

Prognostic Value of HHLA2 in Patients with Solid Tumors: A Meta-Analysis
 ,
,
Abstract
:1. Introduction
2. Results
2.1. Results of the Meta-Analysis
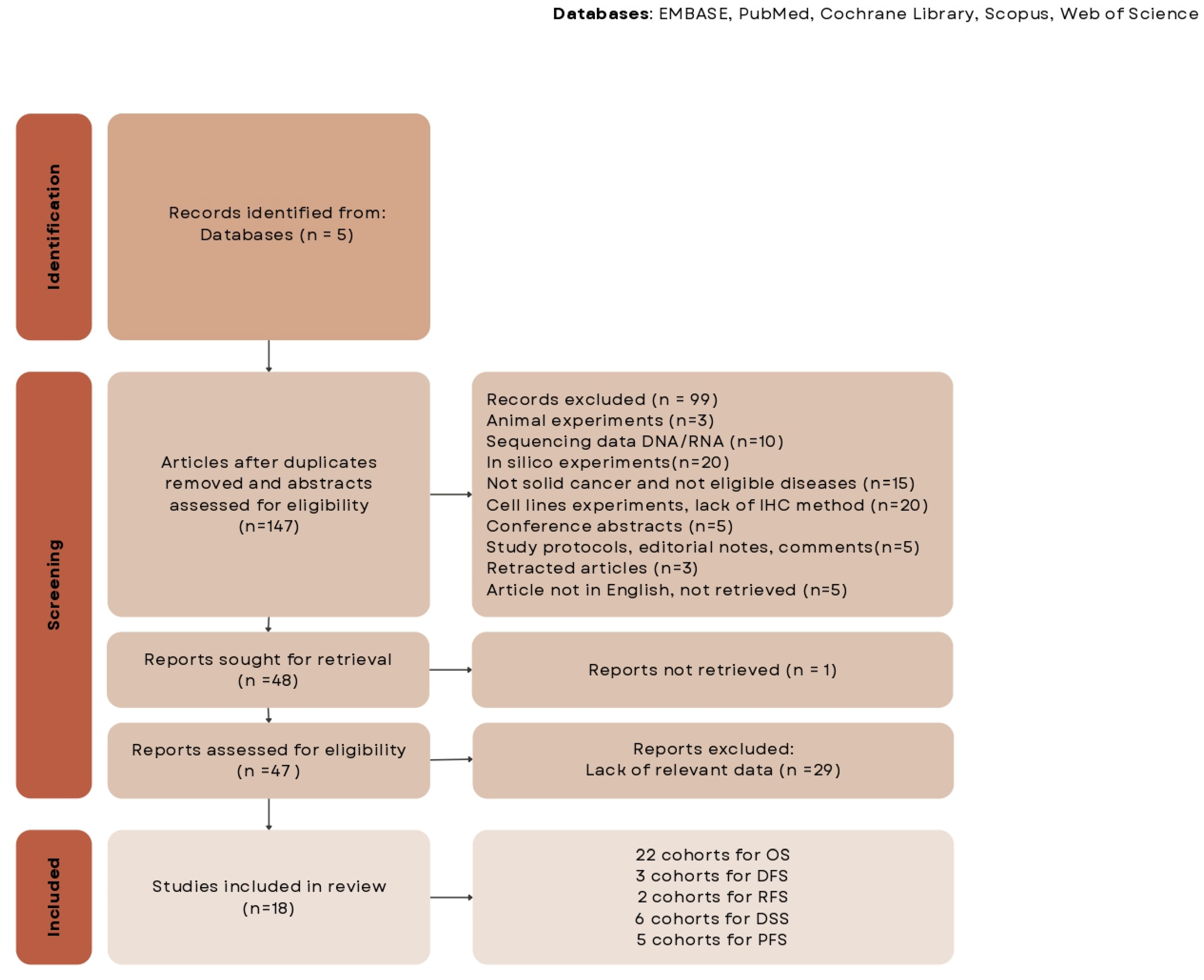
2.1.1. Search Results
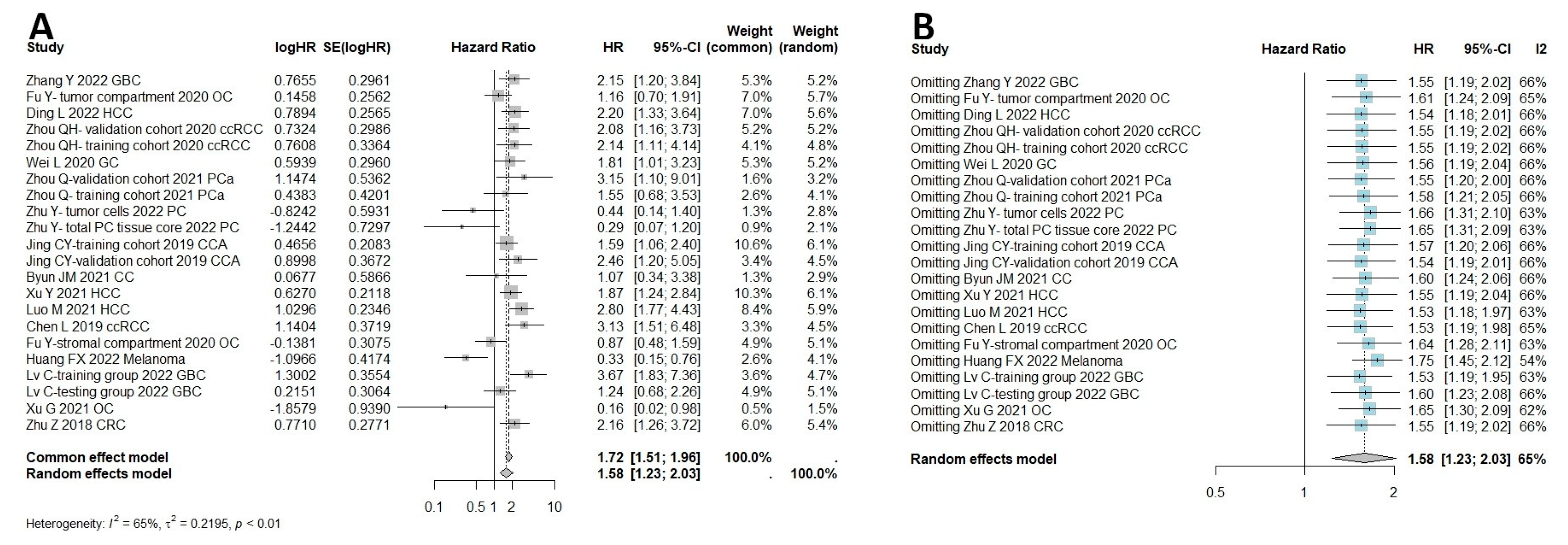
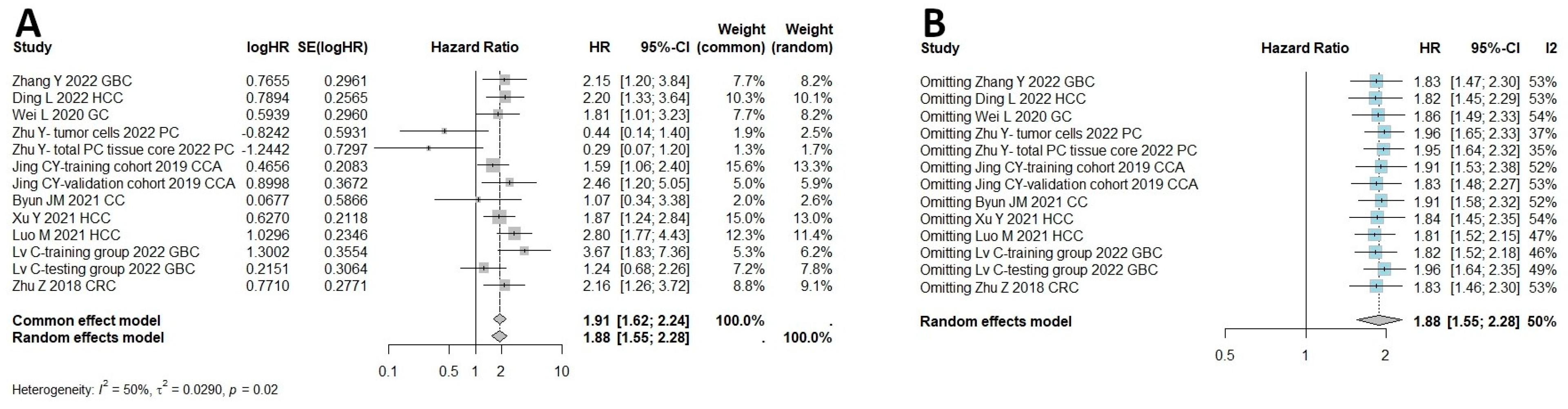
2.1.2. HHLA2 and Survival Outcomes
3. Discussion
4. Materials and Methods
4.1. Meta-Analysis
4.1.1. Literature Search Criteria and Outcomes
4.1.2. Inclusion and Exclusion Criteria
4.1.3. Study Selection and Data Extraction
4.1.4. Study Characteristics
4.1.5. Strategy for Meta-Analysis
4.1.6. Quality Assessment
5. Conclusions and Future Work
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shiravand, Y.; Khodadadi, F.; Kashani, S.M.A.; Hosseini-Fard, S.R.; Hosseini, S.; Sadeghirad, H.; Ladwa, R.; O’Byrne, K.; Kulasinghe, A. Immune Checkpoint Inhibitors in Cancer Therapy. Curr. Oncol. 2022, 29, 3044–3060. [Google Scholar] [CrossRef] [PubMed]
- Lei, Q.; Wang, D.; Sun, K.; Wang, L.; Zhang, Y. Resistance Mechanisms of Anti-PD1/PDL1 Therapy in Solid Tumors. Front. Cell Dev. Biol. 2020, 8, 672. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Lv, C.; Yu, Y.; Wu, B.; Zhang, Y.; Lang, Q.; Liang, Z.; Zhong, C.; Shi, Y.; Han, S.; et al. KIR3DL3-HHLA2 and TMIGD2-HHLA2 pathways: The dual role of HHLA2 in immune responses and its potential therapeutic approach for cancer immunotherapy. J. Adv. Res. 2023, 47, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Mager, D.L.; Hunter, D.G.; Schertzer, M.; Freeman, J.D. Endogenous retroviruses provide the primary polyadenylation signal for two new human genes (HHLA2 and HHLA3). Genomics 1999, 59, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Janakiram, M.; Chinai, J.M.; Zhao, A.; Sparano, J.A.; Zang, X. HHLA2 and TMIGD2: New immunotherapeutic targets of the B7 and CD28 families. Oncoimmunology 2015, 4, e1026534. [Google Scholar] [CrossRef]
