
Assessing Uveitis Risk following Pediatric Down Syndrome Diagnosis: A TriNetX Database Study
 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants, Main Measures and Outcomes
2.2. Statistical Analysis
3. Results
3.1. Baseline Characteristics
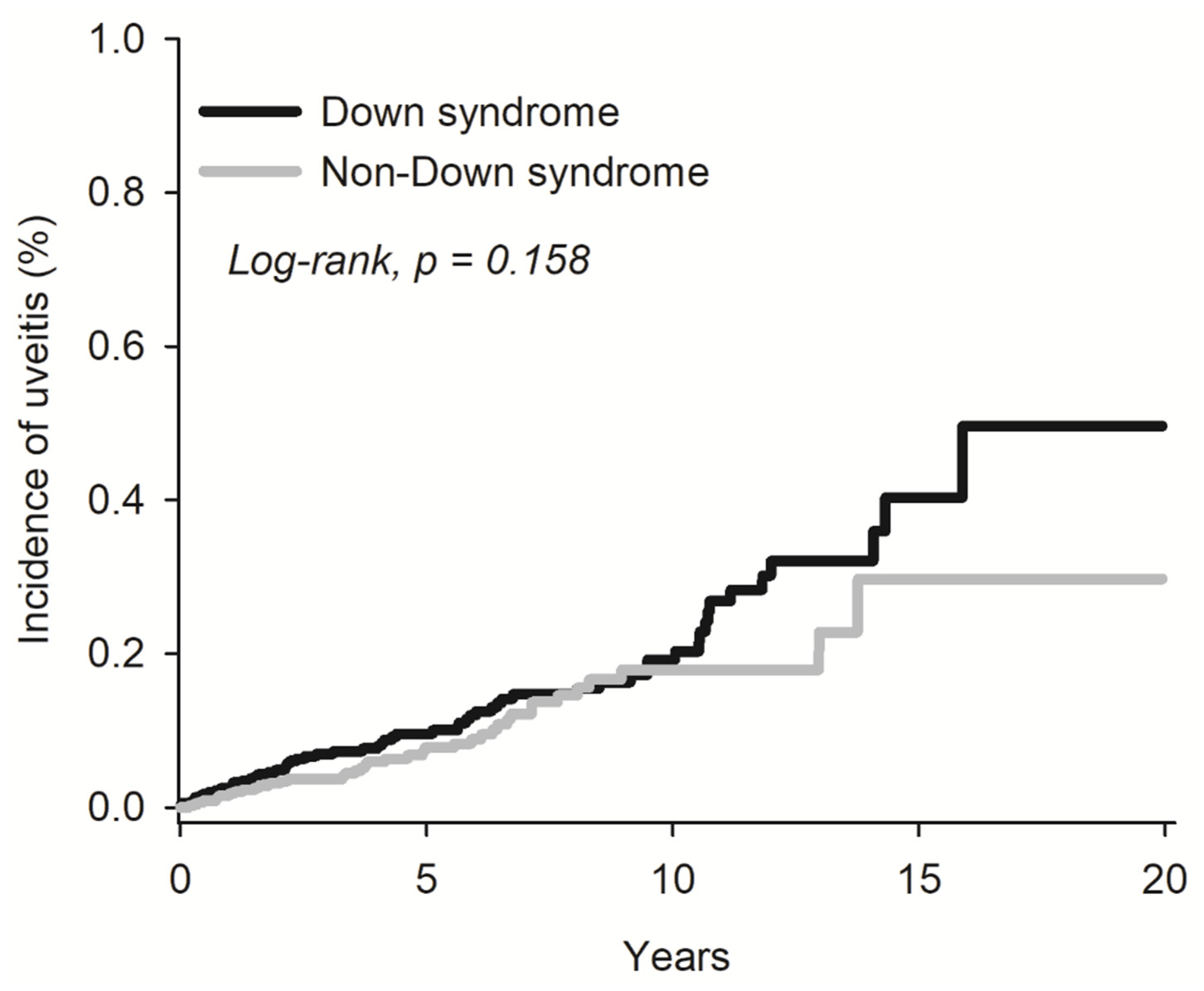
3.2. Risk of Uveitis among Down’s Syndrome Individuals
3.3. Stratification of Uveitis Risk Based on Age and Gender among Down’s Syndrome Individuals
4. Discussion
4.1. Novel Findings
4.2. Clinical Implications
4.3. Comparison to Other Studies
5. Strength and Limitations
6. Conclusions and Future Directions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoshi, N.; Hattori, R.; Hanatani, K.; Okuyama, K.; Yamada, H.; Kishida, T.; Yamada, T.; Sagawa, T.; Sumiyoshi, Y.; Fujimoto, S. Recent trends in the prevalence of Down syndrome in Japan, 1980–1997. Am. J. Med. Genet. 1999, 84, 340–345. [Google Scholar] [CrossRef]
- Lin, S.Y.; Hsieh, C.J.; Chen, Y.L.; Shaw, S.W.; Lin, M.W.; Chen, P.C.; Lee, C.N. The impact of Down syndrome screening on Taiwanese Down syndrome births: A nationwide retrospective study and a screening result from a single medical centre. PLoS ONE 2013, 8, e75428. [Google Scholar] [CrossRef]
- Sun, E.; Kraus, C.L. The Ophthalmic Manifestations of Down Syndrome. Children 2023, 10, 341. [Google Scholar] [CrossRef] [PubMed]
- Foley, C.M.; Deely, D.A.; MacDermott, E.J.; Killeen, O.G. Arthropathy of Down syndrome: An under-diagnosed inflammatory joint disease that warrants a name change. RMD Open 2019, 5, e000890. [Google Scholar] [CrossRef]
