Real-World Analysis of Post-Progression Treatment Patterns and Outcomes for EGFR Mutation-Positive Patients Treated with First-Line Osimertinib

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
Clinical Response and Outcome to Systemic Therapies
2.2. Statistical Methods
3. Results
3.1. Baseline Characteristics and Response to Osimertinib
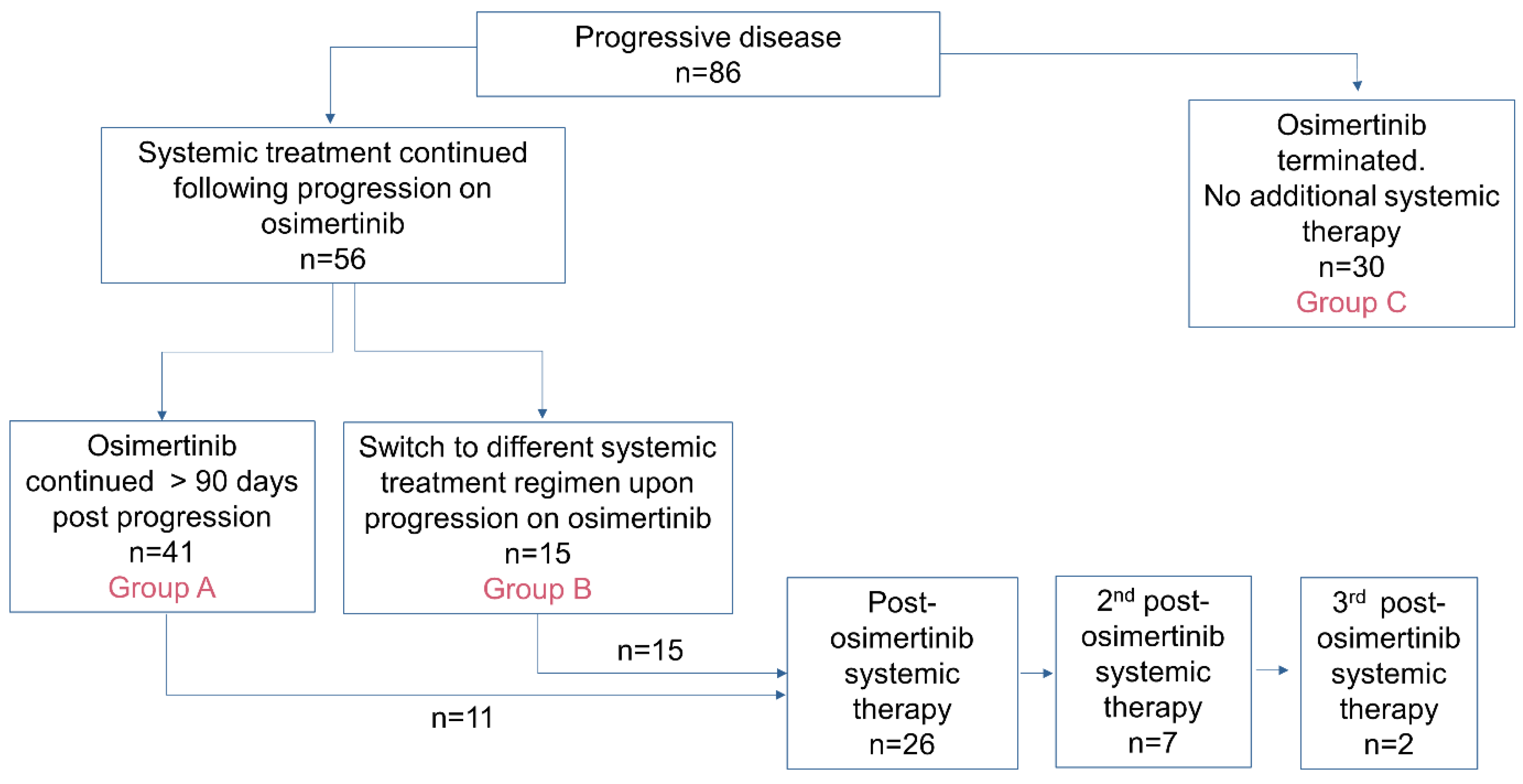
3.2. Post-Osimertinib Treatment Patterns
- Group A (n = 41): upon progression, 1L osimertinib was continued >90 days.
- Group B (n = 15): upon progression, 1L osimertinib was terminated and 2L systemic therapy was initiated.
