Association between Periodontitis and Hematologic Cancer: An NHIRD Cohort Study in Taiwan
by
 and
and
Liang-Gie Huang
1,2,3, 
Cheng-Chia Yu
4,*,
Ming-Ching Lin
2,
Yu-Hsun Wang
5 and
Yu-Chao Chang
1,6,* 1
School of Dentistry, Chung Shan Medical University, Taichung 40201, Taiwan
2
Department of Stomatology, Taichung Veterans General Hospital, Taichung 40705, Taiwan
3
Department of Industrial Engineering and Enterprise Information, Tunghai University, Taichung 40704, Taiwan
4
Institute of Oral Sciences, Chung Shan Medical University, Taichung 40201, Taiwan
5
Department of Medical Research, Chung Shan Medical University Hospital, Taichung 40201, Taiwan
6
Department of Dentistry, Chung Shan Medical University Hospital, Taichung 40201, Taiwan
*
Authors to whom correspondence should be addressed.
Cancers 2024, 16(9), 1671; https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16091671
Submission received: 10 March 2024
/
Revised: 21 April 2024
/
Accepted: 24 April 2024
/
Published: 25 April 2024
(This article belongs to the Special Issue Oral Potentially Malignant Disorders and Oral Cavity Cancer)
Abstract
:Simple Summary
Our study aimed to delineate the variables associated with the link between chronic periodontitis and hematologic cancers. The hazard ratio for hematologic cancers in patients with chronic periodontitis was also evaluated. Comprehensive statistical analyses revealed a 1.25-fold risk of hematologic cancers in the chronic periodontitis group. Factors such as being male and having hypertension were identified as increased risk factors for hematologic cancers. This nuanced exploration, including a subtype analysis for leukemia and lymphoma, contributes valuable insights into the complex relationship between chronic periodontitis and specific hematologic cancer subtypes. These findings could enhance our understanding of potential cancer risk factors in Taiwan.
Abstract
Background: Chronic periodontitis, an inflammation-related disorder affecting global populations, has been revealed to be linked to diverse cancers. Numerous epidemiological studies have not shown a link between chronic periodontitis and blood cancers in Taiwan. Methods: This study included 601,628 patients, diagnosed with newly chronic periodontitis by the ICD-9-CM classification, who were enrolled from 2001 to 2021 in the National Health Insurance Research Database (NHIRD) in Taiwan. In this study, we employed comprehensive statistical analyses to investigate the association between chronic periodontitis and hematologic cancers. Initially, we calculated incidence density and used a Poisson regression to analyze relative risk. Subsequently, we compared the cumulative incidence of hematological cancer in both chronic and non-chronic periodontitis groups using the Kaplan–Meier method. Results: The results revealed a significantly lower cumulative incidence of hematologic cancer in individuals with non-chronic periodontitis over a 12-year follow-up period. To further explore the risk factors, a Cox proportional hazard regression analysis was conducted. Being male (adjusted hazard ratio [aHR] = 1.21, 95% CI: 1.04 to 1.42; p = 0.014) and having hypertension (aHR = 1.34, 95% CI: 1.06 to 1.69; p = 0.015) were demonstrated to be associated with an increased risk of hematologic cancers, respectively. In addition, in a subtype multivariate analysis for categorizing hematologic cancers into lymphoma and leukemia, the aHR for leukemia was 1.48 (95% CI: 1.13 to 1.93; p = 0.004) and aHR for lymphoma was 1.15 (95% CI: 0.96 to 1.37; p = 0.140). Conclusions: This study found that being male and having hypertension were the significant risk factors for hematological malignancies. Moreover, the association between chronic periodontitis and specific subtypes of hematologic cancers was confirmed.
1. Introduction
Chronic periodontitis is an inflammation-related disorder affecting the periodontal tissue, triggered by an imbalance in the oral microbial biofilm. Periodontal disease is prevalent worldwide, affecting 20–50% of the global population, with approximately 10% of people suffering from severe periodontitis [1,2,3]. Recently, significant endeavors have been undertaken to clarify the impact of an imbalanced oral microbiome on diverse systemic conditions, such as cardiovascular disease and cancer [4,5,6]. Epidemiological studies have identified a positive association between chronic periodontitis and the incidence of diverse cancer types, including head and neck cancer, esophageal cancer, gastric cancer, pancreatic cancer, colorectal cancer, lung cancer, breast cancer, gall bladder cancer, liver cancer, prostate cancer, hematological/hematopoietic malignancies, and genitourinary cancers [7,8,9,10,11].
Hematologic cancer, also known as hematological malignancy or blood cancer, refers to cancers that affect the blood, bone marrow, lymphatic system, and lymphoid tissues [12,13]. These cancers originate in the cells of the hematopoietic and lymphoid systems, which are responsible for the production of blood cells and the immune system [14]. The main types of hematologic cancers include (1) Leukemia: A type of cancer that begins in blood-forming tissues, such as bone marrow, and results in the excessive production of abnormal white blood cells. Leukemia can be manifested as an acute or chronic condition. (2) Lymphoma: Cancer that starts in the lymphocytes, a type of white blood cell, and primarily affects the lymph nodes and lymphoid tissues. There are two main types, Hodgkin lymphoma and non-Hodgkin lymphoma [15]. Hematologic cancers can interfere with the normal function of blood cells, weaken the immune system, and cause various symptoms such as fatigue, anemia, frequent infections, and abnormal bleeding [16]. Treatment for hematologic cancers may include chemotherapy, radiation therapy, immunotherapy, targeted therapy, and stem cell transplantation, depending on the specific type and stage of the cancer [17].