- Flores-Aguilar, L.; Iulita, M.F.; Kovecses, O.; Torres, M.D.; Levi, S.M.; Zhang, Y.; Askenazi, M.; Wisniewski, T.; Busciglio, J.; Cuello, A.C. Evolution of neuroinflammation across the lifespan of individuals with Down syndrome. Brain 2020, 143, 3653–3671. [Google Scholar] [CrossRef]
- Sen, E.S.; Dick, A.D.; Ramanan, A.V. Uveitis associated with juvenile idiopathic arthritis. Nat. Rev. Rheumatol. 2015, 11, 338–348. [Google Scholar] [CrossRef]
- Zaki, A.M.; Pasadhika, S.; Huang, J.C.; Thomas, A.S.; Burkholder, B.M.; Lim, L.L.; Llop, S.M.; Suhler, E.B.; Adamus, G.; Rosenbaum, J.T. Characterization of autoimmune eye disease in association with Down’s syndrome. Eye 2024, 38, 386–392. [Google Scholar] [CrossRef]
- Liza-Sharmini, A.T.; Azlan, Z.N.; Zilfalil, B.A. Ocular findings in Malaysian children with Down syndrome. Singap. Med. J. 2006, 47, 14–19. [Google Scholar]
- Shivpuri, A.; Turtsevich, I.; Solebo, A.L.; Compeyrot-Lacassagne, S. Pediatric uveitis: Role of the pediatrician. Front. Pediatr. 2022, 10, 874711. [Google Scholar] [CrossRef]
- Mathan, J.J.; Gokul, A.; Niederer, R.L.; McGhee, C.N.J. Down syndrome and autoimmune eye disease. Eye 2024, 38, 1024–1025. [Google Scholar] [CrossRef]
- Hsia, N.Y.; Hsu, A.Y.; Wang, Y.H.; Li, J.X.; Chen, H.S.; Wei, J.C.; Lin, C.; Tsai, Y. The risk assessment of uveitis after COVID-19 diagnosis: A multicenter population-based study. J. Med. Virol. 2023, 95, e29188. [Google Scholar] [CrossRef] [PubMed]
- Publication Guidelines: TriNetX. 2024. [updated 1 January 2024]. Available online: https://trinetx.com/real-world-resources/publications/trinetx-publication-guidelines/ (accessed on 23 April 2024).
