
Association of Human Papilloma Virus, Cytomegalovirus, and Epstein–Barr Virus with Breast Cancer in Jordanian Women
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection
2.2. DNA Extraction
2.3. HPV Detection in Breast Cancer Samples
2.4. EBV and CMV Detection in Breast Cancer Samples
2.5. Statistical Analysis
3. Results
3.1. Clinicopathological Features within the Study Population
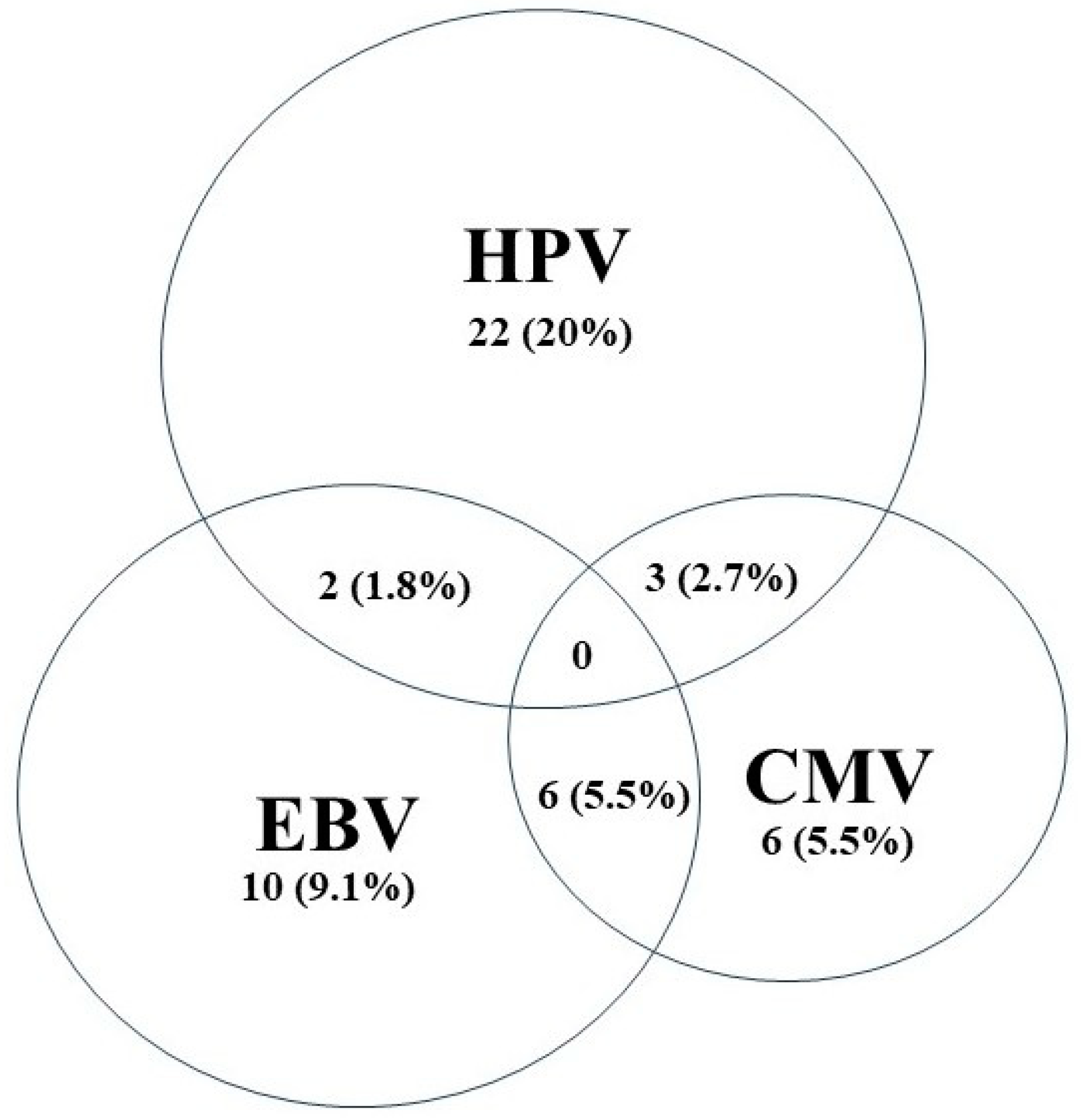
3.2. Detection of High-Risk HPV Subtypes, EBV, and CMV by RT-PCR
3.3. Clinicopathological Association with HR-HPV, CMV, and EBV Positivity
4. Discussion

{kind=link}
| Country | Year | CMV Positive in BC | CMV Positive in Controls | Reference |
|---|---|---|---|---|
| New Zealand | 2015 | 0% | 3% | Richardson et al. [47] |
| Egypt | 2018 | 18% | 5% | El Shazly et al. [43] |
| China | 2018 | 100% | --- | Cui et al. [48] |
| Iraq | 2018 | 6.3% | 5% | Kadhim et al. [56] |
| Iran | 2019 | 54% | 28% | Sepahvand et al. [45] |
| Iran | 2021 | 33% | 12% | Fard et al. [41] |
| Iran | 2021 | 16.3% | 2% | Nakhaie et al. [42] |
| Canada | 2022 | 18.4% | 10% | Yang et al. [46] |
| Egypt | 2024 | 13.8% | 0% | Elnegery et al. [44] |
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Breast Cancer—IARC. Available online: https://www.iarc.who.int/cancer-type/breast-cancer/ (accessed on 7 March 2024).
- Jawad Hashim, M.; Al-Shamsi, F.A.; Al-Marzooqi, N.A.; Al-Qasemi, S.S.; Mokdad, A.H.; Khan, G. Burden of Breast Cancer in the Arab World: Findings from Global Burden of Disease, 2016. J. Epidemiol. Glob. Health 2018, 8, 54–58. [Google Scholar] [CrossRef]
- Jordan Cancer Registry 2023—Google Search. Available online: https://www.google.com/search?sca_esv=ed313d50f24d50b8&q=Jordan+cancer+registry+2023&sa=X&ved=2ahUKEwi15e_J5uKEAxWYUaQEHQznBXwQ1QJ6BAhJEAE&biw=1536&bih=730&dpr=1.25 (accessed on 7 March 2024).
- Winters, S.; Martin, C.; Murphy, D.; Shokar, N.K. Breast Cancer Epidemiology, Prevention, and Screening. Prog. Mol. Biol. Transl. Sci. 2017, 151, 1–32. [Google Scholar] [CrossRef]
- Zamaraev, A.V.; Zhivotovsky, B.; Kopeina, G.S. Viral Infections: Negative Regulators of Apoptosis and Oncogenic Factors. Biochemistry 2020, 85, 1191–1201. [Google Scholar] [CrossRef]
- Williams, V.M.; Filippova, M.; Soto, U.; Duerksen-Hughes, P.J. HPV-DNA Integration and Carcinogenesis: Putative Roles for Inflammation and Oxidative Stress. Future Virol. 2011, 6, 45–57. [Google Scholar] [CrossRef]
