
Meibum Lipidomic Analysis in Evaporative Dry Eye Subjects

 ,
,  ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Lipidomic Profiling Untargeted Analysis
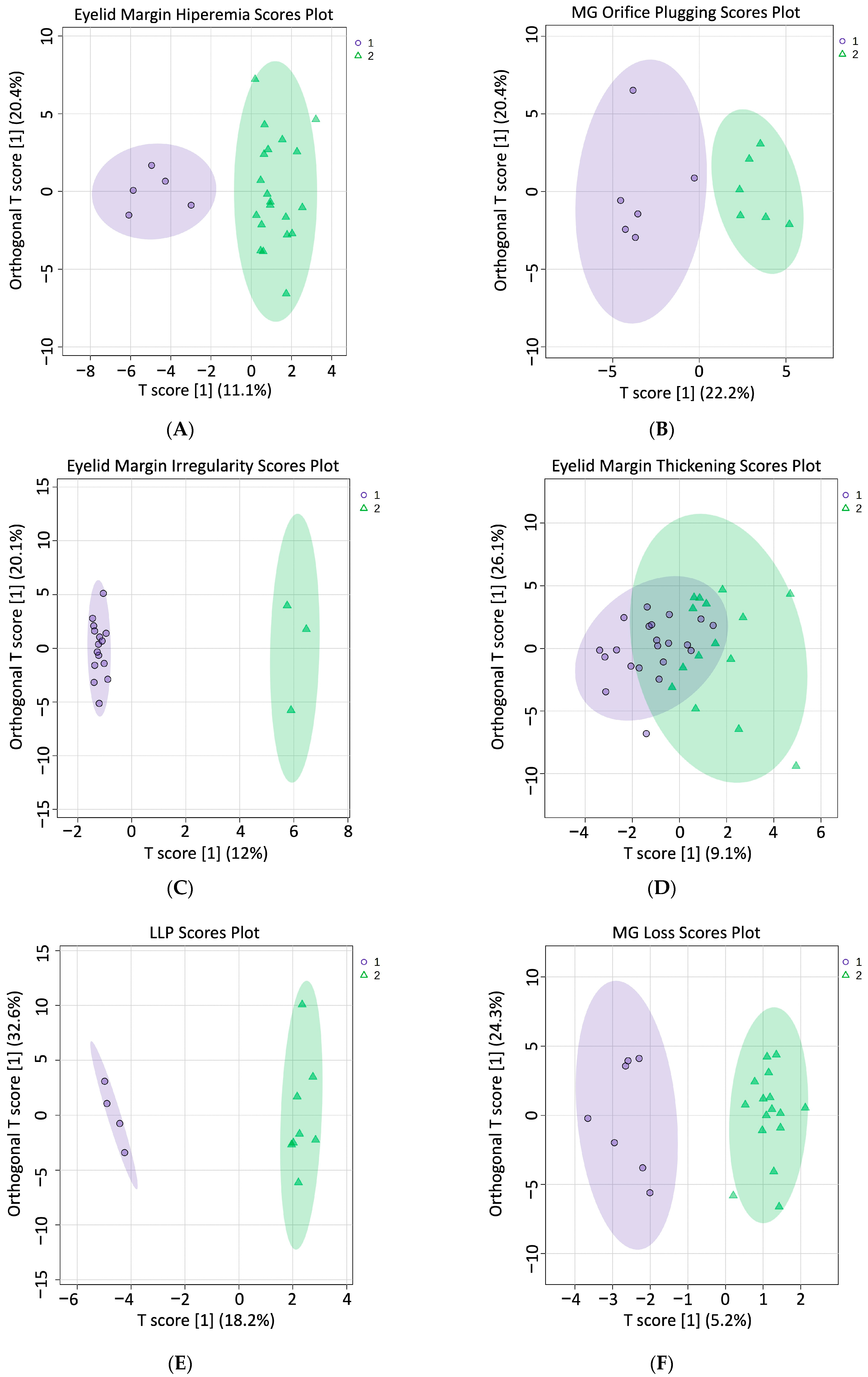
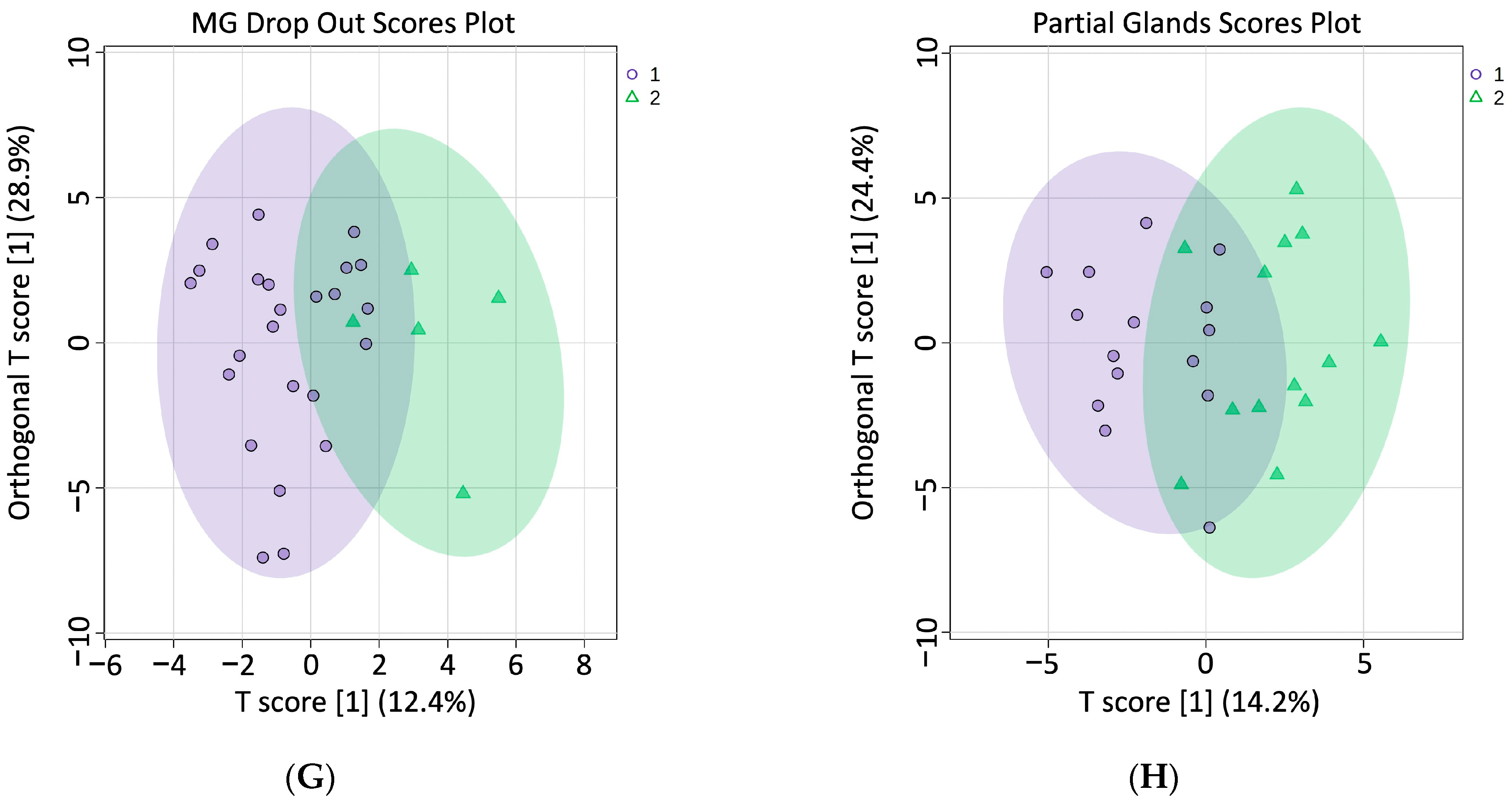
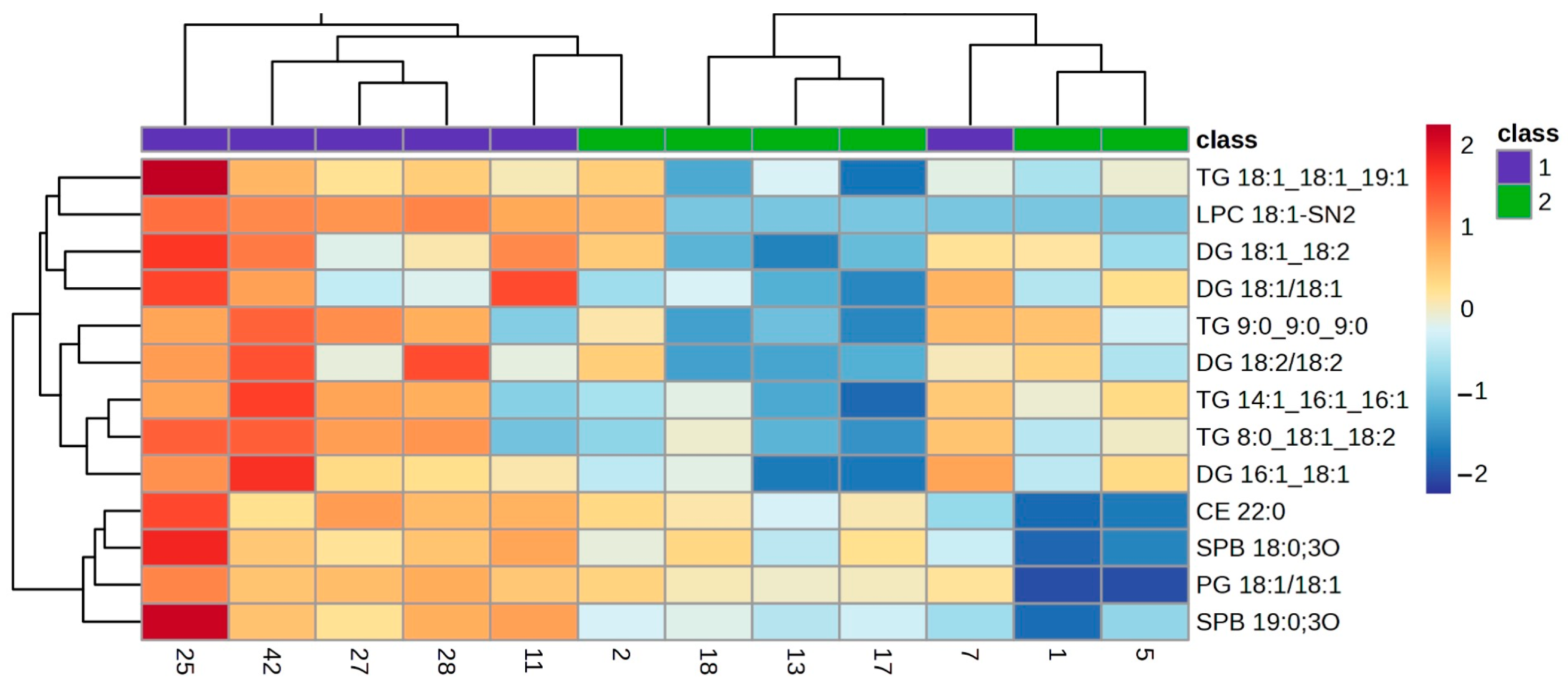
2.2. Comparison of Meibum Lipids between Groups
3. Discussion
4. Materials and Methods
4.1. Sample and Study Design
4.2. Ocular Procedures
4.2.1. Lipid Layer Patterns
4.2.2. Eyelid Margin Abnormalities
4.2.3. Meibography
4.2.4. Meibum Sample Collection
4.3. Materials for Sample Preparation and Liquid Chromatography
4.4. Meibum Sample Preparation
4.5. Liquid Chromatography–Mass Spectrometry Analysis
4.6. Lipid Annotation
4.7. Statistical Analysis
5. Conclusions
6. Future Perspectives
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Knop, E.; Knop, N.; Millar, T.; Obata, H.; Sullivan, D.A. The international workshop on meibomian gland dysfunction: Report of the subcommittee on anatomy, physiology, and pathophysiology of the meibomian gland. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1938–1978. [Google Scholar] [CrossRef] [PubMed]
- Butovich, I.A. Meibomian glands, meibum, and meibogenesis. Exp. Eye Res. 2017, 163, 2–16. [Google Scholar] [CrossRef] [PubMed]
- Cwiklik, L. Tear film lipid layer: A molecular level view. Biochim. Biophys. Acta 2016, 1858, 2421–2430. [Google Scholar] [CrossRef] [PubMed]
- Pflugfelder, S.C.; Stern, M.E. Biological functions of tear film. Exp. Eye Res. 2020, 197, 108115. [Google Scholar] [CrossRef] [PubMed]
- Butovich, I.A.; Uchiyama, E.; Di Pascuale, M.A.; McCulley, J.P. Liquid chromatography-mass spectrometric analysis of lipids present in human meibomian gland secretions. Lipids 2007, 42, 765–776. [Google Scholar] [CrossRef] [PubMed]