Until present, multiple epidemiological studies have investigated the potential risk of hematopoietic cancers in individuals with periodontitis [9,10,18,19,20,21,22]. Nevertheless, these studies have yielded inconsistent results, and the evidence still remains inconclusive. Therefore, we established two objectives to explore in this research: (1) to delineate the variables associated with the connection between chronic periodontitis and hematologic cancers; (2) to evaluate whether a higher hazard ratio for hematologic cancers existed within the group of patients with chronic periodontitis.
2. Materials and Methods
2.1. Data Sources, Study Population, and Participant Selection
Data were sourced from the National Health Insurance Research Database (NHIRD) in Taiwan. The National Health Research Institute initiated its National Health Insurance Program in 1995, aiming to enhance healthcare for the entire Taiwanese population. In terms of the current study, participants newly diagnosed with periodontitis were enrolled from 2001 to 2021 if they had attended dental outpatient visits three times or more. Participants with no history of diagnosed periodontitis were included, from 2000 to 2013. In the subset of those with newly diagnosed periodontitis, individuals with a diagnosed cancer prior to the index date were excluded. For both groups, we implemented 1:1 matching based on age, sex, monthly income, urbanization, and comorbidities.
2.2. The Definitions of Chronic Periodontitis and Hematologic Cancer
The identification of periodontitis was captured using ≥2 outpatient visits for dental treatment based on the ICD-9-CM diagnostic codes 523.4 and 523.5 from 2001 to 2012. Individuals with hematologic cancer were defined as those with ≥2 outpatient visits or 1 hospitalization. Moreover, the ICD-9-CM diagnostic codes for lymphoma and leukemia are 200–203 and 204–208, respectively. In the assessment of independent variables, conditions including hypertension (ICD-9-CM codes: 401–405), hyperlipidemia (ICD-9-CM codes: 272.0–272.4), diabetes mellitus (ICD-9-CM code: 250), chronic obstructive pulmonary disease (ICD-9-CM codes: 491, 492, 496), thyroid disease (ICD-9-CM codes: 240–246), asthma (ICD-9-CM code: 493), myocardial infarction (ICD-9-CM codes: 410–414), stroke (ICD-9-CM codes: 430–438), and insomnia (ICD-9-CM code: 780.52) were considered. The observation period was the year following the starting point at which individuals had been diagnosed through at least 2 outpatient visits or 1 inpatient diagnosis. The ICD-9-CM codes 401, 402, 403, 404, and 405 denote essential hypertension, hypertensive heart disease, hypertensive chronic kidney disease, hypertensive heart and chronic kidney disease, and secondary hypertension, respectively. The ICD-9-CM codes 272.0, 272.1, 272.2, 272.3, and 272.4 correspond to pure hypercholesterolemia, pure hyperglyceridemia, mixed hyperlipidemia, hyperchylomicronemia, and other and unspecified hyperlipidemia, respectively.
2.3. Independent Variable Assessment
We evaluated various independent variables that could be associated with both chronic periodontitis and hematologic cancer. These independent variables included age (<18, 18–64, ≥65 years old), sex (female and male), monthly income (<NTD 25,000, NTD 25,000, NTD 40,000, >NTD 40,000), urbanization (urban, suburban, rural), hypertension (no or yes), hyperlipidemia (no or yes), diabetes (no or yes), chronic obstructive pulmonary disease (no or yes), thyroid disease (no or yes), asthma (no or yes), myocardial infarction (no or yes), stroke (no or yes), and insomnia (no or yes).
2.4. Statistical Analyses
All statistical analyses were performed using SAS version 9.4 software (SAS Institute, Cary, NC, USA). All data values are presented as the mean ± standard error. The variables of demographic characteristics were used to determine the difference between chronic periodontitis and non-chronic periodontitis via Chi-squared tests. Poisson regression analysis was used to verify relative risk of hematologic cancers between chronic periodontitis and non-chronic periodontitis. A Kaplan–Meier analysis was employed to illustrate the cumulative incidence of hematologic cancers between chronic periodontitis and non-chronic periodontitis. Cox proportional hazard models were utilized to calculate the hazard ratios and 95% confidence intervals for hematologic cancers. Differences were considered significant at a p value < 0.05.
3. Results
A total of 601,628 individuals were sampled from the longitudinal health insurance database and categorized into a newly diagnosed periodontitis group (n = 255,052) and a never-diagnosed periodontitis group (n = 346,576), as illustrated in Figure 1. In the newly diagnosed periodontitis group (n = 254,765), those diagnosed with cancer before the index date was also excluded. Prior to propensity score matching, both the newly diagnosed periodontitis group (n = 190,455) and the never-diagnosed periodontitis group (n = 190,455) were matched at a 1:1 ratio based on age and sex (Figure 1). In order to mitigate bias in examining the connections between chronic periodontitis and the outcomes of hematologic cancers, propensity score matching was used to adjust the potential confounding factors. Finally, the periodontitis and non-periodontitis groups included 168,191 and 168,191 individuals, via propensity score matching, for further analysis (Figure 1).
