
Recent Trends in Adipose Tissue-Derived Injectable Therapies for Osteoarthritis: A Scoping Review of Animal Models
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Selection
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Search
2.5. Methodology for Data Collection
2.6. Data Elements
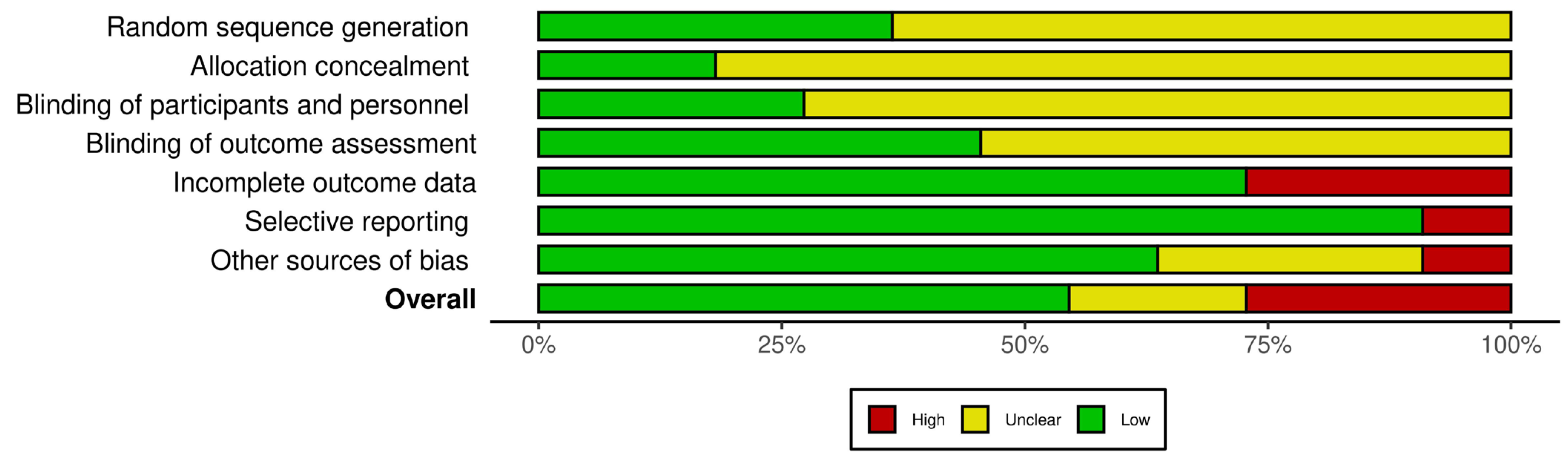
2.7. Evaluation of Biases
3. Results
3.1. Selection of Studies
3.2. Characteristics of Selected Studies
3.3. Animal Models
3.4. Type of Joint
3.5. Induction Methods
3.6. Analysis of Adipose Tissue-Derived Injectable Therapies
3.6.1. Adipose Tissue-Derived Injectable Therapy Type
3.6.2. Therapy Administration Timing and Frequency Following OA Induction
3.7. Evaluation of Adipose Tissue-Derived Injectable Therapies
3.7.1. Time of Evaluation after Administration of Injectable Therapy
3.7.2. Macroscopic Evaluation
3.7.3. Histologic Evaluation
3.7.4. Immunohistochemical Evaluation
3.7.5. Biochemical Evaluation
3.8. Articular Effects of Adipose Tissue-Derived Injectable Therapies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Samvelyan, H.J.; Hughes, D.; Stevens, C.; Staines, K.A. Models of Osteoarthritis: Relevance and New Insights. Calcif. Tissue Int. 2021, 109, 243–256. [Google Scholar] [CrossRef] [PubMed]
- Leifer, V.P.; Katz, J.N.; Losina, E. The burden of OA-health services and economics. Osteoarthr. Cartil. 2022, 30, 10–16. [Google Scholar] [CrossRef]
- Wojdasiewicz, P.; Poniatowski, Ł.A.; Szukiewicz, D. The role of inflammatory and anti-inflammatory cytokines in the pathogenesis of osteoarthritis. Mediat. Inflamm. 2014, 2014, 561459. [Google Scholar] [CrossRef]
- Fujii, Y.; Liu, L.; Yagasaki, L.; Inotsume, M.; Chiba, T.; Asahara, H. Cartilage Homeostasis and Osteoarthritis. Int. J. Mol. Sci. 2022, 23, 6316. [Google Scholar] [CrossRef]
- Chow, Y.Y.; Chin, K.Y. The Role of Inflammation in the Pathogenesis of Osteoarthritis. Mediat. Inflamm. 2020, 2020, 8293921. [Google Scholar] [CrossRef] [PubMed]
- Heidari, B. Knee osteoarthritis prevalence, risk factors, pathogenesis and features: Part I. Casp. J. Intern. Med. 2011, 2, 205–212. [Google Scholar]
- Dou, H.; Wang, S.; Hu, J.; Song, J.; Zhang, C.; Wang, J.; Xiao, L. Osteoarthritis models: From animals to tissue engineering. J. Tissue Eng. 2023, 14, 1–23. [Google Scholar] [CrossRef]
- Zhu, C.; Wu, W.; Qu, X. Mesenchymal stem cells in osteoarthritis therapy: A review. Am. J. Transl. Res. 2021, 13, 448–461. [Google Scholar]
- Zhang, R.; Ma, J.; Han, J.; Zhang, W.; Ma, J. Mesenchymal stem cell related therapies for cartilage lesions and osteoarthritis. Am. J. Transl. Res. 2019, 11, 6275–6289. [Google Scholar]
- Lindroos, B.; Suuronen, R.; Miettinen, S. The Potential of Adipose Stem Cells in Regenerative Medicine. Stem Cell Rev. Rep. 2011, 7, 269–291. [Google Scholar] [CrossRef]
- Mirsaidi, A.; Kleinhans, K.N.; Rimann, M.; Tiaden, A.N.; Stauber, M.; Rudolph, K.L.; Richards, P.J. Telomere length, telomerase activity and osteogenic differentiation are maintained in adipose-derived stromal cells from senile osteoporotic SAMP6 mice. J. Tissue Eng. Regen. Med. 2012, 6, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Kwon, D.G.; Kim, M.K.; Jeon, Y.S.; Nam, Y.C.; Park, J.S.; Ryu, D.J. State of the Art: The Immunomodulatory Role of MSCs for Osteoarthritis. Int. J. Mol. Sci. 2022, 23, 1618. [Google Scholar] [CrossRef] [PubMed]