- Arita, R.; Mori, N.; Shirakawa, R.; Asai, K.; Imanaka, T.; Fukano, Y.; Nakamura, M. Linoleic acid content of human meibum is associated with telangiectasia and plugging of gland orifices in meibomian gland dysfunction. Exp. Eye Res. 2016, 145, 359–362. [Google Scholar] [CrossRef] [PubMed]
- Paranjpe, V.; Tan, J.; Nguyen, J.; Lee, J.; Allegood, J.; Galor, A.; Mandal, N. Clinical signs of meibomian gland dysfunction (MGD) are associated with changes in meibum sphingolipid composition. Ocul. Surf. 2019, 17, 318–326. [Google Scholar] [CrossRef]
- Pucker, A.D.; Haworth, K.M. The presence and significance of polar meibum and tear lipids. Ocul. Surf. 2015, 13, 26–42. [Google Scholar] [CrossRef]
- Suzuki, T.; Kitazawa, K.; Cho, Y.; Yoshida, M.; Okumura, T.; Sato, A.; Kinoshita, S. Alteration in meibum lipid composition and subjective symptoms due to aging and meibomian gland dysfunction. Ocul. Surf. 2022, 26, 310–317. [Google Scholar] [CrossRef]
- Craig, J.P.; Nichols, K.K.; Akpek, E.K.; Caffery, B.; Dua, H.S.; Joo, C.K.; Liu, Z.; Nelson, J.D.; Nichols, J.J.; Tsubota, K.; et al. TFOS DEWS II Definition and Classification Report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef]
- Wolffsohn, J.S.; Arita, R.; Chalmers, R.; Djalilian, A.; Dogru, M.; Dumbleton, K.; Gupta, P.K.; Karpecki, P.; Lazreg, S.; Pult, H.; et al. TFOS DEWS II Diagnostic Methodology report. Ocul. Surf. 2017, 15, 539–574. [Google Scholar] [CrossRef]
- Arita, R.; Minoura, I.; Morishige, N.; Shirakawa, R.; Fukuoka, S.; Asai, K.; Goto, T.; Imanaka, T.; Nakamura, M. Development of Definitive and Reliable Grading Scales for Meibomian Gland Dysfunction. Am. J. Ophthalmol. 2016, 169, 125–137. [Google Scholar] [CrossRef]
- Pult, H. Relationships Between Meibomian Gland Loss and Age, Sex, and Dry Eye. Eye Contact Lens 2018, 44 (Suppl. S2), S318–S324. [Google Scholar] [CrossRef] [PubMed]
- Guillon, J.-P. Non-invasive tearscope plus routine for contact lens fitting. Contact Lens Anterior Eye 1998, 21, S31–S40. [Google Scholar] [CrossRef] [PubMed]