As shown in Table 1, no significant differences were revealed in age, sex, monthly income, urbanization, hypertension, hyperlipidemia, diabetes mellitus, chronic obstructive pulmonary disease, myocardial infarction, and stroke after matching by propensity score. The chronic periodontitis group were aged between 18 and 64 years old (126,975 individuals, about 75.5%). A total of 129,238 patients (76.8%) had a monthly income of less than NTD 25,000 Taiwanese dollars, and 104,740 individuals (62.3%) lived in urban areas (Table 1). Then, we calculated incidence densities and relative risks to gauge the correlation between chronic periodontitis and hematologic cancers (Table 2). The incidence density and 95% confidence interval for non-chronic periodontitis and chronic periodontitis were 0.19 (0.17–0.21) and 0.24 (0.21–0.26), respectively (Table 2).
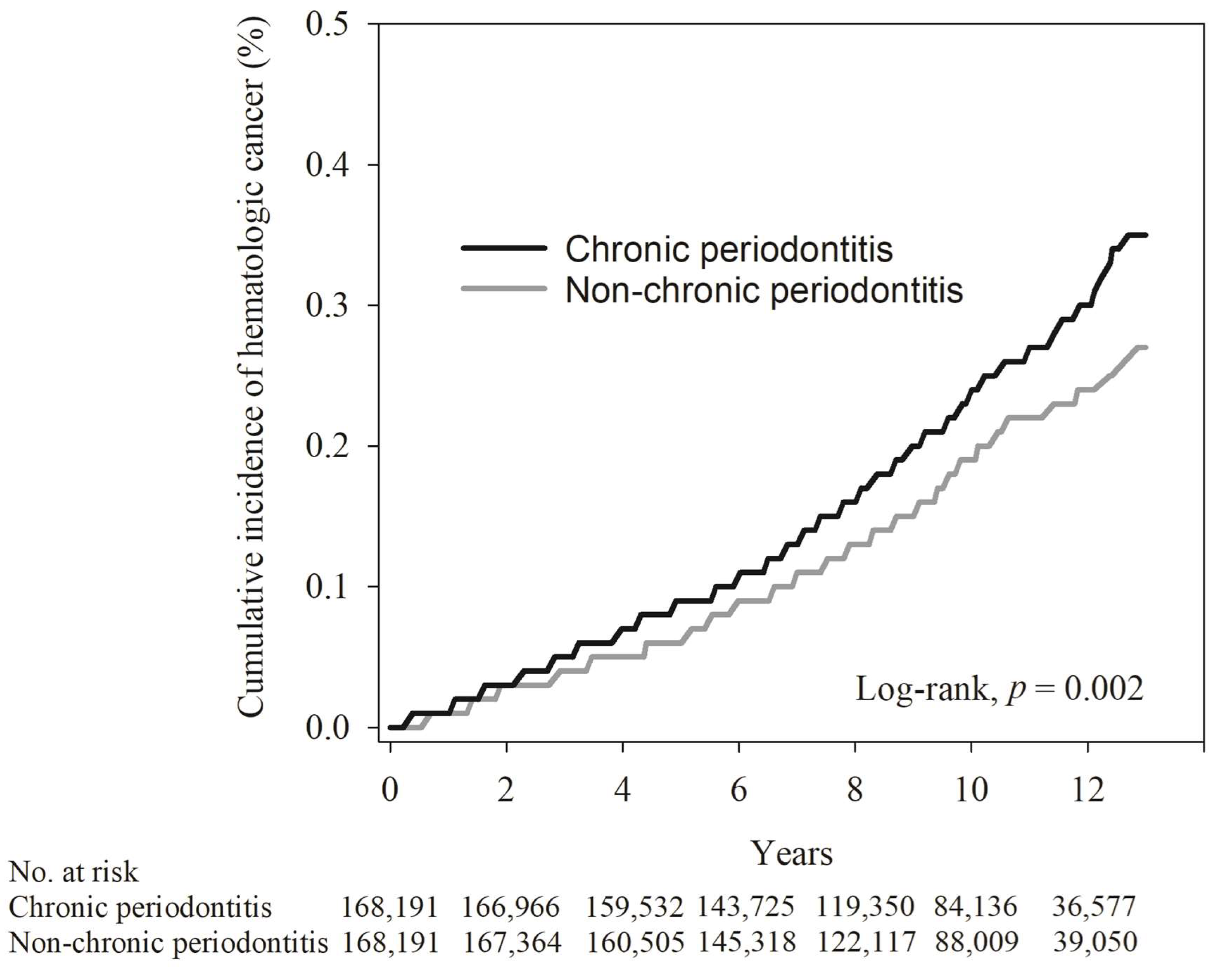
In order to compare the cumulative incidence of hematological cancer in the chronic periodontitis and non-chronic periodontitis groups, the Kaplan–Meier method, with a log-rank test, was used for our analysis. As indicated in Table 3, the average follow-up duration in the non-chronic periodontitis and chronic periodontitis groups was 9.6 ± 2.8 years and 9.4 ± 2.8 years, respectively (determined by the log-rank test, p < 0.001). The mean interquartile ranges for hematologic cancers were 6.3 ± 3.4 years and 6.1 ± 3.2 years for the non-chronic periodontitis and chronic periodontitis groups, respectively (determined by the log-rank test, p = 0.636). As illustrated in Figure 2, the Kaplan–Meier plot for individuals with non-chronic periodontitis exhibited a notably lower cumulative incidence of hematologic cancer compared to those in the chronic periodontitis group during the 12-year follow-up period.