- Group C (n = 30): upon progression, 1L osimertinib was terminated, and no further systemic therapy was received.

3.3. CNS Disease and Non-Systemic Modes of Disease Control
3.4. Systemic Therapy Regimens Post-Progression
3.4.1. Osimertinib Therapy > 90 Day Post Progression
3.4.2. Second-Line Systemic Therapy Regimens Post-Progression
3.5. Treatment Strategy and Outcome
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Del Rivero, J.; Enewold, L.; Thomas, A. Metastatic lung cancer in the age of targeted therapy: Improving long-term survival. Transl. Lung Cancer Res. 2016, 5, 727–730. [Google Scholar] [CrossRef] [PubMed]
- Tudor, R.A.; D’Silva, A.; Tremblay, A.; MacEachern, P.; Morris, D.; Kopciuk, K.; Bebb, D.G. Beyond disease-progression: Clinical outcomes after EGFR-TKIs in a cohort of EGFR mutated NSCLC patients. PLoS ONE 2017, 12, e0181867. [Google Scholar] [CrossRef] [PubMed]
- Recondo, G.; Facchinetti, F.; Olaussen, K.A.; Besse, B.; Friboulet, L. Making the first move in EGFR-driven or ALK-driven NSCLC: First-generation or next-generation TKI? Nat. Rev. Clin. Oncol. 2018, 15, 694–708. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.; Morgensztern, D.; Boshoff, C. The biology and management of non-small cell lung cancer. Nature 2018, 553, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Cardarella SLydon, C.; Dahlberg, S.; Jackman, D.; Jänne, P.; Johnson, B. Five-Year Survival in EGFR-Mutant Metastatic Lung Adenocarcinoma Treated with EGFR-TKIs. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2016, 11, 556–565. [Google Scholar] [CrossRef] [PubMed]
- Inoue, A.; Yoshida, K.; Morita, S.; Imamura, F.; Seto TOkamoto, I.; Nakagawa, K.; Yamamoto, N.; Muto, S.; Fukuoka, M. Characteristics and overall survival of EGFR mutation-positive non-small cell lung cancer treated with EGFR tyrosine kinase inhibitors: A retrospective analysis for 1660 Japanese patients. Jpn. J. Clin. Oncol. 2016, 46, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Lim, S.H.; Kim, M.; Kim, S.; Jung, H.A.; Chang, W.J.; Choi, M.K.; Lee, S.Y.; Sun, J.M.; Ahn, J.S.; et al. Is there any predictor for clinical outcome in EGFR mutant NSCLC patients treated with EGFR TKIs? Cancer Chemother. Pharmacol. 2014, 73, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Kerr, K.M.; Bubendorf, L.; Edelman, M.J.; Marchetti, A.; Mok, T.; Novello, S.; O’Byrne, K.; Stahel, R.; Peters, S.; Felip, E. Second ESMO consensus conference on lung cancer: Pathology and molecular biomarkers for non-small-cell lung cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2014, 25, 1681–1690. [Google Scholar] [CrossRef] [PubMed]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29 (Suppl. S4), iv192–iv237. [Google Scholar] [CrossRef]
- Soria, J.C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskylyong, B.; Kee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in Untreated EGFR-Mutated Advanced Non–Small-Cell Lung Cancer. N. Eng. J. Med. 2017, 378, 113–125. [Google Scholar] [CrossRef]
- Lorenzi, M.; Ferro, A.; Cecere, F.; Scattolin, D.; Del Conte, A.; Follador, A.; Pilotto, S.; Polo, V.; Santarpis, M.; Chiari, R.; et al. First-Line Osimertinib in Patients with EGFR-Mutant Advanced Non-Small Cell Lung Cancer: Outcome and Safety in the Real World: FLOWER Study. Oncologist 2022, 47, e87–e115. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.S.; Ahmed, I.; Miao, E.; Chung, S.; Patel, K.; Kohn, N.; Seetharamu, N. A real world analysis of first line treatment of advanced EGFR mutated non-small cell lung cancer: A multi-center, retrospective study. J. Oncol. Pharm. Pract. 2022, 28, 1140–1151. [Google Scholar] [CrossRef] [PubMed]
- Fu, K.; Xie, F.; Wang, F.; Fu, L. Therapeutic strategies for EGFR-mutated non-small cell lung cancer patients with osimertinib resistance. J. Hematol. Oncol. 2022, 15, 173. [Google Scholar] [CrossRef] [PubMed]
- Melosky, B.; Banerji, S.; Blais, N.; Chu, Q.; Juergens, R.; Leighl, N.B.; Liu, G.; Cheema, P. Canadian consensus: A new systemic treatment algorithm for advanced EGFR-mutated non-small-cell lung cancer. Curr. Oncol. 2020, 27, e146–e155. [Google Scholar] [CrossRef] [PubMed]
- Janne, P. WCLC 2023—Osimertinib with/without Platinum-Based Chemotherapy as First-line Treatment in Patients with EGFRm Advanced NSCLC (FLAURA2). Plenary Session 3. In Proceedings of the World Conference on Lung Cancer, Singapore, 11 September 2023; Available online: https://cattendee.abstractsonline.com/meeting/10925/presentation/2752 (accessed on 30 October 2023).
