
Intestinal Microbiome Associated with Efficacy of Atezolizumab and Bevacizumab Therapy for Hepatocellular Carcinoma
 , , , , , , ,
, , , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Treatment Response and Patient Groups
2.3. Survival Analysis
2.4. Ethics Approval
2.5. Patients
2.6. Treatment Protocol
2.7. Sample Collection and DNA Isolation
2.8. 16S rRNA Gene Sequencing
2.9. Statistical Analyses
3. Results
3.1. Patient Background
3.2. Microbiome Profiling and Comparison of Alpha and Beta Diversities
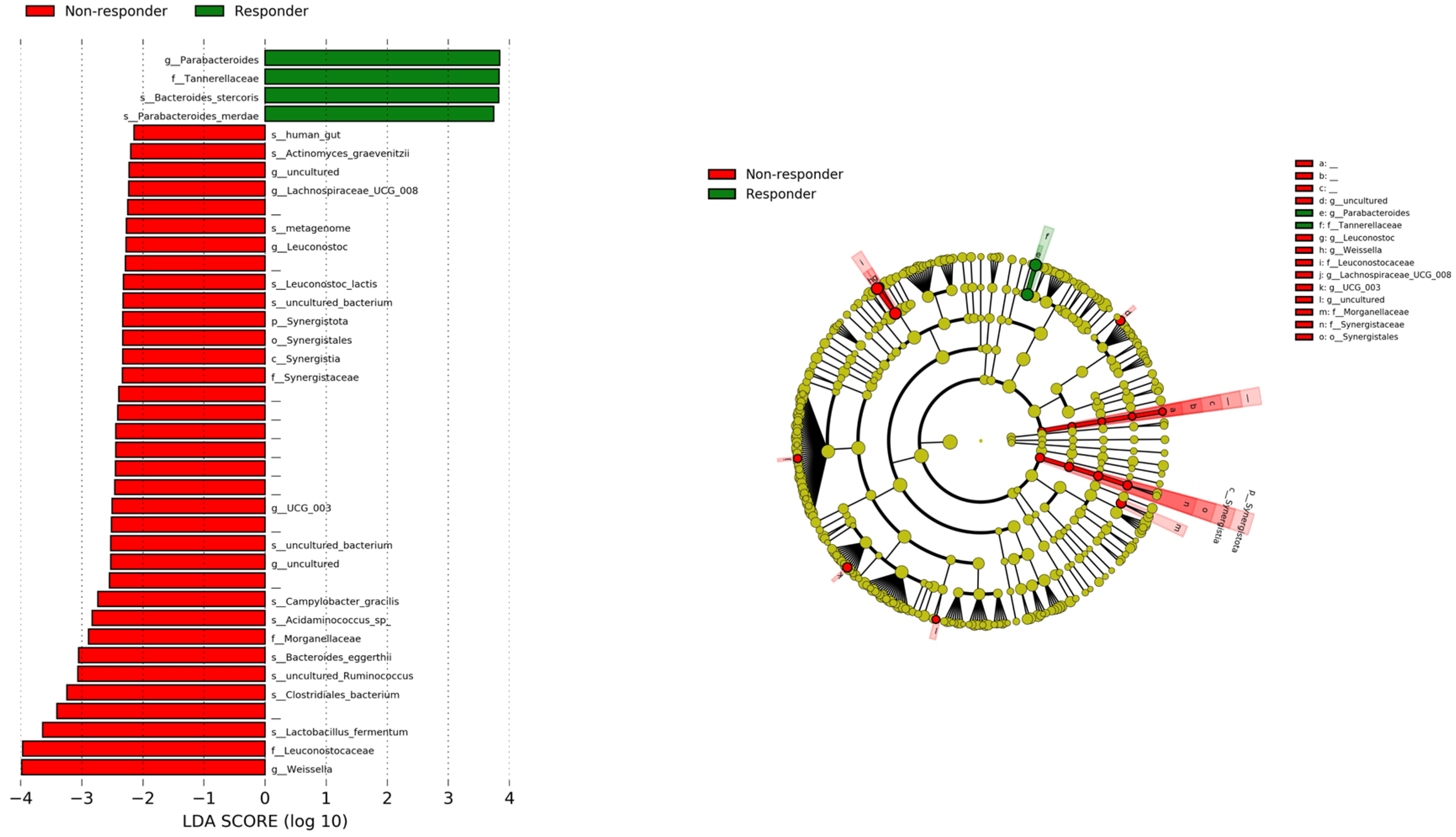
3.3. Comparison of Relative Abundance of Bacterial Communities between Responder and Non-Responder Groups with LEfSe
3.4. Comparison of Progression-Free Survival (PFS) and Overall Survival (OS)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, K.; Kudo, M.; Kawazoe, S.; Osaki, Y.; Ikeda, M.; Okusaka, T.; Tamai, T.; Suzuki, T.; Hisai, T.; Hayato, S.; et al. Phase 2 study of lenvatinib in patients with advanced hepatocellular carcinoma. J. Gastroenterol. 2016, 52, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.-H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef]
- Zhu, A.X.; Park, J.O.; Ryoo, B.-Y.; Yen, C.-J.; Poon, R.; Pastorelli, D.; Blanc, J.-F.; Chung, H.C.; Baron, A.D.; Pfiffer, T.E.F.; et al. Ramucirumab versus placebo as second-line treatment in patients with advanced hepatocellular carcinoma following first-line therapy with sorafenib (REACH): A randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2015, 16, 859–870. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.-L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.-Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.-W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Sharma, P.; Wagner, K.; Wolchok, J.D.; Allison, J.P. Novel cancer immunotherapy agents with survival benefit: Recent successes and next steps. Nat. Rev. Cancer 2011, 11, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.R.; Tykodi, S.S.; Chow, L.Q.M.; Hwu, W.-J.; Topalian, S.L.; Hwu, P.; Drake, C.G.; Camacho, L.H.; Kauh, J.; Odunsi, K.; et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N. Engl. J. Med. 2012, 366, 2455–2465. [Google Scholar] [CrossRef]
- Ansell, S.M.; Lesokhin, A.M.; Borrello, I.; Halwani, A.; Scott, E.C.; Gutierrez, M.; Schuster, S.J.; Millenson, M.M.; Cattry, D.; Freeman, G.J.; et al. PD-1 blockade with nivolumab in relapsed or refractory Hodgkin’s lymphoma. N. Engl. J. Med. 2015, 372, 311–319. [Google Scholar] [CrossRef]
