
Combination Therapy of Immune Checkpoint Inhibitors with Locoregional Therapy for Hepatocellular Carcinoma


Abstract
:Simple Summary
Abstract
1. Introduction
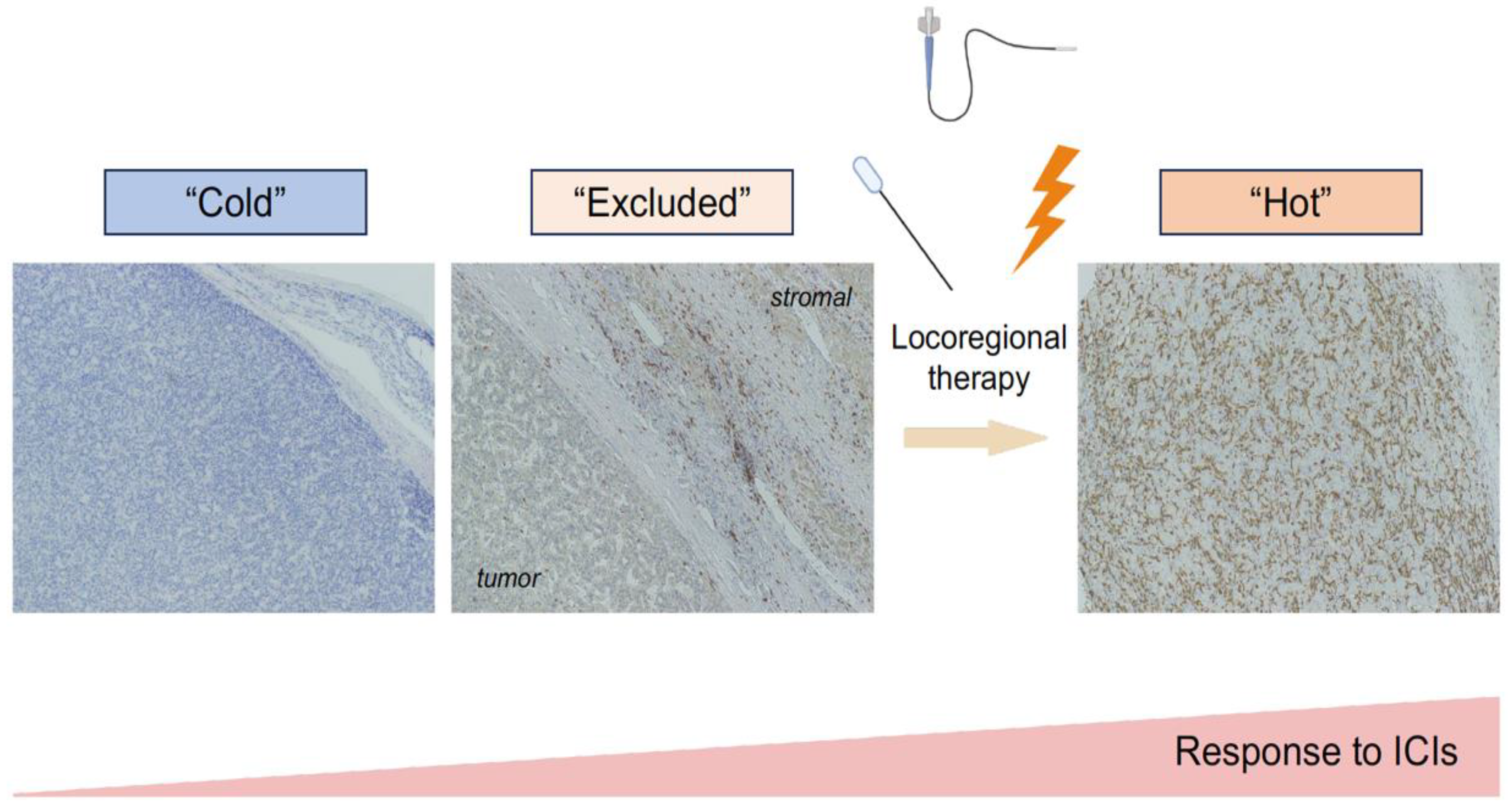
2. Tumor Immune Microenvironment for HCC and ICI Efficacy
Rationale for Combination of ICI and Locoregional Therapies
3. Cancer–Immunity Cycle Acceleration by Locoregional Therapies
3.1. Ablation Therapy
3.2. RFA
3.3. MWA
3.4. Cryoablation
3.5. Transarterial Embolization
3.6. TACE/DEB-TACE
3.7. TARE
3.8. Radiotherapy
3.9. In-Progress Clinical Trials of ICI Plus Locoregional Therapies
3.9.1. Ablation Therapy
3.9.2. TACE
3.9.3. TARE
3.9.4. Stereotactic Body Radiotherapy (SBRT)
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Yang, J.D.; Hainaut, P.; Gores, G.J.; Amadou, A.; Plymoth, A.; Roberts, L.R. A global view of hepatocellular carcinoma: Trends, risk, prevention and management. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 589–604. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Singal, A.G.; Llovet, J.M.; Yarchoan, M.; Mehta, N.; Heimbach, J.K.; Dawson, L.A.; Jou, J.H.; Kulik, L.M.; Agopian, V.G.; Marrero, J.A.; et al. AASLD Practice Guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology 2023. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, N.; Friedman, S.L.; Goossens, N.; Hoshida, Y. Risk factors and prevention of hepatocellular carcinoma in the era of precision medicine. J. Hepatol. 2018, 68, 526–549. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.T.; Fujiwara, N.; Yang, J.D.; Hoshida, Y. Risk stratification and early detection biomarkers for precision HCC screening. Hepatology 2023, 78, 319–362. [Google Scholar] [CrossRef] [PubMed]
- Park, J.W.; Chen, M.; Colombo, M.; Roberts, L.R.; Schwartz, M.; Chen, P.J.; Kudo, M.; Johnson, P.; Wagner, S.; Orsini, L.S.; et al. Global patterns of hepatocellular carcinoma management from diagnosis to death: The BRIDGE Study. Liver Int. 2015, 35, 2155–2166. [Google Scholar] [CrossRef]
- Shiina, S.; Tateishi, R.; Arano, T.; Uchino, K.; Enooku, K.; Nakagawa, H.; Asaoka, Y.; Sato, T.; Masuzaki, R.; Kondo, Y.; et al. Radiofrequency ablation for hepatocellular carcinoma: 10-year outcome and prognostic factors. Am. J. Gastroenterol. 2012, 107, 569–577; quiz 578. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Cheng, A.L.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Lim, H.Y.; Kudo, M.; Breder, V.; Merle, P.; et al. Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J. Hepatol. 2022, 76, 862–873. [Google Scholar] [CrossRef]
- Qin, S.; Chan, S.L.; Gu, S.; Bai, Y.; Ren, Z.; Lin, X.; Chen, Z.; Jia, W.; Jin, Y.; Guo, Y.; et al. Camrelizumab plus rivoceranib versus sorafenib as first-line therapy for unresectable hepatocellular carcinoma (CARES-310): A randomised, open-label, international phase 3 study. Lancet 2023, 402, 1133–1146. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Lau, G.; Kudo, M.; Chan, S.L.; Kelley, R.K.; Furuse, J.; Sukeepaisarnjaroen, W.; Kang, Y.-K.; Dao, T.V.; Toni, E.N.D.; et al. Tremelimumab plus Durvalumab in Unresectable Hepatocellular Carcinoma. NEJM Evid. 2022, 1, EVIDoa2100070. [Google Scholar] [CrossRef]
- Cappuyns, S.; Corbett, V.; Yarchoan, M.; Finn, R.S.; Llovet, J.M. Critical Appraisal of Guideline Recommendations on Systemic Therapies for Advanced Hepatocellular Carcinoma: A Review. JAMA Oncol. 2023. [Google Scholar] [CrossRef]
- Tawbi, H.A.; Schadendorf, D.; Lipson, E.J.; Ascierto, P.A.; Matamala, L.; Castillo Gutierrez, E.; Rutkowski, P.; Gogas, H.J.; Lao, C.D.; De Menezes, J.J.; et al. Relatlimab and Nivolumab versus Nivolumab in Untreated Advanced Melanoma. N. Engl. J. Med. 2022, 386, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Curigliano, G.; Gelderblom, H.; Mach, N.; Doi, T.; Tai, D.; Forde, P.M.; Sarantopoulos, J.; Bedard, P.L.; Lin, C.C.; Hodi, F.S.; et al. Phase I/Ib Clinical Trial of Sabatolimab, an Anti-TIM-3 Antibody, Alone and in Combination with Spartalizumab, an Anti-PD-1 Antibody, in Advanced Solid Tumors. Clin. Cancer Res. 2021, 27, 3620–3629. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Ryoo, B.-Y.; Hsu, C.-H.; Li, D.; Burgoyne, A.; Cotter, C.; Badhrinarayanan, S.; Wang, Y.; Yin, A.; Edubilli, T.R.; et al. Results from the MORPHEUS-liver study: Phase Ib/II randomized evaluation of tiragolumab (tira) in combination with atezolizumab (atezo) and bevacizumab (bev) in patients with unresectable, locally advanced or metastatic hepatocellular carcinoma (uHCC). J. Clin. Oncol. 2023, 41, 4010. [Google Scholar] [CrossRef]
- D’Alessio, A.; Fulgenzi, C.A.M.; Nishida, N.; Schonlein, M.; von Felden, J.; Schulze, K.; Wege, H.; Gaillard, V.E.; Saeed, A.; Wietharn, B.; et al. Preliminary evidence of safety and tolerability of atezolizumab plus bevacizumab in patients with hepatocellular carcinoma and Child-Pugh A and B cirrhosis: A real-world study. Hepatology 2022, 76, 1000–1012. [Google Scholar] [CrossRef]
- Fulgenzi, C.A.M.; Cheon, J.; D’Alessio, A.; Nishida, N.; Ang, C.; Marron, T.U.; Wu, L.; Saeed, A.; Wietharn, B.; Cammarota, A.; et al. Reproducible safety and efficacy of atezolizumab plus bevacizumab for HCC in clinical practice: Results of the AB-real study. Eur. J. Cancer 2022, 175, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M. Prioritized Requirements for First-Line Systemic Therapy for Hepatocellular Carcinoma: Broad Benefit with Less Toxicity. Liver Cancer 2023, 12, 1–6. [Google Scholar] [CrossRef]
