
CYP7B1 as a Biomarker for Prostate Cancer Risk and Progression: Metabolic and Oncogenic Signatures (Diagnostic Immunohistochemistry Analysis by Tissue Microarray in Prostate Cancer Patients—Diamond Study)

 ,
,  ,
,  , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Increased Expression of CYP7B1 in Patients with PC
2.2. The Association between CYP7B1 and Other Proteins Involved in Cancer and Metabolic Processes
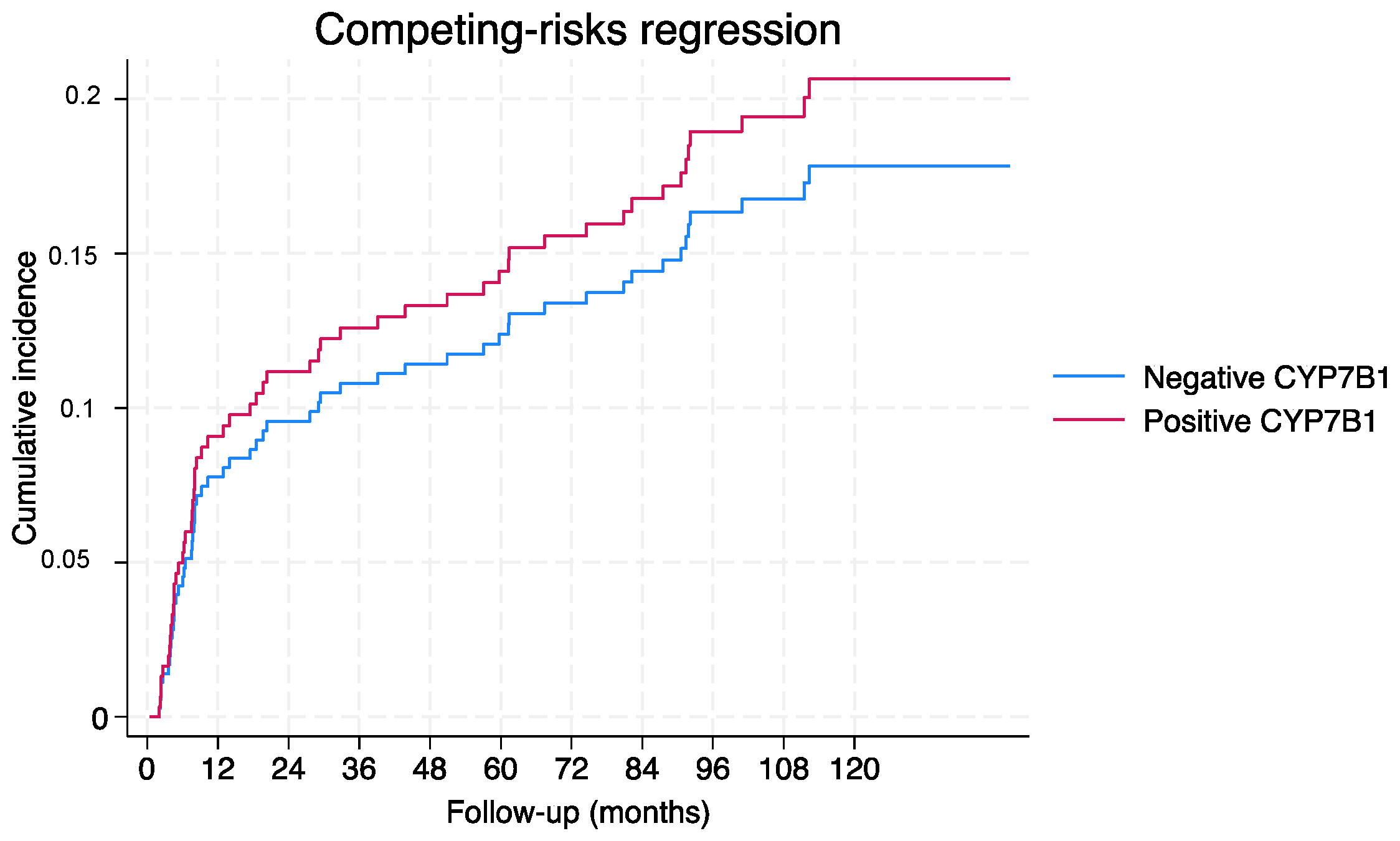
2.3. Association between CYP7B1 Expression and the Risk of Biochemical Recurrence in Patients with PC
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Immunohistochemistry
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Culp, M.B.; Soerjomataram, I.; Efstathiou, J.A.; Bray, F.; Jemal, A. Recent Global Patterns in Prostate Cancer Incidence and Mortality Rates. Eur. Urol. 2020, 77, 38–52. [Google Scholar] [CrossRef]
- He, Y.; Johnson, D.T.; Yang, J.S.; Wu, H.; You, S.; Yoon, J.; Lee, D.-H.; Kim, W.K.; Aldahl, J.; Le, V.; et al. Loss of the tumor suppressor, Tp53, enhances the androgen receptor-mediated oncogenic transformation and tumor development in the mouse prostate. Oncogene 2019, 38, 6507–6520. [Google Scholar] [CrossRef] [PubMed]
- Ando, T.; Nishiyama, T.; Takizawa, I.; Ishizaki, F.; Miyashiro, Y.; Takeda, K.; Hara, N.; Tomita, Y. Dihydrotestosterone synthesis pathways from inactive androgen 5α-androstane-3β,17β-diol in prostate cancer cells: Inhibition of intratumoural 3β-hydroxysteroid dehydrogenase activities by abiraterone. Sci. Rep. 2016, 6, 32198. [Google Scholar] [CrossRef] [PubMed]
- Stiles, A.R.; McDonald, J.G.; Bauman, D.R.; Russell, D.W. CYP7B1: One Cytochrome P450, Two Human Genetic Diseases, and Multiple Physiological Functions. J. Biol. Chem. 2009, 284, 28485–28489. [Google Scholar] [CrossRef] [PubMed]
- Maksymchuk, O.; Gerashchenko, G.; Rosohatska, I.; Kononenko, O.; Tymoshenko, A.; Stakhovsky, E.; Kashuba, V. Cytochrome P450 genes expression in human prostate cancer. Mol. Genet. Metab. Rep. 2024, 38, 101049. [Google Scholar] [CrossRef] [PubMed]
- Maksymchuk, O.V.; Kashuba, V.I. Altered expression of cytochrome P450 enzymes involved in metabolism of androgens and vitamin D in the prostate as a risk factor for prostate cancer. Pharmacol. Rep. 2020, 72, 1161–1172. [Google Scholar] [CrossRef]
