
Prognostic Value of Histone Acetyl Transferase 1 (HAT-1) and Inflammatory Signatures in Pancreatic Cancer
 , , , , ,
, , , , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample Collection
2.2. Immunohistochemical Analysis
2.3. Histopathological Evaluation
2.4. Analytical Statistics
3. Results
3.1. Clinical and Sociodemographic Features of the Patients
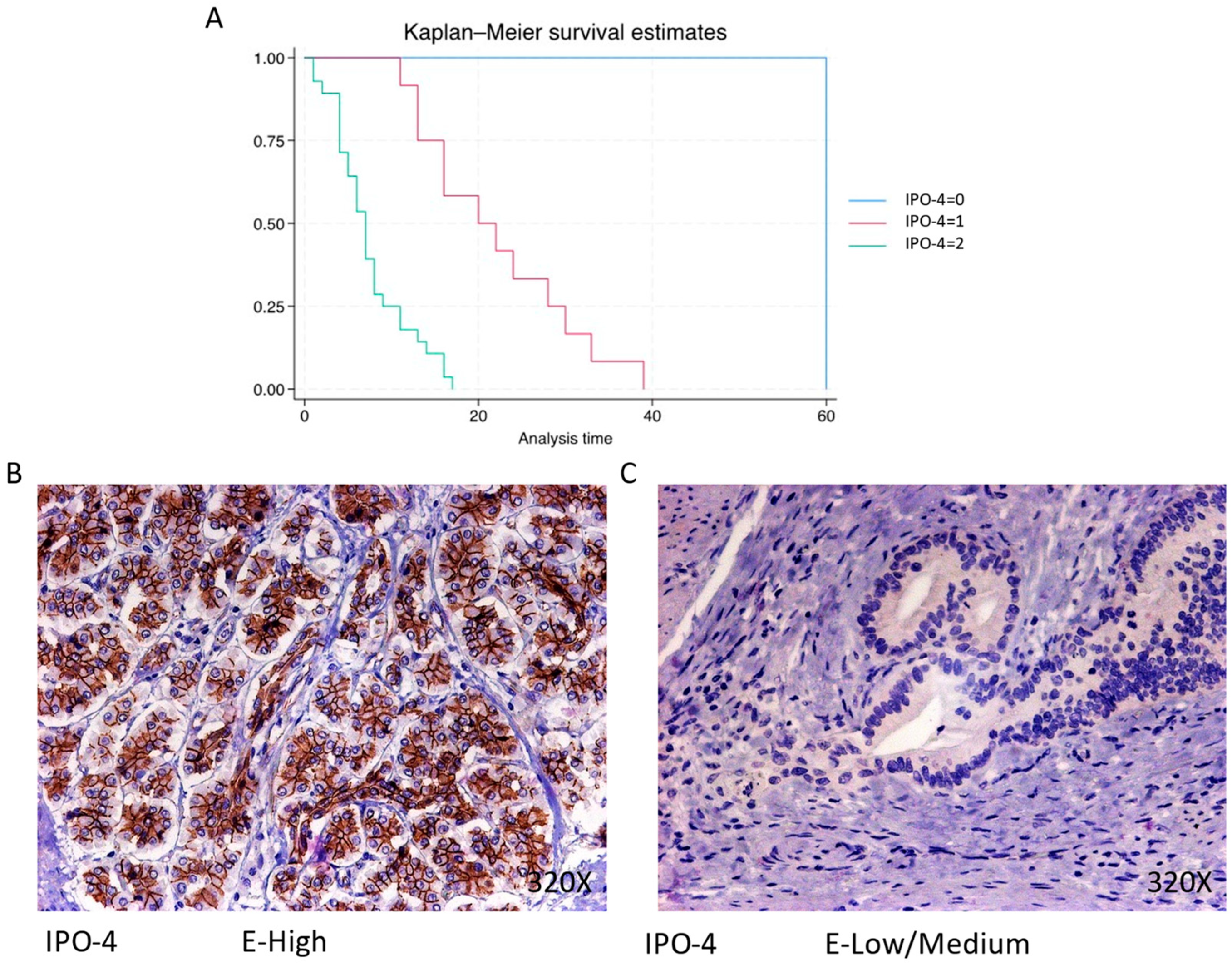
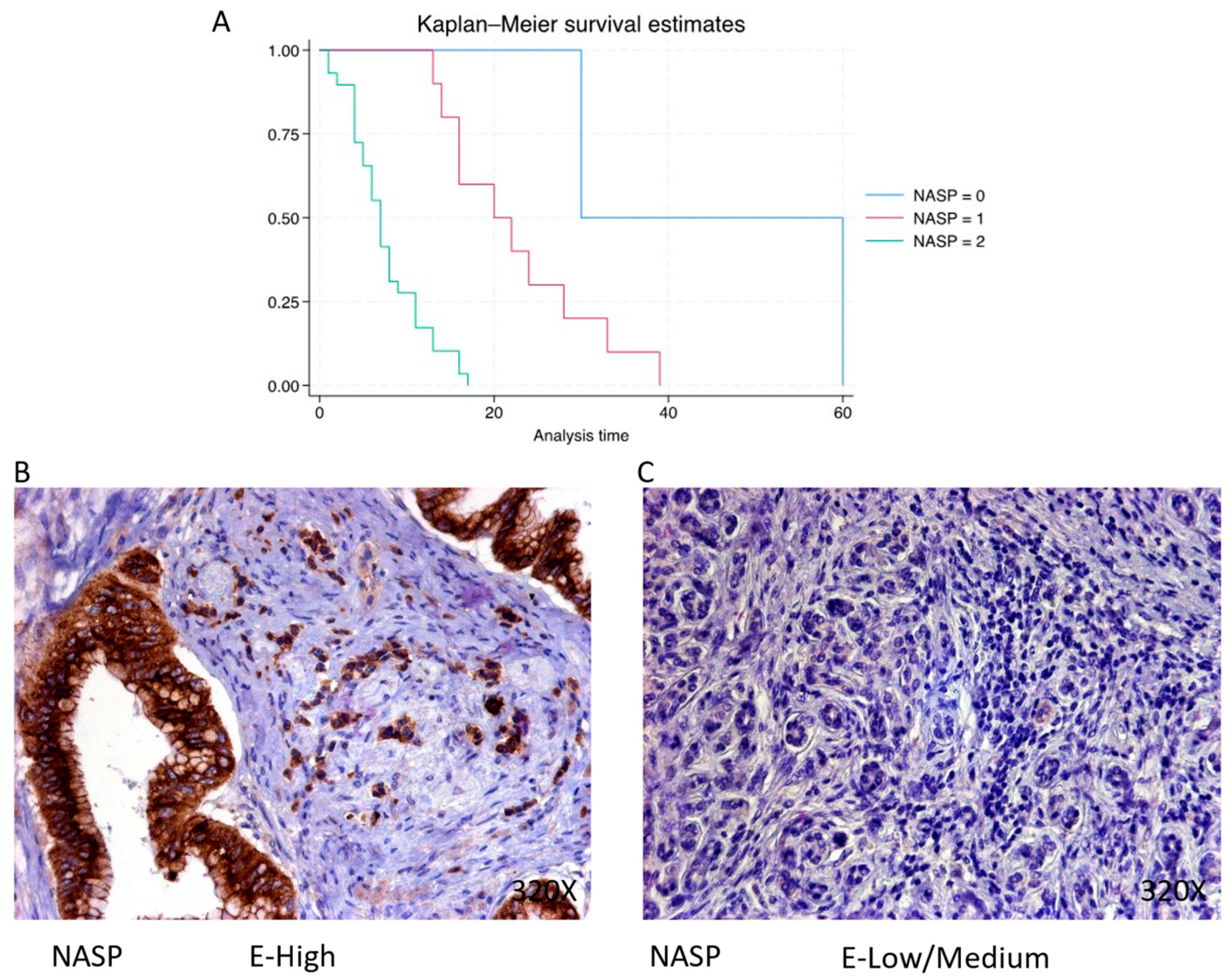
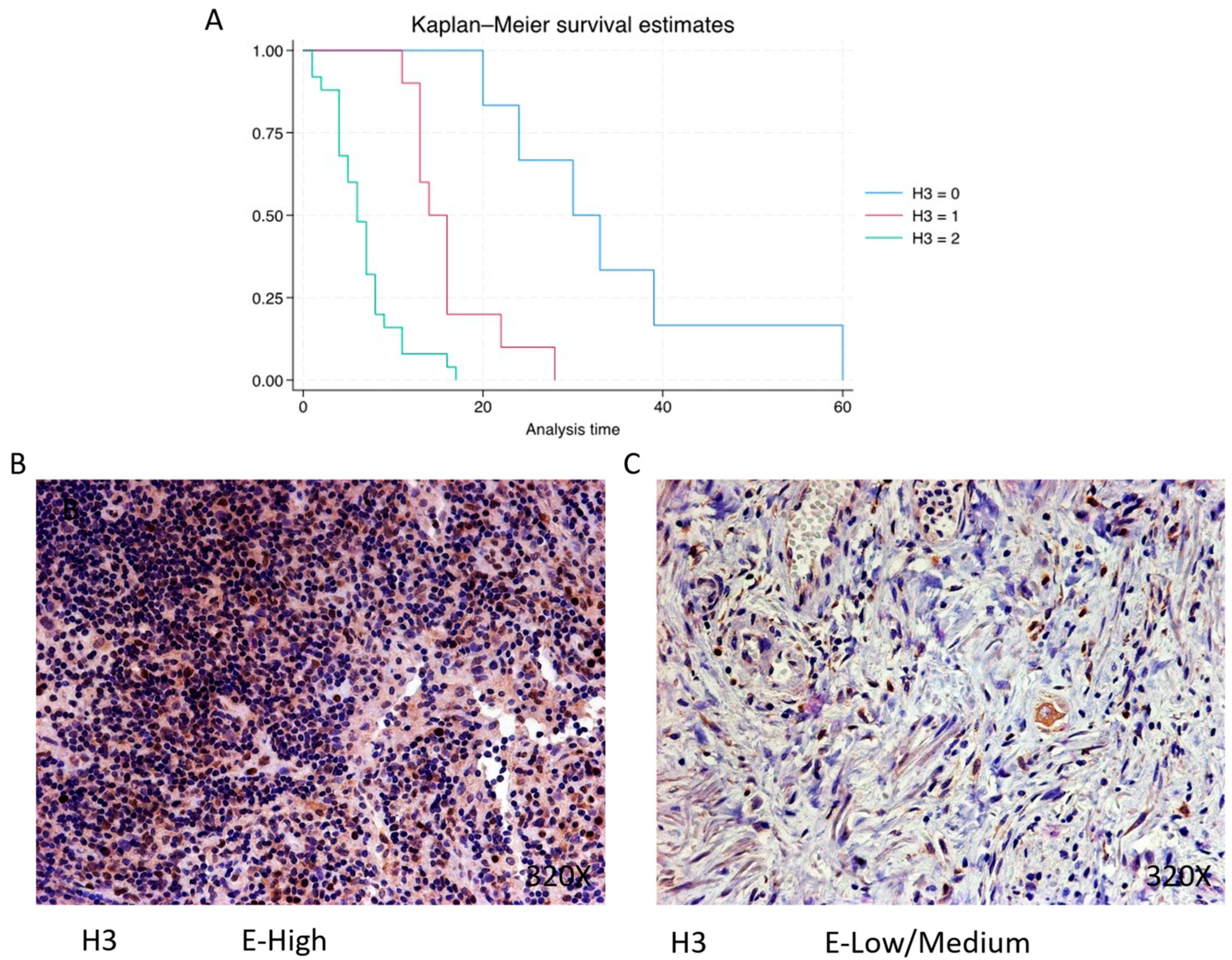
3.2. Patients with Pancreatic Cancer and High Expression Levels of Epigenetic-Related Markers Have Reduced Survival
3.3. Increased Expression of the Metabolic Enzyme PGAM1 Is Associated with Decreased Survival in Pancreatic Cancer Patients
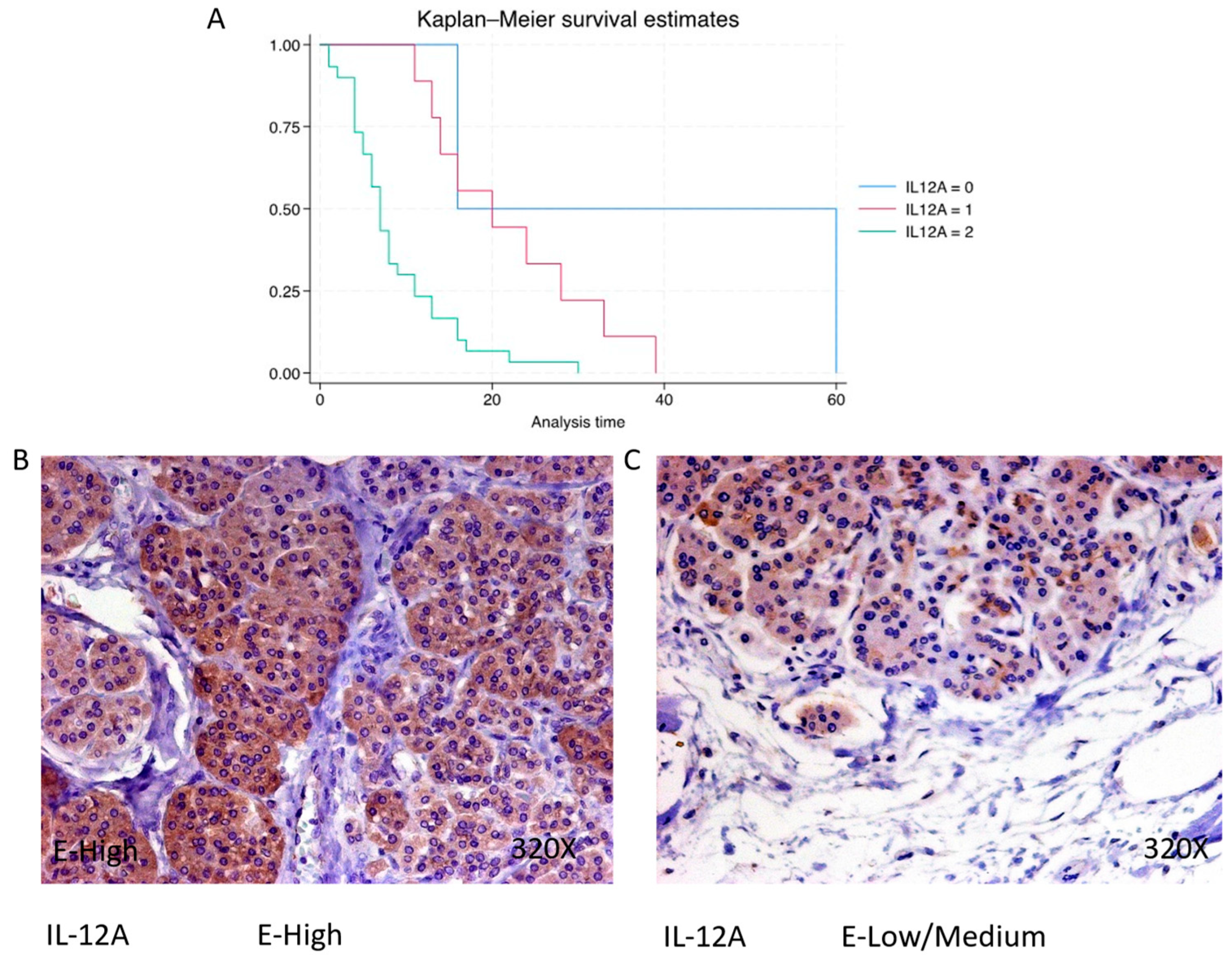
3.4. AIF-1, IL-12A and IL-18 Are Directly Related to Pancreatic Cancer Mortality, Whereas IL-10 Shows an Inverse Association
3.5. Correlation Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tumor stage 4 | 31.71% (13/41) |
| Tumor stage ≤ 4 | 68.29% (28/41) |
| Median levels of Ca 19.9 U/mL (0–37) | 102.10 [44.91–805.00] |
| Median levels of CEA ng/mL (0–5) | 5.43 [2.71–11.31] |
| Median levels of AFP ng/mL (0–13.4) | 2.32 [1.46–4.39] |
| Molecular Marker | Level of Expression | N = 41 n (%): | Median Survival | Q1–Q3 | Hazard Ratio | Confidence Interval | p Value |
|---|---|---|---|---|---|---|---|
| HAT-1 | Negative | 1 (2.44) | 60 | 60–60 | |||
| Low/Moderate | 6 (14.63) | 29 | 25–32.2 | 21.743 | [2.908621–162.5435] | 0.003 ** | |
| High | 34 (82.93) | 7.5 | 5–13 | ||||
| IMP-4 | Negative | 1 (2.44) | 60 | 60–60 | |||
| Low/Moderate | 12 (29.27) | 21 | 15.2–28.5 | 8.094 | [3.080211–21.26741] | <0.001 *** | |
| High | 28 (68.29) | 7 | 4–9.5 | ||||
| IMP-5 | Negative | 2 (4.88) | 45 | 37.5–52.5 | |||
| Low/Moderate | 11 (26.83) | 20 | 16–26 | 7.493 | [3.066998–18.30788] | <0.001 *** | |
| High | 28 (68.29) | 7 | 4–9.5 | ||||
| NASP | Negative | 2 (4.88) | 45 | 37.5–52.5 | |||
| Low/Moderate | 10 (24.39) | 21 | 16–27 | 7.563 | [2.927238–19.53798] | <0.001 *** | |
| High | 29 (70.73) | 7 | 4–11 | ||||
| RBBP7 | Negative | 3 (7.32) | 30 | 23–45 | |||
| Low/Moderate | 5 (12.2) | 24 | 20–33 | 4.024 | [1.787804–9.058966] | <0.001 *** | |
| High | 33 (80.49) | 7 | 5–13 | ||||
| H3 | Negative | 6 (14.63) | 31.5 | 25.5–37.5 | |||
| Low/Moderate | 10 (24.39) | 15 | 13–16 | 5.386 | [2.734019–10.60884] | <0.001 *** | |
| High | 25 (60.98) | 6 | 4–8 | ||||
| H4 | Negative | 6 (14.63) | 31.5 | 25.5–37.5 | |||
| Low/Moderate | 9 (21.95) | 14 | 13–16 | 4.932 | [2.481096–9.801876] | <0.001 *** | |
| High | 26 (63.42) | 6.5 | 4–8 | ||||
| ASF-1 | Negative | 2 (4.88) | 46.5 | 39.8–53.2 | |||
| Low/Moderate | 9 (21.95) | 22 | 16–28 | 9.004 | [3.161273–25.64641] | <0.001 *** | |
| High | 30 (73.17) | 7 | 4.25–11 | ||||
| PGAM1 | Negative | 1 (2.44) | 60 | 60–60 | |||
| Low/Moderate | 4 (9.76) | 25 | 21.5–29.2 | 3.681 | [1.402629–9.661442] | <0.001 *** | |
| High | 36 (87.8) | 8 | 5–13.2 | ||||
| AIF-1 | Negative | 3 (7.32) | 24 | 22–42 | |||
| Low/Moderate | 14 (34.15) | 16 | 13.2–20.8 | 3.703 | [2.005442–6.836674] | <0.001 *** | |
| High | 24 (58.54) | 6 | 4–8 | ||||