To assess the hazard ratio (HR) of hematologic cancers associated with the presence of non-chronic periodontitis and chronic periodontitis, we conducted a Cox proportional hazard regression analysis. Additionally, we utilized the adjusted hazard ratio (aHR) to represent a multivariate analysis that incorporates all variables used in this study. The results are shown in Table 4. In the univariate analysis, it was observed that the group with chronic periodontitis had a higher likelihood of developing hematologic cancers compared to the non-chronic periodontitis group (HR, 1.27; 95% CI: 1.09 to 1.48; p = 0.002), and the multivariate analysis, which included all variables considered in this study, confirmed that the chronic periodontitis group faced an elevated risk of developing hematologic cancers (aHR, 1.25; 95% CI: 1.07 to 1.45; p = 0.004). Moreover, our multivariate Cox proportional hazards model showed that being male (aHR = 1.21, 95% CI: 1.04 to 1.42; p = 0.014) and having hypertension (aHR = 1.34, 95% CI: 1.06 to 1.69; p = 0.015) were risk factors for hematologic cancers. It is worth mentioning that participants aged 18–64 years (aHR = 2.62, 95% CI: 1.77 to 3.89; p < 0.001) and those aged 65 years or older (aHR = 10.46, 95% CI: 6.87 to 15.91; p < 0.001) were also identified as being at higher risk of hematologic cancers.
In the subgroup multivariate analysis (Table 5), the occurrence of hematologic cancer was elevated in the chronic periodontitis group compared to the non-chronic periodontitis group, both in males and females. Notably, the aHR was higher for females than for males (1.30 and 1.25, respectively). Furthermore, chronic periodontal status significantly altered the association between individuals aged 18–64 years and their development of hematologic cancers (p for interaction = 0.012). Additionally, in the subtype multivariate analysis (Table 6), we categorized hematologic cancer into lymphoma and leukemia. The aHR for leukemia was 1.48 (95% CI: 1.13 to 1.93; p = 0.004), while for lymphoma it was 1.15 (95% CI: 0.96 to 1.37; p = 0.140) (Table 6).
4. Discussion
In summary of our comprehensive study on the association between chronic periodontitis and hematologic cancers using rigorous statistical analyses, the 12-year follow-up period revealed a significantly lower cumulative incidence of hematologic cancer in individuals without chronic periodontitis. Our Cox proportional hazard regression analysis identified being male and having hypertension as the significant risk factors for hematologic cancers. Moreover, our subtype analysis highlighted a higher adjusted hazard ratio for leukemia compared to lymphoma. These findings provide valuable insights into the nuanced relationship between chronic periodontitis and specific hematologic cancer subtypes. In addition, our study demonstrated the importance of gender and hypertension in understanding the complex interplay between periodontal health and hematologic malignancies.
The oral and periodontal microbiome might facilitate the development of cancer in distant areas through systemic inflammation, the indirect long-distance impact of virulence factors originating from the oral microbiota, and the direct migration of microorganisms via the bloodstream and oropharyngeal and respiratory pathways. Additionally, it could also affect patients’ response to treatments by interacting with the host immune response [23]. A previous review demonstrated that oral and esophageal cancers were consistent with the increased risk associated with periodontal disease [24]. Gastric and pancreatic cancers demonstrated various degrees of association with periodontal disease in most studies. However, lung, prostate, hematologic, and other cancers displayed either less-consistent associations with periodontal disease or a lack of sufficient studies to establish a predictable pattern [24]. Recently, Heikkilä et al. reported stronger associations of periodontitis with increased overall cancer mortality after adjustments for age, sex, socio-economic status, dental treatments, and diabetes [25].
Hematologic cancer, marked by the abnormal proliferation of undifferentiated white and red blood cells in the bone marrow, results in impaired cell function; as these undifferentiated cells (blasts) enter the bloodstream, they can infiltrate organs, including the oral cavity, leading to clinical manifestations like gingival bleeding and swelling, indicative of potential leukemia [26]. Previous studies have indicated that hematopoietic and lymphatic malignancies such as lymphomas and leukemia exhibited share risk factors like gender, immune dysregulation, older age, smoking, prior chemotherapy, and exposure to radiation [16,21,22]. Some studies have revealed that periodontal disease was associated with elevated risks of combined hematological cancers (HR, 1.18; 95% CI: 1.02 to 1.37) and lymphoid/hematopoietic malignancies in never-smokers (HR, 1.34; 95% CI: 1.08 to 1.67) [9,19]. Michaud et al. have reported that periodontal disease increased the risk of hematopoietic malignancies in male individuals (HR, 1.30; 95% CI: 1.11 to 1.53) [27]. Additionally, a report has suggested a higher association between periodontal disease and non-Hodgkin lymphomas (HR, 1.30; 95% CI: 1.11 to 1.51) [21].