- Tumeh, P.C.; Harview, C.L.; Yearley, J.H.; Shintaku, I.P.; Taylor, E.J.; Robert, L.; Chmielowski, B.; Spasic, M.; Henry, G.; Ciobanu, V.; et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature 2014, 515, 568–571. [Google Scholar] [CrossRef]
- Van Allen, E.M.; Miao, D.; Schilling, B.; Shukla, S.A.; Blank, C.; Zimmer, L.; Sucker, A.; Hillen, U.; Foppen, M.H.G.; Goldinger, S.M.; et al. Genomic correlates of response to CTLA-4 blockade in metastatic melanoma. Science 2015, 350, 207–211. [Google Scholar] [CrossRef]
- Ji, R.R.; Chasalow, S.D.; Wang, L.; Hamid, O.; Schmidt, H.; Cogswell, J.; Alaparthy, S.; Berman, D.; Jure-Kunkel, M.; Siemers, N.O.; et al. An immune-active tumor microenvironment favors clinical response to ipilimumab. Cancer Immunol. Immunother. 2012, 61, 1019–1031. [Google Scholar] [CrossRef] [PubMed]
- Bagaev, A.; Kotlov, N.; Nomie, K.; Svekolkin, V.; Gafurov, A.; Isaeva, O.; Osokin, N.; Kozlov, I.; Frenkel, F.; Gancharova, O.; et al. Conserved pan-cancer microenvironment subtypes predict response to immunotherapy. Cancer Cell 2021, 39, 845–865.e7. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, N.; Nakagawa, H. Clinico-histological and molecular features of hepatocellular carcinoma from nonalcoholic fatty liver disease. Cancer Sci. 2023, 114, 3825–3833. [Google Scholar] [CrossRef] [PubMed]
- Ruiz de Galarreta, M.; Bresnahan, E.; Molina-Sanchez, P.; Lindblad, K.E.; Maier, B.; Sia, D.; Puigvehi, M.; Miguela, V.; Casanova-Acebes, M.; Dhainaut, M.; et al. beta-Catenin Activation Promotes Immune Escape and Resistance to Anti-PD-1 Therapy in Hepatocellular Carcinoma. Cancer Discov. 2019, 9, 1124–1141. [Google Scholar] [CrossRef]
- Murai, H.; Kodama, T.; Maesaka, K.; Tange, S.; Motooka, D.; Suzuki, Y.; Shigematsu, Y.; Inamura, K.; Mise, Y.; Saiura, A.; et al. Multiomics identifies the link between intratumor steatosis and the exhausted tumor immune microenvironment in hepatocellular carcinoma. Hepatology 2023, 77, 77–91. [Google Scholar] [CrossRef]
- Magen, A.; Hamon, P.; Fiaschi, N.; Soong, B.Y.; Park, M.D.; Mattiuz, R.; Humblin, E.; Troncoso, L.; D’Souza, D.; Dawson, T.; et al. Intratumoral dendritic cell-CD4(+) T helper cell niches enable CD8(+) T cell differentiation following PD-1 blockade in hepatocellular carcinoma. Nat. Med. 2023, 29, 1389–1399. [Google Scholar] [CrossRef]
- Chen, D.S.; Mellman, I. Oncology meets immunology: The cancer-immunity cycle. Immunity 2013, 39, 1–10. [Google Scholar] [CrossRef]
- Yamada, T.; Fujiwara, N.; Kubota, N.; Matsushita, Y.; Nakatsuka, T.; Kurosaki, S.; Minami, T.; Tateishi, R.; Ichida, A.; Arita, J.; et al. Lenvatinib recruits cytotoxic GZMK+CD8 T cells in hepatocellular carcinoma. Hepatol. Commun. 2023, 7, e0209. [Google Scholar] [CrossRef]
- Zerbini, A.; Pilli, M.; Fagnoni, F.; Pelosi, G.; Pizzi, M.G.; Schivazappa, S.; Laccabue, D.; Cavallo, C.; Schianchi, C.; Ferrari, C.; et al. Increased immunostimulatory activity conferred to antigen-presenting cells by exposure to antigen extract from hepatocellular carcinoma after radiofrequency thermal ablation. J. Immunother. 2008, 31, 271–282. [Google Scholar] [CrossRef]
- Scheffer, S.R.; Nave, H.; Korangy, F.; Schlote, K.; Pabst, R.; Jaffee, E.M.; Manns, M.P.; Greten, T.F. Apoptotic, but not necrotic, tumor cell vaccines induce a potent immune response in vivo. Int. J. Cancer 2003, 103, 205–211. [Google Scholar] [CrossRef]
- Nelson, B.E.; Adashek, J.J.; Lin, S.H.; Subbiah, V. The abscopal effect in patients with cancer receiving immunotherapy. Med 2023, 4, 233–244. [Google Scholar] [CrossRef] [PubMed]
- Abou-Alfa, G.K.; Fan, J.; Heo, J.; Arai, Y.; Erinjeri, J.P.; Kuhl, C.K.; Lencioni, R.; Ren, Z.; Zeng, A.; Evans, B.; et al. 727TiP A randomised phase III study of tremelimumab (T) plus durvalumab (D) with or without lenvatinib combined with concurrent transarterial chemoembolisation (TACE) versus TACE alone in patients (pts) with locoregional hepatocellular carcinoma (HCC): EMERALD-3. Ann. Oncol. 2022, 33, S874. [Google Scholar] [CrossRef]
- Takayama, T.; Hasegawa, K.; Izumi, N.; Kudo, M.; Shimada, M.; Yamanaka, N.; Inomata, M.; Kaneko, S.; Nakayama, H.; Kawaguchi, Y.; et al. Surgery versus Radiofrequency Ablation for Small Hepatocellular Carcinoma: A Randomized Controlled Trial (SURF Trial). Liver Cancer 2022, 11, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Tateishi, R.; Fujiwara, N. Precision Locoregional Therapies for Hepatocellular Carcinoma: Percutaneous Ablation and Radiotherapy. In Hepatocellular Carcinoma: Translational Precision Medicine Approaches; Hoshida, Y., Ed.; Humana Press: New York, NY, USA; Springer Nature: Cham, Switzerland, 2019; pp. 195–224. [Google Scholar]
- Chu, K.F.; Dupuy, D.E. Thermal ablation of tumours: Biological mechanisms and advances in therapy. Nat. Rev. Cancer 2014, 14, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Duan, Y.; Yang, M.; Guo, Y.; Li, F.; Wang, J.; Si, T. The analysis of immunogenic cell death induced by ablation at different temperatures in hepatocellular carcinoma cells. Front. Cell Dev. Biol. 2023, 11, 1146195. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.Y.; Grimm, C.F.; Ritter, M.; Mohr, L.; Allgaier, H.P.; Weth, R.; Bocher, W.O.; Endrulat, K.; Blum, H.E.; Geissler, M. Activation of dendritic cells by local ablation of hepatocellular carcinoma. J. Hepatol. 2005, 43, 817–822. [Google Scholar] [CrossRef]