| IL-12A | Negative | 2 (4.88) | 38 | 27–49 | |||
| Low/Moderate | 9 (21.95) | 20 | 14–28 | 3.473 | [1.694996–7.11442] | 0.001 ** | |
| High | 30 (73.17) | 7 | 4.25–11 | ||||
| IL-18 | Negative | 3 (7.32) | 24 | 19–26 | |||
| Low/Moderate | 10 (24.39) | 13 | 8.25–29 | 1.958 | [1.100421–3.485366] | 0.022 * | |
| High | 28 (68.29) | 7 | 4–13.8 | ||||
| IL-10 | Negative | 13 (31.7) | 4 | 4–7 | |||
| Low/Moderate | 23 (56.1) | 11 | 7–16 | 0.265 | [0.1416624–0.4964779] | <0.001 *** | |
| High | 5 (12.2) | 24 | 20–30 |
References
- Pourshams, A.; Sepanlou, S.G.; Ikuta, K.S.; Bisignano, C.; Safiri, S.; Roshandel, G.; Sharif, M.; Khatibian, M.; Fitzmaurice, C.; Nixon, M.R.; et al. The Global, Regional, and National Burden of Pancreatic Cancer and Its Attributable Risk Factors in 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2019, 4, 934–947. [Google Scholar] [CrossRef]
- Hu, J.X.; Lin, Y.Y.; Zhao, C.F.; Chen, W.B.; Liu, Q.C.; Li, Q.W.; Gao, F. Pancreatic Cancer: A Review of Epidemiology, Trend, and Risk Factors. World J. Gastroenterol. 2021, 27, 4298. [Google Scholar] [CrossRef]
- Santucci, C.; Mignozzi, S.; Malvezzi, M.; Boffetta, P.; Collatuzzo, G.; Levi, F.; La Vecchia, C.; Negri, E. European Cancer Mortality Predictions for the Year 2024 with Focus on Colorectal Cancer. Ann. Oncol. 2024, 35, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Pekarek, L.; Fraile-Martinez, O.; Garcia-Montero, C.; Alvarez-Mon, M.A.; Acero, J.; Ruiz-Llorente, L.; García-Honduvilla, N.; Albillos, A.; Buján, J.; Alvarez-Mon, M.; et al. Towards an Updated View on the Clinical Management of Pancreatic Adenocarcinoma: Current and Future Perspectives. Oncol. Lett. 2021, 22, 809. [Google Scholar] [CrossRef] [PubMed]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting Cancer Incidence and Deaths to 2030: The Unexpected Burden of Thyroid, Liver, and Pancreas Cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed]
- Orth, M.; Metzger, P.; Gerum, S.; Mayerle, J.; Schneider, G.; Belka, C.; Schnurr, M.; Lauber, K. Pancreatic Ductal Adenocarcinoma: Biological Hallmarks, Current Status, and Future Perspectives of Combined Modality Treatment Approaches. Radiat. Oncol. 2019, 14, 141. [Google Scholar] [CrossRef] [PubMed]
- Luu, T.T. Review of Immunohistochemistry Biomarkers in Pancreatic Cancer Diagnosis. Front. Oncol. 2021, 11, 799025. [Google Scholar] [CrossRef] [PubMed]
- Pekarek, L.; Fraile-Martinez, O.; Garcia-Montero, C.; Saez, M.A.; Barquero-Pozanco, I.; Del Hierro-Marlasca, L.; de Castro Martinez, P.; Romero-Bazán, A.; Alvarez-Mon, M.A.; Monserrat, J.; et al. Clinical Applications of Classical and Novel Biological Markers of Pancreatic Cancer. Cancers 2022, 14, 1866. [Google Scholar] [CrossRef] [PubMed]
- Ortega, M.A.; Fraile-Martinez, O.; Pekarek, L.; García-Montero, C.; Alvarez-Mon, M.A.; Castellanos, A.J.; García-Honduvilla, N.; Buján, J.; Alvarez-Mon, M.; Sáez, M.A.; et al. Oxidative Stress Markers Are Associated with a Poor Prognosis in Patients with Pancreatic Cancer. Antioxidants 2022, 11, 759. [Google Scholar] [CrossRef]