- Shidaifat, F.; Lin, Y.C. Testosterone effect on the expression of genes that mediate testosterone metabolism and genes that mediate the effect of those metabolites on the prostate. Life Sci. 2012, 91, 194–198. [Google Scholar] [CrossRef]
- Lundqvist, J.; Norlin, M. Effects of CYP7B1-related steroids on androgen receptor activation in different cell lines. Biochim. Biophys. Acta 2012, 1821, 973–979. [Google Scholar] [CrossRef]
- Olsson, M.; Gustafsson, O.; Skogastierna, C.; Tolf, A.; Rietz, B.D.; Morfin, R.; Rane, A.; Ekstrom, L. Regulation and expression of human CYP7B1 in prostate: Overexpression of CYP7B1 during progression of prostatic adenocarcinoma. Prostate 2007, 67, 1439–1446. [Google Scholar] [CrossRef]
- Lutz, S.Z.; Hennenlotter, J.; Scharpf, M.O.; Sailer, C.; Fritsche, L.; Schmid, V.; Kantartzis, K.; Wagner, R.; Lehmann, R.; Berti, L.; et al. Androgen receptor overexpression in prostate cancer in type 2 diabetes. Mol. Metab. 2018, 8, 158–166. [Google Scholar] [CrossRef]
- Russo, G.I.; Asmundo, M.G.; Lo Giudice, A.; Trefiletti, G.; Cimino, S.; Ferro, M.; Lombardo, R.; De Nunzio, C.; Morgia, G.; Piombino, E.; et al. Is There a Role of Warburg Effect in Prostate Cancer Aggressiveness? Analysis of Expression of Enzymes of Lipidic Metabolism by Immunohistochemistry in Prostate Cancer Patients (DIAMOND Study). Cancers 2023, 15, 948. [Google Scholar] [CrossRef] [PubMed]
- Russo, G.I.; Soeterik, T.; Puche-Sanz, I.; Broggi, G.; Lo Giudice, A.; De Nunzio, C.; Lombardo, R.; Marra, G. Oncological outcomes of cribriform histology pattern in prostate cancer patients: A systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2022, 26, 646–654. [Google Scholar] [CrossRef]
- Weihua, Z.; Lathe, R.; Warner, M.; Gustafsson, J.-Å. An endocrine pathway in the prostate, ERβ, AR, 5α-androstane-3β,17β-diol, and CYP7B1, regulates prostate growth. Proc. Natl. Acad. Sci. USA 2002, 99, 13589–13594. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Norlin, M. Regulation of steroid hydroxylase CYP7B1 by androgens and estrogens in prostate cancer LNCaP cells. Biochem. Biophys. Res. Commun. 2006, 344, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Broggi, G.; Lo Giudice, A.; Di Mauro, M.; Asmundo, M.G.; Pricoco, E.; Piombino, E.; Caltabiano, R.; Morgia, G.; Russo, G.I. SRSF-1 and microvessel density immunohistochemical analysis by semi-automated tissue microarray in prostate cancer patients with diabetes (DIAMOND study). Prostate 2021, 81, 882–892. [Google Scholar] [CrossRef] [PubMed]