- den Brok, M.H.; Sutmuller, R.P.; Nierkens, S.; Bennink, E.J.; Frielink, C.; Toonen, L.W.; Boerman, O.C.; Figdor, C.G.; Ruers, T.J.; Adema, G.J. Efficient loading of dendritic cells following cryo and radiofrequency ablation in combination with immune modulation induces anti-tumour immunity. Br. J. Cancer 2006, 95, 896–905. [Google Scholar] [CrossRef]
- Mizukoshi, E.; Nakamoto, Y.; Arai, K.; Yamashita, T.; Sakai, A.; Sakai, Y.; Kagaya, T.; Yamashita, T.; Honda, M.; Kaneko, S. Comparative analysis of various tumor-associated antigen-specific t-cell responses in patients with hepatocellular carcinoma. Hepatology 2011, 53, 1206–1216. [Google Scholar] [CrossRef]
- Yang, M.; Yang, X.; Wang, S.; Xu, L.; Ke, S.; Ding, X.; Sun, W.; Gao, J. HMGB1-induced endothelial cell pyroptosis is involved in systemic inflammatory response syndrome following radiofrequency ablation of hepatic hemangiomas. Am. J. Transl. Res. 2019, 11, 7555–7567. [Google Scholar]
- Grover, A.; Sanseviero, E.; Timosenko, E.; Gabrilovich, D.I. Myeloid-Derived Suppressor Cells: A Propitious Road to Clinic. Cancer Discov. 2021, 11, 2693–2706. [Google Scholar] [CrossRef]
- Colligan, S.H.; Amitrano, A.M.; Zollo, R.A.; Peresie, J.; Kramer, E.D.; Morreale, B.; Barbi, J.; Singh, P.K.; Yu, H.; Wang, J.; et al. Inhibiting the biogenesis of myeloid-derived suppressor cells enhances immunotherapy efficacy against mammary tumor progression. J. Clin. Investig. 2022, 132, e158661. [Google Scholar] [CrossRef] [PubMed]
- Arihara, F.; Mizukoshi, E.; Kitahara, M.; Takata, Y.; Arai, K.; Yamashita, T.; Nakamoto, Y.; Kaneko, S. Increase in CD14+HLA-DR -/low myeloid-derived suppressor cells in hepatocellular carcinoma patients and its impact on prognosis. Cancer Immunol. Immunother. 2013, 62, 1421–1430. [Google Scholar] [CrossRef] [PubMed]
- Rochigneux, P.; Nault, J.C.; Mallet, F.; Chretien, A.S.; Barget, N.; Garcia, A.J.; Del Pozo, L.; Bourcier, V.; Blaise, L.; Grando-Lemaire, V.; et al. Dynamic of systemic immunity and its impact on tumor recurrence after radiofrequency ablation of hepatocellular carcinoma. Oncoimmunology 2019, 8, 1615818. [Google Scholar] [CrossRef]
- Zhao, Y.; Li, K.; Sun, J.; He, N.; Zhao, P.; Zang, C.; Yang, X.; Hu, C.; Long, J.; Zhang, H.; et al. Genomic DNA methylation profiling indicates immune response following thermal ablation treatment for HBV-associated hepatocellular carcinoma. Oncol. Lett. 2020, 20, 677–684. [Google Scholar] [CrossRef]
- Mukherjee, S.; Fried, A.; Hussaini, R.; White, R.; Baidoo, J.; Yalamanchi, S.; Banerjee, P. Phytosomal curcumin causes natural killer cell-dependent repolarization of glioblastoma (GBM) tumor-associated microglia/macrophages and elimination of GBM and GBM stem cells. J. Exp. Clin. Cancer Res. 2018, 37, 168. [Google Scholar] [CrossRef]
- Mohammadpour, H.; Pourfathollah, A.A.; Nikougoftar Zarif, M.; Shahbazfar, A.A. Irradiation enhances susceptibility of tumor cells to the antitumor effects of TNF-alpha activated adipose derived mesenchymal stem cells in breast cancer model. Sci. Rep. 2016, 6, 28433. [Google Scholar] [CrossRef] [PubMed]
- Su, T.; Huang, M.; Liao, J.; Lin, S.; Yu, P.; Yang, J.; Cai, Y.; Zhu, S.; Xu, L.; Peng, Z.; et al. Insufficient Radiofrequency Ablation Promotes Hepatocellular Carcinoma Metastasis Through N6-Methyladenosine mRNA Methylation-Dependent Mechanism. Hepatology 2021, 74, 1339–1356. [Google Scholar] [CrossRef]
- Yu, L.; Cheng, M.; Liu, J.; Ye, X.; Wei, Z.; Xu, J.; Xie, Q.; Liang, J. Crosstalk between microwave ablation and ferroptosis: The next hot topic? Front. Oncol. 2023, 13, 1099731. [Google Scholar] [CrossRef]
- Li, W.; Feng, G.; Gauthier, J.M.; Lokshina, I.; Higashikubo, R.; Evans, S.; Liu, X.; Hassan, A.; Tanaka, S.; Cicka, M.; et al. Ferroptotic cell death and TLR4/Trif signaling initiate neutrophil recruitment after heart transplantation. J. Clin. Investig. 2019, 129, 2293–2304. [Google Scholar] [CrossRef]
- Wen, Q.; Liu, J.; Kang, R.; Zhou, B.; Tang, D. The release and activity of HMGB1 in ferroptosis. Biochem. Biophys. Res. Commun. 2019, 510, 278–283. [Google Scholar] [CrossRef]
- Mandt, T.; Bangar, A.; Sauceda, C.; Das, M.; Moderbacher, C.; Ghani, M.; Webster, N.; Newton, I. Stimulating Antitumoral Immunity by Percutaneous Cryoablation and Combination Immunoadjuvant Therapy in a Murine Model of Hepatocellular Carcinoma. J. Vasc. Interv. Radiol. 2023, 34, 1516–1527.e6. [Google Scholar] [CrossRef] [PubMed]
- Osada, S.; Imai, H.; Tomita, H.; Tokuyama, Y.; Okumura, N.; Matsuhashi, N.; Sakashita, F.; Nonaka, K. Serum cytokine levels in response to hepatic cryoablation. J. Surg. Oncol. 2007, 95, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Shi, F.; Zhou, L.; Zhang, M.N.; Chen, Y.; Chang, X.J.; Lu, Y.Y.; Bai, W.L.; Qu, J.H.; Wang, C.P.; et al. Upregulation of circulating PD-L1/PD-1 is associated with poor post-cryoablation prognosis in patients with HBV-related hepatocellular carcinoma. PLoS ONE 2011, 6, e23621. [Google Scholar] [CrossRef]