- Guo, B.; Sawkulycz, X.; Heidari, N.; Rogers, R.; Liu, D.; Slevin, M. Characterisation of novel angiogenic and potent anti-inflammatory effects of micro-fragmented adipose tissue. Int. J. Mol. Sci. 2021, 22, 3271. [Google Scholar] [CrossRef] [PubMed]
- Shanmugasundaram, S.; Vaish, A.; Chavada, V.; Murrell, W.D.; Vaishya, R. Assessment of safety and efficacy of intra-articular injection of stromal vascular fraction for the treatment of knee osteoarthritis—A systematic review. Int. Orthop. 2021, 45, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.A.; Forrest, J.L. Enhancing your practice through evidence-based decision making: PICO, learning how to ask good questions. J. Evidenced Based Dent. Pract. 2001, 1, 136–141. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; Brien, K.K.O.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Ma, Q.; Horsley, T.; et al. Research and Reporting Methods PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Haddaway, N.R.; Page, M.J.; Pritchard, C.C.; McGuinness, L.A. PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis. Campbell Syst. Rev. 2022, 18, e1230. [Google Scholar] [CrossRef]
- Hooijmans, C.R.; Rovers, M.M.; De Vries, R.B.; Leenaars, M.; Ritskes-Hoitinga, M.; Langendam, M.W. SYRCLE’s risk of bias tool for animal studies. BMC Med. Res. Methodol. 2014, 14, 43. [Google Scholar] [CrossRef]
- Muñoz-Criado, I.; Meseguer-Ripolles, J.; Mellado-López, M.; Alastrue-Agudo, A.; Griffeth, R.J.; Forteza-Vila, J.; Cugat, R.; García, M.; Moreno-Manzano, V. Human Suprapatellar Fat Pad-Derived Mesenchymal Stem Cells Induce Chondrogenesis and Cartilage Repair in a Model of Severe Osteoarthritis. Stem Cells Int. 2017, 2017, 4758930. [Google Scholar] [CrossRef]
- Yang, W.T.; Ke, C.Y.; Yeh, K.T.; Huang, S.G.; Lin, Z.Y.; Wu, W.T.; Lee, R.P. Stromal-vascular fraction and adipose-derived stem cell therapies improve cartilage regeneration in osteoarthritis-induced rats. Sci. Rep. 2022, 12, 2828. [Google Scholar] [CrossRef]
- Kamada, K.; Matsushita, T.; Yamashita, T.; Matsumoto, T.; Iwaguro, H.; Sobajima, S.; Kuroda, R. Attenuation of knee osteoarthritis progression in mice through polarization of m2 macrophages by intra-articular transplantation of non-cultured human adipose-derived regenerative cells. J. Clin. Med. 2021, 10, 4309. [Google Scholar] [CrossRef] [PubMed]
- Veronesi, F.; Berni, M.; Marchiori, G.; Cassiolas, G.; Muttini, A.; Barboni, B.; Martini, L.; Fini, M.; Lopomo, N.F.; Marcacci, M.; et al. Evaluation of cartilage biomechanics and knee joint microenvironment after different cell-based treatments in a sheep model of early osteoarthritis. Int. Orthop. 2021, 45, 427–435. [Google Scholar] [CrossRef]
