Multi-Magnet Cochlear Implant Technology and Magnetic Resonance Imaging: The Safety Issue

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johnson, B.J.; Macielak, R.J.; Watson, R.E.; Heimer, J.M.; Wiste, B.J.; Lane, J.I.; Edmonson, H.A.; Carlson, M.L. Magnetic Resonance Imaging in Patients with Cochlear Implants without Magnet Removal: A Radiology-Administered Protocol to Enhance Operational Efficiency and Improve Workflow. Otol. Neurotol. 2023, 44, 664–671. [Google Scholar]
- Erhardt, J.B.; Fuhrer, E.; Gruschke, O.G.; Leupold, J.; Wapler, M.C.; Hennig, J.; Stieglitz, T.; Korvink, J.G. Should patients with brain implants undergo MRI? J. Neural. Eng. 2018, 15, 041002. [Google Scholar] [CrossRef]
- Bestourous, D.E.; Davidson, L.; Reilly, B.K. A Review of Reported Adverse Events in MRI-Safe and MRI-Conditional Cochlear Implants. Otol. Neurotol. 2022, 43, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Technavio. Cochlear Implants Market by End-user, Product, and Geography—Forecast and Analysis 2023–2027. 2023, p. 151. Available online: https://www.technavio.com/report/cochlear-implants-market-industry-analysis. (accessed on 3 February 2024).
- Srinivasan, R.; So, C.W.; Amin, N.; Jaikaransingh, D.; D‘Arco, F.; Nash, R. A review of the safety of MRI in cochlear implant patients with retained magnets. Clin. Radiol. 2019, 74, e9–e972. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.C.; Effendi, F.F.; Kosik, R.O.; Lee, W.J.; Wang, L.J.; Juan, C.J.; Chan, W.P. Utilization of CT and MRI scanning in Taiwan, 2000–2017. Insights Imaging 2023, 14, 23. [Google Scholar] [CrossRef] [PubMed]
- Businesswire. Growth of MRI Systems Market to Be Impacted by the Software Advances in MRI Technology|Technavio. Available online: https://www.businesswire.com/news/home/20191018005143/en/Growth-of-MRI-Systems-Market-to-Be-Impacted-by-the-Software-Advances-in-MRI-Technology-Technavio (accessed on 3 February 2024).
- Dong, S.Z.; Zhu, M.; Bulas, D. Techniques for minimizing sedation in pediatric MRI. J. Magn. Reason. Imaging 2019, 50, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Advanced Bionics. MRI Safety Information for the HiRes Ultra 3D Cochlear Implant. Available online: https://www.advancedbionics.com/us/en/portals/professional-portal/products/mri-safety.html (accessed on 3 February 2024).
- Loth, A.G.; Fischer, K.; Hey, A.K.; Weiß, R.; Leinung, M.; Burck, I.; Linke, A.; Kramer, S.; Stöver, T.; Helbig, S. Magnetic Resonance Imaging in Patients with Hearing Implants—Follow-up on Prevalence and Complications. Otol. Neurotol. 2021, 42, 1334–1341. [Google Scholar] [CrossRef] [PubMed]
- Cass, N.D.; Honce, J.M.; O’Dell, A.L.; Gubbels, S.P. First MRI With New Cochlear Implant with Rotatable Internal Magnet System and Proposal for Standardization of Reporting Magnet-Related Artifact Size. Otol. Neurotol. 2019, 40, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Fussell, W.L.; Patel, N.S.; Carlson, M.L.; Neff, B.A.; Watson, R.E.; Lane, J.I.; Driscoll, C.L.W. Cochlear Implants and Magnetic Resonance Imaging: Experience with over 100 Studies Performed with Magnets in Place. Otol. Neurotol. 2021, 42, 51–58. [Google Scholar] [CrossRef]
- Canzi, P.; Luzzi, S.; Carlotto, E.; Simoncelli, A.; Brondino, N.; Marconi, S.; Magnetto, M.; Lucifero, G.A.; Avato, I.; Manfrin, M.; et al. Customized Cochlear Implant Positioning in a Patient with a Low-Grade Glioma: Towards the Best MRI Artifact Management. Otol. Neurotol. 2022, 43, e628–e634. [Google Scholar] [CrossRef]
- MED-EL. Medical procedures for MED-EL Implant Systems. Available online: https://www.medel.com/docs/default-source/isi-important-safety-information/languages/en-english/ci-cochlear-implants/aw33289_150_manual-medical-procedures-ci-abi-systems-en-english-eu.pdf (accessed on 3 February 2024).