- Jansen, M.C.; van Hillegersberg, R.; Schoots, I.G.; Levi, M.; Beek, J.F.; Crezee, H.; van Gulik, T.M. Cryoablation induces greater inflammatory and coagulative responses than radiofrequency ablation or laser induced thermotherapy in a rat liver model. Surgery 2010, 147, 686–695. [Google Scholar] [CrossRef] [PubMed]
- Mauda-Havakuk, M.; Hawken, N.M.; Owen, J.W.; Mikhail, A.S.; Saxena, A.; Karim, B.; Wakim, P.G.; Pritchard, W.F.; Karanian, J.W.; Wood, B.J. Comparative analysis of the immune response to RFA and cryoablation in a colon cancer mouse model. Sci. Rep. 2022, 12, 18229. [Google Scholar] [CrossRef] [PubMed]
- Galluzzi, L.; Buque, A.; Kepp, O.; Zitvogel, L.; Kroemer, G. Immunological Effects of Conventional Chemotherapy and Targeted Anticancer Agents. Cancer Cell 2015, 28, 690–714. [Google Scholar] [CrossRef]
- Tischfield, D.J.; Gurevich, A.; Johnson, O.; Gatmaytan, I.; Nadolski, G.J.; Soulen, M.C.; Kaplan, D.E.; Furth, E.; Hunt, S.J.; Gade, T.P.F. Transarterial Embolization Modulates the Immune Response within Target and Nontarget Hepatocellular Carcinomas in a Rat Model. Radiology 2022, 303, 215–225. [Google Scholar] [CrossRef] [PubMed]
- Berz, A.M.; Santana, J.G.; Iseke, S.; Gross, M.; Pekurovsky, V.; Laage Gaupp, F.; Savic, L.J.; Borde, T.; Gottwald, L.A.; Boustani, A.M.; et al. Impact of Chemoembolic Regimen on Immune Cell Recruitment and Immune Checkpoint Marker Expression following Transcatheter Arterial Chemoembolization in a VX2 Rabbit Liver Tumor Model. J. Vasc. Interv. Radiol. 2022, 33, 764–774.e764. [Google Scholar] [CrossRef]
- Ayaru, L.; Pereira, S.P.; Alisa, A.; Pathan, A.A.; Williams, R.; Davidson, B.; Burroughs, A.K.; Meyer, T.; Behboudi, S. Unmasking of alpha-fetoprotein-specific CD4(+) T cell responses in hepatocellular carcinoma patients undergoing embolization. J. Immunol. 2007, 178, 1914–1922. [Google Scholar] [CrossRef]
- Montasser, A.; Beaufrere, A.; Cauchy, F.; Bouattour, M.; Soubrane, O.; Albuquerque, M.; Paradis, V. Transarterial chemoembolisation enhances programmed death-1 and programmed death-ligand 1 expression in hepatocellular carcinoma. Histopathology 2021, 79, 36–46. [Google Scholar] [CrossRef]
- Pinato, D.J.; Murray, S.M.; Forner, A.; Kaneko, T.; Fessas, P.; Toniutto, P.; Minguez, B.; Cacciato, V.; Avellini, C.; Diaz, A.; et al. Trans-arterial chemoembolization as a loco-regional inducer of immunogenic cell death in hepatocellular carcinoma: Implications for immunotherapy. J. Immunother. Cancer 2021, 9, e003311. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Fan, W.; Liu, T.; Zhu, B.; Liu, Y.; Wang, S.; Wu, J.; Liu, J.; Zou, F.; Wei, J.; et al. TREM2(+) macrophages suppress CD8(+) T-cell infiltration after transarterial chemoembolisation in hepatocellular carcinoma. J. Hepatol. 2023, 79, 126–140. [Google Scholar] [CrossRef] [PubMed]
- Nambiar, D.K.; Aguilera, T.; Cao, H.; Kwok, S.; Kong, C.; Bloomstein, J.; Wang, Z.; Rangan, V.S.; Jiang, D.; von Eyben, R.; et al. Galectin-1-driven T cell exclusion in the tumor endothelium promotes immunotherapy resistance. J. Clin. Investig. 2019, 129, 5553–5567. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, N.; Nakagawa, H.; Enooku, K.; Kudo, Y.; Hayata, Y.; Nakatsuka, T.; Tanaka, Y.; Tateishi, R.; Hikiba, Y.; Misumi, K.; et al. CPT2 downregulation adapts HCC to lipid-rich environment and promotes carcinogenesis via acylcarnitine accumulation in obesity. Gut 2018, 67, 1493–1504. [Google Scholar] [CrossRef] [PubMed]
- Enooku, K.; Nakagawa, H.; Fujiwara, N.; Kondo, M.; Minami, T.; Hoshida, Y.; Shibahara, J.; Tateishi, R.; Koike, K. Altered serum acylcarnitine profile is associated with the status of nonalcoholic fatty liver disease (NAFLD) and NAFLD-related hepatocellular carcinoma. Sci. Rep. 2019, 9, 10663. [Google Scholar] [CrossRef] [PubMed]
- Fischer, K.; Hoffmann, P.; Voelkl, S.; Meidenbauer, N.; Ammer, J.; Edinger, M.; Gottfried, E.; Schwarz, S.; Rothe, G.; Hoves, S.; et al. Inhibitory effect of tumor cell-derived lactic acid on human T cells. Blood 2007, 109, 3812–3819. [Google Scholar] [CrossRef]
- Goetze, K.; Walenta, S.; Ksiazkiewicz, M.; Kunz-Schughart, L.A.; Mueller-Klieser, W. Lactate enhances motility of tumor cells and inhibits monocyte migration and cytokine release. Int. J. Oncol. 2011, 39, 453–463. [Google Scholar] [CrossRef]
- Savic, L.J.; Schobert, I.T.; Peters, D.; Walsh, J.J.; Laage-Gaupp, F.M.; Hamm, C.A.; Tritz, N.; Doemel, L.A.; Lin, M.; Sinusas, A.; et al. Molecular Imaging of Extracellular Tumor pH to Reveal Effects of Locoregional Therapy on Liver Cancer Microenvironment. Clin. Cancer Res. 2020, 26, 428–438. [Google Scholar] [CrossRef]
- Lugade, A.A.; Sorensen, E.W.; Gerber, S.A.; Moran, J.P.; Frelinger, J.G.; Lord, E.M. Radiation-induced IFN-gamma production within the tumor microenvironment influences antitumor immunity. J. Immunol. 2008, 180, 3132–3139. [Google Scholar] [CrossRef]
- Salem, R.; Lewandowski, R.J.; Mulcahy, M.F.; Riaz, A.; Ryu, R.K.; Ibrahim, S.; Atassi, B.; Baker, T.; Gates, V.; Miller, F.H.; et al. Radioembolization for hepatocellular carcinoma using Yttrium-90 microspheres: A comprehensive report of long-term outcomes. Gastroenterology 2010, 138, 52–64. [Google Scholar] [CrossRef]
- Sangro, B.; Inarrairaegui, M.; Bilbao, J.I. Radioembolization for hepatocellular carcinoma. J. Hepatol. 2012, 56, 464–473. [Google Scholar] [CrossRef] [PubMed]