- Lv, X.; He, J.; Zhang, X.; Luo, X.; He, N.; Sun, Z.; Xia, H.; Liu, V.; Zhang, L.; Lin, X.; et al. Comparative Efficacy of Autologous Stromal Vascular Fraction and Autologous Adipose-Derived Mesenchymal Stem Cells Combined With Hyaluronic Acid for the Treatment of Sheep Osteoarthritis. Cell Transplant. 2018, 27, 1111–1125. [Google Scholar] [CrossRef]
- Berni, M.; Veronesi, F.; Fini, M.; Giavaresi, G.; Marchiori, G. Relations between Structure/Composition and Mechanics in Osteoarthritic Regenerated Articular Tissue: A Machine Learning Approach. Int. J. Mol. Sci. 2023, 24, 13374. [Google Scholar] [CrossRef] [PubMed]
- Veronesi, F.; Fini, M.; Martini, L.; Berardinelli, P.; Russo, V.; Filardo, G.; Di Matteo, B.; Marcacci, M.; Kon, E. In Vivo Model of Osteoarthritis to Compare Allogenic Amniotic Epithelial Stem Cells and Autologous Adipose Derived Cells. Biology 2022, 11, 681. [Google Scholar] [CrossRef]
- Filardo, G.; Tschon, M.; Perdisa, F.; Brogini, S.; Cavallo, C.; Desando, G.; Giavaresi, G.; Grigolo, B.; Martini, L.; Nicoli Aldini, N.; et al. Micro-fragmentation is a valid alternative to cell expansion and enzymatic digestion of adipose tissue for the treatment of knee osteoarthritis: A comparative preclinical study. Knee Surg. Sport. Traumatol. Arthrosc. 2022, 30, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Desando, G.; Bartolotti, I.; Martini, L.; Giavaresi, G.; Aldini, N.N.; Fini, M.; Roffi, A.; Perdisa, F.; Filardo, G.; Kon, E.; et al. Regenerative features of adipose tissue for osteoarthritis treatment in a rabbit model: Enzymatic digestion versus mechanical disruption. Int. J. Mol. Sci. 2019, 20, 2636. [Google Scholar] [CrossRef]
- Kuroda, Y.; Matsumoto, T.; Hayashi, S.; Hashimoto, S.; Takayama, K.; Kirizuki, S.; Tsubosaka, M.; Kamenaga, T.; Takashima, Y.; Matsushita, T.; et al. Intra-articular autologous uncultured adipose-derived stromal cell transplantation inhibited the progression of cartilage degeneration. J. Orthop. Res. 2019, 37, 1376–1386. [Google Scholar] [CrossRef]
- Ohashi, H.; Nishida, K.; Yoshida, A.; Nasu, Y.; Nakahara, R.; Matsumoto, Y.; Takeshita, A.; Kaneda, D.; Saeki, M.; Ozaki, T. Adipose-derived extract suppresses il-1β-induced inflammatory signaling pathways in human chondrocytes and ameliorates the cartilage destruction of experimental osteoarthritis in rats. Int. J. Mol. Sci. 2021, 22, 9781. [Google Scholar] [CrossRef]
- Little, C.B.; Smith, M.M.; Cake, M.A.; Read, R.A.; Murphy, M.J.; Barry, F.P. The OARSI histopathology initiative e recommendations for histological assessments of osteoarthritis in sheep and goats. Osteoarthr. Cartil. 2010, 18, S80–S92. [Google Scholar] [CrossRef]
- Laverty, S.; Girard, C.A.; Williams, J.M.; Hunziker, E.B.; Pritzker, K.P.H. The OARSI histopathology initiative—Recommendations for histological assessments of osteoarthritis in the rabbit. Osteoarthr. Cartil. 2010, 18, S53–S65. [Google Scholar] [CrossRef] [PubMed]
- Pritzker, K.P.H.; Gay, S.; Jimenez, S.A.; Ostergaard, K.; Pelletier, J.P.; Revell, K.; Salter, D.; van den Berg, W.B. Osteoarthritis cartilage histopathology: Grading and staging. Osteoarthr. Cartil. 2006, 14, 13–29. [Google Scholar] [CrossRef] [PubMed]