- Cochlear. CochlearTM Nucleus® Implants Magnetic Resonance Imaging (MRI) Guidelines. Available online: https://www.cochlear.com/us/en/professionals/resources-and-training/mri-guidelines (accessed on 4 February 2024).
- Eerkens, H.J.; Smits, C.; Hofman, M.B.M. Cochlear Implant Magnet Dislocation: Simulations and Measurements of Force and Torque at 1.5T Magnetic Resonance Imaging. Ear. Hear. 2021, 42, 1276–1283. [Google Scholar] [CrossRef]
- Leinung, M.; Loth, A.; Gröger, M.; Burck, I.; Vogl, T.; Stöver, T.; Helbig, S. Cochlear implant magnet dislocation after MRI: Surgical management and outcome. Eur. Arch. Otorhinolaryngol. 2020, 277, 1297–1304. [Google Scholar] [CrossRef]
- Alberalar, N.D.; Reis, J.; Piechotta, P.L.; Beetz, N.L.; Fehrenbach, U.; Geisel, D.; Thomas, A.; Busse, H.; Denecke, T. Complications of cochlear implants with MRI scans in different body regions: Type, frequency and impact. Insights Imaging 2023, 14, 9. [Google Scholar] [CrossRef] [PubMed]
- Canzi, P.; Aprile, F.; Simoncelli, A.; Manfrin, M.; Magnetto, M.; Lafe, E.; Minervini, D.; Avato, I.; Terrani, S.; Scribante, A.; et al. MRI-induced artifact by a cochlear implant with a novel magnet system: An experimental cadaver study. Eur. Arch. Otorhinolaryngol. 2021, 278, 3753–3762. [Google Scholar] [CrossRef] [PubMed]
- Tysome, J.R.; Tam, Y.C.; Patterson, I.; Graves, M.J.; Gazibegovic, D. Assessment of a Novel 3T MRI Compatible Cochlear Implant Magnet: Torque, Forces, Demagnetization, and Imaging. Otol. Neurotol. 2019, 40, e966–e974. [Google Scholar] [CrossRef]
- Canzi, P.; Berrettini, S.; Albera, A.; Barbara, M.; Bruschini, L.; Canale, A.; Carlotto, E.; Covelli, E.; Cuda, D.; Dispenza, F.; et al. Current trends on subtotal petrosectomy with cochlear implantation in recalcitrant chronic middle ear disorders. Acta Otorhinolaryngol. Ital. 2023, 43 (Suppl. S1), S67–S75. [Google Scholar] [CrossRef]
- Grupe, G.; Wagner, J.; Hofmann, S.; Stratmann, A.; Mittmann, P.; Ernst, A.; Todt, I. Prevalence and complications of MRI scans of cochlear implant patients. HNO 2017, 65 (Suppl. S1), 35–40. [Google Scholar] [CrossRef]
- Advanced Bionics. Technical Specifications HiRes Ultra 3D Cochlear Implant. Available online: https://www.advancedbionics.com/content/dam/advancedbionics/Documents/Regional/en-gb/Professional/Ultra-3D-Tech-Specs-Brochure.pdf (accessed on 7 April 2024).
- Med-El. Synchrony 2 Cochlear Implant. Available online: https://sf.cdn.medel.com/docs/librariesprovider2/product/synchrony2/med-el_synchrony-2-factsheet.pdf?sfvrsn=51f16642_4 (accessed on 7 April 2024).
- Cochlear. Cochlear Nucleus Profile Plus Series Implant. Available online: https://www.cochlear.com/us/en/professionals/products-and-candidacy/nucleus/implant/nucleus-profile-plus (accessed on 7 April 2024).
