
Involvement of Mast Cells in the Pathology of COVID-19: Clinical and Laboratory Parallels
 , , , , ,
, , , , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Laboratory Analyses
2.3. Histological Analyses
2.4. Statistical Analysis
3. Results
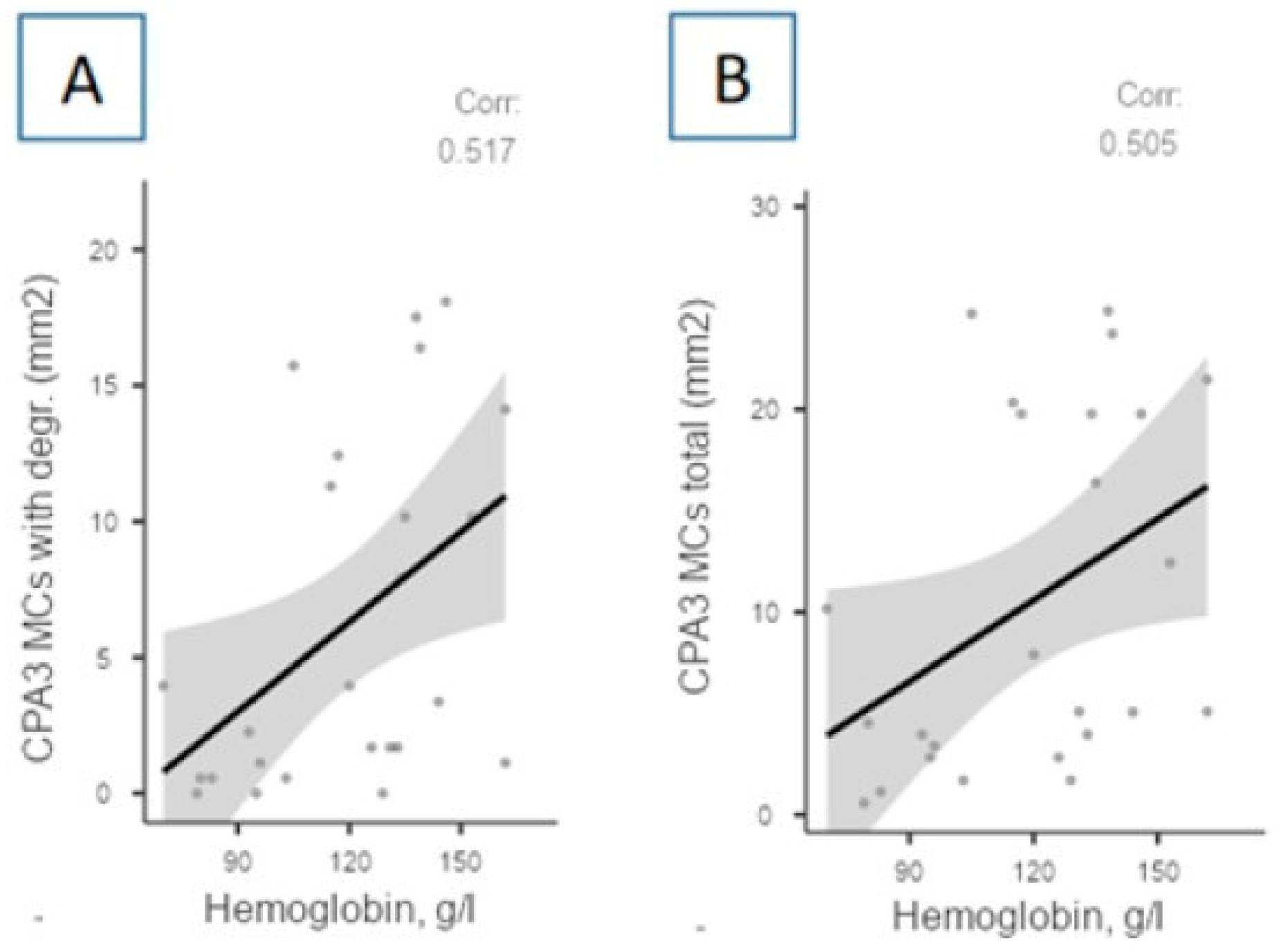
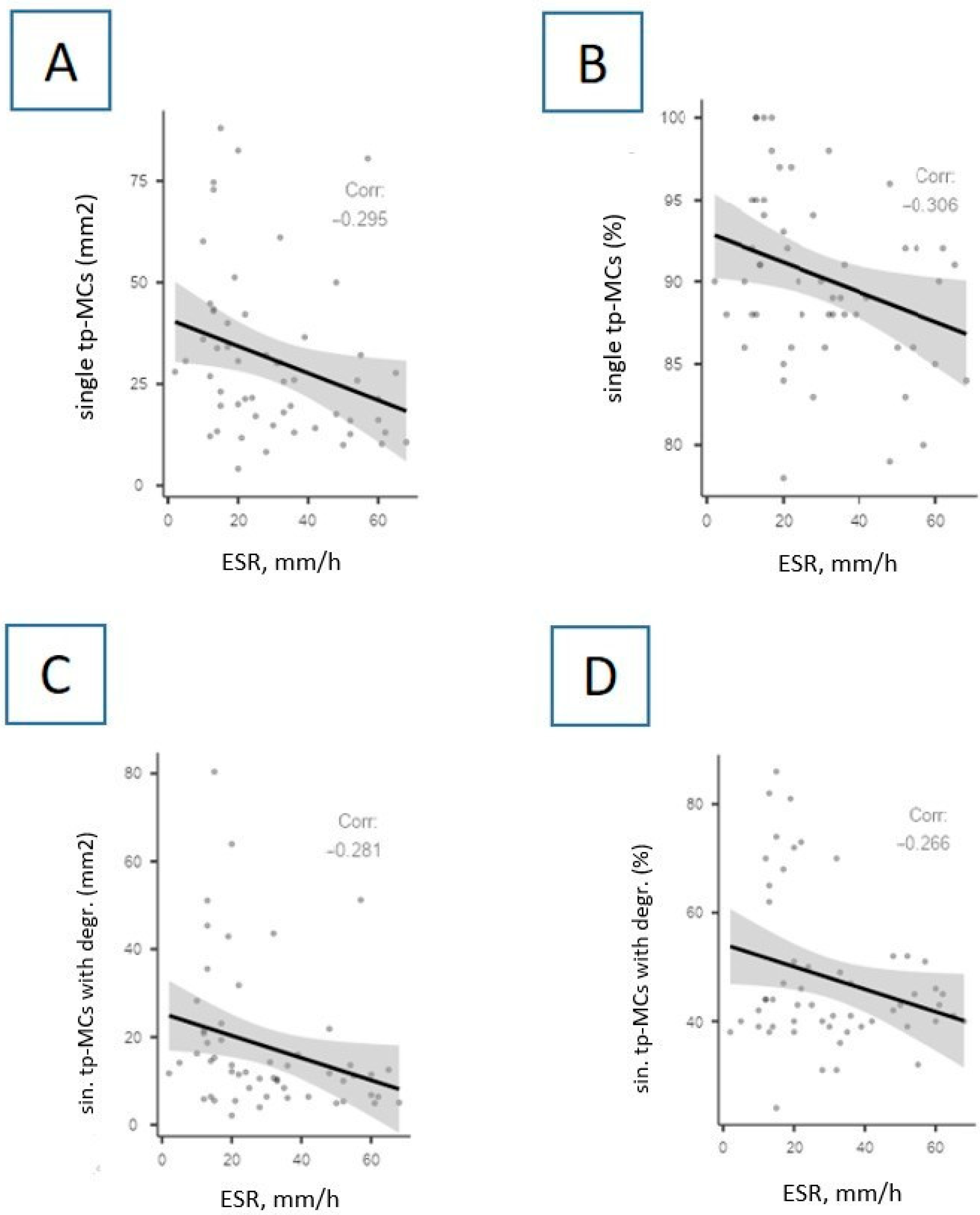
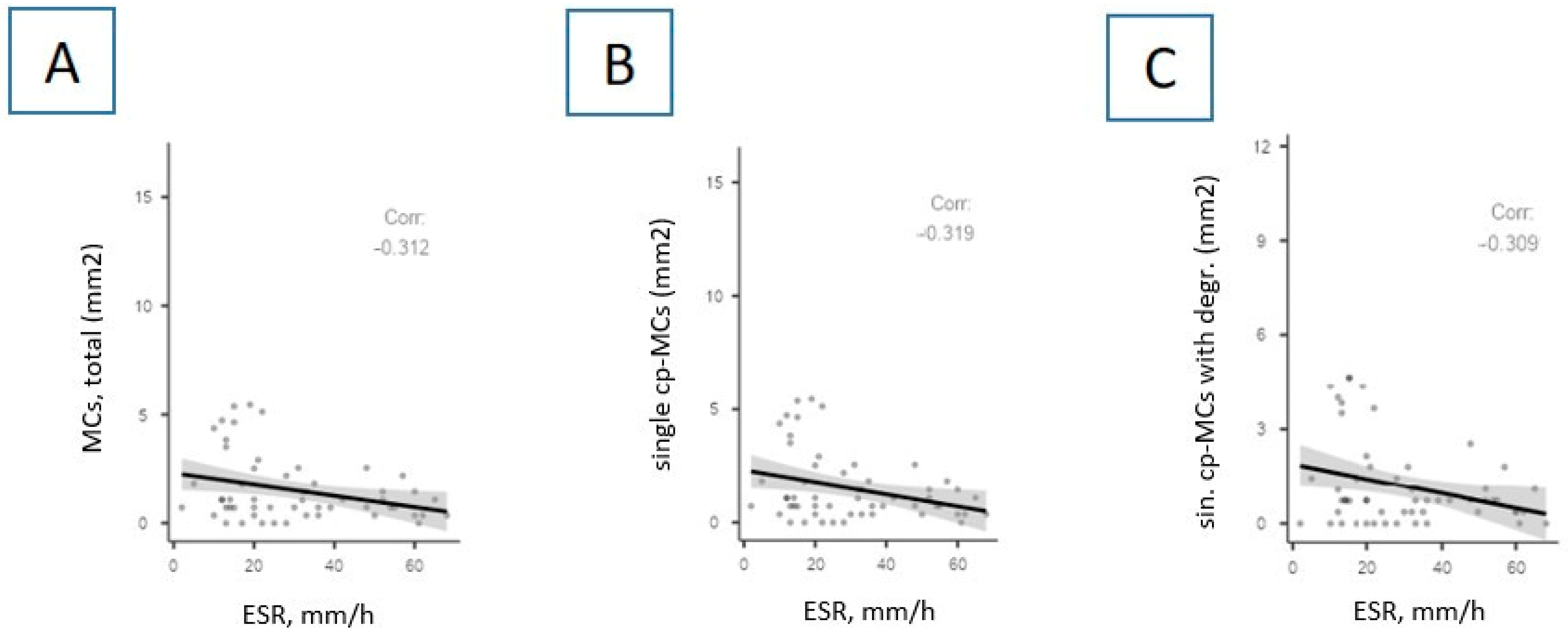
3.1. The Relationship between MCs and General Blood Test Parameters
3.2. MCs and C-Reactive Protein
3.3. MCs and Coagulogram Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COVID-19 | coronavirus disease 2019 |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus-2 |
| ARDS | acute respiratory distress syndrome |
| MCs | mast cells |
| COPD | chronic obstructive pulmonary disease |
| TNF-α | tumor necrosis factor alpha |
| IL | interleukin |
| CPA3 | carboxypeptidase A3 |
| CKD | chronic kidney disease |
| GFR | glomerular filtration rate |
| ESR | erythrocyte sedimentation rate |
| aPTT | activated partial thromboplastin time |
| PTI | prothrombin index |
| INR | international normalized ratio |
| CRP | C-reactive protein |
| Me | median |
| CHD | coronary heart disease |
| CHF | chronic heart failure |
| NIV | non-invasive ventilation |
| IMV | invasive mechanical ventilation |
| GBT | general blood test |
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/#:~:text=Globally%2C%20as%20of%205%3A57pm%20CEST%2C,6%2C974%2C473%20deaths%2C%20reported%20to%20WHO (accessed on 2 November 2023).