- Schadendorf, D.; Hodi, F.S.; Robert, C.; Weber, J.S.; Margolin, K.; Hamid, O.; Patt, D.; Chen, T.-T.; Berman, D.M.; Wolchok, J.D. Pooled Analysis of Long-Term Survival Data From Phase II and Phase III Trials of Ipilimumab in Unresectable or Metastatic Melanoma. J. Clin. Oncol. 2015, 33, 1889–1894. [Google Scholar] [CrossRef]
- Paulos, C.M.; Wrzesinski, C.; Kaiser, A.; Hinrichs, C.S.; Chieppa, M.; Cassard, L.; Palmer, D.C.; Boni, A.; Muranski, P.; Yu, Z.; et al. Microbial translocation augments the function of adoptively transferred self/tumor-specific CD8+ T cells via TLR4 signaling. J. Clin. Investig. 2007, 117, 2197–2204. [Google Scholar] [CrossRef] [PubMed]
- Iida, N.; Dzutsev, A.; Stewart, C.A.; Smith, L.; Bouladoux, N.; Weingarten, R.A.; Molina, D.A.; Salcedo, R.; Back, T.; Cramer, S.; et al. Commensal bacteria control cancer response to therapy by modulating the tumor microenvironment. Science 2019, 342, 967–970. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.X.; Schwabe, R.F. The gut microbiome and liver cancer: Mechanisms and clinical translation. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 527–539. [Google Scholar] [CrossRef] [PubMed]
- Schwabe, R.F.; Greten, T.F. Gut microbiome in HCC—Mechanisms, diagnosis and therapy. J. Hepatol. 2020, 72, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Li, J.; Jin, C.; Yang, J.; Zheng, C.; Chen, K.; Xie, Y.; Yang, Y.; Bo, Z.; Wang, J.; et al. Association of gut microbiome and primary liver cancer: A two-sample Mendelian randomization and case-control study. Liver Int. 2022, 43, 221–233. [Google Scholar] [CrossRef]
- Zhang, L.; Chen, C.; Chai, D.; Li, C.; Guan, Y.; Liu, L.; Kuang, T.; Deng, W.; Wang, W. The association between antibiotic use and outcomes of HCC patients treated with immune checkpoint inhibitors. Front. Immunol. 2022, 13, 956533. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.C.; Wu, C.J.; Hung, Y.W.; Lee, C.J.; Chi, C.T.; Lee, I.C.; Kuo, Y.-L.; Chou, S.-H.; Luo, J.-C.; Hou, M.-C.; et al. Gut microbiota and metabolites associate with outcomes of immune checkpoint inhibitor-treated unresectable hepatocellular carcinoma. J. Immunother. Cancer 2022, 10, e004779. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Pugh, R.N.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [PubMed]