- Zhou, Q.-H.; Li, K.-W.; Chen, X.; He, H.-X.; Peng, S.-M.; Peng, S.-R.; Wang, Q.; Li, Z.-A.; Tao, Y.-R.; Cai, W.-L.; et al. HHLA2 and PD-L1 co-expression predicts poor prognosis in patients with clear cell renal cell carcinoma. J. Immunother. Cancer 2020, 8, e000157. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Huang, Z.; Yu, X.; Li, Z.; Zheng, L.; Xu, J. HHLA2 Expression is Associated with Poor Survival in Patients with Hepatocellular Carcinoma. Biologics 2021, 15, 329–341. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zhu, D.; Feng, J.; Zhou, Y.; Wang, Q.; Feng, H.; Zhang, J.; Jiang, J. Overexpression of HHLA2 in human clear cell renal cell carcinoma is significantly associated with poor survival of the patients. Cancer Cell Int. 2019, 19, 101. [Google Scholar] [CrossRef] [PubMed]
- Ding, L.; Yu, Q.; Yang, S.; Yang, W.-J.; Liu, T.; Xian, J.-R.; Tian, T.-T.; Li, T.; Chen, W.; Wang, B.-L.; et al. Comprehensive Analysis of HHLA2 as a Prognostic Biomarker and Its Association With Immune Infiltrates in Hepatocellular Carcinoma. Front. Immunol. 2022, 13, 831101. [Google Scholar] [CrossRef]
- Cheng, H.; Janakiram, M.; Borczuk, A.; Lin, J.; Qiu, W.; Liu, H.; Chinai, J.M.; Halmos, B.; Perez-Soler, R.; Zang, X. HHLA2, a New Immune Checkpoint Member of the B7 Family, Is Widely Expressed in Human Lung Cancer and Associated with EGFR Mutational Status. Clin. Cancer Res. 2017, 23, 825–832. [Google Scholar] [CrossRef]
- Zhang, C.; Xu, J.; Ye, J.; Zhang, X. Prognostic value of HHLA2 expression in solid tumors: A meta-analysis based on the Chinese population. Medicine 2021, 100, e26789. [Google Scholar] [CrossRef]
- Zhou, Q.; Li, K.; Lai, Y.; Yao, K.; Wang, Q.; Zhan, X.; Peng, S.; Cai, W.; Yao, W.; Zang, X.; et al. B7 score and T cell infiltration stratify immune status in prostate cancer. J. Immunother. Cancer 2021, 9, e002455. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Lin, Y.; Liang, R.; Li, Y.; Ge, L. Clinical Significance of the HHLA2 Protein in Hepatocellular Carcinoma and the Tumor Microenvironment. J. Inflamm. Res. 2021, 14, 4217–4228. [Google Scholar] [CrossRef]
- Wei, L.; Tang, L.; Chang, H.; Huo, S.; Li, Y. HHLA2 overexpression is a novel biomarker of malignant status and poor prognosis in gastric cancer. Hum. Cell 2020, 33, 116–122. [Google Scholar] [CrossRef]