- Benites-Zapata, V.A.; Ulloque-Badaracco, J.R.; Alarcón-Braga, E.A.; Fernández-Alonso, A.M.; López-Baena, M.T.; Pérez-López, F.R. Telomerase Activity and Telomere Length in Women with Breast Cancer or without Malignancy: A Systematic Review and Meta-Analysis. Maturitas 2024, 180, 107882. [Google Scholar] [CrossRef]
- White, M.K.; Pagano, J.S.; Khalili, K. Viruses and Human Cancers: A Long Road of Discovery of Molecular Paradigms. Clin. Microbiol. Rev. 2014, 27, 463–481. [Google Scholar] [CrossRef]
- Saleh, T.; Khasawneh, A.I.; Himsawi, N.; Abu-Raideh, J.; Ejeilat, V.; Elshazly, A.M.; Gewirtz, D.A. Senolytic Therapy: A Potential Approach for the Elimination of Oncogene-Induced Senescent HPV-Positive Cells. Int. J. Mol. Sci. 2022, 23, 15512. [Google Scholar] [CrossRef]
- AK, G.; AB, R. The Invisible Enemy—How Human Papillomaviruses Avoid Recognition and Clearance by the Host Immune System. Open Virol. J. 2012, 6, 249–256. [Google Scholar] [CrossRef]
- Middeldorp, J.M.; Pegtel, D.M. Multiple Roles of LMP1 in Epstein-Barr Virus Induced Immune Escape. Semin. Cancer Biol. 2008, 18, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Arias-Calvachi, C.; Blanco, R.; Calaf, G.M.; Aguayo, F. Epstein-Barr Virus Association with Breast Cancer: Evidence and Perspectives. Biology 2022, 11, 799. [Google Scholar] [CrossRef]
- Kudela, E.; Kudelova, E.; Kozubík, E.; Rokos, T.; Pribulova, T.; Holubekova, V.; Biringer, K. HPV-Associated Breast Cancer: Myth or Fact? Pathogens 2022, 11, 1510. [Google Scholar] [CrossRef]
- Geisler, J.; Touma, J.; Rahbar, A.; Söderberg-Nauclér, C.; Vetvik, K. A Review of the Potential Role of Human Cytomegalovirus (HCMV) Infections in Breast Cancer Carcinogenesis and Abnormal Immunity. Cancers 2019, 11, 1842. [Google Scholar] [CrossRef] [PubMed]
- Gao, A.; Kouznetsova, V.L.; Tsigelny, I.F. Bovine Leukemia Virus Relation to Human Breast Cancer: Meta-Analysis. Microb. Pathog. 2020, 149, 104417. [Google Scholar] [CrossRef]
- Lawson, J.S.; Glenn, W.K. Mouse Mammary Tumour Virus (MMTV) in Human Breast Cancer—The Value of Bradford Hill Criteria. Viruses 2022, 14, 721. [Google Scholar] [CrossRef]
- Khasawneh, A.I.; Himsawi, N.; Abu-Raideh, J.; Salameh, M.; Abdullah, N.; Khasawneh, R.; Saleh, T. Prevalence of Human Papillomavirus Associated with Head and Neck Squamous Cell Carcinoma in Jordanian Patients. Open Microbiol. J. 2020, 14, 57–64. [Google Scholar] [CrossRef]
- Khasawneh, A.I.; Asali, F.F.; Kilani, R.M.; Abu-Raideh, J.A.; Himsawi, N.M.; Salameh, M.A.; Al Ghabbiesh, G.H.; Saleh, T. Prevalence and Genotype Distribution of Human Papillomavirus among a Subpopulation of Jordanian Women. Int. J. Women’s Health Reprod. Sci. 2021, 9, 17–23. [Google Scholar] [CrossRef]