This study was a cohort study aiming to investigate the association between chronic periodontitis and hematologic cancers in the Taiwanese population. The strength of this cohort design allows for the establishment of a cause relationship between chronic periodontitis and hematologic cancers. A 12-year follow-up period would enable researchers to observe the occurrence of these events. Through the use of the NHIRD, a large sample size, up to 601,628 patients, were recruited in this register-based cohort study. This could enhance its statistical power. With the adjustment of potential confounding variables, the results on the association between chronic periodontitis and hematologic cancers are more reliable and valid.
However, some possible limitations to the current study should be noted. First, the study extracted data from the NHIRD in Taiwan, while the diagnosis of chronic periodontitis was based on ICD-9 codes. However, there was no corresponding ICD-9 code for the new classification of periodontal diseases and conditions in 2017 [28]. The severity of the chronic periodontitis also could not be obtained from the NHIRD. Second, there is no record of oral habits such as alcohol consumption, betel nut chewing, cigarette smoking, lifestyle, dietary habits, and environmental factors in the NHIRD. These confounding variables may be unmeasured or unknown confounders that could impact the association between chronic periodontitis and hematologic cancers and should be underscored.
5. Conclusions
Through comprehensive statistical analyses using NHIRD, we found a higher hazard ratio for hematologic cancers in patients with chronic periodontitis. Furthermore, our study identified being male and having hypertension as the significant risk factors for hematologic cancers. The nuanced understanding gained from our investigation sheds light on the complex relationship between chronic periodontitis and specific subtypes of hematologic cancers. These findings could provide valuable insights for future research and clinical considerations.
Author Contributions
Conceptualization, Y.-C.C.; methodology, M.-C.L. and Y.-H.W.; resources, Y.-C.C.; writing—original draft, L.-G.H.; writing—review and editing, C.-C.Y. and Y.-C.C.; supervision, Y.-C.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Chung Shan Medical University Hospital (CSMUH No.CS2-15017).
Informed Consent Statement
Due to this dataset was analyzed anonymously, no informed consent from participants was required.
Data Availability Statement
Restrictions apply to the availability of these data. Data was obtained from National Health Insurance database and are available from the authors with the permission of National Health Insurance Administration of Taiwan.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Keams, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of severe periodontitis in 1990–2010: A systematic review and meta-regression. J. Dent. Res. 2014, 93, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Bernabe, E.; Marcenes, W.; Hernandez, C.R.; Bailey, J.; Abreu, L.G.; Alipour, V.; Amini, S.; Arabloo, J.; Arefi, Z.; Arora, A.; et al. Global, regional, and national levels and trends in burden of oral conditions from 1990 to 2017: A systematic analysis for the global burden of disease 2017 study. J. Dent. Res. 2020, 99, 362–373. [Google Scholar] [PubMed]
- Hajishengallis, G.; Chavakis, T. Local and systemic mechanisms linking periodontal disease and inflammatory comorbidities. Nat. Rev. Immunol. 2021, 21, 426–440. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Cheng, L.; You, Y.; Tang, C.; Ren, B.; Li, Y.; Xu, X.; Zhou, X. Oral microbiota in human systematic diseases. Int. J. Oral Sci. 2022, 14, 14. [Google Scholar] [CrossRef] [PubMed]
- Pisano, M.; Giordano, F.; Sangiovanni, G.; Capuano, N.; Acerra, A.; D’Ambrosio, F. The Interaction between the Oral Microbiome and Systemic Diseases: A Narrative Review. Microbiol. Res. 2023, 14, 1862–1878. [Google Scholar] [CrossRef]
- Moraes, R.C.d.; Dias, F.L.; Figueredo, C.M.d.S.; Fischer, R.G. Association between Chronic Periodontitis and Oral/Oropharyngeal Cancer. Braz. Dent. J. 2016, 27, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Nie, S.; Zhu, Y.; Lu, M. Teeth loss, teeth brushing and esophageal carcinoma: A systematic review and meta-analysis. Sci. Rep. 2015, 5, 15203. [Google Scholar] [CrossRef]
- Nwizu, N.N.; Marshall, J.R.; Moysich, K.; Genco, R.J.; Hovey, K.M.; Mai, X.; LaMonte, M.J.; Freudenheim, J.L.; Wactawski-Wende, J. Periodontal disease and incident cancer risk among postmenopausal women: Results from the women’s health initiative observational cohort. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1255–1265. [Google Scholar] [CrossRef]