- Passaro, A.; Wang, J.; Wang, Y.; Lee, S.-H.; Melosky, B.; Shih, J.-Y.; Wang, J.; Azuma, K.; Juan-Vidal, O.; Cono, M.; et al. Amivantamab plus chemotherapy with and without lazertinib in EGFR-mutant advanced NSCLC after disease progression on osimertinib: Primary results from the phase 3 MARIPOSA-2 study. Ann. Oncol. 2023, 35, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Cho, B. Amivantamab plus lazertinib vs osimertinib as first-line treatment in patients with EGFR-mutated, advanced non-small cell lung cancer (NSCLC): Primary results from MARIPOSA, a phase III, global, randomized, controlled trial. Presidential Symposium 3. In Proceedings of the ESMO Congress, Madrid, Spain, 23 October 2023. [Google Scholar]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Edge, S.; Greene, F.; Bryd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. (Eds.) AJCC Cancer Staging Manual, 8th ed.; Springer International Publishing: Berlin/Heidelberg, Germany; American Joint Commision on Cancer: Chicago, IL, USA, 2017. [Google Scholar]
- Lindeman, N.I.; Cagle, P.T.; Aisner, D.L.; Arcila, M.E.; Beasley, M.B.; Bernicker, E.H.; Colasacco, C.; Dacic, S.; HIrsch, F.R.; Kerr, K.; et al. Updated Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment with Targeted Tyrosine Kinase Inhibitors: Guideline from the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology. Arch. Pathol. Lab. Med. 2018, 142, 321–346. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Izano, M.A.; Tran, N.; Fu, A.; Toland, L.; Idryo, D.; Hilbelink, R.; Tu, H.; Hsu, H.; Sommers, C.; Riothe, M.; et al. Implementing Real-World RECIST-based Tumor Response Assessment in Patients With Metastatic Non-small Cell Lung Cancer. Clin. Lung Cancer 2022, 23, 191–194. [Google Scholar] [CrossRef]
- Fleming, T.R.; Rothmann, M.D.; Lu, H.L. Issues in Using Progression-Free Survival When Evaluating Oncology Products. J. Clin. Oncol. 2009, 27, 2874–2880. [Google Scholar] [CrossRef] [PubMed]
- Stata Statistical Software, Release 12 [Computer program]; StataCorp: College Station, TX, USA, 2011.
- Ramalingam, S.S.; Vansteenkiste, J.; Planchard, D.; Cho, B.C.; Gray, J.E.; Ohe, Y.; Zhou, C.; Reungwetwattana, T.; Cheng, Y.; Chewaskulyong, B.; et al. Overall Survival with Osimertinib in Untreated, EGFR-Mutated Advanced NSCLC. N. Eng. J. Med. 2020, 382, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Griesinger, F.; Roeper, J.; Pöttgen, C.; Willborn, K.C.; Eberhardt, W.E.E. Brain metastases in ALK-positive NSCLC—Time to adjust current treatment algorithms. Oncotarget 2018, 9, 35181–35194. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Bi, J.; Moreira, A.; Chachoua Am Velcheti, V.; Lay, S.C.M.; Puneka, S.R.; Sabri, J.K.; Shum, E. Real-world clinical outcomes in a U.S. Asian population with stage IV NSCLC treated with osimertinib (Osi) stratified by EGFR subtype. JCO 2023, 41 (Suppl. S16), e21128. [Google Scholar] [CrossRef]