- Zanza, C.; Romenskaya, T.; Manetti, A.C.; Franceschi, F.; La Russa, R.; Bertozzi, G.; Maiese, A.; Savioli, G.; Volonnino, G.; Longhitano, Y. Cytokine Storm in COVID-19: Immunopathogenesis and Therapy. Medicina 2022, 58, 144. [Google Scholar] [CrossRef] [PubMed]
- Karki, R.; Kanneganti, T.D. Innate immunity, cytokine storm, and inflammatory cell death in COVID-19. J. Transl. Med. 2022, 20, 542. [Google Scholar] [CrossRef] [PubMed]
- Brock, I.; Maitland, A. Mast Cells and COVID-19: A case report implicating a role of mast cell activation in the prevention and treatment of COVID-19. J. Vaccines Vaccin. 2021, 36–39. [Google Scholar] [CrossRef]
- Potapnev, M.P. Cytokine storm. Causes and consequences. Immunol.-Immunol. 2021, 42, 175–188. [Google Scholar]
- Budnevsky, A.V.; Avdeev, S.N.; Kosanovic, D.; Shishkina, V.V.; Filin, A.A.; Esaulenko, D.I.; Ovsyannikov, E.S.; Samoylenko, T.V.; Redkin, A.N.; Suvorova, O.A.; et al. Role of mast cells in the pathogenesis of severe lung damage in COVID-19 patients. Respir. Res 2022, 23, 371. [Google Scholar] [CrossRef] [PubMed]
- Atyakshin, D.A.; Bukhvalov, I.B.; Timann, M. Mast cell proteases in specific tissular microenvironment formation: Pathogenetic and diagnostical aspects. Therapiya-Therapy 2018, 6, 128–140. [Google Scholar] [CrossRef]
- Sutanto, H. Mechanobiology of Type 1 hypersensitivity: Elucidating the impacts of mechanical forces in allergic reactions. Mechanobiol. Med. 2024, 2, 100041. [Google Scholar] [CrossRef]
- Theoharides, T.C. COVID-19, pulmonary mast cells, cytokine storms, and beneficial actions of luteolin. Biofactors 2020, 46, 306–308. [Google Scholar] [CrossRef] [PubMed]
- Company, C.; Piqueras, L.; Naim Abu Nabah, Y.; Escudero, P.; Blanes, J.I.; Jose, P.J.; Morcillo, E.J.; Sanz, M.J. Contributions of ACE and mast cell chymase to endogenous angiotensin II generation and leucocyte recruitment in vivo. Cardiovasc. Res. 2011, 92, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Budnevsky, A.V.; Ovsyannikov, E.S.; Shishkina, V.V.; Esaulenko, D.I.; Shumilovich, B.R.; Savushkina, I.A.; Alekseeva, N.G. Possible Unexplored Aspects of Covid-19 Pathogenesis: The Role of Carboxypeptidase A3. Int. J. Biomed. 2022, 12, 179–182. [Google Scholar] [CrossRef]
- Budnevsky, A.V.; Avdeev, S.N.; Ovsyannikov, E.S.; Shishkina, V.V.; Esaulenko, D.I.; Filin, A.A.; Savushkina, I.A.; Perveeva, I.M.; Alekseeva, N.G. The role of mast cells and their proteases in lung damage associated with COVID-19. Pul’monologiya 2023, 33, 17–26. [Google Scholar] [CrossRef]
- Motta Junior, J.D.S.; Miggiolaro, A.F.R.D.S.; Nagashima, S.; de Paula, C.B.V.; Baena, C.P.; Scharfstein, J.; de Noronha, L. Mast cells in alveolar septa of COVID-19 patients: A pathogenic pathway that may link interstitial edema to immunothrombosis. Front. Immunol. 2020, 11, 574862. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Ren, L.; Zhang, L.; Zhong, J.; Xiao, Y.; Jia, Z.; Guo, L.; Yang, J.; Wang, C.; Jiang, S.; et al. Heightened innate immune responses in the respiratory tract of COVID-19 patients. Cell. Host. Microbe 2020, 27, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Gebremeskel, S.; Schanin, J.; Coyle, K.M.; Butuci, M.; Luu, T.; Brock, E.C.; Xu, A.; Wong, A.; Leung, J.; Korver, W.; et al. Mast cell and eosinophil activation are associated with COVID-19 and TLR-mediated viral inflammation: Implications for an Anti-Siglec-8 antibody. Front. Immunol. 2021, 12, 650331. [Google Scholar] [CrossRef]