- Crombie, J.L.; LaCasce, A.S. Epstein Barr Virus Associated B-Cell Lymphomas and Iatrogenic Lymphoproliferative Disorders. Front. Oncol. 2019, 9, 436516. [Google Scholar] [CrossRef]
- Rovigatti, U.; Papaioannou, G.; Mammas, I.N.; Koutsaftiki, C.; Papatheodoropoulou, A.; Theodoridou, M.; Spandidos, D.A. Neuroblastoma in Childhood and Its Potential Viral Involvement: A Webinar by the Paediatric Virology Study Group. World Acad. Sci. J. 2022, 4, 16. [Google Scholar] [CrossRef]
- van Elsland, D.; Neefjes, J. Bacterial Infections and Cancer. EMBO Rep. 2018, 19, e46632. [Google Scholar] [CrossRef]
- Yahia, Z.A.; Adam, A.A.M.; Elgizouli, M.; Hussein, A.; Masri, M.A.; Kamal, M.; Mohamed, H.S.; Alzaki, K.; Elhassan, A.M.; Hamad, K.; et al. Epstein Barr Virus: A Prime Candidate of Breast Cancer Aetiology in Sudanese Patients. Infect. Agents Cancer 2014, 9, 9. [Google Scholar] [CrossRef]
- Aboulkassim, T.; Yasmeen, A.; Akil, N.; Batist, G.; Moustafa Al, A.E. Incidence of Epstein–Barr Virus in Syrian Women with Breast Cancer: A Tissue Microarray Study. Hum. Vaccin. Immunother. 2015, 11, 951. [Google Scholar] [CrossRef] [PubMed]
- Mofrad, M.G.; Kazeminezhad, B.; Faghihloo, E. Prevalence of Epstein-Barr Virus (EBV) in Iranian Breast Carcinoma Patients. Asian Pac. J. Cancer Prev. 2020, 21, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Afzal, S.; Fiaz, K.; Noor, A.; Sindhu, A.S.; Hanif, A.; Bibi, A.; Asad, M.; Nawaz, S.; Zafar, S.; Ayub, S.; et al. Interrelated Oncogenic Viruses and Breast Cancer. Front. Mol. Biosci. 2022, 9, 781111. [Google Scholar] [CrossRef] [PubMed]
- Kadivar, M.; Monabati, A.; Joulaee, A.; Hosseini, N. Epstein-Barr Virus and Breast Cancer: Lack of Evidence for an Association in Iranian Women. Pathol. Oncol. Res. 2011, 17, 489–492. [Google Scholar] [CrossRef] [PubMed]
- Aguayo, F.; Khan, N.; Koriyama, C.; González, C.; Ampuero, S.; Padilla, O.; Solís, L.; Eizuru, Y.; Corvalán, A.; Akiba, S. Human Papillomavirus and Epstein-Barr Virus Infections in Breast Cancer from Chile. Infect. Agents Cancer 2011, 6, 7. [Google Scholar] [CrossRef] [PubMed]
- Al Hamad, M.; Matalka, I.; Al Zoubi, M.S.; Armogida, I.; Khasawneh, R.; Al-Husaini, M.; Sughayer, M.; Jaradat, S.; Al-Nasser, A.D.; Mazzanti, C.M. Human Mammary Tumor Virus, Human Papilloma Virus, and Epstein-Barr Infection Are Associated with Sporadic Breast Cancer. Breast Cancer 2020, 14, 1178223420976388. [Google Scholar] [CrossRef] [PubMed]