- Todt, I.; Guerkov, R.; Gehl, H.B.; Sudhoff, H. Comparison of Cochlear Implant Magnets and Their MRI Artifact Size. BioMed Res. Int. 2020, 2020, 5086291. [Google Scholar] [CrossRef]
- Canzi, P.; Magnetto, M.; Simoncelli, A.; Manfrin, M.; Aprile, F.; Lafe, E.; Carlotto, E.; Avato, I.; Scribante, A.; Preda, L.; et al. The role of cochlear implant positioning on MR imaging quality: A preclinical in vivo study with a novel implant magnet system. Eur. Arch. Otorhinolaryngol. 2022, 279, 2889–2898. [Google Scholar] [CrossRef]
- Winchester, A.; Kay-Rivest, E.; Bruno, M.; Hagiwara, M.; Moonis, G.; Jethanamest, D. Image Quality and Artifact Reduction of a Cochlear Implant with Rotatable Magnets. Otol. Neurotol. 2023, 44, e223–e229. [Google Scholar] [CrossRef]
- Ay, N.; Gehl, H.B.; Sudhoff, H.; Todt, I. Effect of head position on cochlear implant MRI artifact. Eur. Arch. Otorhinolaryngol. 2021, 278, 2763–2767. [Google Scholar] [CrossRef] [PubMed]
- Sharon, J.D.; Northcutt, B.G.; Aygun, N.; Francis, H.W. Magnetic Resonance Imaging at 1.5 Tesla with a Cochlear Implant Magnet in Place: Image Quality and Usability. Otol. Neurotol. 2016, 37, 1284–1290. [Google Scholar] [CrossRef] [PubMed]
- Amin, N.; Pai, I.; Touska, P.; Connor, S.E.J. Utilization of SEMAC-VAT MRI for improved visualization of posterior fossa structures in patients with cochlear implants. Otol. Neurotol. 2021, 42, e451–e458. [Google Scholar] [CrossRef] [PubMed]
- Canzi, P.; Carlotto, E.; Simoncelli, A.; Lafe, E.; Scribante, A.; Minervini, D.; Nardo, M.; Malpede, S.; Chiapparini, L.; Benazzo, M. The usefulness of the O-MAR algorithm in MRI skull base assessment to manage cochlear implant-related artifacts. Acta Otorhinolaryngol. Ital. 2023, 43, 273–282. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Questions | Answers | |
|---|---|---|
| D E M | Have you ever had an MRI scan since you had been provided with an CI? If no, end of questionnaire | |
| What is your gender and date of birth? | ||
| When did you undergo cochlear implantation? | ||
| M R I | When did you undergo your first MRI scan with the CI? | |
| Which was the manufacturer of the MRI scanner? | ||
| Which was the magnetic field strength used? | ||
| Where conditions regarding maximum specific absorption rate (SAR) observed? | ||
| Which body region was examined? | ||
| What was the indication for the execution of the MRI scan? | ||
| Do you know if and what precautions have been taken regarding MRI? | ||