- Nishihara, D.; Kijima, T.; Arai, K.; Kamai, T. Increased co-expression of stromal HHLA2 and fibroblast activation protein in upper tract urothelial carcinoma. Int. Urol. Nephrol. 2023, 55, 867–874. [Google Scholar] [CrossRef]
- Jing, C.-Y.; Fu, Y.-P.; Yi, Y.; Zhang, M.-X.; Zheng, S.-S.; Huang, J.-L.; Gan, W.; Xu, X.; Lin, J.-J.; Zhang, J.; et al. HHLA2 in intrahepatic cholangiocarcinoma: An immune checkpoint with prognostic significance and wider expression compared with PD-L1. J. Immunother. Cancer 2019, 7, 77. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Dong, W. Overexpression of HHLA2, a member of the B7 family, is associated with worse survival in human colorectal carcinoma. Onco. Targets. Ther. 2018, 11, 1563–1570. [Google Scholar] [CrossRef] [PubMed]
- Koirala, P.; Roth, M.E.; Gill, J.; Chinai, J.M.; Ewart, M.R.; Piperdi, S.; Geller, D.S.; Hoang, B.H.; Fatakhova, Y.V.; Ghorpade, M.; et al. HHLA2, a member of the B7 family, is expressed in human osteosarcoma and is associated with metastases and worse survival. Sci. Rep. 2016, 6, 31154. [Google Scholar] [CrossRef] [PubMed]
- Luchini, C.; Stubbs, B.; Solmi, M.; Veronese, N. Assessing the quality of studies in meta-analyses: Advantages and limitations of the Newcastle Ottawa Scale. World J. Meta-Anal. 2017, 5, 80. [Google Scholar] [CrossRef]
- Xu, G.; Shi, Y.; Ling, X.; Wang, D.; Liu, Y.; Lu, H.; Peng, Y.; Zhang, B. HHLA2 predicts better survival and exhibits inhibited proliferation in epithelial ovarian cancer. Cancer Cell Int. 2021, 21, 252. [Google Scholar] [CrossRef]
- Huang, F.-X.; Wu, J.-W.; Cheng, X.-Q.; Wang, J.-H.; Wen, X.-Z.; Li, J.-J.; Zhang, Q.; Jiang, H.; Ding, Q.-Y.; Zhu, X.-F.; et al. HHLA2 predicts improved prognosis of anti-PD-1/PD-L1 immunotherapy in patients with melanoma. Front. Immunol. 2022, 13, 902167. [Google Scholar] [CrossRef]