- Najm, A.; le Goff, B.; Venet, G.; Garraud, T.; Amiaud, J.; Biha, N.; Charrier, C.; Touchais, S.; Crenn, V.; Blanchard, F.; et al. IMSYC immunologic synovitis score: A new score for synovial membrane characterization in inflammatory and non-inflammatory arthritis. Jt. Bone Spine 2019, 86, 77–81. [Google Scholar] [CrossRef]
- Pauli, C.; Grogan, S.P.; Patil, S.; Otsuki, S.; Hasegawa, A.; Koziol, J.; Lotz, M.K.; D’Lima, D.D. MAcroscopic And Histopathologic Analysis Of Human Knee Menisci In Aging And Osteoarthritis. Osteoarthr. Cartil. 2011, 19, 1132–1141. [Google Scholar] [CrossRef] [PubMed]
- Xiang, X.N.; Zhu, S.Y.; He, H.C.; Yu, X.; Xu, Y.; He, C.Q. Mesenchymal stromal cell-based therapy for cartilage regeneration in knee osteoarthritis. Stem Cell Res. Ther. 2022, 13, 14. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Li, Z.; Alexander, P.G.; Ocasio-nieves, B.D. Pathogenesis of Osteoarthritis: Risk Factors, Regulatory Pathways in Chondrocytes, and Experimental Models. Biology 2020, 9, 194. [Google Scholar] [CrossRef] [PubMed]
- Coaccioli, S.; Sarzi-puttini, P.; Zis, P.; Rinonapoli, G.; Varrassi, G. Osteoarthritis: New Insight on Its Pathophysiology. J. Clin. Med. 2022, 11, 6013. [Google Scholar] [CrossRef] [PubMed]
- Cope, P.J.; Ourradi, K.; Li, Y.; Sharif, M. Models of osteoarthritis: The good, the bad and the promising. Osteoarthr. Cartil. 2019, 27, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Zaki, S.; Blaker, C.L.; Little, C.B. OA foundations e experimental models of osteoarthritis. Osteoarthr. Cartil. 2022, 30, 357–380. [Google Scholar] [CrossRef]
- Kuyinu, E.L.; Narayanan, G.; Nair, L.S.; Laurencin, C.T. Animal models of osteoarthritis: Classification, update, and measurement of outcomes. J. Orthop. Surg. Res. 2016, 11, 19. [Google Scholar] [CrossRef]
- Yao, Q.; Wu, X.; Tao, C.; Gong, W.; Chen, M.; Qu, M.; Zhong, Y.; He, T.; Chen, S.; Xiao, G. Osteoarthritis: Pathogenic signaling pathways and therapeutic targets. Signal Transduct. Target. Ther. 2023, 8, 56. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Papalia, R.; De Salvatore, S.; Picozzi, R.; Sarubbi, A.; Denaro, V. Induced Models of Osteoarthritis in Animal Models: A Systematic Review. Biology 2023, 12, 283. [Google Scholar] [CrossRef] [PubMed]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; Blanco, F.J.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, N.; Mak, C.; Bojanic, C.; To, K.; Khan, W. Meta-Analysis of Adipose Tissue Derived Cell-Based Therapy for the Treatment of Knee Osteoarthritis. Cells 2021, 10, 1365. [Google Scholar] [CrossRef] [PubMed]
- Primorac, D.; Molnar, V.; Matiši, V.; Hudetz, D.; Jelč, Ž.; Rod, E.; Cukelj, F.; Vidovi, D. Comprehensive Review of Knee Osteoarthritis Pharmacological Treatment and the Latest Professional Societies’ Guidelines. Pharmaceuticals 2021, 14, 205. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.; Yu, X.; Yang, Q.; Liu, X.; Fang, J.; Dai, X. Autologous Micro-Fragmented Adipose Tissue as Stem Cell-Based Natural Scaffold for Cartilage Defect Repair. Cell Transplant. 2019, 28, 1709–1720. [Google Scholar] [CrossRef]