- Tan, J.; Anderson, D.E.; Rathore, A.P.S.; O’Neill, A.; Mantri, C.K.; Saron, W.A.A.; Lee, C.; Cui, C.W.; Kang, A.E.Z.; Foo, R.; et al. Signatures of mast cell activation are associated with severe COVID-19. MedRxiv 2021. [Google Scholar] [CrossRef]
- Suttle, M.M.; Harvima, I.T. Mast cell chymase in experimentally induced psoriasis. J. Dermatol. 2016, 43, 693–696. [Google Scholar] [CrossRef] [PubMed]
- Dell’Italia, L.J.; Collawn, J.F.; Ferrario, C.M. Multifunctional role of chymase in acute and chronic tissue injury and remodeling. Circ. Res. 2018, 122, 319–336. [Google Scholar] [CrossRef] [PubMed]
- Soria-Castro, R.; Meneses-Preza, Y.G.; Rodríguez-López, G.M.; Romero-Ramírez, S.; Sosa-Hernández, V.A.; Cervantes-Díaz, R.; Pérez-Fragoso, A.; Torres-Ruíz, J.J.; Gómez-Martín, D.; Campillo-Navarro, M.; et al. Severe COVID-19 is marked by dysregulated serum levels of carboxypeptidase A3 and serotonin. J. Leukoc. Biol. 2021, 110, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Vliagoftis, H.; Lacy, P.; Luy, B.; Adamko, D.; Hollenberg, M.; Befus, D.; Moqbel, R. Mast cell tryptase activates peripheral blood eosinophils to release granule-associated enzymes. Int. Arch. Allergy Immunol. 2004, 135, 196–204. [Google Scholar] [CrossRef]
- Abonia, J.P.; Blanchard, C.; Butz, B.B.; Rainey, H.F.; Collins, M.H.; Stringer, K.; Putnam, P.E.; Rothenberg, M.E. Involvement of mast cells in eosinophilic esophagitis. J. Allergy Clin. Immunol. 2010, 126, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, R.H.; Sidhu, S.S.; Raman, K.; Solon, M.; Solberg, O.D.; Caughey, G.H.; Woodruff, P.G.; Fahy, J.V. Accumulation of intraepithelial mast cells with a unique protease phenotype in T(H)2-high asthma. J. Allergy Clin. Immunol. 2010, 125, 1046–1053. [Google Scholar] [CrossRef] [PubMed]
- Takabayashi, T.; Kato, A.; Peters, A.T.; Suh, L.A.; Carter, R.; Norton, J.; Grammer, L.C.; Tan, B.K.; Chandra, R.K.; Conley, D.B.; et al. Glandular mast cells with distinct phenotype are highly elevated in chronic rhinosinusitis with nasal polyps. J. Allergy Clin. Immunol. 2012, 130, 410–420. [Google Scholar] [CrossRef] [PubMed]
- Jafarzadeh, A.; Chauhan, P.; Saha, B.; Jafarzadeh, S.; Nemati, M. Contribution of monocytes and macrophages to the local tissue inflammation and cytokine storm in COVID-19: Lessons from SARS and MERS, and potential therapeutic interventions. Life Sci. 2020, 257, 118102. [Google Scholar] [CrossRef] [PubMed]
- Thomas, T.; Stefanoni, D.; Dzieciatkowska, M.; Issaian, A.; Nemkov, T.; Hill, R.C.; Francis, R.O.; Hudson, K.E.; Buehler, P.W.; Zimring, J.C.; et al. Evidence of Structural Protein Damage and Membrane Lipid Remodeling in Red Blood Cells from COVID-19 Patients. J. Proteome Res. 2020, 19, 4455–4469. [Google Scholar] [CrossRef]