- Michaud, D.S.; Lu, J.; Peacock-Villada, A.Y.; Barber, J.R.; Joshu, C.E.; Prizment, A.E.; Beck, J.D.; Offenbacher, S.; Platz, E.A. Periodontal disease assessed using clinical dental measurements and cancer risk in the ARIC study. J. Natl. Cancer Inst. 2018, 110, 843–854. [Google Scholar] [CrossRef]
- Kim, E.H.; Nam, S.; Park, C.H.; Kim, Y.; Lee, M.; Ahn, J.B.; Shin, S.J.; Park, Y.R.; Jung, H.I.; Kim, B.; et al. Periodontal disease and cancer risk: A nationwide population-based cohort study. Front. Oncol. 2022, 12, 901098. [Google Scholar] [CrossRef] [PubMed]
- Karagianni, P.; Giannouli, S.; Voulgarelis, M. From the (Epi)genome to metabolism and vice versa; examples from hematologic malignancy. Int. J. Mol. Sci. 2021, 22, 6321. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Wu, J.; Wang, Q.; Liang, Y.; Li, X.; Chen, G.; Ma, L.; Liu, X.; Zhou, F. Global burden of hematologic malignancies and evolution patterns over the past 30 years. Blood Cancer J. 2023, 13, 82. [Google Scholar] [CrossRef] [PubMed]
- Hassan, G.; Seno, M. Blood and Cancer: Cancer Stem Cells as Origin of Hematopoietic Cells in Solid Tumor Microenvironments. Cells 2020, 9, 1293. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Huang, J.; Huang, J.; Xue, H.; Liang, Z.; Wu, J.; Chen, C. Nanomedicine—A promising therapy for hematological malignancies. Biomater. Sci. 2020, 8, 2376–2393. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Shi, X.; Li, Y.; Xia, J.; Gu, Y.; Qian, Q.; Hong, Y. Hematopoietic and lymphatic cancers in patients with periodontitis: A systematic review and meta-analysis. Med. Oral Patol. Oral Cir. Bucal 2020, 25, e21–e28. [Google Scholar] [CrossRef] [PubMed]
- Sochacka-Ćwikła, A.; Mączyński, M.; Regiec, A. FDA-Approved Drugs for Hematological Malignancies—The Last Decade Review. Cancers 2022, 14, 87. [Google Scholar] [CrossRef]
- Kristinsson, S.Y.; Koshiol, J.; Bjorkholm, M.; Goldin, L.R.; McMaster, M.L.; Turesson, I. Immune-related and inflammatory conditions and risk of lymphoplasmacytic lymphoma or Waldenstrom macroglobulinemia. J. Natl. Cancer Inst. 2010, 102, 557–567. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.D.; Tsai, M.C.; Huang, C.C.; Kao, L.T.; Chen, C.H. A population-based study on the associations between chronic periodontitis and the risk of cancer. Int. J. Clin. Oncol. 2016, 21, 219–223. [Google Scholar] [CrossRef]
- Mai, X.; LaMonte, M.J.; Hovey, K.M.; Freudenheim, J.L.; Andrews, C.A.; Genco, R.J. Periodontal disease severity and cancer risk in postmenopausal women: The Buffalo OsteoPerio Study. Cancer Causes Control 2016, 27, 217–228. [Google Scholar] [CrossRef]
- Bertrand, K.A.; Shingala, J.; Evens, A.; Birmann, B.M.; Giovannucci, E.; Michaud, D.S. Periodontal disease and risk of non-Hodgkin lymphoma in the Health Professionals Follow-Up Study. Int. J. Cancer 2017, 140, 1020–1026. [Google Scholar] [CrossRef] [PubMed]
- Barton, M.K. Evidence accumulates indicating periodontal disease as a risk factor for colorectal cancer or lymphoma. CA Cancer J. Clin. 2017, 67, 173–174. [Google Scholar] [CrossRef] [PubMed]
- Di Spirito, F. Oral-Systemic Health and Disorders: Latest Prospects on Oral Antisepsis. Appl. Sci. 2022, 12, 8185. [Google Scholar] [CrossRef]
- Fitzpatrick, S.G.; Katz, J. The association between periodontal disease and cancer: A review of the literature. J. Dent. 2010, 38, 83–95. [Google Scholar] [CrossRef] [PubMed]
- Heikkilä, P.; But, A.; Sorsa, T.; Haukka, J. Periodontitis and cancer mortality: Register-based cohort study of 68,273 adults in 10-year follow-up. Int. J. Cancer 2018, 142, 2244–2253. [Google Scholar] [CrossRef] [PubMed]
- Angst, P.D.M.; Maier, J.; Nogueira, R.D.S.; Manso, I.S.; Tedesco, T.K. Oral health status of patients with leukemia: A systematic review with meta-analysis. Arch. Oral Biol. 2020, 120, 104948. [Google Scholar] [CrossRef] [PubMed]
- Michaud, D.S.; Liu, Y.; Meyer, M.; Giovannucci, E.; Joshipura, K. Periodontal disease, tooth loss, and cancer risk in male health professionals: A prospective cohort study. Lancet Oncol. 2008, 9, 550–558. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89, S159–S172. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of participant selection.

Figure 2.
The Kaplan–Meier plot for the cumulative incidence of hematologic cancer in chronic periodontitis and non-chronic periodontitis subjects.
Figure 2.
The Kaplan–Meier plot for the cumulative incidence of hematologic cancer in chronic periodontitis and non-chronic periodontitis subjects.


{kind=link}
{kind=link}
Table 1.