- Khodabandehlou, N.; Mostafaei, S.; Etemadi, A.; Ghasemi, A.; Payandeh, M.; Hadifar, S.; Hossein Norooznezhad, A.; Kazemnejad, A.; Moghoofei, M. Human Papilloma Virus and Breast Cancer: The Role of Inflammation and Viral Expressed Proteins. BMC Cancer 2019, 19, 61. [Google Scholar] [CrossRef] [PubMed]
- Nagi, K.; Gupta, I.; Jurdi, N.; Jabeen, A.; Yasmeen, A.; Batist, G.; Vranic, S.; Al-Moustafa, A.E. High-Risk Human Papillomaviruses and Epstein–Barr Virus in Breast Cancer in Lebanese Women and Their Association with Tumor Grade: A Molecular and Tissue Microarray Study. Cancer Cell Int. 2021, 21, 308. [Google Scholar] [CrossRef] [PubMed]
- Gupta, I.; Jabeen, A.; Al-Sarraf, R.; Farghaly, H.; Vranic, S.; Sultan, A.A.; Al Moustafa, A.E.; Al-Thawadi, H. The Co-Presence of High-Risk Human Papillomaviruses and Epstein-Barr Virus Is Linked with Tumor Grade and Stage in Qatari Women with Breast Cancer. Hum. Vaccin. Immunother. 2021, 17, 982. [Google Scholar] [CrossRef] [PubMed]
- El-Sheikh, N.; Mousa, N.O.; Tawfeik, A.M.; Saleh, A.M.; Elshikh, I.; Deyab, M.; Ragheb, F.; Moneer, M.M.; Kawashti, A.; Osman, A.; et al. Assessment of Human Papillomavirus Infection and Risk Factors in Egyptian Women with Breast Cancer. Breast Cancer 2021, 15, 1178223421996279. [Google Scholar] [CrossRef]
- Sigaroodi, A.; Nadji, S.A.; Naghshvar, F.; Nategh, R.; Emami, H.; Velayati, A.A. Human Papillomavirus Is Associated with Breast Cancer in the North Part of Iran. Sci. World J. 2012, 2012, 837191. [Google Scholar] [CrossRef] [PubMed]
- Sughayer, M.A.; Abdelhadi, M.; Abdeen, G.; Otay, L.; Dayeh, T. Human Papillomavirus Genotypes in Invasive Cervical Cancer in Jordan. Int. J. Gynecol. Obstet. 2010, 108, 74–75. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.H.M.; Al-Alwan, N.A.S.; Al-Alwany, S.H.M. Detection and Genotyping of Human Papillomavirus in Breast Cancer Tissues from Iraqi Patients. East. Mediterr. Health J. 2014, 20, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Bishtawi, M.; Saleh, H.; Khadra, M. Prevalence of HPV types in jordanian women with abnormal pap smear igcs19-0625 153 alarming rise in cervical cytological abnormalities in women living in jordan. Int. J. Gynecol. Cancer 2019, 29, A70. [Google Scholar] [CrossRef]