- Ortega, M.A.; Pekarek, L.; Fraile-Martinez, O.; Garcia-Montero, C.; Saez, M.A.; Asúnsolo, A.; Alvarez-Mon, M.A.; Monserrat, J.; Ruiz-Llorente, L.; García-Honduvilla, N.; et al. Implication of ERBB2 as a Predictive Tool for Survival in Patients with Pancreatic Cancer in Histological Studies. Curr. Oncol. 2022, 29, 2442–2453. [Google Scholar] [CrossRef]
- Martinez-Useros, J.; Garcia-Foncillas, J. Can Molecular Biomarkers Change the Paradigm of Pancreatic Cancer Prognosis? Biomed. Res. Int. 2016, 2016, 4873089. [Google Scholar] [CrossRef] [PubMed]
- Khushman, M.; Bhardwaj, A.; Patel, G.K.; Laurini, J.A.; Roveda, K.; Tan, M.C.; Patton, M.C.; Singh, S.; Taylor, W.; Singh, A.P. Exosomal Markers (CD63 and CD9) Expression Pattern Using Immunohistochemistry in Resected Malignant and Non-Malignant Pancreatic Specimens. Pancreas 2017, 46, 782. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, K.; Neumann, A.; Hinsch, A.; Nentwich, M.F.; El Gammal, A.T.; Vashist, Y.; Perez, D.; Bockhorn, M.; Izbicki, J.R.; Mann, O. Cyclin D1 Is a Strong Prognostic Factor for Survival in Pancreatic Cancer: Analysis of CD G870A Polymorphism, FISH and Immunohistochemistry. J. Surg. Oncol. 2015, 111, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.A.; Tang, J.; Tudur-Smith, C.; Neoptolemos, J.P.; Ghaneh, P. Meta-Analysis of Immunohistochemical Prognostic Markers in Resected Pancreatic Cancer. Br. J. Cancer 2011, 104, 1440. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The next Generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D. Hallmarks of Cancer: New Dimensions. Cancer Discov. 2022, 12, 31–46. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.; Gibbs, P. Inflammation, Biomarkers and Immuno-Oncology Pathways in Pancreatic Cancer. J. Pers. Med. 2019, 9, 20. [Google Scholar] [CrossRef] [PubMed]
- An, S.; Kim, S.K.; Kwon, H.Y.; Kim, C.S.; Bang, H.J.; Do, H.; Kim, B.R.; Kim, K.; Kim, Y. Expression of Immune-Related and Inflammatory Markers and Their Prognostic Impact in Colorectal Cancer Patients. Int. J. Mol. Sci. 2023, 24, 11579. [Google Scholar] [CrossRef] [PubMed]
- Sebestyén, A.; Dankó, T.; Sztankovics, D.; Moldvai, D.; Raffay, R.; Cervi, C.; Krencz, I.; Zsiros, V.; Jeney, A.; Petővári, G. The Role of Metabolic Ecosystem in Cancer Progression—Metabolic Plasticity and MTOR Hyperactivity in Tumor Tissues. Cancer Metastasis Rev. 2021, 40, 989. [Google Scholar] [CrossRef] [PubMed]
- Fraile-Martinez, O.; García-Montero, C.; Pekarek, L.; Saz, J.V.; Alvarez-Mon, M.Á.; Barrena-Blázquez, S.; García-Honduvilla, N.; Buján, J.; Asúnsolo, Á.; Coca, S.; et al. Decreased Survival in Patients with Pancreatic Cancer May Be Associated with an Increase in Histopathological Expression of Inflammasome Marker NLRP3. Histol. Histopathol. 2024, 39, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Esposito, I.; Konukiewitz, B.; Schlitter, A.M.; Klöppel, G. Pathology of Pancreatic Ductal Adenocarcinoma: Facts, Challenges and Future Developments. World J. Gastroenterol. 2014, 20, 13833–13841. [Google Scholar] [CrossRef] [PubMed]
- García-Montero, C.; Fraile-Martinez, O.; Rodriguez-Martín, S.; Funes Moñux, R.M.; Saz, J.V.; Bravo, C.; De Leon-Luis, J.A.; Ruiz-Minaya, M.; Pekarek, L.; Saez, M.A.; et al. Irregular Expression of Cellular Stress Response Markers in the Placenta of Women with Chronic Venous Disease. Antioxidants 2022, 11, 2277. [Google Scholar] [CrossRef] [PubMed]