- Muthu, S.; Patil, S.C.; Jeyaraman, N.; Jeyaraman, M.; Gangadaran, P.; Rajendran, R.L.; Oh, E.J.; Khanna, M.; Chung, H.Y.; Ahn, B.C. Comparative effectiveness of adipose-derived mesenchymal stromal cells in the management of knee osteoarthritis: A meta-analysis. World J. Orthop. 2023, 14, 23–41. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Lan, Z.; Yan, J.; Tang, Z.; Zhou, L.; Jin, D.; Jin, Q. Effect of intra-knee injection of autologous adipose stem cells or mesenchymal vascular components on short-term outcomes in patients with knee osteoarthritis: An updated meta-analysis of randomized controlled trials. Arthritis Res. Ther. 2023, 25, 147. [Google Scholar] [CrossRef] [PubMed]
- Aletto, C.; Oliva, F.; Maffulli, N. Journal of Clinical Orthopaedics and Trauma Knee intra-articular administration of stromal vascular fraction obtained from adipose tissue: A systematic review. J. Clin. Orthop. Trauma 2022, 25, 101773. [Google Scholar] [CrossRef]
- Lana, J.F.S.D.; Lana, A.V.S.D.; da Fonseca, L.F.; Coelho, M.A.; Marques, G.G.; Mosaner, T.; Ribeiro, L.L.; Azzini, G.O.M.; Santos, G.S.; Fonseca, E.; et al. Stromal Vascular Fraction for Knee Osteoarthritis—An Update. J. Stem Cells Regen. Med. 2022, 18, P11–P20. [Google Scholar] [CrossRef]
- Schipper, J.A.M.; van Laarhoven, C.J.H.C.M.; Schepers, R.H.; Tuin, A.J.; Harmsen, M.C.; Spijkervet, F.K.L.; Jansma, J.; van Dongen, J.A. Mechanical Fractionation of Adipose Tissue—A Scoping Review of Procedures to Obtain Stromal Vascular Fraction. Bioengineering 2023, 10, 1175. [Google Scholar] [CrossRef] [PubMed]
- Ude, C.C.; Shah, S.; Ogueri, K.S.; Nair, L.S.; Laurencin, C.T. Stromal Vascular Fraction for Osteoarthritis of the Knee Regenerative Engineering. Regen. Eng. Transl. Med. 2022, 8, 210–224. [Google Scholar] [CrossRef] [PubMed]
- Molnar, V.; Pavelić, E.; Vrdoljak, K.; Čemerin, M.; Klarić, E.; Matišić, V.; Bjelica, R.; Brlek, P.; Kovačić, I.; Tremolada, C.; et al. Mesenchymal Stem Cell Mechanisms of Action and Clinical Effects in Osteoarthritis: A Narrative Review. Genes 2022, 13, 949. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author, Year | Animal Model | Method of OA Induction | Groups and Types of Treatment | Therapy Administration Timing and Frequency after OA Induction | Period of Analysis |
|---|---|---|---|---|---|
| Muñoz-Criado et al., 2017 [19] | mouse | intra-articular injection of collagenase II with CaCl2 |
| once, at 5 days | 4 weeks |
| Kamada et al., 2021 [21] | mouse | medial meniscotibial ligament resection |
| once, immediately | 4 and 8 weeks |
| Ohashi et al., 2021 [29] | rat | anterior cruciate ligament, medial meniscus and medial collateral ligaments transection |
| weekly, for six weeks | 1 and 5 weeks |
| Yang et al., 2022 [20] | rat | intra-articular injection of sodium iodoacetate |
| once, at 2 weeks | 7 and 14 days |
| Kuroda et al., 2019 [28] | rabbit | anterior cruciate ligament transection |
| once, at 8 weeks | 8 and 12 weeks |
| Desando et al., 2019 [27] | rabbit | anterior cruciate ligament transection |
| once, at 8 weeks | 1 and 4 weeks |
| Filardo et al., 2021 [26] | rabbit | anterior cruciate ligament transection |