- McKay, K.M.; Apostolopoulos, N.; Dahrouj, M.; Nguyen, H.V.; Reddy, A.; Blazes, M.; Lacy, M.; Pepple, K.L.; Lee, A.Y.; Lee, C.S. Assessing the Uniformity of Uveitis Clinical Concepts and Associated ICD-10 Codes Across Health Care Systems Sharing the Same Electronic Health Records System. JAMA Ophthalmol. 2021, 139, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Bull, M.J.; Trotter, T.; Santoro, S.L.; Christensen, C.; Grout, R.W.; The Council on Genetics. Health Supervision for Children and Adolescents with Down Syndrome. Pediatrics 2022, 149, e2022057010. [Google Scholar] [CrossRef] [PubMed]
- Tugal-Tutkun, I. Pediatric uveitis. J. Ophthalmic. Vis. Res. 2011, 6, 259–269. [Google Scholar] [PubMed]
- Yeung, I.Y.; Popp, N.A.; Chan, C.C. The role of sex in uveitis and ocular inflammation. Int. Ophthalmol. Clin. 2015, 55, 111–131. [Google Scholar] [CrossRef] [PubMed]
- Siiskonen, M.; Hirn, I.; Pesälä, R.; Ohtonen, P.; Hautala, N. Encouraging visual outcomes in children with idiopathic and JIA associated uveitis: A population-based study. Pediatr. Rheumatol. 2023, 21, 56. [Google Scholar] [CrossRef]
- Huggard, D.; Kelly, L.; Ryan, E.; McGrane, F.; Lagan, N.; Roche, E.; Balfe, J.; Leahy, T.R.; Franklin, O.; Doherty, D.G.; et al. Increased systemic inflammation in children with Down syndrome. Cytokine 2020, 127, 154938. [Google Scholar] [CrossRef]
- Siak, J.; Jansen, A.; Waduthantri, S.; Teoh, C.S.; Jap, A.; Chee, S.P. The Pattern of Uveitis among Chinese, Malays, and Indians in Singapore. Ocul. Immunol. Inflamm. 2017, 25, S81–S93. [Google Scholar] [CrossRef]
- Clarke, L.A.; Guex-Crosier, Y.; Hofer, M. Epidemiology of uveitis in children over a 10-year period. Clin. Exp. Rheumatol. 2013, 31, 633–637. [Google Scholar] [CrossRef]
- Agarwal, A.; Rübsam, A.; Zur Bonsen, L.; Pichi, F.; Neri, P.; Pleyer, U. A Comprehensive Update on Retinal Vasculitis: Etiologies, Manifestations and Treatments. J. Clin. Med. 2022, 11, 2525. [Google Scholar] [CrossRef]
- Jabs, D.A.; Nussenblatt, R.B.; Rosenbaum, J.T. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am. J. Ophthalmol. 2005, 140, 509–516. [Google Scholar] [PubMed]
- Dickman, S.L.; Gaffney, A.; McGregor, A.; Himmelstein, D.U.; McCormick, D.; Bor, D.H.; Woolhandler, S. Trends in Health Care Use Among Black and White Persons in the US, 1963–2019. JAMA Netw. Open 2022, 5, e2217383. [Google Scholar] [CrossRef] [PubMed]
- Demir, U. The relation of neutrophil/lymphocyte ratio, platelet/lymphocyte ratio and mean platelet volume with idiopathic acute anterior uveitis. Eur. J. Inflamm. 2024, 22, 1721727X231216196. [Google Scholar] [CrossRef]
- Groen-Hakan, F.; Eurelings, L.; van Laar, J.; Rothova, A. Relevance of erythrocyte sedimentation rate and C-reactive protein in patients with active uveitis. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 175–180. [Google Scholar] [CrossRef]
- Diala, F.G.I.; McCarthy, K.; Chen, J.L.; Tsui, E. Multimodal imaging in pediatric uveitis. Ther. Adv. Ophthalmol. 2021, 13, 25158414211059244. [Google Scholar] [CrossRef]


{kind=link}
| Before PSM | After PSM | |||||
|---|---|---|---|---|---|---|
| Down Syndrome N = 53,997 | Non-Down Syndrome N = 5,445,550 | SMD | Down Syndrome N = 53,993 | Non-Down Syndrome N = 53,993 | SMD | |
| Age | 5.21 ± 5.76 | 6.39 ± 6.03 | 0.200 | 5.21 ± 5.76 | 5.21 ± 5.76 | <0.001 |