- Ortega, M.A.; Pekarek, L.; Garcia-Montero, C.; Fraile-Martinez, O.; Saez, M.A.; Asúnsolo, A.; Alvarez-Mon, M.A.; Monserrat, J.; Coca, S.; Toledo-Lobo, M.V.; et al. Prognostic Role of IRS-4 in the Survival of Patients with Pancreatic Cancer. Histol. Histopathol. 2022, 37, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Ortega, M.A.; Fraile-Martínez, O.; García-Montero, C.; Ruiz-Grande, F.; Barrena, S.; Montoya, H.; Pekarek, L.; Zoullas, S.; Alvarez-Mon, M.A.; Sainz, F.; et al. Chronic Venous Disease Patients Show Increased IRS-4 Expression in the Great Saphenous Vein Wall. J. Int. Med. Res. 2021, 49, 03000605211041275. [Google Scholar] [CrossRef] [PubMed]
- Capone, V.; Della Torre, L.; Carannante, D.; Babaei, M.; Altucci, L.; Benedetti, R.; Carafa, V. HAT1: Landscape of Biological Function and Role in Cancer. Cells 2023, 12, 1075. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Fan, P.; Zhao, J.; Meng, Z.; Wu, H.; Wang, B.; Jin, X. Overexpressed Histone Acetyltransferase 1 Regulates Cancer Immunity by Increasing Programmed Death-Ligand 1 Expression in Pancreatic Cancer. J. Exp. Clin. Cancer Res. 2019, 38, 47. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Ren, D.; Zhou, Y.; Shen, J.; Wu, H.; Jin, X. Histone Acetyltransferase 1 Promotes Gemcitabine Resistance by Regulating the PVT1/EZH2 Complex in Pancreatic Cancer. Cell Death Dis. 2021, 12, 878. [Google Scholar] [CrossRef] [PubMed]
- Poziello, A.; Nebbioso, A.; Stunnenberg, H.G.; Martens, J.H.A.; Carafa, V.; Altucci, L. Recent Insights into Histone Acetyltransferase-1: Biological Function and Involvement in Pathogenesis. Epigenetics 2021, 16, 838–850. [Google Scholar] [CrossRef] [PubMed]
- Ortega, M.A.; De Leon-Oliva, D.; Garcia-Montero, C.; Fraile-Martinez, O.; Boaru, D.L.; del Val Toledo Lobo, M.; García-Tuñón, I.; Royuela, M.; García-Honduvilla, N.; Bujan, J.; et al. Understanding HAT1: A Comprehensive Review of Noncanonical Roles and Connection with Disease. Genes 2023, 14, 915. [Google Scholar] [CrossRef] [PubMed]
- Campos, E.I.; Fillingham, J.; Li, G.; Zheng, H.; Voigt, P.; Kuo, W.H.W.; Seepany, H.; Gao, Z.; Day, L.A.; Greenblatt, J.F.; et al. The Program for Processing Newly Synthesized Histones H3.1 and H4. Nat. Struct. Mol. Biol. 2010, 17, 1343–1351. [Google Scholar] [CrossRef] [PubMed]
- Gruber, J.J.; Geller, B.; Lipchik, A.M.; Chen, J.; Salahudeen, A.A.; Ram, A.N.; Ford, J.M.; Kuo, C.J.; Snyder, M.P. HAT1 Coordinates Histone Production and Acetylation via H4 Promoter Binding. Mol. Cell 2019, 75, 711–724.e5. [Google Scholar] [CrossRef] [PubMed]
- Pardal, A.J.; Bowman, A.J. A Specific Role for Importin-5 and NASP in the Import and Nuclear Hand-off of Monomeric H3. eLife 2022, 11, 81755. [Google Scholar] [CrossRef] [PubMed]
- Chervona, Y.; Costa, M. Histone Modifications and Cancer: Biomarkers of Prognosis? Am. J. Cancer Res. 2012, 2, 589. [Google Scholar] [PubMed]
- Lin, H.; Han, Q.; Wang, J.; Zhong, Z.; Luo, H.; Hao, Y.; Jiang, Y. Methylation-Mediated Silencing of RBP7 Promotes Breast Cancer Progression through PPAR and PI3K/AKT Pathway. J. Oncol. 2022, 2022, 9039110. [Google Scholar] [CrossRef] [PubMed]