- Al-Qudah, M.A.; Al-Shaikh, A.F.; Haddad, H.K.; Elhassan, M.A.; Elhassan, O.B.; Dababneh, M.N.; Zaitoun, A.W.; Al Ghamdi, N.S.; Al-Najjar, B.Y. Prevalence and Detection of Sexually Transmitted Cases of Laryngeal Carcinoma Papilloma Virus · Cyclin-Dependent Kinase Inhibitor P16 · Cyclin B · Cyclin E · PCR. Head Neck Pathol. 2020, 14, 909–914. [Google Scholar] [CrossRef]
- Freij, M.A.; Saleh, H.H.; Farsakh, H.A.A.; Khadra, M.M.; Ijmail, A.A.; Rahal, B.O.; Waldali, M.H.; Najeeb, N.S.; Tahtamouni, L.H. Type-Specific Prevalence of Human Papillomavirus among Women with Abnormal Cytology in Jordan. Eur. J. Gynaecol. Oncol. 2017, 38, 901–904. [Google Scholar] [CrossRef]
- Yasmeen, A.; Bismar, T.A.; Kandouz, M.; Foulkes, W.D.; Desprez, P.-Y.; Al Moustafa, A.-E. E6/E7 of HPV Type 16 Promotes Cell Invasion and Metastasis of Human Breast Cancer Cells. Cell Cycle 2007, 6, 2038–2042. [Google Scholar] [CrossRef] [PubMed]
- Akil, N.; Yasmeen, A.; Kassab, A.; Ghabreau, L.; Darnel, A.D.; Al Moustafa, A.-E. High-Risk Human Papillomavirus Infections in Breast Cancer in Syrian Women and Their Association with Id-1 Expression: A Tissue Microarray Study. Br. J. Cancer 2008, 99, 404–407. [Google Scholar] [CrossRef]
- Fard, Z.T.; Khayamzadeh, M.; Zarei, M. Molecular Detection of Human Cytomegalovirus in Breast Cancer of Iranian Women Using Real-Time PCR. Int. J. Cancer Manag. 2021, 14, 115720. [Google Scholar] [CrossRef]
- Nakhaie, M.; Charostad, J.; Ghaderi-Zefrehi, H.; Arabzadeh, S.A.M.; Pourhosseini, F.; Makvandi, M. Prevalence of Human Cytomegalovirus in Breast Cancer: A Systematic Review. Asian Pac. J. Cancer Biol. 2021, 6, 161–169. [Google Scholar] [CrossRef]
- El Shazly, D.F.; Bahnassey, A.A.; Omar, O.S.; Elsayed, E.T.; Al-Hindawi, A.; El-Desouky, E.; Youssef, H.; Zekri, A.R.N. Detection of Human Cytomegalovirus in Malignant and Benign Breast Tumors in Egyptian Women. Clin. Breast Cancer 2018, 18, e629–e642. [Google Scholar] [CrossRef] [PubMed]
- Elnegery, A.A.; Abou Elela, M.A.; Mohamed, S.T.; Ragab, O.F.A.; Yussif, S.M.I.; Abou El-Khier, N.T. Human Cytomegalovirus and COX2 Expression among Women with Breast Tumors. Egypt. J. Med. Microbiol. 2024, 33, 73–82. [Google Scholar] [CrossRef]
- Sepahvand, P.; Makvandi, M.; Samarbafzadeh, A.; Talaei-Zadeh, A.; Ranjbari, N.; Nisi, N.; Azaran, A.; Jalilian, S.; Pirmoradi, R.; Makvandi, K.; et al. Human Cytomegalovirus DNA among Women with Breast Cancer. Asian Pac. J. Cancer Prev. 2019, 20, 2275. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Tang, X.; Hasing, M.E.; Pang, X.; Ghosh, S.; McMullen, T.P.W.; Brindley, D.N.; Hemmings, D.G. Human Cytomegalovirus Seropositivity and Viral DNA in Breast Tumors Are Associated with Poor Patient Prognosis. Cancers 2022, 14, 1148. [Google Scholar] [CrossRef] [PubMed]
