.; Wijesundara, M.B. Soft robotic rehabilitation exoskeleton (rehab glove) for hand therapy. In Proceedings of the International Design Engineering Technical Conferences and Computers and Information in Engineering Conference, Cleveland, OH, USA, 6–9 August 2017; Volume 58158, p. V003T13A005. [Google Scholar]
- Singh, I.; Erel, V.; Gu, Y.; Lindsay, A.R.; Patterson, R.M.; Swank, C.; Wijesundara, M.B. Development of Soft Pneumatic Actuator Based Wrist Exoskeleton for Assistive Motion. In Proceedings of the 2023 IEEE/ASME International Conference on Advanced Intelligent Mechatronics (AIM), Seattle, WA, USA, 28–30 June 2023; pp. 359–366. [Google Scholar]
- Mikova, L.; Gmiterko, A.; Hroncova, D. State space representation of dynamical systems. Am. J. Mech. Eng. 2016, 4, 385–389. [Google Scholar]
- Van Overschee, P.; De Moor, B. Subspace Identification for Linear Systems: Theory—Implementation—Applications; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Conductance. Available online: https://www.pfeiffer-vacuum.com/en/know-how/introduction-to-vacuum-technology/fundamentals/conductance/ (accessed on 1 October 2023).













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Component Name | Model | Dimensions (L × W × H) mm | Weight (g) |
|---|---|---|---|
| Pump | Parker D1020-23-01 | 85 × 30 × 75 | 257.48 |
| Solenoid Valve (Fingers) | Clippard E210C | 45 × 15 × 20 | 10.01 |
| Solenoid Valve (Wrist) | Clippard E210H | 45 × 15 × 20 | 9.91 |
| Proportional Valve (Fingers) | Parker 910-000042-030 | 30 × 10 × 20 | 47.00 |
| Proportional Valve (Wrist) | Parker 910-000045-030 | 30 × 10 × 20 | 47.00 |
| Pressure Sensor (Range: 0 to 206.84 kPa) | Honeywell ABPMANN004BGAA5 | 7.3 × 6.3 × 18.6 | 7.08 |
| Vacuum Sensor (Range: −115 to 0 kPa) | NXP MPXV6115V | 18.01 × 10.54 × 5.38 | 1.30 |
| Microcontroller | ESP-32 | 50 × 25 × 10 | 10.46 |
| Thumb Actuator | 5.5 | 4 |
| Index Actuator | 4.5 | 3.4 |
| Middle Actuator | 5.8 | 4.6 |
| Ring Actuator | 4.5 | 3.4 |
| Little Actuator | 5.2 | 4.1 |
| Wrist Actuator | 8.1 | 6.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ridremont, T.; Singh, I.; Bruzek, B.; Erel, V.; Jamieson, A.; Gu, Y.; Merzouki, R.; Wijesundara, M.B.J. Soft Robotic Bilateral Rehabilitation System for Hand and Wrist Joints. Machines 2024, 12, 288. https://0-doi-org.brum.beds.ac.uk/10.3390/machines12050288
Ridremont T, Singh I, Bruzek B, Erel V, Jamieson A, Gu Y, Merzouki R, Wijesundara MBJ. Soft Robotic Bilateral Rehabilitation System for Hand and Wrist Joints. Machines. 2024; 12(5):288. https://0-doi-org.brum.beds.ac.uk/10.3390/machines12050288
Chicago/Turabian StyleRidremont, Tanguy, Inderjeet Singh, Baptiste Bruzek, Veysel Erel, Alexandra Jamieson, Yixin Gu, Rochdi Merzouki, and Muthu B. J. Wijesundara. 2024. "Soft Robotic Bilateral Rehabilitation System for Hand and Wrist Joints" Machines 12, no. 5: 288. https://0-doi-org.brum.beds.ac.uk/10.3390/machines12050288