- Kong, F.; Li, L.; Wang, C.; Zhang, Q.; He, S. MiR-381-3p Suppresses Biological Characteristics of Cancer in Head-Neck Squamous Cell Carcinoma Cells by Targeting Nuclear Autoantigenic Sperm Protein (NASP). Biosci. Biotechnol. Biochem. 2020, 84, 703–713. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Zhu, H.; Zhang, X.; He, X.; Xu, X. Comprehensive Analysis of Pan-Cancer Reveals Potential of ASF1B as a Prognostic and Immunological Biomarker. Cancer Med. 2021, 10, 6897–6916. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Zhang, L.; Zhou, M.; Wang, E.; Meng, B.; Li, Q.; Wang, X.; Wang, Y.; Li, Q. Anti-silencing Function 1B Promotes the Progression of Pancreatic Cancer by Activating C-Myc. Int. J. Oncol. 2023, 62, 8. [Google Scholar] [CrossRef] [PubMed]
- Sharif, F.; Rasul, A.; Ashraf, A.; Hussain, G.; Younis, T.; Sarfraz, I.; Chaudhry, M.A.; Bukhari, S.A.; Ji, X.Y.; Selamoglu, Z.; et al. Phosphoglycerate Mutase 1 in Cancer: A Promising Target for Diagnosis and Therapy. IUBMB Life 2019, 71, 1418–1427. [Google Scholar] [CrossRef]
- Qin, C.; Yang, G.; Yang, J.; Ren, B.; Wang, H.; Chen, G.; Zhao, F.; You, L.; Wang, W.; Zhao, Y. Metabolism of Pancreatic Cancer: Paving the Way to Better Anticancer Strategies. Mol. Cancer 2020, 19, 50. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Tan, X.; Liu, P.; Wu, Y.; Qian, S.; Zhang, X. Phosphoglycerate Mutase 1 (PGAM1) Promotes Pancreatic Ductal Adenocarcinoma (PDAC) Metastasis by Acting as a Novel Downstream Target of the PI3K/Akt/MTOR Pathway. Oncol. Res. 2018, 26, 1123–1131. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Liu, X. Phosphoglycerate Mutase 1: Its Glycolytic and Non-Glycolytic Roles in Tumor Malignant Behaviors and Potential Therapeutic Significance. Onco Targets Ther. 2020, 13, 1787. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Yuan, Y.; Yuan, H.; Wang, J.; Yun, H.; Geng, Y.; Zhao, M.; Li, L.; Weng, Y.; Liu, Z.; et al. Histone Acetyltransferase 1 Is a Succinyltransferase for Histones and Non-Histones and Promotes Tumorigenesis. EMBO Rep. 2021, 22, e50967. [Google Scholar] [CrossRef] [PubMed]
- Deininger, M.H.; Meyermann, R.; Schluesener, H.J. The Allograft Inflammatory Factor-1 Family of Proteins. FEBS Lett. 2002, 514, 115–121. [Google Scholar] [CrossRef] [PubMed]
- De Leon-Oliva, D.; Garcia-Montero, C.; Fraile-Martinez, O.; Boaru, D.L.; García-Puente, L.; Rios-Parra, A.; Garrido-Gil, M.J.; Casanova-Martín, C.; García-Honduvilla, N.; Bujan, J.; et al. AIF1: Function and Connection with Inflammatory Diseases. Biology 2023, 12, 694. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Sun, S.; Zhu, C.; Xie, F.; Cai, Q.; Sun, H.; Chen, G.; Liang, X.; Xie, H.; Shi, J.; et al. Expression of Allograft Inflammatory Factor-1 (AIF-1) in Hepatocellular Carcinoma. Med. Sci. Monit. 2018, 24, 6218–6228. [Google Scholar] [CrossRef]