- Crabb, D.W.; Im, G.Y.; Szabo, G.; Mellinger, J.L.; Lucey, M.R. Diagnosis and Treatment of Alcohol-Associated Liver Diseases: 2019 Practice Guidance From the American Association for the Study of Liver Diseases. Hepatology 2020, 71, 306–333. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, K.; Kuzuya, T.; Honda, T.; Ito, T.; Ishizu, Y.; Nakamura, M.; Miyahara, R.; Kawashima, H.; Ishigami, M.; Fujishiro, M. Relationship Between Adverse Events and Microbiomes in Advanced Hepatocellular Carcinoma Patients Treated with Sorafenib. Anticancer Res. 2020, 40, 665–676. [Google Scholar] [CrossRef] [PubMed]
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumugam, M.; Asnicar, F.; et al. Author Correction: Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat. Biotechnol. 2019, 37, 1091. [Google Scholar] [CrossRef] [PubMed]
- Quast, C.; Pruesse, E.; Yilmaz, P.; Gerken, J.; Schweer, T.; Yarza, P.; Peplies, J.; Glöckner, F.O. The SILVA ribosomal RNA gene database project: Improved data processing and web-based tools. Nucleic Acids Res. 2013, 41, D590–D596. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Dhariwal, A.; Chong, J.; Habib, S.; King, I.L.; Agellon, L.B.; Xia, J. MicrobiomeAnalyst: A web-based tool for comprehensive statistical, visual and meta-analysis of microbiome data. Nucleic Acids Res. 2017, 45, W180–W188. [Google Scholar] [CrossRef] [PubMed]
- Segata, N.; Izard, J.; Waldron, L.; Gevers, D.; Miropolsky, L.; Garrett, W.S.; Huttenhower, C. Metagenomic biomarker discovery and explanation. Genome Biol. 2011, 12, R60. [Google Scholar] [CrossRef] [PubMed]
- Valero, C.; Lee, M.; Hoen, D.; Weiss, K.; Kelly, D.W.; Adusumilli, P.S.; Paik, P.K.; Plitas, G.; Ladanyi, M.; Postow, M.A.; et al. Pretreatment neutrophil-to-lymphocyte ratio and mutational burden as biomarkers of tumor response to immune checkpoint inhibitors. Nat. Commun. 2021, 12, 729. [Google Scholar] [CrossRef]
- Andrews, M.C.; Duong, C.P.M.; Gopalakrishnan, V.; Iebba, V.; Chen, W.-S.; Derosa, L.; Khan, A.W.; Cogdill, A.P.; White, M.G.; Wong, M.C.; et al. Gut microbiota signatures are associated with toxicity to combined CTLA-4 and PD-1 blockade. Nat. Med. 2021, 27, 1432–1441. [Google Scholar] [CrossRef]
- Song, P.; Yang, D.; Wang, H.; Cui, X.; Si, X.; Zhang, X.; Zhang, L. Relationship between intestinal flora structure and metabolite analysis and immunotherapy efficacy in Chinese NSCLC patients. Thorac. Cancer 2020, 11, 1621–1632. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, Y.; Bolgarina, Z.; Desai, H.N.; Senaratne, M.; Swami, S.S.; Aye, S.L.; Mohammed, L. The Role of Gut Microbiome in Hepatocellular Carcinoma: A Systematic Review. Cureus 2023, 15, e43862. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.; Cai, Y.; Yang, Y. The Gut Microbiome and Hepatocellular Carcinoma: Implications for Early Diagnostic Biomarkers and Novel Therapies. Liver Cancer 2021, 11, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Xie, C.; Pocha, C. Crosstalk between Gut Microbiota and Hepatocellular Carcinoma. Gastrointest. Disord. 2023, 5, 127–143. [Google Scholar] [CrossRef]
- Maesaka, K.; Sakamori, R.; Yamada, R.; Doi, A.; Tahata, Y.; Ohkawa, K.; Oshita, M.; Miyazaki, M.; Yakushijin, T.; Nozaki, Y.; et al. Pretreatment with antibiotics is associated with reduced therapeutic response to atezolizumab plus bevacizumab in patients with hepatocellular carcinoma. PLoS ONE 2023, 18, e0281459. [Google Scholar] [CrossRef] [PubMed]
- Matson, V.; Fessler, J.; Bao, R.; Chongsuwat, T.; Zha, Y.; Alegre, M.-L.; Luke, J.J.; Gajewski, T.F. The commensal microbiome is associated with anti-PD-1 efficacy in metastatic melanoma patients. Science 2018, 359, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Zheng, X.; Kang, W.; Hao, H.; Mao, Y.; Zhang, H.; Chen, Y.; Tan, Y.; He, Y.; Zhao, W.; et al. Metagenomic and metabolomic analyses reveal synergistic effects of fecal microbiota transplantation and anti-PD-1 therapy on treating colorectal cancer. Front. Immunol. 2022, 13, 874922. [Google Scholar] [CrossRef]
- Bai, D.-S.; Zhang, C.; Chen, P.; Jin, S.-J.; Jiang, G.-Q. The prognostic correlation of AFP level at diagnosis with pathological grade, progression, and survival of patients with hepatocellular carcinoma. Sci. Rep. 2017, 7, 12870. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Responder n = 28 | Non-Responder n = 9 | p-Value | |
|---|---|---|---|
| Age † | 74 (63–79) | 75 (71–85) | 0.184 |
| Gender (male/female) | 23/5 | 5/4 | 0.178 |
| Body mass index † | 23.3 (20.9–26.8) | 24.0 (20.9–25.3) | 0.804 |
| Etiology (HBV/HCV/Alcohol/NBNC) | 5/7/10/6 | 1/6/2/0 | 0.128 |
| BCLC stage (A/B/C) | 3/6/19 | 0/3/6 | 0.707 |
| Child–Pugh grade (A/B) | 28/0 | 6/3 | 0.011 |
| Child–Pugh score (5/6/7) | 22/6/0 | 3/3/3 | 0.007 |
| Treatment history (1/2/3/4) | 26/2/0/0 | 4/3/0/2 | 0.005 |
| AST (IU/L) † | 36 (27–51) | 37 (20–46) | 0.710 |
| ALT (IU/L) † | 29 (21–38) | 25 (15–30) | 0.279 |
| γ-GTP (IU/L) † | 77 (55–136) | 33 (31–186) | 0.583 |
| Total bilirubin (mg/dL) † | 0.8 (0.7–1.1) | 0.7 (0.5–1.0) | 0.246 |
| Albumin (g/dL) † | 3.8 (3.6–4.0) | 3.4 (2.6–3.8) | 0.051 |
| HbA1c (%) † | 6.1 (5.6–6.8) | 6.2 (5.7–6.7) | 0.657 |
| AFP (ng/mL) † | 9.5 (5.0–410.8) | 564.0 (13.0–845.0) | 0.123 |