- Arita, R.; Morishige, N.; Fujii, T.; Fukuoka, S.; Chung, J.L.; Seo, K.Y.; Itoh, K. Tear Interferometric Patterns Reflect Clinical Tear Dynamics in Dry Eye Patients. Investig. Ophthalmol. Vis. Sci. 2016, 57, 3928–3934. [Google Scholar] [CrossRef]
- Robciuc, A.; Hyotylainen, T.; Jauhiainen, M.; Holopainen, J.M. Ceramides in the pathophysiology of the anterior segment of the eye. Curr. Eye Res. 2013, 38, 1006–1016. [Google Scholar] [CrossRef]
- Tiffany, J.M. Individual variations in human meibomian lipid composition. Exp. Eye Res. 1978, 27, 289–300. [Google Scholar] [CrossRef]
- Harvey, D.J. Identification by gas chromatography/mass spectrometry of long-chain fatty acids and alcohols from hamster meibomian glands using picolinyl and nicotinate derivatives. Biomed. Chromatogr. 1989, 3, 251–254. [Google Scholar] [CrossRef]
- Shine, W.E.; McCulley, J.P. The role of cholesterol in chronic blepharitis. Investig. Ophthalmol. Vis. Sci. 1991, 32, 2272–2280. [Google Scholar]
- Shine, W.E.; McCulley, J.P. Meibomianitis: Polar lipid abnormalities. Cornea 2004, 23, 781–783. [Google Scholar] [CrossRef]
- Yang, Q.; Li, B.; Sheng, M. Meibum lipid composition in type 2 diabetics with dry eye. Exp. Eye Res. 2021, 206, 108522. [Google Scholar] [CrossRef] [PubMed]
- Eom, Y.; Choi, K.E.; Kang, S.Y.; Lee, H.K.; Kim, H.M.; Song, J.S. Comparison of meibomian gland loss and expressed meibum grade between the upper and lower eyelids in patients with obstructive meibomian gland dysfunction. Cornea 2014, 33, 448–452. [Google Scholar] [CrossRef] [PubMed]