- Chew, V.; Lee, Y.H.; Pan, L.; Nasir, N.J.M.; Lim, C.J.; Chua, C.; Lai, L.; Hazirah, S.N.; Lim, T.K.H.; Goh, B.K.P.; et al. Immune activation underlies a sustained clinical response to Yttrium-90 radioembolisation in hepatocellular carcinoma. Gut 2019, 68, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Rivoltini, L.; Bhoori, S.; Camisaschi, C.; Bergamaschi, L.; Lalli, L.; Frati, P.; Citterio, D.; Castelli, C.; Mazzaferro, V. Y(90)-radioembolisation in hepatocellular carcinoma induces immune responses calling for early treatment with multiple checkpoint blockers. Gut 2023, 72, 406–407. [Google Scholar] [CrossRef] [PubMed]
- Domouchtsidou, A.; Barsegian, V.; Mueller, S.P.; Best, J.; Ertle, J.; Bedreli, S.; Horn, P.A.; Bockisch, A.; Lindemann, M. Impaired lymphocyte function in patients with hepatic malignancies after selective internal radiotherapy. Cancer Immunol. Immunother. 2018, 67, 843–853. [Google Scholar] [CrossRef] [PubMed]
- Mole, R.H. Whole body irradiation; radiobiology or medicine? Br. J. Radiol. 1953, 26, 234–241. [Google Scholar] [CrossRef]
- Chen, L.; Zhang, R.; Lin, Z.; Tan, Q.; Huang, Z.; Liang, B. Radiation therapy in the era of immune treatment for hepatocellular carcinoma. Front. Immunol. 2023, 14, 1100079. [Google Scholar] [CrossRef]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Kurata, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Overall Survival with Durvalumab after Chemoradiotherapy in Stage III NSCLC. N. Engl. J. Med. 2018, 379, 2342–2350. [Google Scholar] [CrossRef]
- Sung, W.; Hong, T.S.; Poznansky, M.C.; Paganetti, H.; Grassberger, C. Mathematical Modeling to Simulate the Effect of Adding Radiation Therapy to Immunotherapy and Application to Hepatocellular Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2022, 112, 1055–1062. [Google Scholar] [CrossRef]
- Cao, W.; Chen, G.; Wu, L.; Yu, K.N.; Sun, M.; Yang, M.; Jiang, Y.; Jiang, Y.; Xu, Y.; Peng, S.; et al. Ionizing Radiation Triggers the Antitumor Immunity by Inducing Gasdermin E-Mediated Pyroptosis in Tumor Cells. Int. J. Radiat. Oncol. Biol. Phys. 2023, 115, 440–452. [Google Scholar] [CrossRef]
- Du, S.S.; Chen, G.W.; Yang, P.; Chen, Y.X.; Hu, Y.; Zhao, Q.Q.; Zhang, Y.; Liu, R.; Zheng, D.X.; Zhou, J.; et al. Radiation Therapy Promotes Hepatocellular Carcinoma Immune Cloaking via PD-L1 Upregulation Induced by cGAS-STING Activation. Int. J. Radiat. Oncol. Biol. Phys. 2022, 112, 1243–1255. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.; Kang, Z.; Foo, T.K.; Shen, Z.; Xia, B. Disrupted BRCA1-PALB2 interaction induces tumor immunosuppression and T-lymphocyte infiltration in HCC through cGAS-STING pathway. Hepatology 2023, 77, 33–47. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.C.; Ho, A.S.; Peng, C.L.; Chang, J.; Sie, Z.L.; Wang, C.L.; Chen, Y.L.; Chen, C.Y. Sorafenib suppresses radioresistance and synergizes radiotherapy-mediated CD8(+) T cell activation to eradicate hepatocellular carcinoma. Int. Immunopharmacol. 2022, 112, 109110. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Zhang, Y.; Hong, W.; Wang, B.; Chen, Y.; Yang, P.; Zhou, J.; Fan, J.; Zeng, Z.; Du, S. Gut microbiota modulate radiotherapy-associated antitumor immune responses against hepatocellular carcinoma Via STING signaling. Gut Microbes 2022, 14, 2119055. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Dou, X.; Chen, S.; Yu, X.; Huang, X.; Zhang, L.; Chen, Y.; Wang, J.; Yang, K.; Bugno, J.; et al. YTHDF2 inhibition potentiates radiotherapy antitumor efficacy. Cancer Cell 2023, 41, 1294–1308.e1298. [Google Scholar] [CrossRef]
- Hack, S.P.; Spahn, J.; Chen, M.; Cheng, A.L.; Kaseb, A.; Kudo, M.; Lee, H.C.; Yopp, A.; Chow, P.; Qin, S. IMbrave 050: A Phase III trial of atezolizumab plus bevacizumab in high-risk hepatocellular carcinoma after curative resection or ablation. Future Oncol. 2020, 16, 975–989. [Google Scholar] [CrossRef]
- Goyal, L.; Vogel, A.; Zhu, A.X.; Cheng, A.-L.; Yau, T.; Zhou, J.; Uppot, R.N.; Kim, E.; Malhotra, U.; Siegel, A.B.; et al. P024 KEYNOTE-937 trial in progress: Adjuvant pembrolizumab for hepatocellular carcinoma and complete radiologic response after surgical resection or local ablation. Gut 2021, 70, A22. [Google Scholar] [CrossRef]
- Knox, J.; Cheng, A.; Cleary, S.; Galle, P.; Kokudo, N.; Lencioni, R.; Park, J.; Zhou, J.; Mann, H.; Morgan, S.; et al. A phase 3 study of durvalumab with or without bevacizumab as adjuvant therapy in patients with hepatocellular carcinoma at high risk of recurrence after curative hepatic resection or ablation: EMERALD-2. Ann. Oncol. 2019, 30, iv59–iv60. [Google Scholar] [CrossRef]
- Lyu, N.; Kong, Y.; Li, X.; Mu, L.; Deng, H.; Chen, H.; He, M.; Lai, J.; Li, J.; Tang, H.; et al. Ablation Reboots the Response in Advanced Hepatocellular Carcinoma With Stable or Atypical Response During PD-1 Therapy: A Proof-of-Concept Study. Front. Oncol. 2020, 10, 580241. [Google Scholar] [CrossRef]
- Vogel, A.; Waidmann, O.; Müller, T.; Siegler, G.M.; Goetze, T.O.; Toni, E.N.D.; Gonzalez-Carmona, M.A.; Hausner, G.; Geissler, M.; Weikersthal, L.F.v.; et al. IMMULAB: A phase II trial of immunotherapy with pembrolizumab in combination with local ablation for patients with early-stage hepatocellular carcinoma (HCC). J. Clin. Oncol. 2023, 41, 555. [Google Scholar] [CrossRef]