- Winfree, K.B.; Sheffield, K.M.; Cui, Z.L.; Sugihara, T.; Feliciano, J. Study of patient characteristics, treatment patterns, EGFR testing patterns and outcomes in real-world patients with EGFRm+ non-small cell lung cancer. Curr. Med. Res. Opin. 2022, 38, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Zhou, F.; Liu, Z.; Xiong, A.; Jia, Y.; Zhou, S.; Zhou, C.; Li, X.; Jian, R.; Han, R.; et al. Predictive and prognostic significance of M descriptors of the 8th TNM classification for advanced NSCLC patients treated with immune checkpoint inhibitors. Transl. Lung Cancer Res. 2020, 9, 1053–1066. [Google Scholar] [CrossRef] [PubMed]
- Nieva, J.; Reckamp, K.L.; Potter, D.; Taylor, A.; Sun, P. Retrospective Analysis of Real-World Management of EGFR-Mutated Advanced NSCLC, After First-Line EGFR-TKI Treatment: US Treatment Patterns, Attrition, and Survival Data. Drugs-Real World Outcomes 2022, 9, 333–345. [Google Scholar] [CrossRef]
- Schoenfeld, A.J.; Yu, H.A. The Evolving Landscape of Resistance to Osimertinib. J. Thorac. Oncol. 2020, 15, 18–21. [Google Scholar] [CrossRef]
- Frisone, D.; Friedlaender, A.; Malapelle, U.; Banna, G.; Addeo, A. A BRAF new world. Crit. Rev. Oncol./Hematol. 2020, 152, 103008. [Google Scholar] [CrossRef]
- Marcoux, N.; Gettinger, S.N.; O’Kane, G.; Arbour, K.C.; Neal, J.W.; Husain, H.; Evans, T.L.; Brahmer, J.R.; Muzikanski, A.; Bonomi, P.D.; et al. EGFR-Mutant Adenocarcinomas That Transform to Small-Cell Lung Cancer and Other Neuroendocrine Carcinomas: Clinical Outcomes. J. Clin. Oncol. 2019, 37, 278–285. [Google Scholar] [CrossRef]
- Schoenfeld, A.J.; Chan, J.M.; Kubota, D.; Sato, H.; Rizvi, H.; Daneshbod, Y.; Chang, J.C.; Paik, P.K.; Offin, M.; Arcila, M.E.; et al. Tumor Analyses Reveal Squamous Transformation and Off-Target Alterations As Early Resistance Mechanisms to First-line Osimertinib in EGFR-Mutant Lung Cancer. Clin. Cancer Res. 2020, 26, 2654–2663. [Google Scholar] [CrossRef] [PubMed]
- Population Statistics|Alberta.ca. Available online: https://www.alberta.ca/population-statistics (accessed on 23 October 2023).


{kind=link}
{kind=link}
| Characteristic | Entire Cohort (n = 150) | Progressive Disease Noted during 1L Osimertinib Therapy (n = 86) | ||
|---|---|---|---|---|
| Osimertinib ≥ 90 Days Post-PD Group A (n = 41) | 2L Systemic Therapy at PD Group B (n = 15) | No additional Systemic Therapy at PD Group C (n = 30) | ||
| Sex | ||||
| Female Male | 93 (62) 57 (38) | 24 (58) 17 (42) | 9 (60) 6 (40) | 22 (73) 8 (27) |
| Smoking history | ||||
| Ever Never | 66 (44) 84 (56) | 22 (54) 19 (46) | 8 (53) 7 (47) | 18 (60) 12 (40) |
| Age (years) | ||||
| Median (IQR) | 68.3 (61.3–78.4) | 64.3 (54.9–77.6) | 69.2 (59.4–75.3) | 71.5 (62.4–80.4) |
| Asian ancestry | ||||
| No Yes | 104 (69) 46 (31) | 25 (61) 16 (49) | 12 (80) 3 (20) | 19 (63) 11 (37) |
| EGFR mutation | ||||
| Exon 19 deletion Exon 21L858R | 87 (58) 63 (42) | 23 (56) 18 (44) | 5 (33) 10 (67) | 17 (57) 13 (43) |
| ECOG at 1L osimertinib initiation | ||||
| ECOG < 2 ECOG ≥ 2 | 100 (67) 50 (33) | 34 (83) 7 (17) | 12 (80) 3 (20) | 10 (33) 20 (67) |
| TNM 8th Edition M-stage at 1L osimertinib initiation | ||||
| M0 M1a M1b M1c | 16 (11) 37 (24) 48 (32) 49 (33) | 5 (13) 10 (24) 16 (39) 10 (24) | 0 (0) 4 (26) 4 (26) 7 (48) | 2 (7) 6 (20) 10 (33) 12 (40) |
| ≥3 sites of metastatic disease at 1L osimertinib initiation | ||||
| No Yes | 112 (81) 29 (19) | 36 (88) 5 (12) | 8 (54) 7 (46) * | 24 (60) 6 (20) |