- Palladino, M. Complete blood count alterations in COVID-19 patients: A narrative review. Biochem. Med. 2021, 31, 030501. [Google Scholar] [CrossRef]
- Prieto-García, A.; Zheng, D.; Adachi, R.; Xing, W.; Lane, W.S.; Chung, K.; Anderson, P.; Hansbro, P.M.; Castells, M.; Stevens, R.L. Mast cell restricted mouse and human tryptase·heparin complexes hinder thrombin-induced coagulation of plasma and the generation of fibrin by proteolytically destroying fibrinogen. J. Biol. Chem. 2012, 287, 7834–7844. [Google Scholar] [CrossRef] [PubMed]
- Sutanto, H.; Soegiarto, G. Risk of Thrombosis during and after a SARS-CoV-2 Infection: Pathogenesis, Diagnostic Approach, and Management. Hematol. Rep. 2023, 15, 225–243. [Google Scholar] [CrossRef] [PubMed]
- Soni, M.; Gopalakrishnan, R.; Vaishya, R.; Prabu, P. D-dimer level is a useful predictor for mortality in patients with COVID-19: Analysis of 483 cases. Diabetes Metab. Syndr. 2020, 14, 2245–2249. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | COVID-19 Group | The Control Group |
|---|---|---|
| Number of subjects | 55 | 30 |
| Male, n (%) | 29 (53) | 16 (53) |
| Female, n (%) | 26 (47) | 14 (47) |
| Age, years | 67 [62; 71] | 64.5 [58; 70] |
| PCR SARS-CoV-2 «+», n (%) | 55 (100) | 0 (0) |
| Bilateral pneumonia, n (%) | 55 (100) | 0 (0) |
| ARDS, n (%) | 55 (100) | 0 (0) |
| Arterial hypertension, n (%) | 45 (82) | 25 (83) |
| Coronary heart disease, n (%) | 6 (11) | 4 (13) |
| Ischemic brain stroke, n (%) | 10 (18) | 5 (17) |
| Chronic heart failure (CHF), n (%) | 15 (27) | 9 (30) |
| Obesity, n (%) | 14 (25) | 8 (27) |
| I degree | 11 (20) | 5 (17) |
| II degree | 1 (2) | 1 (3) |
| III degree | 2 (4) | 2 (7) |
| Chronic kidney disease, n (%) (C1–C2 stages) | 11 (20) | 7 (23) |
| COVID-19 Group, Number of MCs per mm2 | The Control Group, Number of MCs per mm2 | p-Test Value | COVID-19 Group, % MCs | The Control Group, % MCs | p-Test Value | |
|---|---|---|---|---|---|---|
| Single tryptase + MCs without degranulation | 10.4 [7.13; 18.9] | 1.78 [1.17; 2.22] | <0.001 | 46.43 [35.31; 50.32] | 7.97 [6.44; 11.1] | <0.001 |
| Single tryptase + MCs with degranulation | 12.0 [6.61; 20.12] | 14.78 [10.41; 19.91] | 0.408 | 43.02 [39.51; 51.11] | 72.13 [65.21; 77.21] | <0.001 |
| Single tryptase + MCs total | 26.0 [16.1; 38.3] | 16.78 [12.82; 22.5] | 0.005 | 89.84 [86.91; 93.92] | 81.94 [73.1; 86.72] | <0.001 |
| Co-adjacent tryptase + MCs without degranulation | 0.53 [0.07; 0.8] | 0 [0; 0.44] | <0.001 | 2.02 [0.23; 3.81] | 0 [0; 0.61] | <0.001 |
| Co-adjacent tryptase + MCs with degranulation | 0.53 [0.27; 0.8] | 0.56 [0.44; 1.33] | 0.061 | 2.13 [1.02; 3.45] | 3.77 [2.74; 5.23] | <0.001 |
| Co-adjacent tryptase + MCs total | 1.07 [0.53; 1.71] | 0.89 [0.44; 1.50] | 0.391 | 4.04 [2.71; 6.64] | 4.6 [3.71; 5.48] | 0.858 |
| Fragments of tryptase + MCs | 1.33 [0.67; 2.13] | 2.56 [1.39; 5.72] | <0.001 | 5.36 [3.17; 6.87] | 11.7 [9.84; 22.02] | <0.001 |