- Richardson, A.K.; Currie, M.J.; Robinson, B.A.; Morrin, H.; Phung, Y.; Pearson, J.F.; Anderson, T.P.; Potter, J.D.; Walker, L.C. Cytomegalovirus and Epstein-Barr Virus in Breast Cancer. PLoS ONE 2015, 10, e0118989. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.; Wang, Q.; Wang, H.B.; Wang, B.; Li, L. Protein and DNA Evidences of HCMV Infection in Primary Breast Cancer Tissues and Metastatic Sentinel Lymph Nodes. Cancer Biomark. 2018, 21, 769–780. [Google Scholar] [CrossRef] [PubMed]
- Richardson, A.K.; Walker, L.C.; Cox, B.; Rollag, H.; Robinson, B.A.; Morrin, H.; Pearson, J.F.; Potter, J.D.; Paterson, M.; Surcel, H.M.; et al. Breast Cancer and Cytomegalovirus. Clin. Transl. Oncol. 2020, 22, 585–602. [Google Scholar] [CrossRef] [PubMed]
- El Baba, R.; Herbein, G. Immune Landscape of CMV Infection in Cancer Patients: From “Canonical” Diseases Toward Virus-Elicited Oncomodulation. Front. Immunol. 2021, 12, 730765. [Google Scholar] [CrossRef] [PubMed]
- Balegamire, S.J.; McClymont, E.; Croteau, A.; Dodin, P.; Gantt, S.; Besharati, A.A.; Renaud, C.; Mâsse, B.; Boucoiran, I. Prevalence, Incidence, and Risk Factors Associated with Cytomegalovirus Infection in Healthcare and Childcare Worker: A Systematic Review and Meta-Analysis. Syst. Rev. 2022, 11, 131. [Google Scholar] [CrossRef]
- Lachmann, R.; Loenenbach, A.; Waterboer, T.; Brenner, N.; Pawlita, M.; Michel, A.; Thamm, M.; Poethko-Müller, C.; Wichmann, O.; Wiese-Posselt, M. Cytomegalovirus (CMV) Seroprevalence in the Adult Population of Germany. PLoS ONE 2018, 13, e0200267. [Google Scholar] [CrossRef]
- Kalkan, A.; Ozdarendeli, A.; Bulut, Y.; Yekeler, H.; Cobanoglu, B.; Doymaz, M.Z. Investigation of Epstein-Barr Virus DNA in Formalin-Fixed and Paraffin- Embedded Breast Cancer Tissues. Med. Princ. Pract. 2005, 14, 268–271. [Google Scholar] [CrossRef] [PubMed]
- Metwally, S.A.; Abo-Shadi, M.A.; Abdel Fattah, N.F.; Barakat, A.B.; Rabee, O.A.; Osman, A.M.; Helal, A.M.; Hashem, T.; Moneer, M.M.; Chehadeh, W.; et al. Presence of Hpv, Ebv and Hmtv Viruses among Egyptian Breast Cancer Women: Molecular Detection and Clinical Relevance. Infect. Drug Resist. 2021, 14, 2327–2339. [Google Scholar] [CrossRef] [PubMed]
- Mekrazi, S.; Kallel, I.; Jamai, D.; Yengui, M.; Khabir, A.; Gdoura, R. Epstein-Barr Virus in Breast Carcinoma and in Triple Negative Cases Impact on Clinical Outcomes. Pathol. Res. Pract. 2023, 245, 154484. [Google Scholar] [CrossRef] [PubMed]