| Metastatic disease in liver, bone or CNS present upon 1L osimertinib initiation | ||||
| Liver Bone Central Nervous System | 28 (19) 72 (48) 35 (23) | 7 (17) 19 (46) 8 (20) | 2 (13) 10 (67) 5 (33) | 10 (67) * 15 (100) * 6 (40) |
| Concurrent mutations (known at time of osimertinib initiation) | ||||
| None BRAF KRAS PIK3CA ERBB2 | 141 (94) 1 (<1) 1 (<1) 7 (5) 0 (0) | 40 (98) 1 (2) 0 (0) 0 (0) 0 (0) | 15 0 (0) 0 (0) 0 (0) 0 (0) | 26 (87) 0 (0) 1 (3) 3 (10) 0 (0) |
| Duration of treatment (months) Median (IQR) | 15.6 (6.0–26.9) | 26.8 * (18.7–33.8) | 9.4 (6.9–16.0) | 8.0 (2.7–25.7) |
| Tolerability | ||||
| Adverse events—no intervention required | 71% | 83% | 67% | 57% |
| Toxicity | ||||
| Adverse events—intervention required (dose reduction, treatment break, hospitalization, treatment termination) | 35% | 29% | 40% | 17% |
| Real-world objective response rate (rwORR) | 49% | 54% | 60% | 56% |
| Real-world disease control rate (rwDCR) | 82% | 100% | 100% | 76% * |
| Primary resistance | 5% | 0% | 0% | 3% |
| Time to progression | ||||
| Median [95% confidence interval] | 17.4 [14.7–23.3] | 13.5 [10.0–17.2] | 8.8 [5.6–11.9] | 8.6 [5.8–16.2] |
| Nature of progression | ||||
| Unknown (rapid clinical decline) Thoracic progression only Distant progression only Thoracic + distant progression | - | 0 (0) 22 (54) 11 (27) 8 (19) | 0 (0) 6 (40) 3 (20) 6 (40) | 15 (50) 6 (20) 3 (10) 6 (20) |
| Metastatic disease in liver, bone or CNS present upon progression | ||||
| Liver Bone Central Nervous System | - | 7 (17) 25 (61) 10 (24) | 6 (40) 10 (67) 5 (33) | 4 (13) 17 (57) 5 (17) |
| ≥3 Unique sites of metastatic disease upon progression | ||||
| No Yes | - | 29 (71) 12 (29) | 7 (46) 8 (53) | 22 (73) 8 (27) |
| Development or progression of CNS disease | ||||
| No Yes | - | 38 (93) 3 (7) | 13 (7) 2 (13) | 29 (97) 1 (3) |
| Survival post-progression on with osimertinib | ||||
| Median [95% Confidence interval] | - | 14.9 [8.7–24.9] | 11.8 [4.9–17.0] | 1.9 * [0.9–3.7] |
| Survival following osimertinib initiation | ||||
| Median [95% Confidence interval] | 28.9 [25.9–NR] | 34.7 [25.2–45.9] | 22.8 [15.4–NR] | 9.5 * [7.1–18.5] |
| 3-year survival rate | 27% | 46% | 33% | 0% * |
| Characteristic | Osimertinib ≥ 90 Days Post-PD Group A (n = 41) n (%) |
|---|---|
| Sex | |
| Female Male | 24 (58) 17 (42) |
| Age (years) at 1L osimertinib continuation | |
| Median (IQR) | 65.1 (56.4–78.1) |
| Asian ancestry | |
| No Yes | 25 (61) 16 (39) |
| EGFR mutation | |
| Exon 19 deletion Exon 21L858R | 23 (56) 18 (44) |
| TNM 8th Edition M-stage at 1L osimertinib continuation | |
| M0 M1a M1b M1c | 4 (10) 11 (27) 11 (27) 15 (36) |
| ≥3 sites of metastatic disease | |
| No Yes | 29 (71) 12 (29) |
| Metastatic disease in liver, bone or CNS present upon 1L osimertinib continuation | |
| Liver Bone Central Nervous System | 7 (17) 25 (61) 10 (24) |
| CNS present (but controlled) at 1L osimertinib continuation | 7/10 (70%) |
| Osimertinib continued on reduced dose | |
| No Yes (50% reduction to 40mg/day) | 37 (82) 7 (17) |
| Adverse events post-progression (requiring intervention) | |
| Treatment break (Grade 2 Fatigue; 14 days) | 1 (2) |
| Duration of treatment post-progression (months) | |
| Median (IQR) | 6.9 (4.3–14.3) |