- Bhatt, R.S.; Berjis, A.; Konge, J.C.; Mahoney, K.M.; Klee, A.N.; Freeman, S.S.; Chen, C.-H.; Jegede, O.A.; Catalano, P.J.; Pignon, J.-C.; et al. KIR3DL3 Is an Inhibitory Receptor for HHLA2 that Mediates an Alternative Immunoinhibitory Pathway to PD1. Cancer Immunol. Res. 2021, 9, 156–169. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, H.; Lv, C.; Wu, B.; Yu, Y.; Zhong, C.; Lang, Q.; Liang, Z.; Li, Y.; Shi, Y.; et al. HHLA2 promotes tumor progression by long non-coding RNA H19 in human gallbladder cancer. Int. J. Oncol. 2022, 61, 112. [Google Scholar] [CrossRef]
- Guyot, P.; Ades, A.E.; Ouwens, M.J.N.M.; Welton, N.J. Enhanced secondary analysis of survival data: Reconstructing the data from published Kaplan-Meier survival curves. BMC Med. Res. Methodol. 2012, 12, 9. [Google Scholar] [CrossRef]
- Lv, C.; Han, S.; Wu, B.; Liang, Z.; Li, Y.; Zhang, Y.; Lang, Q.; Zhong, C.; Fu, L.; Yu, Y.; et al. Novel immune scoring dynamic nomograms based on B7-H3, B7-H4, and HHLA2: Potential prediction in survival and immunotherapeutic efficacy for gallbladder cancer. Front. Immunol. 2022, 13, 984172. [Google Scholar] [CrossRef]
- Zhu, Y.; Chen, J.; Liu, Y.; Zheng, X.; Feng, J.; Chen, X.; Jiang, T.; Li, Y.; Chen, L. Prognostic values of B7-H3, B7-H4, and HHLA2 expression in human pancreatic cancer tissues based on mIHC and spatial distribution analysis. Pathol. Res. Pract. 2022, 234, 153911. [Google Scholar] [CrossRef]
- Byun, J.M.; Cho, H.J.; Park, H.Y.; Lee, D.S.; Choi, I.H.; Kim, Y.N.; Jeong, C.H.; Kim, D.H.; Hwa Im, D.; Min, B.J.; et al. The clinical significance of HERV-H LTR -associating 2 expression in cervical adenocarcinoma. Medicine 2021, 100, e23691. [Google Scholar] [CrossRef]
- Fu, Y.; Ding, Y.; Liu, J.; Zheng, X.; Wei, W.; Ying, Y.; Wu, C.; Jiang, J.; Ju, J. B7-H7 is a prognostic biomarker in epithelial ovarian cancer. Transl. Cancer Res. 2020, 9, 5360–5370. [Google Scholar] [CrossRef]
- Niu, Y.; Wang, W.; Jiang, X.; Huang, Y.; Yan, S.; Jiang, Y. High expression of HHLA2 predicts poor prognosis in medullary thyroid carcinoma. Jpn. J. Clin. Oncol. 2022, 52, 759–765. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Spiegelhalter, D.J. A re-evaluation of random-effects meta-analysis. J. R. Stat. Soc. Ser. A Stat. Soc. 2009, 172, 137–159. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Patient Source | Sample Size | Method | Cancer Type | HHLA2 + Expression | Outcome | HR Ratio | Multivare (M)/ Univare (U) | Cohort | Cell Types | Cut Off | Citation |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ding L | 2022 | China | 189 | IHC | HCC | 0.481 | OS/RFS | Reported | U/M | Tumor cells | H-score ≥ 5 | [9] | |