- Slim, F.A.; Ouellette, G.; Ennour-Idrissi, K.; Jacob, S.; Diorio, C.; Durocher, F. An Isoform of AIF1 Involved in Breast Cancer Aejaz Nasir. Cancer Cell Int. 2018, 18, 167. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhao, X.; Zheng, H.; Zhu, C.; Liu, Y. AIF-1, a Potential Biomarker of Aggressive Tumor Behavior in Patients with Non-Small Cell Lung Cancer. PLoS ONE 2022, 17, e0279211. [Google Scholar] [CrossRef] [PubMed]
- Rao, M.; Yang, Z.; Huang, K.; Liu, W.; Chai, Y. Correlation of AIF-1 Expression with Immune and Clinical Features in 1270 Glioma Samples. J. Mol. Neurosci. 2022, 72, 420–432. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Wang, D.; Li, N.; Sheng, J.; Xie, M.; Zhou, Z.; Cheng, G.; Fan, Y. The Novel Tumor Microenvironment-Related Prognostic Gene AIF1 May Influence Immune Infiltrates and Is Correlated with TIGIT in Esophageal Cancer. Ann. Surg. Oncol. 2022, 29, 2930–2940. [Google Scholar] [CrossRef] [PubMed]
- Ye, Y.; Miao, S.; Lu, R.; Xia, X.; Chen, Y.; Zhang, J.; Wu, X.; He, S.; Qiang, F.; Zhou, J. Allograft Inflammatory Factor-1 Is an Independent Prognostic Indicator That Regulates β-Catenin in Gastric Cancer. Oncol. Rep. 2014, 31, 828–834. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Zhang, D.; Hu, J.; Xu, S.; Xu, C.; Shen, Y. Allograft Inflammatory Factor 1 Is a Potential Diagnostic, Immunological, and Prognostic Biomarker in Pan-Cancer. Aging 2023, 15, 2582. [Google Scholar] [CrossRef] [PubMed]
- Kadoya, M.; Yamamoto, A.; Hamaguchi, M.; Obayashi, H.; Mizushima, K.; Ohta, M.; Seno, T.; Oda, R.; Fujiwara, H.; Kohno, M.; et al. Allograft Inflammatory Factor-1 Stimulates Chemokine Production and Induces Chemotaxis in Human Peripheral Blood Mononuclear Cells. Biochem. Biophys. Res. Commun. 2014, 448, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.Y.; Yan, D.J.; Chen, Z.W. Role of AIF-1 in the Regulation of Inflammatory Activation and Diverse Disease Processes. Cell. Immunol. 2013, 284, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Gil, M.A.; Fraile-Martinez, O.; García-Montero, C.; Toledo, M.D.V.; Guijarro, L.G.; De León-Luis, J.A.; Bravo, C.; Díaz-Pedrero, R.; López-Gonzalez, L.; Saez, M.A.; et al. Histopathological Clues of Enhanced Inflammation in the Placental Tissue of Women with Chronic Venous Disease in Lower Limbs during Pregnancy. J. Pers. Med. 2024, 14, 87. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, K.; Nakanishi, K.; Tsutsui, H. Interleukin-18 in Health and Disease. Int. J. Mol. Sci. 2019, 20, 649. [Google Scholar] [CrossRef] [PubMed]
- Vignali, D.A.A.; Kuchroo, V.K. IL-12 Family Cytokines: Immunological Playmakers. Nat. Immunol. 2012, 13, 722–728. [Google Scholar] [CrossRef] [PubMed]
- El-Kabarity, R.H.; Naguib, A.H. Serum Levels of IL-18, IL-12 and TH-1/TH-2 Ratio in Patients with Pre-Eclampsia. Egypt. J. Immunol. 2011, 18, 1–8. [Google Scholar] [PubMed]
- Behzadi, P.; Behzadi, E.; Ranjbar, R. Il-12 Family Cytokines: General Characteristics, Pathogenic Microorganisms, Receptors, and Signalling Pathways. Acta Microbiol. Immunol. Hung. 2016, 63, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Ortega, M.A.; De Leon-Oliva, D.; García-Montero, C.; Fraile-Martinez, O.; Boaru, D.L.; de Castro, A.V.; Saez, M.A.; Lopez-Gonzalez, L.; Bujan, J.; Alvarez-Mon, M.A.; et al. Reframing the Link between Metabolism and NLRP3 Inflammasome: Therapeutic Opportunities. Front. Immunol. 2023, 14, 1232629. [Google Scholar] [CrossRef] [PubMed]