- Galor, A.; Sanchez, V.; Jensen, A.; Burton, M.; Maus, K.; Stephenson, D.; Chalfant, C.; Mandal, N. Meibum sphingolipid composition is altered in individuals with meibomian gland dysfunction-a side by side comparison of Meibum and Tear Sphingolipids. Ocul. Surf. 2022, 23, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Khanal, S.; Bai, Y.; Ngo, W.; Nichols, K.K.; Wilson, L.; Barnes, S.; Nichols, J.J. Human meibum and tear film derived cholesteryl and wax esters in meibomian gland dysfunction and tear film structure. Ocul. Surf. 2022, 23, 12–23. [Google Scholar] [CrossRef] [PubMed]
- Kind, T.; Okazaki, Y.; Saito, K.; Fiehn, O. LipidBlast templates as flexible tools for creating new in-silico tandem mass spectral libraries. Anal. Chem. 2014, 86, 11024–11027. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Tu, J.; Xiong, X.; Shen, X.; Zhu, Z.J. LipidCCS: Prediction of Collision Cross-Section Values for Lipids with High Precision To Support Ion Mobility-Mass Spectrometry-Based Lipidomics. Anal. Chem. 2017, 89, 9559–9566. [Google Scholar] [CrossRef] [PubMed]
- Borchman, D.; Foulks, G.N.; Yappert, M.C. Confirmation of changes in human meibum lipid infrared spectra with age using principal component analysis. Curr. Eye Res. 2010, 35, 778–786. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Queiruga, J.; Pena-Verdeal, H.; Sabucedo-Villamarin, B.; Giraldez, M.J.; Garcia-Resua, C.; Yebra-Pimentel, E. Meibomian gland secretion quality association with ocular parameters in university students during COVID-19 restrictions. Int. Ophthalmol. 2023, 43, 2349–2362. [Google Scholar] [CrossRef]
- Kunnen, C.M.; Brown, S.H.; Lazon de la Jara, P.; Holden, B.A.; Blanksby, S.J.; Mitchell, T.W.; Papas, E.B. Influence of Meibomian Gland Expression Methods on Human Lipid Analysis Results. Ocul. Surf. 2016, 14, 49–55. [Google Scholar] [CrossRef]
- Ha, M.; Kim, J.S.; Hong, S.Y.; Chang, D.J.; Whang, W.J.; Na, K.S.; Kim, E.C.; Kim, H.S.; Hwang, H.S. Relationship between eyelid margin irregularity and meibomian gland dropout. Ocul. Surf. 2021, 19, 31–37. [Google Scholar] [CrossRef]