- Shi, L.; Zhou, C.; Long, X.; Li, H.; Chen, C.; Peng, C.; Li, P.; Li, J.; Gu, S.; Liang, B.; et al. 949P Thermal ablation plus toripalimab in patients with advanced hepatocellular carcinoma: Phase I results from a multicenter, open-label, controlled phase I/II trial (IR11330). Ann. Oncol. 2021, 32, S826. [Google Scholar] [CrossRef]
- Kudo, M.; Guo, Y.; Hua, Y.; Zhao, M.; Xing, W.; Zhang, Y.; Liu, R.; Ren, Z.; Gu, S.; Lin, Z.; et al. TALENTACE: A phase III, open-label, randomized study of on-demand transarterial chemoembolization combined with atezolizumab + bevacizumab or on-demand transarterial chemoembolization alone in patients with untreated hepatocellular carcinoma. J. Clin. Oncol. 2022, 40, TPS487. [Google Scholar] [CrossRef]
- Saborowski, A.; Waldschmidt, D.; Hinrichs, J.; Ettrich, T.J.; Martens, U.M.; Mekolli, A.; Toni, E.N.D.; Berg, T.; Geißler, M.; Hausner, G.; et al. IMMUTACE: A biomarker-orientated phase II, single-arm, open-label AIO study of transarterial chemoembolization (TACE) in combination with nivolumab performed for intermediate-stage hepatocellular carcinoma (HCC; AIO-HEP-0217)—Updated efficacy results. J. Clin. Oncol. 2022, 40, 4116. [Google Scholar] [CrossRef]
- Xiaoyun, Z.; Zhu, X.; Feng, X.; Han, W.; Yan, M.L.; Xie, F.; Zhang, S.; Zhang, Y.; Jiang, X.; Peng, W.; et al. 715P The safety and efficacy of lenvatinib combined with TACE and PD-1 inhibitors (Len-TAP) versus TACE alone in the conversion resection for initially unresectable hepatocellular carcinoma: Interim results from a multicenter prospective cohort study. Ann. Oncol. 2022, 33, S870. [Google Scholar] [CrossRef]
- Fulgenzi, C.A.M.; Cortellini, A.; D’Alessio, A.; Thomas, R.; Tait, P.; Ross, P.J.; Young, A.-M.; Talbot, T.; Goldin, R.; Ward, C.; et al. A phase Ib study of pembrolizumab following trans-arterial chemoembolization (TACE) in hepatocellular carcinoma (HCC): PETAL. J. Clin. Oncol. 2022, 40, e16195. [Google Scholar] [CrossRef]
- Harding, J.J.; Yarmohammadi, H.; Reiss, K.A.; Chou, J.F.; Capanu, M.; Do, R.K.G.; Khalil, D.; Dika, I.H.E.; Giardina, J.D.; Merghoub, T.; et al. Nivolumab (NIVO) and drug eluting bead transarterial chemoembolization (deb-TACE): Preliminary results from a phase I study of patients (pts) with liver limited hepatocellular carcinoma (HCC). J. Clin. Oncol. 2020, 38, 525. [Google Scholar] [CrossRef]
- Duffy, A.G.; Ulahannan, S.V.; Makorova-Rusher, O.; Rahma, O.; Wedemeyer, H.; Pratt, D.; Davis, J.L.; Hughes, M.S.; Heller, T.; ElGindi, M.; et al. Tremelimumab in combination with ablation in patients with advanced hepatocellular carcinoma. J. Hepatol. 2017, 66, 545–551. [Google Scholar] [CrossRef]
- He, A.R.; Toskich, B. The ROWAN study: Safety and efficacy of transarterial radioembolization with Y-90 glass microspheres and the STRIDE regimen in hepatocellular carcinoma. J. Clin. Oncol. 2023, 41, TPS622. [Google Scholar] [CrossRef]
- de la Torre-Aláez, M.; Matilla, A.; Varela, M.; Iñarrairaegui, M.; Reig, M.; Lledó, J.L.; Arenas, J.I.; Lorente, S.; Testillano, M.; Márquez, L.; et al. Nivolumab after selective internal radiation therapy for the treatment of hepatocellular carcinoma: A phase 2, single-arm study. J. Immunother. Cancer 2022, 10, e005457. [Google Scholar] [CrossRef]
- Tai, D.; Loke, K.; Gogna, A.; Kaya, N.A.; Tan, S.H.; Hennedige, T.; Ng, D.; Irani, F.; Lee, J.; Lim, J.Q.; et al. Radioembolisation with Y90-resin microspheres followed by nivolumab for advanced hepatocellular carcinoma (CA 209-678): A single arm, single centre, phase 2 trial. Lancet Gastroenterol. Hepatol. 2021, 6, 1025–1035. [Google Scholar] [CrossRef]
- McRee, A.J.; Helft, P.R.; Harris, W.P.; Sanoff, H.K.; Johnson, M.; Yu, M.; O’Neil, B. A study of pembrolizumab (pembro) in combination with Y90 radioembolization in patients (pts) with poor prognosis hepatocellular carcinoma (HCC) with preserved liver function. J. Clin. Oncol. 2022, 40, 422. [Google Scholar] [CrossRef]
- Fenton, S.E.; Kircher, S.M.; Mulcahy, M.F.; Mahalingam, D.; Salem, R.; Lewandowski, R.; Kulik, L.; Benson, A.B.; Kalyan, A. A phase I study of nivolumab (NIVO) in combination with TheraSphere (Yttrium-90) in patients with advanced hepatocellular cancer. J. Clin. Oncol. 2021, 39, e16183. [Google Scholar] [CrossRef]
- Chen, Y.; Yang, P.; Du, S.; Zhou, J.; Huang, C.; Zhu, W.; Hu, Y.; Yu, Y.; Liu, T.; Zeng, Z. A phase II study of stereotactic body radiotherapy (SBRT) combined with sintilimab in patients with recurrent or oligometastatic hepatocellular carcinoma (HCC). J. Clin. Oncol. 2022, 40, 4071. [Google Scholar] [CrossRef]
- Wang, K.; Yu, H.M.; Xiang, Y.J.; Cheng, Y.Q.; Ni, Q.Z.; Guo, W.X.; Shi, J.; Feng, S.; Zhai, J.; Cheng, S.Q. Efficacy and safety of radiotherapy combined with atezolizumab plus bevacizumab in treating hepatocellular carcinoma with portal vein tumour thrombus: A study protocol. BMJ Open 2022, 12, e064688. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Yue, J.; Shi, X.; Cui, K.; Li, L.; Zhang, C.; Sun, P.; Zhong, J.; Li, Z.; Zhao, L. Protocol of notable-HCC: A phase Ib study of neoadjuvant tislelizumab with stereotactic body radiotherapy in patients with resectable hepatocellular carcinoma. BMJ Open 2022, 12, e060955. [Google Scholar] [CrossRef]