| Zhou QH | 2020 | China | 197 | IHC | ccRCC | 0.411 | OS/PFS | Reported | U/M | Validation cohort | Tumor cells | >20% | [6] |
| Zhou QH | 2020 | China | 206 | IHC | ccRCC | 0.44 | OS/PFS | Reported | U/M | Training cohort | Tumor cells | >20% | [6] |
| Zhang Y | 2022 | China | 89 | IHC | GBC | 0.50 | OS | Reported | U | Not specified | H-score > 80 | [23] | |
| Wei L | 2020 | China | 182 | IHC | GC | 0.68 | OS | Reported | U/M | Tumor cells | final score ≥ 8 | [14] | |
| Zhou Q | 2021 | China | 113 | IHC | PCa | 0.68 | OS/DSS | Reported | U/M | Validation cohort | Tumor cells | H score > 80 | [12] |
| Zhou Q | 2021 | China | 126 | IHC | PCa | 0.69 | OS/DSS | Reported | U/M | Training cohort | Tumor cells | H score > 80 | [12] |
| Zhu Y | 2022 | China | 63 | IHC | PC | 0.81 | OS | Reported | U/M | Tumor cells cohort | Tumor cells | H score > 80 | [26] |
| Zhu Y | 2022 | China | 63 | IHC | PC | 0.67 | OS | Reported | U/M | Tissue core cohort | All types of cells | H score > 80 | [26] |
| Byun J M | 2021 | Korea | 76 | IHC | CvC | 0.81 | OS/DFS | Reported | U/M | Tumor cells | staining 0, +/++, +++ | [27] | |
| Xu Y | 2021 | China | 205 | IHC | HCC | 0.33 | OS | Reported | U/M | All types of cells | NA | [7] | |
| Luo M | 2021 | China | 202 | IHC | HCC | 0.51 | OS | Reported | U/M | Tumor cells | IRS > 3 | [13] | |
| Chen L | 2019 | China | 86 | IHC | RCC | 0.30 | OS | Reported | U/M | All types of cells | H score > 90 | [8] | |
| Fu YY | 2020 | China | 119 | IHC | OC | 0.54 | OS/DFS | Reported | U/M | Stromal compartment | Stromal cells | >6.13% | [28] |
| Fu YY | 2020 | China | 119 | IHC | OC | 0.50 | OS/DFS | Reported | U/M | Tumor compartment | Tumor cells | >31.51% | [28] |
| Huang FX | 2022 | China | 81 | IHC | MM | 0.22 | OS/PFS | Reported | U/M | Tumor cells | >50% | [21] | |