Demographic characteristics of chronic periodontitis and non-chronic periodontitis groups.
| Before PSM | After PSM | |||||
|---|---|---|---|---|---|---|
| Chronic Periodontitis (N = 190,455) | Non-Chronic Periodontitis (N = 190,455) | ASD * | Chronic Periodontitis (N = 168,191) | Non-Chronic Periodontitis (N = 168,191) | ASD * | |
| Age | <0.001 | 0.020 | ||||
| <18 | 27,966 (14.7) | 27,966 (14.7) | 27,752 (16.5) | 27,191 (16.2) | ||
| 18–64 | 146,987(77.2) | 146,987(77.2) | 126,975 (75.5) | 128,304 (76.3) | ||
| ≥65 | 15,502 (8.1) | 15,502 (8.1) | 13,464 (8.0) | 12,696 (7.5) | ||
| Mean ± SD | 36.9 ± 17.4 | 36.9 ± 17.4 | <0.001 | 36.4 ± 17.3 | 35.9 ± 17.5 | 0.028 |
| Sex | <0.001 | 0.007 | ||||
| Female | 91,390 (48.0) | 91,390 (48.0) | 82,563 (49.1) | 81,969 (48.7) | ||
| Male | 99,065 (52.0) | 99,065 (52.0) | 85,628 (50.9) | 86,222 (51.3) | ||
| Monthly income | 0.248 | 0.009 | ||||
| <NTD 25,000 | 132,774 (69.7) | 151,904 (79.8) | 129,238 (76.8) | 129,770 (77.2) | ||
| NTD 25,000–NTD 40,000 | 23,046 (12.1) | 18,783 (9.9) | 18,720 (11.1) | 18,653 (11.1) | ||
| >NTD 40,000 | 34,635 (18.2) | 19,768 (10.4) | 20,233 (12.0) | 19,768 (11.8) | ||
| Urbanization | 0.230 | 0.020 | ||||
| Urban | 123,462 (64.8) | 103,567 (54.4) | 104,740 (62.3) | 103,464 (61.5) | ||
| Suburban | 54,691 (28.7) | 66,238 (34.8) | 51,213 (30.4) | 52,753 (31.4) | ||
| Rural | 12,302 (6.5) | 20,650 (10.8) | 12,238 (7.3) | 11,974 (7.1) | ||
| Hypertension | 16,527 (8.7) | 13,370 (7.0) | 0.062 | 12,994 (7.7) | 12,545 (7.5) | 0.010 |
| Hyperlipidemia | 6721 (3.5) | 4176 (2.2) | 0.080 | 4199 (2.5) | 4158 (2.5) | 0.002 |
| Diabetes | 6959 (3.7) | 5764 (3.0) | 0.035 | 5499 (3.3) | 5430 (3.2) | 0.002 |
| COPD ** | 3043 (1.6) | 2161 (1.1) | 0.040 | 2012 (1.2) | 2102 (1.2) | 0.005 |
| Thyroid disease | 2312 (1.2) | 1415 (0.7) | 0.048 | 1418 (0.8) | 1412 (0.8) | <0.001 |
| Asthma | 2825 (1.5) | 2171 (1.1) | 0.030 | 2097 (1.2) | 2097 (1.2) | <0.001 |
| Myocardial infarction | 5119 (2.7) | 3519 (1.8) | 0.056 | 3361 (2.0) | 3411 (2.0) | 0.002 |
| Stroke | 2411 (1.3) | 2359 (1.2) | 0.002 | 2078 (1.2) | 2088 (1.2) | 0.001 |
| Insomnia | 2940 (1.5) | 1963 (1.0) | 0.046 | 1933 (1.1) | 1927 (1.1) | <0.001 |
PSM: propensity score matching; * ASD: absolute standardized difference; ** COPD: chronic obstructive pulmonary disease.
Table 2.
Poisson regression of relative risk of chronic periodontitis group and non-chronic periodontitis groups.
Table 2.
Poisson regression of relative risk of chronic periodontitis group and non-chronic periodontitis groups.
| Non-Chronic Periodontitis | Chronic Periodontitis | |
|---|---|---|
| N | 168,191 | 168,191 |
| Person years | 1,581,487 | 1,605,135 |
| No. of hematologic cancer cases | 293 | 381 |
| ID (95% C.I.) | 0.19 (0.17–0.21) | 0.24 (0.21–0.26) |
| Relative risk (95% C.I.) | Reference | 1.28 (1.10–1.49) |
ID: incidence density (per 1000 person years).
Table 3.
The cumulative incidence of hematologic cancer in chronic periodontitis and non-chronic periodontitis subjects.
Table 3.
The cumulative incidence of hematologic cancer in chronic periodontitis and non-chronic periodontitis subjects.
| Chronic Periodontitis (N = 168,191) | Non-Chronic Periodontitis (N = 168,191) | p Value | |
|---|---|---|---|
| Follow-up duration (years) | 9.6 ± 2.8 | 9.4 ± 2.8 | <0.001 |
| Time to hematologic cancer (years) | 6.3 ± 3.4 | 6.1 ± 3.2 | 0.636 |
Table 4.