- Broggi, G.; Lo Giudice, A.; Di Mauro, M.; Pricoco, E.; Piombino, E.; Ferro, M.; Caltabiano, R.; Morgia, G.; Russo, G.I. Insulin signaling, androgen receptor and PSMA immunohistochemical analysis by semi-automated tissue microarray in prostate cancer with diabetes (DIAMOND study). Transl. Res. 2021, 238, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Weihua, Z.; Mäkelä, S.; Andersson, L.C.; Salmi, S.; Saji, S.; Webster, J.I.; Jansesn, E.V.; Nilsson, S.; Warner, M.; Gustafsson, J.-Å. A role for estrogen receptor β in the regulation of growth of the ventral prostate. Proc. Natl. Acad. Sci. USA 2001, 98, 6330–6335. [Google Scholar] [CrossRef]
- Chang, B.; Zheng, S.L.; Hawkins, G.A.; Isaacs, S.D.; Wiley, K.E.; Turner, A.; Carpten, J.D.; Bleecker, E.R.; Walsh, P.C.; Trent, J.M.; et al. Joint effect of HSD3B1 and HSD3B2 genes is associated with hereditary and sporadic prostate cancer susceptibility. Cancer Res. 2002, 62, 1784–1789. [Google Scholar]
- Jakobsson, J.; Karypidis, H.; Johansson, J.-E.; Roh, H.-K.; Rane, A.; Ekström, L. A functional C–G polymorphism in the CYP7B1 promoter region and its different distribution in Orientals and Caucasians. Pharmacogenom. J. 2004, 4, 245–250. [Google Scholar] [CrossRef]
- Wu, W.; Maneix, L.; Insunza, J.; Nalvarte, I.; Antonson, P.; Kere, J.; Yu, N.Y.-L.; Tohonen, V.; Katayama, S.; Einarsdottir, E.; et al. Estrogen receptor β, a regulator of androgen receptor signaling in the mouse ventral prostate. Proc. Natl. Acad. Sci. USA 2017, 114, E3816–E3822. [Google Scholar] [CrossRef]
- Kakiyama, G.; Marques, D.; Martin, R.; Takei, H.; Rodriguez-Agudo, D.; LaSalle, S.A.; Hashiguchi, T.; Liu, X.; Green, R.; Erickson, S.; et al. Insulin resistance dysregulates CYP7B1 leading to oxysterol accumulation: A pathway for NAFL to NASH transition. J. Lipid Res. 2020, 61, 1629–1644. [Google Scholar] [CrossRef] [PubMed]