- Mirlekar, B.; Pylayeva-Gupta, Y. IL-12 Family Cytokines in Cancer and Immunotherapy. Cancers 2021, 13, 167. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Cheon, S.; Cho, D. The Dual Effects of Interleukin-18 in Tumor Progression. Cell. Mol. Immunol. 2007, 4, 329–335. [Google Scholar] [PubMed]
- Lutz, V.; Hellmund, V.M.; Picard, F.S.R.; Raifer, H.; Ruckenbrod, T.; Klein, M.; Bopp, T.; Savai, R.; Duewell, P.; Keber, C.U.; et al. IL18 Receptor Signaling Regulates Tumor-Reactive CD8+ T-Cell Exhaustion via Activation of the IL2/STAT5/MTOR Pathway in a Pancreatic Cancer Model. Cancer Immunol. Res. 2023, 11, 421–434. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Yu, X.; Werner, J.; Bazhin, A.V.; D’Haese, J.G. The Role of Interleukin-18 in Pancreatitis and Pancreatic Cancer. Cytokine Growth Factor Rev. 2019, 50, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Zheng, L.; Jiang, J.; Zhao, Y.; Wang, X.; Shen, M.; Zhu, F.; Tian, R.; Shi, C.; Xu, M.; et al. Blocking NF-ΚB Is Essential for the Immunotherapeutic Effect of Recombinant IL18 in Pancreatic Cancer. Clin. Cancer Res. 2016, 22, 5939–5950. [Google Scholar] [CrossRef] [PubMed]
- Bellone, G.; Smirne, C.; Mauri, F.A.; Tonel, E.; Carbone, A.; Buffolino, A.; Dughera, L.; Robecchi, A.; Pirisi, M.; Emanuelli, G. Cytokine Expression Profile in Human Pancreatic Carcinoma Cells and in Surgical Specimens: Implications for Survival. Cancer Immunol. Immunother. 2006, 55, 684–698. [Google Scholar] [CrossRef] [PubMed]
- Iyer, S.S.; Cheng, G. Role of Interleukin 10 Transcriptional Regulation in Inflammation and Autoimmune Disease. Crit. Rev. Immunol. 2012, 32, 23–63. [Google Scholar] [CrossRef] [PubMed]
- Mannino, M.H.; Zhu, Z.; Xiao, H.; Bai, Q.; Wakefield, M.R.; Fang, Y. The Paradoxical Role of IL-10 in Immunity and Cancer. Cancer Lett. 2015, 367, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Yako, Y.Y.; Kruger, D.; Smith, M.; Brand, M. Cytokines as Biomarkers of Pancreatic Ductal Adenocarcinoma: A Systematic Review. PLoS ONE 2016, 11, 154016. [Google Scholar] [CrossRef] [PubMed]
- González-Borja, I.; Viúdez, A.; Alors-Pérez, E.; Goñi, S.; Amat, I.; Ghanem, I.; Pazo-Cid, R.; Feliu, J.; Alonso, L.; López, C.; et al. Cytokines and Lymphoid Populations as Potential Biomarkers in Locally and Borderline Pancreatic Adenocarcinoma. Cancers 2022, 14, 5993. [Google Scholar] [CrossRef]
- Feng, L.; Qi, Q.; Wang, P.; Chen, H.; Chen, Z.; Meng, Z.; Liu, L. Serum Levels of IL-6, IL-8, and IL-10 Are Indicators of Prognosis in Pancreatic Cancer. J. Int. Med. Res. 2018, 46, 5228–5236. [Google Scholar] [CrossRef]
- Zhao, C.; Pu, Y.; Zhang, H.; Hu, X.; Zhang, R.; He, S.; Zhao, Q.; Mu, B. IL10-Modified Human Mesenchymal Stem Cells Inhibit Pancreatic Cancer Growth through Angiogenesis Inhibition. J. Cancer 2020, 11, 5345. [Google Scholar] [CrossRef]















| Antigen | Species | Dilution | Provider | Protocol Specification |
|---|---|---|---|---|
| HAT-1 | Rabbit monoclonal | 1:1000 | Abcam Cambridge, UK (ab193097) | 100% Triton 0.1% in PBS, 10 min, before incubation with blocking solution |