- Huang, B.; Fei, F.; Wen, H.; Zhu, Y.; Wang, Z.; Zhang, S.; Hu, L.; Chen, W.; Zheng, Q. Impacts of gender and age on meibomian gland in aged people using artificial intelligence. Front. Cell Dev. Biol. 2023, 11, 1199440. [Google Scholar] [CrossRef] [PubMed]
- Foulks, G.N.; Bron, A.J. Meibomian gland dysfunction: A clinical scheme for description, diagnosis, classification, and grading. Ocul. Surf. 2003, 1, 107–126. [Google Scholar] [CrossRef] [PubMed]
- Pult, H.; Riede-Pult, B.H. Non-contact meibography: Keep it simple but effective. Contact Lens Anterior Eye J. Br. Contact Lens Assoc. 2012, 35, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, A.; Bron, A.J.; Korb, D.R.; Amano, S.; Paugh, J.R.; Pearce, E.I.; Yee, R.; Yokoi, N.; Arita, R.; Dogru, M. The international workshop on meibomian gland dysfunction: Report of the diagnosis subcommittee. Investig. Ophthalmol. Vis. Sci. 2011, 52, 2006–2049. [Google Scholar] [CrossRef] [PubMed]
- Meier, F.; Brunner, A.D.; Koch, S.; Koch, H.; Lubeck, M.; Krause, M.; Goedecke, N.; Decker, J.; Kosinski, T.; Park, M.A.; et al. Online Parallel Accumulation-Serial Fragmentation (PASEF) with a Novel Trapped Ion Mobility Mass Spectrometer. Mol. Cell Proteom. 2018, 17, 2534–2545. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Queiruga, J.; Pena-Verdeal, H.; Sabucedo-Villamarin, B.; Giraldez, M.J.; Garcia-Resua, C.; Yebra-Pimentel, E. A cross-sectional study of non-modifiable and modifiable risk factors of dry eye disease states. Contact Lens Anterior Eye J. Br. Contact Lens Assoc. 2023, 46, 101800. [Google Scholar] [CrossRef] [PubMed]
- Sabucedo-Villamarin, B.; Pena-Verdeal, H.; Garcia-Queiruga, J.; Giraldez, M.J.; Garcia-Resua, C.; Yebra-Pimentel, E. Categorization of the Aqueous Deficient Dry Eye by a Cut-Off Criterion of TMH Measured with Tearscope. Life 2022, 12, 2007. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Queiruga, J.; Pena-Verdeal, H.; Sabucedo-Villamarin, B.; Garcia-Resua, C.; Giraldez, M.J.; Yebra-Pimentel, E. Analysis of the Differences in Ocular Surface Damage and Inflammatory Signs between Healthy and Evaporative Dry Eye Participants. Ocul. Immunol. Inflamm. 2023, 31, 970–977. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Kind, T.; Vaniya, A.; Gennity, I.; Fahrmann, J.F.; Fiehn, O. An in silico MS/MS library for automatic annotation of novel FAHFA lipids. J. Cheminform 2015, 7, 53. [Google Scholar] [CrossRef]
- Zhou, Z.; Luo, M.; Chen, X.; Yin, Y.; Xiong, X.; Wang, R.; Zhu, Z.J. Ion mobility collision cross-section atlas for known and unknown metabolite annotation in untargeted metabolomics. Nat. Commun. 2020, 11, 4334. [Google Scholar] [CrossRef]
- Leaptrot, K.L.; May, J.C.; Dodds, J.N.; McLean, J.A. Ion mobility conformational lipid atlas for high confidence lipidomics. Nat. Commun. 2019, 10, 985. [Google Scholar] [CrossRef] [PubMed]
- Rocha, B.; Illiano, A.; Calamia, V.; Pinto, G.; Amoresano, A.; Ruiz-Romero, C.; Blanco, F.J. Targeted phospholipidomic analysis of synovial fluid as a tool for osteoarthritis deep phenotyping. Osteoarthr. Cart. Open 2021, 3, 100219. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lipid Class | Nº Lipids | |
|---|---|---|
| Ceramides | (Cer) | 15 |
| Hexosyceramides | (HexCer) | 1 |
| Monodiacyglycerophosphocholines | (LPC) | 8 |
| Diacylglycerophosphocholines | (PC) | 15 |
| Diacylglycerophosphoethanolamines | (PE) | 2 |
| Diacylglycerophosphoglycerols | (PG) | 2 |
| Diacylglycerophosphoinositols | (PI) | 1 |
| Ceramide phosphocholenes | (SM) | 10 |
| Sphingosines | (SPB) | 10 |
| Cholesterol Ester | (CE) | 16 |
| Diacyglycerols | (DG) | 13 |
| Triacylglycerols | (TG) | 38 |
| Procedure | Scheme | Classification Criteria | |
|---|---|---|---|
| LLP | Guillon et al. [14] |
| |