| C O M P L I C | Has the examination been discontinued? If yes why? | |
| Did you have any pain during the examination? If yes, how strong this was? where was it located? | ||
| Did you experiment any other symptoms during the MRI? | ||
| Did your hearing get worse after the MRI? | ||
| Did your need a refit of the speech processor after the MRI? | ||
| Did you need an external stronger magnet after the MRI? | ||
| Did the internal magnet change its position during the MRI? | ||
| Have other complications occurred? | ||
| Have any special measures been taken after MRI? (Please specify) |
| Authors, Year | Subjects | Scans | Scanner Model | Tesla | SAR | Examined Region | Preventive Measures | Complications |
|---|---|---|---|---|---|---|---|---|
| Cass et al., 2019 [11] | 1 | 1 | Philips | 1.5 | NA | Brain | NA | None |
| Fussel et al., 2020 [12] | 1 | 1 | NA | 1.5 | Max 3.2 | NA | None | None |
| Johnson et al., 2023 [1] | 22 | 22 | NA | 1.5, 3 | Max 1 | NA | None | None |
| Canzi et al., 2022 [13] | 1 | 1 | Philips | 1.5 | 2.6 | Brain | None | None |
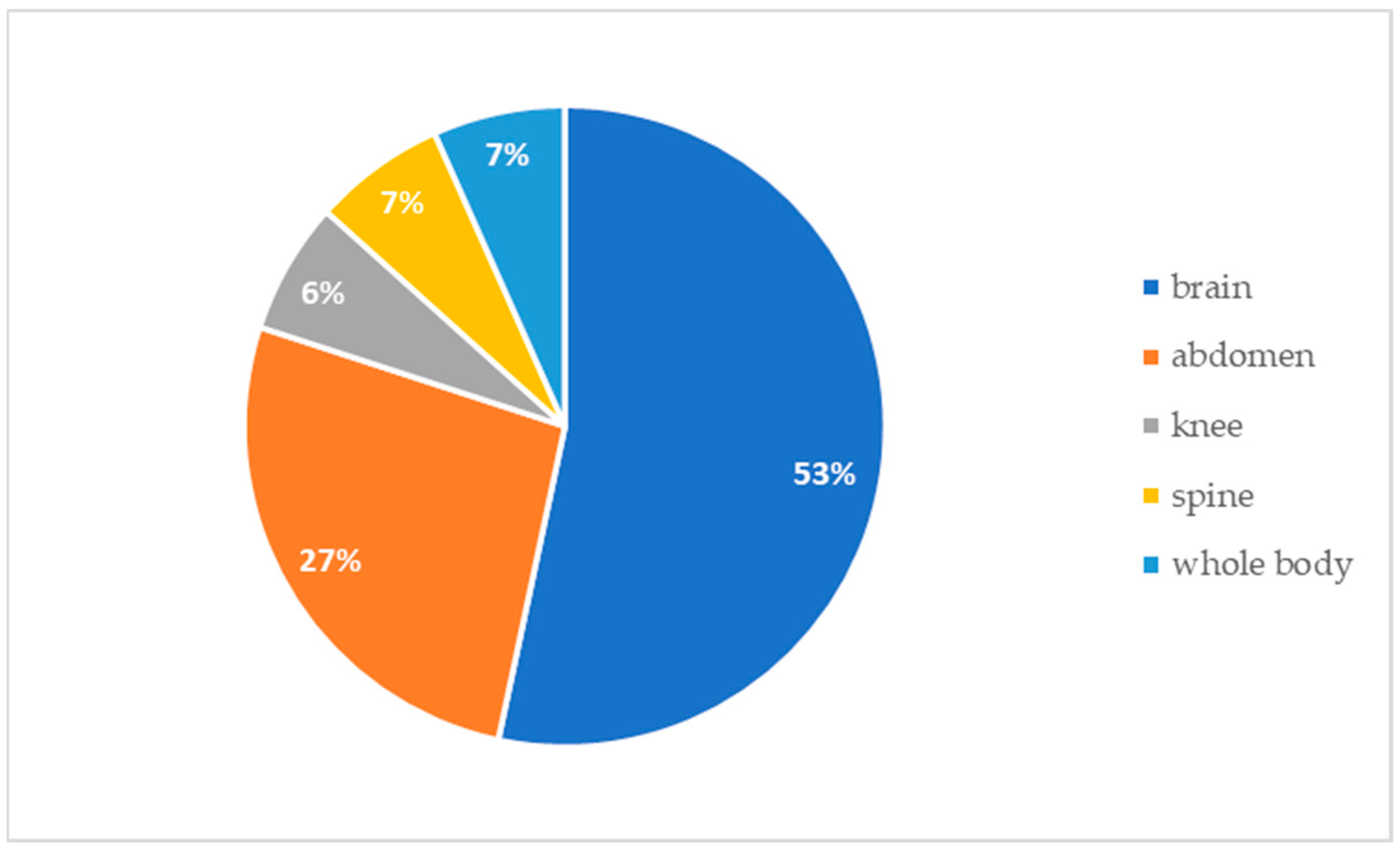
| Our experience | 47 | 65 | Philips, General Electric | 1.5 | Max 3.2 head Max 2.6 body | 1 Whole body 1 Spine 1 Knee 4 Abdomen 58 Brain | 55 None 8 Wrap (6 with LA) 2 Sedation | 62 None 3 Pain (1 exam interruption) |
| 3 | Max 2.6 head Max 2.0 body |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canzi, P.; Carlotto, E.; Zanoletti, E.; Frijns, J.H.M.; Borsetto, D.; Caruso, A.; Chiapparini, L.; Ciorba, A.; Conte, G.; Creber, N.; et al. Multi-Magnet Cochlear Implant Technology and Magnetic Resonance Imaging: The Safety Issue. Audiol. Res. 2024, 14, 401-411. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres14030034
Canzi P, Carlotto E, Zanoletti E, Frijns JHM, Borsetto D, Caruso A, Chiapparini L, Ciorba A, Conte G, Creber N, et al. Multi-Magnet Cochlear Implant Technology and Magnetic Resonance Imaging: The Safety Issue. Audiology Research. 2024; 14(3):401-411. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres14030034
Chicago/Turabian StyleCanzi, Pietro, Elena Carlotto, Elisabetta Zanoletti, Johan H. M. Frijns, Daniele Borsetto, Antonio Caruso, Luisa Chiapparini, Andrea Ciorba, Giorgio Conte, Nathan Creber, and et al. 2024. "Multi-Magnet Cochlear Implant Technology and Magnetic Resonance Imaging: The Safety Issue" Audiology Research 14, no. 3: 401-411. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres14030034