- Brown, T.J.; Minn, A.J.; Carpenter, E.L.; Ben-Josef, E.; Karasic, T.B. A phase I clinical trial of stereotactic body radiotherapy with atezolizumab and bevacizumab in advanced hepatocellular carcinoma. J. Clin. Oncol. 2023, 41, TPS626. [Google Scholar] [CrossRef]
- Juloori, A.; Katipally, R.R.; Lemons, J.M.; Singh, A.K.; Iyer, R.; Robbins, J.R.; George, B.; Hall, W.A.; Pitroda, S.P.; Arif, F.; et al. Phase 1 Randomized Trial of Stereotactic Body Radiation Therapy Followed by Nivolumab plus Ipilimumab or Nivolumab Alone in Advanced/Unresectable Hepatocellular Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2023, 115, 202–213. [Google Scholar] [CrossRef]
- Chiang, C.L.; Chiu, K.W.H.; Chan, K.S.K.; Lee, F.A.S.; Li, J.C.B.; Wan, C.W.S.; Dai, W.C.; Lam, T.C.; Chen, W.; Wong, N.S.M.; et al. Sequential transarterial chemoembolisation and stereotactic body radiotherapy followed by immunotherapy as conversion therapy for patients with locally advanced, unresectable hepatocellular carcinoma (START-FIT): A single-arm, phase 2 trial. Lancet Gastroenterol. Hepatol. 2023, 8, 169–178. [Google Scholar] [CrossRef]
- Chiang, C.L.; Chang, S.L.; Chan, S.-K.; Lee, A.S.; Chiu, K.W.H.; Yeung, V.T.Y.; Wong, N.S.M.; Lee, V.W.Y.; Lau, V.W.H.; Man, N.K.; et al. Preliminary results of sequential transarterial chemoembolization and stereotactic body radiotherapy followed by immunotherapy using single tremelimumab regular interval durvalumab in locally advanced, unresectable hepatocellular carcinoma (START-FIT using STRIDE): A single-arm, phase II study. J. Clin. Oncol. 2023, 41, 4124. [Google Scholar] [CrossRef]
- Yu, J.; Yu, X.L.; Han, Z.Y.; Cheng, Z.G.; Liu, F.Y.; Zhai, H.Y.; Mu, M.J.; Liu, Y.M.; Liang, P. Percutaneous cooled-probe microwave versus radiofrequency ablation in early-stage hepatocellular carcinoma: A phase III randomised controlled trial. Gut 2017, 66, 1172–1173. [Google Scholar] [CrossRef]
- Sherman, M. Recurrence of hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 2045–2047. [Google Scholar] [CrossRef] [PubMed]
- Number, P. IMMUTACE: A Phase 2 Single-Arm, Open-Label Study of Transarterial Chemoembolization in Combination With Nivolumab Performed for Intermediate-Stage Hepatocellular Carcinoma. Gastroenterol. Hepatol. 2021, 17, 16–17. [Google Scholar]
- Li, J.X.; Su, T.S.; Gong, W.F.; Zhong, J.H.; Yan, L.Y.; Zhang, J.; Li, L.Q.; He, M.L.; Zhang, R.J.; Du, Y.Q.; et al. Combining stereotactic body radiotherapy with camrelizumab for unresectable hepatocellular carcinoma: A single-arm trial. Hepatol. Int. 2022, 16, 1179–1187. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.H.; Lan, C.H.; Wu, K.L.; Wu, Y.M.; Jane, W.N.; Hsiao, M.; Wu, H.C. Hepatocellular carcinoma-targeted nanoparticles for cancer therapy. Int. J. Oncol. 2018, 52, 389–401. [Google Scholar] [CrossRef]
- Repáraz, D.; Aparicio, B.; Llopiz, D.; Hervás-Stubbs, S.; Sarobe, P. Therapeutic Vaccines against Hepatocellular Carcinoma in the Immune Checkpoint Inhibitor Era: Time for Neoantigens? Int. J. Mol. Sci. 2022, 23, 2022. [Google Scholar] [CrossRef]
- Fujiwara, N.; Kobayashi, M.; Fobar, A.J.; Hoshida, A.; Marquez, C.A.; Koneru, B.; Panda, G.; Taguri, M.; Qian, T.; Raman, I.; et al. A blood-based prognostic liver secretome signature and long-term hepatocellular carcinoma risk in advanced liver fibrosis. Med 2021, 2, 836–850.e10. [Google Scholar] [CrossRef]
- Pfister, D.; Nunez, N.G.; Pinyol, R.; Govaere, O.; Pinter, M.; Szydlowska, M.; Gupta, R.; Qiu, M.; Deczkowska, A.; Weiner, A.; et al. NASH limits anti-tumour surveillance in immunotherapy-treated HCC. Nature 2021, 592, 450–456. [Google Scholar] [CrossRef]
- Fujiwara, N.; Kubota, N.; Crouchet, E.; Koneru, B.; Marquez, C.A.; Jajoriya, A.K.; Panda, G.; Qian, T.; Zhu, S.; Goossens, N.; et al. Molecular signatures of long-term hepatocellular carcinoma risk in nonalcoholic fatty liver disease. Sci. Transl. Med. 2022, 14, eabo4474. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Clinical Trial Identifier (Study Acronym) * | Study Phase | #Pt. | Locations | Eligible HCC Stage | Combined ICI and TKI | ORR | DCR | Median PFS, RFS | OS | TRAE † | Clinical Trial Status (As of 15 September 2023) | Reference |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ablation (or surgical resection) | ||||||||||||
| NCT04102098 (IMbrave050) | 3 | 668 | Global | Adjuvant | Atezolizumab + bevacizumab | - | - | 22.1 m | - | 41.0% | Active, not recruiting | [87] |
| NCT03383458 (CheckMate 9DX) | 3 | 545 | Global | Adjuvant | Nivolumab | - | - | - | - | - | Active, not recruiting | |
| NCT03867084 (KEYNOTE-937) | 3 | 950 | Global | Adjuvant | Pembrolizumab | - | - | - | - | - | Active, not recruiting | [88] |
| NCT03847428 (EMERALD-2) | 3 | 908 | Global | Adjuvant | Durvalumab +/− bevacizumab | - | - | - | - | - | Active, not recruiting | [89] |
| NCT04727307 (AB-LATE02) | 2 | 202 | France | Neoadjuvant | Atezolizumab + bevacizumab | - | - | - | - | - | Recruiting | n.a. |
| NCT03939975 | 2 | 50 | China | BCLC B/C | Pembrolizumab or nivolumab or toripalimab | 24.0% | 68.0% | 5.0 m | 16.9 m | 14.0% | Completed | [90] |
| NCT03753659 (IMMULAB) | 2 | 30 | Germany | BCLC A | Pembrolizumab | - | - | 17.4 m | - | - | Active, not recruiting | [91] |
| NCT03864211 (IR11330) | 1/2 | 145 | China | BCLC C | Toripalimab | 31.2–37.5% | - | - | - | 25.0% | Active, not recruiting | [92] |