| IPO-4 | Rabbit monoclonal | 1:100 | Abcam (ab181046) | 10 mM sodium citrate pH = 6 before incubation with blocking solution |
| IPO-5 | Rabbit polyclonal | 1:100 | Abcam (ab187175) | 100% Triton 0.1% in PBS, 10 min, before incubation with blocking solution |
| NASP | Mouse monoclonal | 1:100 | Santa Cruz Biotechnology, Santa Cruz, CA, USA (sc.514669) | 10 mM sodium citrate pH = 6 before incubation with blocking solution |
| RBBP7 | Rabbit monoclonal | 1:2000 | Abcam (ab259957) | 10 mM sodium citrate pH = 6 before incubation with blocking solution |
| H3 | Rabbit polyclonal | 1:100 | Abcam (ab1791) | 100% Triton 0.1% in PBS, 10 min, before incubation with blocking solution |
| H4 | Rabbit monoclonal | 1:500 | Abcam (ab51997) | EDTA pH = 9 before incubation with blocking solution |
| ASF-1 | Rabbit polyclonal | 1:100 | Abcam (ab235358) | 100% Triton 0.1% in PBS, 10 min, before incubation with blocking solution |
| PGAM-1 | Rabbit monoclonal | 1:25 | Abcam (ab247037) | EDTA pH = 9 before incubation with blocking solution |
| AIF-1 | Goat polyclonal | 1:500 | Abcam (ab5076) | EDTA pH = 9 before incubation with blocking solution |
| IL-12A | Rabbit monoclonal | 1:100 | Abcam (ab131039) | EDTA pH = 9 before incubation with blocking solution |
| IL-18 | Rabbit monoclonal | 1:250 | Abcam (ab243091) | 10 mM sodium citrate pH = 6 before incubation with blocking solution |
| IL-10 | Rabbit Polyclonal | 1:100 | Abcam (ab217941) | 100% Triton 0.1% in PBS, 10 min, before incubation with blocking solution |
| Age (Median [IQR]) | 72.00 [45.00–88.00] |
| Sex (n (%)) | |
| Men | 27 (65.85%) |
| Women | 14 (34.15%) |
| Smoking habits | 18 (43.90%) |
| Drinking habits | 11 (26.83%) |
| Obesity | 2 (4.88%) |
| Type 2 diabetes mellitus | 15 (55.56%) |
| Chronic maladies | 4 (9.76%) |
| Previous malignancies | 11 (26.83%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortega, M.A.; Jiménez-Álvarez, L.; Fraile-Martinez, O.; Garcia-Montero, C.; Guijarro, L.G.; Pekarek, L.; Barrena-Blázquez, S.; Asúnsolo, Á.; López-González, L.; Toledo-Lobo, M.D.V.; et al. Prognostic Value of Histone Acetyl Transferase 1 (HAT-1) and Inflammatory Signatures in Pancreatic Cancer. Curr. Issues Mol. Biol. 2024, 46, 3839-3865. https://0-doi-org.brum.beds.ac.uk/10.3390/cimb46050239
Ortega MA, Jiménez-Álvarez L, Fraile-Martinez O, Garcia-Montero C, Guijarro LG, Pekarek L, Barrena-Blázquez S, Asúnsolo Á, López-González L, Toledo-Lobo MDV, et al. Prognostic Value of Histone Acetyl Transferase 1 (HAT-1) and Inflammatory Signatures in Pancreatic Cancer. Current Issues in Molecular Biology. 2024; 46(5):3839-3865. https://0-doi-org.brum.beds.ac.uk/10.3390/cimb46050239
Chicago/Turabian StyleOrtega, Miguel A., Laura Jiménez-Álvarez, Oscar Fraile-Martinez, Cielo Garcia-Montero, Luis G. Guijarro, Leonel Pekarek, Silvestra Barrena-Blázquez, Ángel Asúnsolo, Laura López-González, María Del Val Toledo-Lobo, and et al. 2024. "Prognostic Value of Histone Acetyl Transferase 1 (HAT-1) and Inflammatory Signatures in Pancreatic Cancer" Current Issues in Molecular Biology 46, no. 5: 3839-3865. https://0-doi-org.brum.beds.ac.uk/10.3390/cimb46050239