- Shadood, H.K.A.L.; Atiya, S.A.-A.; Kardar, G.A.; Shadood, H.K.A.L.; Atiya, S.A.-A.; Kardar, G.A. Correlation of Breast Cancer with the Epstein Bar Virus and Human Cytomegalovirus Frequency and the Expression of Estrogen Receptor-Beta and IL-6 Receptor in Iraqi Women. Nat. Sci. 2018, 10, 182–192. [Google Scholar] [CrossRef]
- Farahmand, M.; Monavari, S.H.; Shoja, Z.; Ghaffari, H.; Tavakoli, M.; Tavakoli, A. Epstein–Barr Virus and Risk of Breast Cancer: A Systematic Review and Meta-Analysis. Future Oncol. 2019, 15, 2873–2885. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Luo, M.-L.; Desmedt, C.; Nabavi, S.; Yadegarynia, S.; Hong, A.; Konstantinopoulos, P.A.; Gabrielson, E.; Hines-Boykin, R.; Pihan, G.; et al. Epstein-Barr Virus Infection of Mammary Epithelial Cells Promotes Malignant Transformation. EBioMedicine 2016, 9, 148–160. [Google Scholar] [CrossRef] [PubMed]
- Tempera, I.; Lieberman, P.M. Oncogenic Viruses as Entropic Drivers of Cancer Evolution. Front. Virol. 2021, 1, 753366. [Google Scholar] [CrossRef] [PubMed]
- Kannampuzha, S.; Gopalakrishnan, A.V.; Padinharayil, H.; Alappat, R.R.; Anilkumar, K.V.; George, A.; Dey, A.; Vellingiri, B.; Madhyastha, H.; Ganesan, R.; et al. Onco-Pathogen Mediated Cancer Progression and Associated Signaling Pathways in Cancer Development. Pathogens 2023, 12, 770. [Google Scholar] [CrossRef] [PubMed]
- Al Moustafa, A.-E.; Al-Antary, N.; Aboulkassim, T.; Akil, N.; Batist, G.; Yasmeen, A. Co-Prevalence of Epstein-Barr Virus and High-Risk Human Papillomaviruses in Syrian Women with Breast Cancer. Hum. Vaccin. Immunother. 2016, 12, 1936–1939. [Google Scholar] [CrossRef]
- Al-Thawadi, H.; Gupta, I.; Jabeen, A.; Skenderi, F.; Aboulkassim, T.; Yasmeen, A.; Malki, M.I.; Batist, G.; Vranic, S.; Al Moustafa, A.E. Co-Presence of Human Papillomaviruses and Epstein-Barr Virus Is Linked with Advanced Tumor Stage: A Tissue Microarray Study in Head and Neck Cancer Patients. Cancer Cell Int. 2020, 20, 361. [Google Scholar] [CrossRef]
- Fernandes, Q.; Gupta, I.; Vranic, S.; Al Moustafa, A.E. Human Papillomaviruses and Epstein–Barr Virus Interactions in Colorectal Cancer: A Brief Review. Pathogens 2020, 9, 300. [Google Scholar] [CrossRef] [PubMed]

| HR-HPV | CMV | EBV | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| + | − | p Value | + | − | p Value | + | − | p Value | ||
| Age | ≤56 | 18 | 38 | 0.047 | 7 | 49 | 0.786 | 8 | 48 | 0.612 |