- Pandak, W.M.; Kakiyama, G. The acidic pathway of bile acid synthesis: Not just an alternative pathway. Liver Res. 2019, 3, 88–98. [Google Scholar] [CrossRef]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.F.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer—2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| PC (n = 286) | BPH (n = 104) | p-Value | |
|---|---|---|---|
| Age (years median) | 68 (63–72) | 78 (72–81) | <0.01 |
| Diabetes, n (%) | 44 (15.38) | 28 (26.92) | 0.01 |
| Fasting blood glucose (mg/dL), median (Q1–Q3) | 97 (88–107) | 95 (84–116) | 0.71 |
| Total cholesterol (mg/dL), median (Q1–Q3) | 191.5 (168–221.5) | 175 (150–199) | <0.01 |
| Triglycerides (mg/dL), median (Q1–Q3) | 97 (68–130) | 117 (69–164) | <0.01 |
| PSA (ng/mL), median (Q1–Q3) | 7.8 (5.7–11.6) | 2.05 (0.87–4.32) | <0.01 |
| BCR, n (%) | 56 (19.6) | - |
| CYP7B1 | p-Value | ||
|---|---|---|---|
| Negative (n = 251) | Positive (n = 139) | ||
| Age (years), median (Q1–Q3) | 71 (65–76) | 68 (63–71) | <0.01 |
| PSA (ng/mL), median (Q1–Q3) | 6.1 (3.53–9.6) | 7.2 (5.4–11) | <0.01 |
| Fasting glucose (mg/dL), median (Q1–Q3) | 96 (87–109) | 97 (88–111) | 0.9 |
| Total cholesterol (mg/dL), median (Q1–Q3) | 181.5 (156–210) | 190.5 (165.5- 218) | 0.1 |
| Triglycerides (mg/dL), median (Q1–Q3) | 100 (68–137) | 103 (72–146) | 0.9 |
| Diabetes, n (%) | 59 (23.5) | 33 (23.74) | 0.95 |
| Group, n (%) | <0.01 | ||
| BPH | 94 (37.45) | 10 (7.19) | |
| PC | 157 (62.55) | 129 (92.81) | |
| ISUP Gleason score in PC patients, n (%) | 0.25 | ||
| 1 | 49 (31.21) | 33 (25.58) | |
| 2 | 63 (40.13) | 47 (36.43) | |
| 3 | 34 (21.66) | 32 (24.81) | |
| 4 | 4 (2.55) | 10 (7.75) | |
| 5 | 7 (4.46) | 7 (5.43) | |
| Pathological stage in PC patients, n (%) | 0.04 | ||
| T2 | 111 (70.70) | 86 (66.67) | |
| T3 | 33 (21.02) | 20 (15.50) | |
| T4 | 13 (8.28) | 23 (17.83) | |
| Classification risk of PC, n (%) | 0.2 | ||
| Low risk | 56 (35.67) | 44 (34.11) | |
| Intermediate risk | 74 (47.13) | 52 (40.31) | |
| High risk | 27 (17.20) | 33 (25.58) | |
| Ki-67-positive score, n (%) | 31 (12.35) | 22 (15.83) | 0.3 |
| AR-positive score, n (%) | 110 (43.82) | 72 (51.80) | 0.1 |
| PSMA-positive score, n (%) | 71 (28.29) | 77 (55.40) | <0.01 |
| IR-α-positive score, n (%) | 132 (52.59) | 127 (91.37) | <0.01 |
| IR-β-positive score, n (%) | 4 (1.59) | 19 (13.67) | <0.01 |