| PPI (yes/no) | 18/10 | 5/4 | 0.705 |
| Antibiotics (yes/no) | 3/25 | 1/8 | 1.000 |
| C-reactive protein (mg/dL) † | 0.20 (0.09–0.50) | 0.38 (0.04–1.46) | 0.645 |
| NLR † | 1.96 (1.29–3.32) | 2.71 (1.64–3.62) | 0.357 |
| P. merdae (+) or B. stercoris (+) n = 33 | P. merdae (−) and B. stercoris (−) n = 4 | p-Value | |
|---|---|---|---|
| Age † | 73 (63–79) | 83 (79–85) | 0.047 |
| Gender (male/female) | 26/7 | 2/2 | 0.244 |
| Body mass index † | 24.0 (20.9–27.0) | 21.7 (20.1–23.3) | 0.240 |
| Etiology (HBV/HCV/Alcohol/NBNC) | 6/10/11/6 | 0/3/1/0 | 0.460 |
| BCLCstage (A/B/C) | 3/8/22 | 0/1/3 | 1 |
| Child–Pugh grade (A/B) | 31/2 | 3/1 | 0.298 |
| Child–Pugh score (5/6/7) | 24/7/2 | 1/2/1 | 0.104 |
| Treatment history (1/2/3/4) | 27/5/1 | 3/0/1 | 0.278 |
| AST (IU/L) † | 35 (25–45) | 134 (88–174) | 0.106 |
| ALT (IU/L) † | 27 (21–35)) | 52 (23–107) | 0.365 |
| γ-GTP (IU/L) † | 72 (34–132) | 266 (147–447) | 0.149 |
| Total bilirubin (mg/dL) † | 0.8 (0.6–1.2) | 0.9 (0.7–1.0) | 0.825 |
| Albumin (g/dL) † | 3.8 (3.6–4.0) | 3.0 (2.8–3.3) | 0.039 |
| HbA1c (%) † | 6.1 (5.7–6.8) | 6.2 (5.9–6.8) | 0.980 |
| AFP (ng/mL) † | 10.0 (5.0–494.0) | 4335.5 (429.8–36,901.0) | 0.027 |
| PPI (yes/no) | 21/12 | 2/2 | 0.625 |
| Antibiotics (yes/no) | 4/29 | 0/4 | 1.000 |
| C-reactive protein (mg/dL) † | 0.20 (0.09–0.44) | 1.27 (0.82–1.47) | 0.186 |
| NLR † | 1.97 (1.22–2.75) | 3.65 (3.20–4.08) | 0.070 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inukai, Y.; Yamamoto, K.; Honda, T.; Yokoyama, S.; Ito, T.; Imai, N.; Ishizu, Y.; Nakamura, M.; Ishigami, M.; Kawashima, H. Intestinal Microbiome Associated with Efficacy of Atezolizumab and Bevacizumab Therapy for Hepatocellular Carcinoma. Cancers 2024, 16, 1675. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16091675
Inukai Y, Yamamoto K, Honda T, Yokoyama S, Ito T, Imai N, Ishizu Y, Nakamura M, Ishigami M, Kawashima H. Intestinal Microbiome Associated with Efficacy of Atezolizumab and Bevacizumab Therapy for Hepatocellular Carcinoma. Cancers. 2024; 16(9):1675. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16091675
Chicago/Turabian StyleInukai, Yosuke, Kenta Yamamoto, Takashi Honda, Shinya Yokoyama, Takanori Ito, Norihiro Imai, Yoji Ishizu, Masanao Nakamura, Masatoshi Ishigami, and Hiroki Kawashima. 2024. "Intestinal Microbiome Associated with Efficacy of Atezolizumab and Bevacizumab Therapy for Hepatocellular Carcinoma" Cancers 16, no. 9: 1675. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16091675