| Sex | ||||||
| Female | 25,285 (46.83) | 2,627,251 (48.25) | 0.028 | 25,283 (46.83) | 24,597 (45.56) | 0.025 |
| Male | 28,406 (52.61) | 2,698,624 (49.56) | 0.061 | 28,404 (52.61) | 28,401 (52.60) | <0.001 |
| Race | ||||||
| White | 31,459 (58.26) | 2,721,257 (49.97) | 0.167 | 31,456 (58.26) | 31,462 (58.27) | <0.001 |
| Black or African American | 6009 (11.13) | 1,042,017 (19.14) | 0.225 | 6009 (11.13) | 6006 (11.12) | <0.001 |
| Asian | 1651 (3.06) | 217,522 (3.99) | 0.051 | 1650 (3.06) | 1651 (3.06) | <0.001 |
| Comorbidities | ||||||
| Other hypothyroidism | 1210 (2.24) | 8017 (0.15) | 0.194 | 1206 (2.23) | 1208 (2.24) | <0.001 |
| Asthma | 795 (1.47) | 151,927 (2.79) | 0.091 | 795 (1.47) | 783 (1.45) | 0.002 |
| Congenital malformation of heart, unspecified | 440 (0.82) | 3927 (0.07) | 0.112 | 437 (0.81) | 430 (0.80) | 0.001 |
| Hypertensive diseases | 316 (0.59) | 12,014 (0.22) | 0.058 | 316 (0.59) | 316 (0.59) | <0.001 |
| Atopic dermatitis | 149 (0.28) | 45,580 (0.84) | 0.075 | 149 (0.28) | 145 (0.27) | 0.001 |
| Celiac disease | 70 (0.13) | 1792 (0.03) | 0.034 | 69 (0.13) | 67 (0.12) | 0.001 |
| Crohn’s disease [regional enteritis] | 33 (0.06) | 1999 (0.04) | 0.011 | 33 (0.06) | 35 (0.07) | 0.001 |
| Ulcerative colitis | 18 (0.03) | 1105 (0.02) | 0.008 | 18 (0.03) | 18 (0.03) | <0.001 |
| Down Syndrome | Non-Down Syndrome | ||||
|---|---|---|---|---|---|
| N | No. of Event | N | No. of Event | HR (95% CI) | |
| Uveitis | 53,993 | 61 | 53,993 | 40 | 1.33 (0.89–1.99) |
| H20, Iridocyclitis | 53,993 | 50 | 53,993 | 34 | 1.28 (0.83–1.99) |
| H30, Chorio-retinal inflammation | 53,993 | 10 | 53,993 | 10 | 1.42 (0.51–4.01) |
| H35.06, Retinal vasculitis | 53,993 | 10 | 53,993 | 0 | N/A |
| H44.11, Panuveitis | 53,993 | 10 | 53,993 | 0 | N/A |
| H44.13, Sympathetic uveitis | 53,993 | 10 | 53,993 | 10 | 3.28 (0.36–29.54) |
| Down Syndrome | Non-Down Syndrome | ||||
|---|---|---|---|---|---|
| N | No. of Event | N | No. of Event | HR (95% CI) | |
| Age | |||||
| 0–1 | 23,363 | 21 | 23,363 | 13 | 1.36 (0.68–2.72) |
| 0–5 | 32,824 | 30 | 32,824 | 19 | 1.34 (0.75–2.39) |
| 6–18 | 21,161 | 31 | 21,161 | 24 | 1.15 (0.67–1.96) |
| Sex | |||||
| Female | 25,278 | 35 | 25,278 | 21 | 1.49 (0.87–2.56) |
| Male | 28,399 | 26 | 28,399 | 27 | 0.82 (0.48–1.41) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, A.Y.; Wang, Y.-H.; Lin, C.-J.; Li, Y.-L.; Hsia, N.-Y.; Lai, C.-T.; Kuo, H.-T.; Chen, H.-S.; Tsai, Y.-Y.; Wei, J.C.-C. Assessing Uveitis Risk following Pediatric Down Syndrome Diagnosis: A TriNetX Database Study. Medicina 2024, 60, 710. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina60050710
Hsu AY, Wang Y-H, Lin C-J, Li Y-L, Hsia N-Y, Lai C-T, Kuo H-T, Chen H-S, Tsai Y-Y, Wei JC-C. Assessing Uveitis Risk following Pediatric Down Syndrome Diagnosis: A TriNetX Database Study. Medicina. 2024; 60(5):710. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina60050710
Chicago/Turabian StyleHsu, Alan Y., Yu-Hsun Wang, Chun-Ju Lin, You-Ling Li, Ning-Yi Hsia, Chun-Ting Lai, Hou-Ting Kuo, Huan-Sheng Chen, Yi-Yu Tsai, and James Cheng-Chung Wei. 2024. "Assessing Uveitis Risk following Pediatric Down Syndrome Diagnosis: A TriNetX Database Study" Medicina 60, no. 5: 710. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina60050710