| IGF-1R-positive score, n (%) | 36 (14.34) | 28 (20.14) | 0.1 |
| ATPLy-positive score, n (%) | 92 (36.65) | 95 (68.35) | <0.01 |
| SRSF-1-positive score, n (%) | 99 (39.44) | 89 (64.03) | <0.01 |
| CPT1-a-positive score, n (%) | 33 (13.15) | 32 (23.02) | 0.01 |
| SCD-1-positive score, n (%) | 39 (15.54) | 26 (18.71) | 0.4 |
| SREBP1-positive score, n (%) | 70 (27.89) | 26 (18.71) | 0.04 |
| FAS-positive score, n (%) | 111 (44.22) | 101 (72.66) | <0.01 |
| ACC-1-positive score, n (%) | 69 (27.49) | 75 (53.96) | <0.01 |
| Positive Expression of CYP7B1 | p-Value | |
|---|---|---|
| Age, OR (CI) | 1.00 (0.97–1.04) | 0.8 |
| PSA, OR (CI) | 1.01 (0.99–1.03) | 0.3 |
| Fasting glucose, OR (CI) | 1.00 (0.99–1.02) | 0.6 |
| Total cholesterol, OR (CI) | 1.00 (0.99–1.01) | 0.6 |
| Triglycerides, OR (CI) | 1.00 (0.99–1.00) | 0.7 |
| Diabetes, OR (CI) | 0.91 (0.47–1.74) | 0.8 |
| Ki-67-positive score, OR (CI) | 0.91 (0.49–1.67) | 0.8 |
| AR-positive score, OR (CI) | 1.36 (0.85–2.17) | 0.2 |
| PSMA-positive score, OR (CI) | 1.66 (1.04–2.66) | 0.03 |
| IR-α-positive score, OR (CI) | 5.73 (2.77–11.84) | <0.01 |
| IR-β-positive score, OR (CI) | 6.61 (2.19–19.96) | <0.01 |
| IGF-1R-positive score, OR (CI) | 0.93 (0.53–1.63) | 0.8 |
| ATPLy-positive score, OR (CI) | 3.73 (2.40–5.79) | <0.01 |
| SRSF-1-positive score, OR (CI) | 2.04 (1.27–3.29) | <0.01 |
| CPT1-a-positive score, OR (CI) | 1.33 (0.74–2.41) | 0.3 |
| SCD-1-positive score, OR (CI) | 1.22 (0.67–2.21) | 0.5 |
| SREBP1-positive score, OR (CI) | 0.61 (0.35–1.06) | 0.08 |
| FAS-positive score, OR (CI) | 2.15 (1.28–3.62) | <0.01 |
| ACC-1-positive score, OR (CI) | 1.83 (1.14–2.93) | 0.01 |
| ATPLy + vs. − (OR 95% CI) | CPT-1a, + vs. − (OR 95% CI) | SCD + vs. − (OR 95% CI) | SREBP + vs. − (OR 95% CI) | |
|---|---|---|---|---|
| PSA, continuous | 1.01 (0.98–1.03) | 1.00 (0.97–1.02) | 0.98 (0.95–1.01) | 0.96 (0.92–1.00) |
| Fasting blood glucose, continuous | 0.99 (0.98–1.01) | 1.00 (0.99–1.02) | 0.99 (0.98–1.01) | 1.00 (0.99–1.01) |
| Total cholesterol, continuous | 0.99 (0.98–1.00) | 0.99 (0.98–1.01) | 0.99 (0.98–1.00) | 0.99 (0.98–1.00) |
| Triglycerides, continuous | 1.00 (0.99–1.01) | 1.00 (0.99–1.01) | 0.99 (0.98–1.00) | 0.99 (0.98–1.00) |
| Diabetes, yes vs. no | 1.11 (0.58–2.16) | 0.82 (0.49–2.43) | 1.58 (0.74–3.39) | 0.51 (0.22–1.21) |