| once, at 8 weeks | 2 and 4 months |
| Lv et al., 2018 [23] | sheep | anterior cruciate ligament transection and medial meniscectomy |
| twice, at 12 and 15 weeks | 3 months |
| Veronesi et al., 2021 [22] | sheep | lateral meniscectomy |
| once, at 6 weeks | 3 months |
| Veronesi et al., 2022 [25] | sheep | lateral meniscectomy |
| once, at 6 weeks | 3 and 6 months |
| Berni et al., 2023 [24] | sheep | lateral meniscectomy |
| once, at 6 weeks | 3 and 6 months |
| Author, Year | Macroscopic Evaluation | Histologic Evaluation | Immunohistochemical Evaluation | Articular Biochemical Evaluation | Main Findings |
|---|---|---|---|---|---|
| Muñoz-Criado et al., 2017 [19] | NE | OARSI score | SOX-9 | NE | chemically induced OA in the mice led to aggressive joint degeneration; significant increase in SOX-9 expression within the developing cartilage in the hADSC-treated group; endogenous induction of cartilage repair through hADSC injection rather than assuming cell replacement |
| Kamada et al., 2021 [21] | NE | OARSI score | collagen type II, MMP-13, ADAMTS-5, IL-6, IL-1β | NE | lower histological OARSI in the treated group compared to the control group; increased number of type II collagen-positive cells, decreased number of chondrocytes expressing MMP-13, ADAMTS-5, IL-6, and IL-1 in the treated group compared to the control group |
| Ohashi et al., 2021 [29] | descriptive evaluation | modified Mankin, histologic score | NE | NE | significantly lower modified Mankin histologic score in the treated group compared to the control group at 2- and 6-weeks evaluation |
| Yang et al., 2022 [20] | descriptive evaluation | observational | collagen type II, collagen type I | NE | both SVF and ADSC therapies exhibited, upon histological evaluation, a discernible thick layer of cartilage with a regular surface; both therapeutic interventions significantly reduced plasma IL-1β levels on days 7 and 14 after treatment compared to the control group |
| Kuroda et al., 2019 [28] | OARSI score | OARSI score | collagen type II, MMP-13, SOX-9 | NE | macroscopically and histologically significantly lower OARSI scores and less cartilage damage in the treated group than the control group; immunohistochemically, the SVF group showed a significantly lower proportion of MMP-13-positive cells and a significantly higher percentage of type II collagen-positive areas than the control group; the proportion of SOX-9-positive cells was significantly higher in the SVF group than in the control group |
| Desando et al., 2019 [27] | NE | Laverty score, modified Pauli’s score | NE | NE | on day 7, SVF exhibited a significantly lower histologic scores compared to MFAT- and ASC-treated groups; on day 30, MFAT showed a significantly higher histologic score than SVF and ASCs; both SVF and MFAT groups displayed time-dependent effects on cartilage |
| Filardo et al., 2021 [26] | Hanashi score | Laverty score | collagen type II, MMP-1, TNF-α | NE | MFAT showed the best results both in terms of qualitative and semi-quantitative evaluations of articular cartilage, with a more uniform staining, a smoother surface and a significantly better Laverty score |