| >56 | 9 | 45 | 8 | 46 | 10 | 44 | ||||
| Luminal A | ER+/PR+, HER2− | 20 | 53 | 0.595 | 10 | 63 | 0.783 | 11 | 62 | 0.166 |
| Luminal B | ER+/PR+, HER2+ | 4 | 17 | 2 | 19 | 2 | 19 | |||
| HER+ | ER−/PR−, HER2+ | 2 | 4 | 1 | 5 | 1 | 5 | |||
| TNBC | ER−/PR−, HER2− | 1 | 9 | 2 | 8 | 4 | 6 | |||
| Stage | Stage I | 10 | 38 | 0.726 | 11 | 37 | 0.015 | 9 | 39 | 0.841 |
| Stage II | 6 | 12 | 0 | 18 | 2 | 16 | ||||
| Stage III | 4 | 11 | 3 | 12 | 3 | 12 | ||||
| Stage IV | 7 | 22 | 1 | 28 | 4 | 25 | ||||
| Grade | Grade 1 | 0 | 10 | 0.110 | 3 | 7 | 0.147 | 2 | 8 | 0.798 |
| Grade 2 | 18 | 42 | 9 | 51 | 9 | 51 | ||||
| Grade 3 | 9 | 31 | 3 | 37 | 7 | 33 | ||||
| LV | Present | 15 | 42 | 0.666 | 4 | 53 | 0.051 | 7 | 50 | 0.304 |
| Not identified | 12 | 41 | 11 | 42 | 11 | 42 | ||||
| LN | Positive | 18 | 56 | 0.454 | 7 | 67 | 0.131 | 12 | 62 | 1.000 |
| Negative | 9 | 22 | 7 | 24 | 5 | 26 | ||||
| Smoking history | Yes | 4 | 10 | 0.743 | 4 | 10 | 0.098 | 1 | 13 | 0.459 |
| No | 23 | 73 | 11 | 85 | 17 | 79 | ||||
| Family history | Positive | 22 | 64 | 0.238 | 3 | 11 | 0.511 | 7 | 13 | 0.057 |
| Negative | 3 | 17 | 17 | 75 | 11 | 75 | ||||
| CIS | Positive | 2 | 56 | 0.011 | 12 | 69 | 0.755 | 11 | 70 | 0.242 |
| Negative | 25 | 27 | 3 | 26 | 7 | 22 | ||||
| Tumor size | >3 cm | 16 | 39 | 0.376 | 7 | 78 | 1.000 | 11 | 44 | 0.440 |
| ≤3 cm | 11 | 44 | 8 | 47 | 7 | 48 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khasawneh, A.I.; Himsawi, N.; Sammour, A.; Al Shboul, S.; Alorjani, M.; Al-Momani, H.; Shahin, U.; Al-Momani, H.; Alotaibi, M.R.; Saleh, T. Association of Human Papilloma Virus, Cytomegalovirus, and Epstein–Barr Virus with Breast Cancer in Jordanian Women. Medicina 2024, 60, 699. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina60050699
Khasawneh AI, Himsawi N, Sammour A, Al Shboul S, Alorjani M, Al-Momani H, Shahin U, Al-Momani H, Alotaibi MR, Saleh T. Association of Human Papilloma Virus, Cytomegalovirus, and Epstein–Barr Virus with Breast Cancer in Jordanian Women. Medicina. 2024; 60(5):699. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina60050699
Chicago/Turabian StyleKhasawneh, Ashraf I., Nisreen Himsawi, Ashraf Sammour, Sofian Al Shboul, Mohammed Alorjani, Hadeel Al-Momani, Uruk Shahin, Hafez Al-Momani, Moureq R. Alotaibi, and Tareq Saleh. 2024. "Association of Human Papilloma Virus, Cytomegalovirus, and Epstein–Barr Virus with Breast Cancer in Jordanian Women" Medicina 60, no. 5: 699. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina60050699