| Pathological stage, pT3/4 vs. pT2 | 1.27 (0.76–2.12) | 1.08 (0.79–2.04) | 0.94 (0.49–1.80) | 1.04 (0.60–1.85) |
| ISUP Gleason, ≥4 vs. <4 | 1.82 (0.77–4.30) | 0.75 (0.44–3.02) | 1.53 (0.61–3.82) | 0.79 (0.30–2.04) |
| AR, + vs. − | 1.71 (1.06–2.77) † | 2.27 (1.24–4.16) † | 2.87 (1.53–5.39) † | 2.16 (1.25–3.73) † |
| PSMA, + vs. − | 1.12 (0.70–1.80) | 0.97 (0.54–1.75) | 1.16 (0.64–2.12) | 0.94 (0.55–1.61) |
| Ki-67, + vs. − | 1.33 (0.71–2.50) | 1.37 (0.66–2.84) | 2.16 (1.07–4.32) † | 1.02 (0.51–2.04) |
| IR-α, + vs. − | 2.56 (1.43–4.56) † | 2.55 (1.03–6.27) † | 1.20 (0.56–2.56) | 1.93 (0.92–4.05) |
| IR-β, + vs. − | 1.08 (0.45–2.59) | 2.45 (1.01–6.11) † | 1.24 (0.44–3.51) | 1.33 (0.52–3.38) |
| IGF-1R, + vs. − | 1.30 (0.73–2.32) | 0.96 (0.47–1.95) | 1.01 (0.49–2.07) | 0.35 (0.16–0.78) † |
| ATPLy + vs. − | - | 1.26 (0.69–2.32) | 1.43 (0.76–2.68) | 1.41 (0.81–2.47) |
| CPT-1a, + vs. − | 1.26 (0.69–2.32) | - | 2.15 (1.08–4.24) † | 2.95 (1.58–5.49) † |
| SCD + vs. − | 1.43 (0.76–2.68) | 2.15 (1.08–4.24) † | - | 2.87 (1.53–5.39) † |
| SREBP -1+ vs. − | 1.41 (0.81–2.47) | 2.95 (1.57–5.48) † | 2.87 (1.53–5.39) † | - |
| FAS + vs. − | 4.84 (2.84–8.25) † | 2.16 (1.05–4.41) † | 3.17 (1.42–7.04) † | 1.74 (0.94–3.21) |
| CYP7B1 + vs. − | 3.73 (2.40–5.79) † | 1.98 (1.15–3.39) † | 1.25 (0.72–2.16) | 0.59 (0.36–0.99) † |
| FAS + vs. − (OR 95% CI) | ACC-1 + vs. − (OR 95% CI) | CYP7B1 + vs. − (OR 95% CI) | |
|---|---|---|---|
| PSA, continuous | 1.00 (0.98–1.03) | 0.99 (0.97–1.01) | 1.20 (0.93–1.54) |
| Fasting blood glucose, continuous | 0.99 (0.98–1.00) | 0.99 (0.98–1.01) | 0.99 (0.98–1.01) |
| Total cholesterol, continuous | 0.99 (0.99–1.00) | 0.99 (0.98–1.00) | 1.01 (0.99–1.01) |
| Triglycerides, continuous | 0.99 (0.99.1.00) | 0.99 (0.98–1.00) | 1.00 (0.99–1.04) |
| Diabetes, yes vs. no | 0.50 (0.26–0.97) | 1.60 (0.83–3.06) | 0.82 (0.47–1.41) |
| Pathological stage, pT3/4 vs. pT2 | 0.71 (0.42–1.20) | 1.30 (0.93–1.80) | 1.20 (0.72–1.98) |
| ISUP Gleason, ≥4 vs. <4 | 1.47 (0.60–3.60) | 1.21 (0.98–1.52) | 2.01 (0.91–4.47) |
| AR, + vs. − | 2.19 (1.30–3.69) † | 3.65 (2.22–5.93) † | 1.37 (0.91–2.09) |
| PSMA, + vs. − | 1.64 (1.00–2.71) † | 1.80 (1.13–2.89) † | 3.15 (2.04–4.85) † |