| Lv et al., 2018 [23] | ICRS score | cartilage thickness | collagen type X | IL-1β, IL-6 | high-dose ADSC combined with HA significantly suppressed the expression of IL-1β and IL-6 in synovial fluid; there were no statistically significant differences observed in the treatment combinations of low-dose ADSC with HA and SVF with HA |
| Veronesi et al., 2021 [22] | gross articular damage score | NE | NE | IL-1β, CTX2, TNF-α, IL-6, PGE2 | levels of pro-inflammatory cytokines (CTX2, PGE2, IL-1β) in synovial fluid, as assessed by ELISA, exhibited decreased values in the SVF-treated group; significantly lower levels of TNF-α and IL-6 were observed in both SVF- and AESC-treatment groups compared to the control and ADSC groups |
| Veronesi et al., 2022 [25] | gross articular damage score | OARSI score | collagen type II, collagen type I, MMP-13, IL-1β | IL-1β, CTX2, TNF-α, IL-6, PGE2 | SVF treatment showed superior effectiveness compared to AESC treatment, which, in turn, exhibited superiority over ADSC treatment; SVF outperformed AESC concerning macroscopic scores at three months, Krenn scores at six months, histologic OARSI scores at three and six months; at both the 3-week and 6-week evaluation stages, the percentage of cells expressing COL1A1 and MMP-13 was significantly lower, while those expressing COL2A1 were significantly higher in the SVF-treatment group compared to AESC, ADSC, and control |
| Berni et al., 2023 [24] | gross articular damage score | cartilage thickness fibrillation index | collagen type II | IL-1β, CTX2, TNF-α, IL-6, PGE2 | concerning articular cartilage viscoelastic parameters, notably the elastic modulus and cartilage relaxation time, SVF exhibited pronounced effectiveness at 3- and 6-months evaluation; comparative analysis with the other treatments revealed SVF’s superior success in attenuating the deterioration of articular cartilage viscoelastic parameters |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adam, A.O.; Benea, H.R.C.; Fotescu, H.M.; Alcalá Ruiz, M.; Cimpean, G.C.; Ciornei, V.; Cernacovschi, A.; Edves, A.R.; Crisan, M. Recent Trends in Adipose Tissue-Derived Injectable Therapies for Osteoarthritis: A Scoping Review of Animal Models. Medicina 2024, 60, 707. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina60050707
Adam AO, Benea HRC, Fotescu HM, Alcalá Ruiz M, Cimpean GC, Ciornei V, Cernacovschi A, Edves AR, Crisan M. Recent Trends in Adipose Tissue-Derived Injectable Therapies for Osteoarthritis: A Scoping Review of Animal Models. Medicina. 2024; 60(5):707. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina60050707
Chicago/Turabian StyleAdam, Alina Otilia, Horea Rares Ciprian Benea, Horia Mihnea Fotescu, Miriam Alcalá Ruiz, George Claudiu Cimpean, Vladimir Ciornei, Arsenii Cernacovschi, Andrei Rares Edves, and Maria Crisan. 2024. "Recent Trends in Adipose Tissue-Derived Injectable Therapies for Osteoarthritis: A Scoping Review of Animal Models" Medicina 60, no. 5: 707. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina60050707