| Total amount of tryptase + MCs | 30.1 [18.2; 41.6] | 22.1 [15.2; 27.9] | 0.033 | - | - | - |
| COVID-19 Group, Number of MCs per mm2 | The Control Group, Number of MCs per mm2 | p-Test Value | COVID-19 Group, % MCs | The Control Group, % MCs | p-Test Value | |
|---|---|---|---|---|---|---|
| Single chymase + MCs without degranulation | 0 [0; 0.36] | 0.44 [0.13; 0.89] | <0.001 | 0 [0; 33.33] | 23.9 [16.81; 33.33] | 0.030 |
| Single chymase + MCs with degranulation | 0.73 [0.36; 1.45] | 1.2 [0.47; 2.76] | 0.048 | 75 [25; 100] | 65.1 [55.33; 71.51] | 0.123 |
| Single chymase + MCs total | 1.07 [0.36; 1.82] | 1.8 [0.7; 3.43] | 0.034 | 100 [100; 100] | 92.31 [81.81; 100] | <0.001 |
| Co-adjacent chymase + MCs without degranulation | 0 [0; 0] | 0 [0; 0] | 0.184 | 0 [0; 0] | 0 [0; 0] | 0.184 |
| Co-adjacent chymase + MCs with degranulation | 0 [0; 0] | 0 [0; 0.08] | 0.011 | 0 [0; 0] | 0 [0; 1.5] | 0.013 |
| Co-adjacent chymase + MCs total | 0 [0; 0] | 0 [0; 0.08] | 0.011 | 0 [0; 0] | 0 [0; 1.5] | 0.013 |
| Fragments of chymase + MCs | 0 [0; 0] | 0.13 [0; 0.67] | <0.001 | 0 [0; 0] | 7.69 [0; 12.9] | <0.001 |
| Total amount of chymase + MCs | 1.07 [0.54; 2] | 1.87 [0.8; 4.57] | 0.013 | - | - | - |
| COVID-19 Group, Number of MCs per mm2 | The Control Group, Number of MCs per mm2 | p-Test Value | COVID-19 Group, % MCs | The Control Group, % MCs | p-Test Value | |
|---|---|---|---|---|---|---|
| Single CPA3 + MCs without degranulation | 4.35 [1.81; 7.21] | 3.48 [2.32; 4.11] | 0.796 | 47.22 [36.33; 66.66] | 60.38 [52.38; 80.14] | 0.072 |
| Single CPA3 + MCs with degranulation | 6.49 [1.12; 11.11] | 2.07 [1.01; 2.71] | <0.001 | 52.78 [33.33; 63.66] | 39.61 [19.85; 47.62] | 0.062 |
| Co-adjacent CPA3 + MCs total | 0.41 [0.11; 0.52] | 0.06 [0; 0.11] | <0.001 | 0 [0; 0.03] | 0 [0; 0] | 0.058 |
| Fragments of CPA3+ MCs | 1.52 [0.12; 2.31] | 1.27 [0.57; 1.71] | 0.779 | 10 [0; 19.0] | 23.05 [7.68; 34.5] | 0.099 |
| Total amount of CPA3 + MCs | 10.84 [3.51; 19.82] | 5.56 [4.22; 6.81] | 0.01 | - | - | - |
| Parameters | Single Tryptase + MCs without Degranulation, % | Single Tryptase + MCs with Degranulation, % | Single Tryptase + MCs Total, % | Co-AdjacentTryptase + MCs without Degranulation, % | Co-Adjacent Tryptase + MCs with Degranulation, % | Co-Adjacent Tryptase + MCs Total, % | Fragments of Tryptase + MCs, % |
|---|---|---|---|---|---|---|---|
| aPTT No. 1 **, s | 0.070 | −0.137 | −0.191 | 0.276 * | 0.161 | 0.283 * | 0.048 |
| aPTT No. 2 ***, s | 0.087 | −0.183 | −0.302 | 0.292 | 0.222 | 0.350 * | 0.157 |
| Fibrinogen No. 1 **, g/L | 0.087 | −0.209 | −0.353 * | 0.471 * | −0.022 | 0.333 * | 0.243 |
| Fibrinogen No. 2 ***, g/L | 0.141 | −0.221 | −0.241 | 0.232 | −0.021 | 0.167 | 0.218 |
| INR No. 1. ** | −0.093 | 0.018 | −0.150 | 0.283 | −0.056 | 0.204 | 0.039 |
| INR No. 2 *** | 0.212 | −0.231 | 0.035 | 0.306 | −0.181 | 0.077 | −0.191 |
| Prothrombin index No. 1. **, % | −0.219 | 0.236 | 0.066 | −0.147 | −0.077 | −0.115 | −0.013 |