| Ki-67, + vs. − | 1.67 (0.83–3.38) | 1.11 (0.60–2.03) | 1.33 (0.74–2.41) |
| IR-α, + vs. − | 3.31 (1.84–5.95) † | 9.99 (4.35–22.93) † | 9.54 (5.02–18.12) † |
| IR-β, + vs. − | 1.77 (0.63–4.95) | 1.85 (0.77–4.43) | 9.78 (3.25–29.37) † |
| IGF-1R, + vs. − | 0.80 (0.44–1.44) | 1.18 (0.67–2.05) | 1.50 (0.87–2.59) |
| ATPLy + vs. − | 4.84 (2.84–8.25) † | 4.97 (2.95–8.39) † | 3.73 (2.40–5.79) † |
| CPT-1a, + vs. − | 2.16 (1.05–4.41) † | 2.12 (1.16–3.87) † | 1.98 (1.15–3.39) † |
| SCD + vs. − | 3.17 (1.42–7.04) † | 2.63 (1.40–4.91) † | 1.25 (0.72–2.16) |
| SREBP-1 + vs. − | 1.74 (0.94–3.21) | 2.53 (1.45–4.40) † | 0.59 (0.36–0.99) † |
| FAS + vs. − | - | 11.29 (5.76–22.14) † | 3.35 (2.14–5.25) † |
| CYP7B1 + vs. − | 3.35 (2.14–5.25) † | 3.09 (2.00–4.77) † | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russo, G.I.; Durukan, E.; Asmundo, M.G.; Lo Giudice, A.; Salzano, S.; Cimino, S.; Rescifina, A.; Fode, M.; Abdelhameed, A.S.; Caltabiano, R.; et al. CYP7B1 as a Biomarker for Prostate Cancer Risk and Progression: Metabolic and Oncogenic Signatures (Diagnostic Immunohistochemistry Analysis by Tissue Microarray in Prostate Cancer Patients—Diamond Study). Int. J. Mol. Sci. 2024, 25, 4762. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms25094762
Russo GI, Durukan E, Asmundo MG, Lo Giudice A, Salzano S, Cimino S, Rescifina A, Fode M, Abdelhameed AS, Caltabiano R, et al. CYP7B1 as a Biomarker for Prostate Cancer Risk and Progression: Metabolic and Oncogenic Signatures (Diagnostic Immunohistochemistry Analysis by Tissue Microarray in Prostate Cancer Patients—Diamond Study). International Journal of Molecular Sciences. 2024; 25(9):4762. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms25094762
Chicago/Turabian StyleRusso, Giorgio Ivan, Emil Durukan, Maria Giovanna Asmundo, Arturo Lo Giudice, Serena Salzano, Sebastiano Cimino, Antonio Rescifina, Mikkel Fode, Ali Saber Abdelhameed, Rosario Caltabiano, and et al. 2024. "CYP7B1 as a Biomarker for Prostate Cancer Risk and Progression: Metabolic and Oncogenic Signatures (Diagnostic Immunohistochemistry Analysis by Tissue Microarray in Prostate Cancer Patients—Diamond Study)" International Journal of Molecular Sciences 25, no. 9: 4762. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms25094762