| Reason for osimertinib termination | |
| Toxicity Death New treatment identified Further progressive disease Osimertinib ongoing | 1 (2) 12 (29) 1 (2) 15 (37) 12 (29) |
| Second-Line (non-osimertinib) therapy received | 11 (38) |
| Clinical Measure | By Post-Osimertinib Systemic Therapy Line | ||
|---|---|---|---|
| 2L n (%) (n = 26) | 3L n (%) (n = 7) | 4L n (%) (n = 2) | |
| Cytotoxic chemotherapy | 17 (65) | 6 (86) | 0 (0) |
| Platinum-doublet NSCLC regimen Single-agent regimen | (n = 17) (n = 0) | (n = 0) (n = 6) | |
| Immune checkpoint inhibitor | 0 (0) | 0 (0) | 1 (50) |
| Targeted therapy | 7 (27) | 1 (14) | 1 (50) |
| Second generation EGFR TKI Osimertinib rechallenge after treatment break SAVANNAH (osimertinib + savolitinib) trial Tepotinib | (n = 2) (n = 1) (n = 4) (n = 0) | (n = 0) (n = 1) (n = 0) (n = 0) | (n = 0) (n = 0) (n = 0) (n = 1) |
| Cytotoxic chemotherapy and targeted therapy | 2 (8) | 0 (0) | 0 (0) |
| Platinum-doublet + osimertinib MARIPOSA-2 trial (Arm C: platinum doublet + amivantamab + lazertinib) | (n = 1) (n = 1) | ||
| ECOG at initiation | |||
| ECOG < 2 ECOG ≥ 2 | 19 (73) 7 (27) | 4 (57) 3 (43) | 1 (50) 1 (50) |
| M-stage at initiation | |||
| M0 M1a M1b M1c | 1 (4) 4 (15) 7 (27) 14 (54) | 0 (0) 1 (15) 1 (15) 5 (70) | 0 (0) 0 (0) 0 (0) 2 (100) |
| Duration of treatment (months) Median (IQR) | 3.7 (1.4–11.4) | 1.8 (0–4.2) | 3.8 (2.5–5.1) |
| Real-world progression-free survival (months) Median [95% confidence interval] | 7.0 [5.2–9.0] | 5.0 [0.7–NR] | NR |
| Nature of initial progression | (n = 18) | (n = 6) | (n = 2) |
| Thoracic progression only Distant progression only Both thoracic and distant progression | 7 (39) 3 (17) 8 (44) | 2 (33) 2 (33) 2 (33) | 0 (0) 1 (50) 1 (50) |
| Progressive disease in the brain upon initial progression | (n = 18) | (n = 6) | (n = 2) |
| No Yes | 9 (50) 9 (50) | 6 (100) 0 (0) | 1 (50) 1 (50) |
| Reason for treatment termination | |||
| Treatment ongoing Completed as planned Progressive disease ECOG decline/death Adverse events | 6 (23) 1 (3) 12 (44) 4 (15) 4 (15) | 1 (14) 1 (14) 4 (58) 1 (14) 0 (0) | 1 (50) 0 (0) 0 (0) 1 (50) 0 (0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gibson, A.J.W.; Dean, M.L.; Litt, I.; Box, A.; Cheung, W.Y.; Navani, V. Real-World Analysis of Post-Progression Treatment Patterns and Outcomes for EGFR Mutation-Positive Patients Treated with First-Line Osimertinib. Curr. Oncol. 2024, 31, 2427-2440. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol31050182
Gibson AJW, Dean ML, Litt I, Box A, Cheung WY, Navani V. Real-World Analysis of Post-Progression Treatment Patterns and Outcomes for EGFR Mutation-Positive Patients Treated with First-Line Osimertinib. Current Oncology. 2024; 31(5):2427-2440. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol31050182
Chicago/Turabian StyleGibson, Amanda Jane Williams, Michelle Liane Dean, Ishjot Litt, Adrian Box, Winson Y. Cheung, and Vishal Navani. 2024. "Real-World Analysis of Post-Progression Treatment Patterns and Outcomes for EGFR Mutation-Positive Patients Treated with First-Line Osimertinib" Current Oncology 31, no. 5: 2427-2440. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol31050182