| Prothrombin index No. 2 ***, % | −0.122 | 0.047 | −0.349 | 0.255 | 0.326 | 0.311 | 0.328 |
| Parameters | Single Chymase + MCs without Degranulation, % | Single Chymase + MCs with Degranulation, % | Single Chymase + MCs Total, % Abs. | Co-Adjacent Chymase + MCs without Degranulation, % Abs. | Co-Adjacent Chymase + MCs with Degranulation, % | Co-Adjacent Chymase + MCs Total, % | Fragments of Chymase + MCs, % | Total Amount of Chymase + MCs, Abs. |
|---|---|---|---|---|---|---|---|---|
| aPTT No. 1 **, s | −0.052 | 0.125 | 0.131 | - | 0.016 | 0.016 | −0.086 | 0.129 |
| aPTT No. 2 ***, s | −0.260 | 0.368 * | −0.082 | - | 0.055 | 0.055 | 0.095 | −0.077 |
| Fibrinogen No. 1 **, g/L | 0.186 | −0.146 | −0.404 * | - | 0.046 | 0.046 | 0.120 | −0.398 * |
| Fibrinogen No. 2 ***, g/L | 0.180 | −0.148 | −0.283 | - | −0.092 | −0.092 | - | −0.288 |
| INR No. 1 ** | −0.091 | 0.037 | 0.074 | - | 0.118 | 0.675 | - | 0.096 |
| INR No. 2 *** | −0.026 | 0.081 | 0.728 * | 0.744 * | - | - | - | 0.728 * |
| Prothrombin index No. 1 **, % | 0.022 | −0.285 | −0.159 | - | - | - | - | −0.159 |
| Prothrombin index No. 2 ***, % | −0.146 | 0.146 | 0.151 | - | - | - | - | 0.151 |
| Parameters | Single CPA3 + MCs without Degranulation, Abs. | Single CPA3 + MCs with Degranulation, Abs. | Fragments of CPA3 + MCs, Abs. | Co-Adjacent CPA3 + MCs Total, Abs. | Total Number of CPA3 + MCs, Abs. |
|---|---|---|---|---|---|
| aPTT No. 1 **, s | 0.260 | 0.304 * | 0.335 | −0.090 | 0.375 * |
| aPTT No. 2 ***, s | 0.025 | −0.182 | 0.238 | −0.260 | −0.003 |
| Fibrinogen No. 1 **, g/L | −0.112 | −0.106 | 0.038 | −0.300 | −0.102 |
| Fibrinogen No. 2 ***, g/L | −0.297 | −0.110 | −0.072 | 0.032 | −0.226 |
| INR No. 1 ** | −0.257 | 0.170 | 0.345 | 0.112 | −0.812 * |
| INR No. 2 *** | −0.232 | 0.218 | 0.418 | 0.245 | −0.453 |
| Prothrombin index No. 1 **, % | 0.249 | 0.068 | −0.093 | −0.134 | 0.270 |
| Prothrombin index No. 2 ***, % | 0.107 | −0.107 | 0.000 | −0.112 | 0.036 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Budnevsky, A.V.; Avdeev, S.N.; Kosanovic, D.; Ovsyannikov, E.S.; Savushkina, I.A.; Alekseeva, N.G.; Feigelman, S.N.; Shishkina, V.V.; Filin, A.A.; Esaulenko, D.I.; et al. Involvement of Mast Cells in the Pathology of COVID-19: Clinical and Laboratory Parallels. Cells 2024, 13, 711. https://0-doi-org.brum.beds.ac.uk/10.3390/cells13080711
Budnevsky AV, Avdeev SN, Kosanovic D, Ovsyannikov ES, Savushkina IA, Alekseeva NG, Feigelman SN, Shishkina VV, Filin AA, Esaulenko DI, et al. Involvement of Mast Cells in the Pathology of COVID-19: Clinical and Laboratory Parallels. Cells. 2024; 13(8):711. https://0-doi-org.brum.beds.ac.uk/10.3390/cells13080711
Chicago/Turabian StyleBudnevsky, Andrey V., Sergey N. Avdeev, Djuro Kosanovic, Evgeniy S. Ovsyannikov, Inessa A. Savushkina, Nadezhda G. Alekseeva, Sofia N. Feigelman, Viktoria V. Shishkina, Andrey A. Filin, Dmitry I. Esaulenko, and et al. 2024. "Involvement of Mast Cells in the Pathology of COVID-19: Clinical and Laboratory Parallels" Cells 13, no. 8: 711. https://0-doi-org.brum.beds.ac.uk/10.3390/cells13080711