Cox proportional hazard model analysis for risk of hematologic cancers.
| Univariate | Multivariate † | |||
|---|---|---|---|---|
| HR (95% C.I.) | p Value | HR (95% C.I.) | p Value | |
| Group | ||||
| Non-chronic periodontitis | Reference | Reference | ||
| Chronic periodontitis | 1.27 (1.09–1.48) | 0.002 | 1.25 (1.07–1.45) | 0.004 |
| Age | ||||
| <18 | Reference | Reference | ||
| 18–64 | 2.87 (1.95–4.24) | <0.001 | 2.62 (1.77–3.89) | <0.001 |
| ≥65 | 13.54 (9.06–20.23) | <0.001 | 10.46 (6.87–15.91) | <0.001 |
| Sex | ||||
| Female | Reference | Reference | ||
| Male | 1.21 (1.04–1.41) | 0.014 | 1.21 (1.04–1.42) | 0.014 |
| Monthly income | ||||
| <NTD 25,000 | Reference | Reference | ||
| NTD 25,000–NTD 40,000 | 0.80 (0.62–1.04) | 0.096 | 0.96 (0.74–1.26) | 0.793 |
| >NTD 40,000 | 1.07 (0.86–1.33) | 0.561 | 1.25 (0.99–1.58) | 0.058 |
| Urbanization | ||||
| Urban | Reference | Reference | ||
| Suburban | 1.04 (0.88–1.22) | 0.676 | 0.96 (0.82–1.14) | 0.672 |
| Rural | 1.04 (0.77–1.40) | 0.801 | 0.81 (0.60–1.09) | 0.162 |
| Hypertension | 3.25 (2.70–3.93) | <0.001 | 1.34 (1.06–1.69) | 0.015 |
| Hyperlipidemia | 2.88 (2.10–3.93) | <0.001 | 1.31 (0.94–1.85) | 0.114 |
| Diabetes | 2.75 (2.08–3.63) | <0.001 | 1.18 (0.87–1.60) | 0.294 |
| COPD ** | 2.82 (1.86–4.27) | <0.001 | 1.10 (0.71–1.70) | 0.670 |
| Thyroid disease | 1.88 (1.04–3.41) | 0.038 | 1.55 (0.85–2.83) | 0.151 |
| Asthma | 2.09 (1.29–3.39) | 0.003 | 1.25 (0.76–2.06) | 0.372 |
| Myocardial infarction | 3.79 (2.83–5.09) | <0.001 | 1.36 (0.98–1.88) | 0.065 |
| Stroke | 2.78 (1.80–4.29) | <0.001 | 0.89 (0.56–1.39) | 0.600 |
| Insomnia | 2.55 (1.60–4.08) | <0.001 | 1.32 (0.82–2.12) | 0.252 |
** COPD: chronic obstructive pulmonary disease. † Adjusted for age, sex, monthly income, urbanization, and comorbidities.
Table 5.
Subgroup analysis for risk of hematologic cancer.
| Chronic Periodontitis | Non-Chronic Periodontitis | aHR (95% C.I.) | p Value | |||
|---|---|---|---|---|---|---|
| N | No. of Hematologic Cancer | N | No. of Hematologic Cancer | |||
| Age | ||||||
| <18 a | 30,327 | 281 | 30,324 | 246 | 0.55 (0.25–1.20) | 0.130 |
| 18–64 b | 33,416 | 344 | 33,600 | 326 | 1.49 (1.23–1.80) | <0.001 |
| ≥65 b | 6728 | 45 | 6547 | 32 | 1.00 (0.75–1.31) | 0.977 |
| p for interaction = | 0.012 | |||||
| Sex c | ||||||
| Female | 37,004 | 397 | 36,999 | 376 | 1.30 (1.03–1.63) | 0.026 |
| Male | 33,467 | 273 | 33,472 | 228 | 1.25 (1.02–1.53) | 0.033 |
| p for interaction = | 0.810 | |||||
aHR: adjusted HR. a: adjusted for age, sex, and urbanization. b: adjusted for age, sex, monthly income, urbanization, and comorbidities. c: adjusted for age, monthly income, urbanization, and comorbidities.
Table 6.
Subtype analysis for risk of hematologic cancer.
| Chronic Periodontitis | Non-Chronic Periodontitis | aHR † (95% C.I.) | p Value | |||
|---|---|---|---|---|---|---|
| N | No. of Event | N | No. of Event | |||
| Hematologic cancer | ||||||
| Lymphoma | 168,191 | 256 | 168,191 | 214 | 1.15 (0.96–1.37) | 0.140 |
| Leukemia | 168,191 | 136 | 168,191 | 89 | 1.48 (1.13–1.93) | 0.004 |
aHR: adjusted HR. † Adjusted for age, sex, monthly income, urbanization, and comorbidities.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Huang, L.-G.; Yu, C.-C.; Lin, M.-C.; Wang, Y.-H.; Chang, Y.-C. Association between Periodontitis and Hematologic Cancer: An NHIRD Cohort Study in Taiwan. Cancers 2024, 16, 1671. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16091671
AMA Style
Huang L-G, Yu C-C, Lin M-C, Wang Y-H, Chang Y-C. Association between Periodontitis and Hematologic Cancer: An NHIRD Cohort Study in Taiwan. Cancers. 2024; 16(9):1671. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16091671
Chicago/Turabian StyleHuang, Liang-Gie, Cheng-Chia Yu, Ming-Ching Lin, Yu-Hsun Wang, and Yu-Chao Chang. 2024. "Association between Periodontitis and Hematologic Cancer: An NHIRD Cohort Study in Taiwan" Cancers 16, no. 9: 1671. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers16091671
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.