| Eyelid Margin Abnormalities | Hyperaemia | Arita et al. [12] |
|
| MG orifice plugging | Arita et al. [12] |
| |
| Irregularity | Arita et al. [12] |
| |
| Eyelid margin thickening | Arita et al. [12] |
| |
| Meibography | MG loss | Pult et al. [13] |
|
| MG drop out | Arita et al. [12] |
| |
| Partial glands | Arita et al. [12] |
| |
| Scores Range | Scores Included in Statistical Study | n | ||
|---|---|---|---|---|
| Group 1 | Group 2 | |||
| LLP | 1 to 5 | =1 | ≥4 | 12 |
| Eyelid Margin Hyperaemia | 0 to 6 | ≤1 | ≥4 | 25 |
| MG Orifice Plugging | 0 to 6 | =0 | ≥4 | 12 |
| Eyelid Margin Irregularity | 0 to 4 | =0 | ≥3 | 17 |
| Eyelid Margin Thickening | 0 to 4 | =0 | ≥2 | 36 |
| MG Loss | 0 to 6 | =0 | ≥3 | 23 |
| MG Drop Out | 0 to 4 | =0 | ≥3 | 29 |
| Partial Glands | 0 to 6 | ≤2 | ≥5 | 28 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia-Queiruga, J.; Pena-Verdeal, H.; Sabucedo-Villamarin, B.; Paz-Tarrio, M.; Guitian-Fernandez, E.; Garcia-Resua, C.; Yebra-Pimentel, E.; Giraldez, M.J. Meibum Lipidomic Analysis in Evaporative Dry Eye Subjects. Int. J. Mol. Sci. 2024, 25, 4782. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms25094782
Garcia-Queiruga J, Pena-Verdeal H, Sabucedo-Villamarin B, Paz-Tarrio M, Guitian-Fernandez E, Garcia-Resua C, Yebra-Pimentel E, Giraldez MJ. Meibum Lipidomic Analysis in Evaporative Dry Eye Subjects. International Journal of Molecular Sciences. 2024; 25(9):4782. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms25094782
Chicago/Turabian StyleGarcia-Queiruga, Jacobo, Hugo Pena-Verdeal, Belen Sabucedo-Villamarin, Monica Paz-Tarrio, Esteban Guitian-Fernandez, Carlos Garcia-Resua, Eva Yebra-Pimentel, and Maria J. Giraldez. 2024. "Meibum Lipidomic Analysis in Evaporative Dry Eye Subjects" International Journal of Molecular Sciences 25, no. 9: 4782. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms25094782