| NCT04652440 | 1/2 | 30 | China | BCLC A/B | Tislelizumab | - | - | - | - | - | Recruiting | n.a. |
| TACE | ||||||||||||
| NCT04340193 (CheckMate 74W) | 3 | 26 | Global | BCLC B/C | Nivolumab + ipilimumab | - | - | - | - | - | Active, not recruiting | n.a. |
| NCT04712643 (TALENTACE) | 3 | 342 | China, Japan | BCLC B/C | Atezolizumab + bevacizumab | - | - | - | - | - | Active, not recruiting | [93] |
| NCT05301842 (EMERALD-3) | 3 | 725 | Global | BCLC B/C | Durvalumab + tremelimumab +/− lenvatinib | - | - | - | - | - | Recruiting | [32] |
| NCT04268888 (TACE-3) | 2/3 | 522 | United Kingdom | BCLC B | Nivolumab | - | - | - | - | - | Recruiting | n.a. |
| NCT03572582 (IMMUTACE) | 2 | 49 | Germany | BCLC B | Nivolumab | 71.4% | 75.5% | 7.2 m | 28.3 m | 34.7% | Completed | [94] |
| NCT04814030 (AIPD1) | 2 | 80 | China | BCLC C | Sintilimab | - | - | - | - | - | Recruiting | n.a. |
| NCT05751343 | 2 | 55 | China | BCLC B/C | Atezolizumab + bevacizumab | - | - | - | - | - | Recruiting | n.a. |
| NCT03638141 | 2 | 30 | United States | BCLC B | Durvalumab + tremelimumab | - | - | - | - | - | Recruiting | n.a. |
| NCT04997850 | 1/2 | 142 | China | BCLC B/C | Camrelizumab or sintilimab + lenvatinib | 78.9% | 94.4% | 17.1 m | - | 53.5% | Enrolling by invitation | [95] |
| NCT03397654 (PETAL) | 1/2 | 26 | United Kingdom | BCLC B | Pembrolizumab | - | - | 10.8 m | - | 21.0% | Active, not recruiting | [96] |
| NCT03143270 | 1 | 20 | United States | BCLC B | Nivolumab | 22.2% | 100.0% | - | - | - | Active, not recruiting | [97] |
| Ablation and TACE | ||||||||||||
| NCT01853618 | 1/2 | 61 | United States | BCLC B/C | Tremelimumab | 26.3% | - | 7.4 m | 12.3 m | - | Completed | [98] |
| NCT04220944 | 1 | 45 | China | BCLC B/C | Sintilimab | - | - | - | - | - | Recruiting | n.a. |
| TARE | ||||||||||||
| NCT05377034 (STRATUM) | 2 | 176 | Singapore | BCLC B/C | Atezolizumab + bevacizumab | - | - | - | - | - | Recruiting | n.a. |
| NCT05063565 (ROWAN) | 2 | 100 | United States, Spain | BCLC B/C | Durvalumab + tremelimumab | - | - | - | - | - | Recruiting | [99] |
| NCT03380130 (NASIR-HCC) | 2 | 41 | Spain | BCLC B/C | Nivolumab | 41.5% | 92.7% | 9.0 m | 20.9 m | 21.4% | Completed | [100] |
| NCT03033446 | 2 | 40 | Singapore | BCLC B/C | Nivolumab | 30.6% | - | - | - | 6.0% | Active, not recruiting | [101] |
| NCT03099564 | 1 | 30 | United States | BCLC B/C | Pembrolizumab | 27.0% | 84.7% | 8.6 m | 22.0 m | - | Active, not recruiting | [102] |
| NCT04605731 | 1 | 32 | United States | BCLC B/C | Durvalumab + tremelimumab | - | - | - | - | - | Recruiting | n.a. |
| NCT02837029 | 1 | 27 | United States | BCLC B/C | Nivolumab | - | 82.0% | - | - | - | Completed | [103] |
| NCT03812562 | 1 | 2 | United States | Neoadjuvant | Nivolumab | - | - | - | - | - | Active, not recruiting | n.a. |
| SBRT | ||||||||||||
| NCT04167293 (ISBRT01) | 2/3 | 116 | China | BCLC C | Sintilimab | - | - | - | - | - | Recruiting | n.a. |
| NCT04913480 | 2 | 37 | Hong Kong | BCLC B/C | Durvalumab | - | - | - | - | - | Recruiting | n.a. |
| NCT03857815 | 2 | 30 | China | BCLC B | Sintilimab | 96.0% | - | - | - | 4.0% | Recruiting | [104] |
| NCT05396937 | 2 | 42 | China | BCLC C | Atezolizumab + bevacizumab | - | - | - | - | - | Recruiting | [105] |
| NCT03316872 | 2 | 30 | Canada | BCLC B/C | Pembrolizumab | - | - | - | - | - | Recruiting | n.a. |
| NCT05286320 | 1/2 | 27 | Taiwan | BCLC B/C | Pembrolizumab + lenvatinib | Not yet recruiting | n.a. | |||||
| NCT04857684 | 1 | 20 | United States | Neoadjuvant | Atezolizumab + bevacizumab | - | - | - | - | - | Recruiting | n.a. |
| NCT05185531 (Notable-HCC) | 1 | 20 | China | Neoadjuvant | Tislelizumab | - | - | - | - | - | Recruiting | [106] |
| NCT05096715 | 1 | 20 | United States | BCLC B/C | Atezolizumab + bevacizumab | - | - | - | - | - | Not yet recruiting | n.a. |
| NCT05488522 | 1 | 18 | United States | BCLC B/C | Atezolizumab + bevacizumab | - | - | - | - | - | Recruiting | [107] |
| NCT03203304 | 1 | 14 | United States | BCLC B/C | Nivolumab + ipilimumab | 57.1% | - | 11.6 m | 41.6 m | 61.6% | Terminated | [108] |
| TACE and SBRT | ||||||||||||
| NCT03817736 (START-FIT) | 2 | 33 | Hong Kong | BCLC B/C | Avelumab | 42.4% | - | - | - | 33.3% | Active, not recruiting | [109] |
| NCT04988945 | 2 | 33 | Hong Kong | BCLC B/C | Durvalumab + tremelimumab | 81.3% | - | - | - | 31.3% | Recruiting | [110] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamai, Y.; Fujiwara, N.; Tanaka, T.; Mizuno, S.; Nakagawa, H. Combination Therapy of Immune Checkpoint Inhibitors with Locoregional Therapy for Hepatocellular Carcinoma. Cancers 2023, 15, 5072. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15205072
Tamai Y, Fujiwara N, Tanaka T, Mizuno S, Nakagawa H. Combination Therapy of Immune Checkpoint Inhibitors with Locoregional Therapy for Hepatocellular Carcinoma. Cancers. 2023; 15(20):5072. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15205072
Chicago/Turabian StyleTamai, Yasuyuki, Naoto Fujiwara, Takamitsu Tanaka, Shugo Mizuno, and Hayato Nakagawa. 2023. "Combination Therapy of Immune Checkpoint Inhibitors with Locoregional Therapy for Hepatocellular Carcinoma" Cancers 15, no. 20: 5072. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15205072