| Lv C | 2022 | China | 95 | IHC | GBC | 0.53 | OS/DSS | Reported | U/M | Validation cohort | All types of cells | H score > 91 | [25] |
| Lv C | 2022 | China | 103 | IHC | GBC | 0.60 | OS/DSS | Reported | U/M | Training cohort | All types of cells | H score > 90 | [25] |
| Niu Y | 2022 | China | 51 | IHC | MTC | 0.31 | DFS | Reported | M | Tumor cells | >50% | [29] | |
| Xu G | 2021 | China | 64 | IHC | OC | 0.17 | OS | Reported | U/M | All types of cells | >0% | [20] | |
| Nishihara D | 2023 | Japan | 85 | IHC | UC | 0.68 | DSS/PFS | Reported | U/M | Tumor cells cohort | Tumor cells | >20% | [15] |
| Nishihara D | 2023 | Japan | 85 | IHC | UC | 0.55 | DSS/PFS | Reported | U/M | Tissue core cohort | Stromal cells | >20% | [15] |
| Zhu Z | 2018 | China | 63 | IHC | CRC | 0.47 | OS | Reported | U/M | All types of cells | H score > median | [17] | |
| Jing CY | 2019 | China | 153 | IHC | CCA | 0.49 | OS | Reported | M | Training cohort | Tumor cells | NA | [16] |
| Jing CY | 2019 | China | 65 | IHC | CCA | 0.68 | OS/RFS | Reported | M | Validation cohort | Tumor cells | NA | [16] |
| Study | Selection | Comparability | Exposure | Scores | Citation | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Representativeness of the Exposed Cohort | Selection of the Nonexposed Cohort | Ascertainment of Exposure | Demonstration That Outcome of Interest Was Not Present at Start of Study | Comparability of Cohorts on the Basis of the Design or Analysis | Assessment of Outcome | Was Followed-Up for Long Enough for Outcomes to Occur | Adequacy of Follow Up of Cohorts | |||
| Ding L, 2022 | ★ | ★ | ★ | - | ★★ | ★ | - | ★ | 7 | [9] |
| Zhou QH, 2020 | ★ | ★ | ★ | - | ★★ | ★ | ★ | ★ | 8 | [6] |
| Zhang, 2022 | ★ | ★ | ★ | - | ★ | - | ★ | ★ | 6 | [23] |
| Wei L, 2020 | ★ | ★ | ★ | - | ★★ | - | ★ | ★ | 7 | [14] |
| Zhou Q, 2021 | ★ | ★ | ★ | - | ★★ | ★ | ★ | ★ | 8 | [12] |
| Zhu Y, 2022 | ★ | ★ | ★ | - | ★★ | - | ★ | - | [26] | |
| Byun J M, 2021 | ★ | ★ | ★ | - | ★★ | ★ | ★ | ★ | 8 | [27] |
| Xu Y, 2021 | ★ | ★ | ★ | - | ★★ | - | ★ | ★ | 7 | [7] |
| Luo M, 2021 | ★ | ★ | ★ | - | ★★ | - | ★ | ★ | 7 | [13] |
| Chen L, 2019 | ★ | ★ | ★ | - | ★★ | - | ★ | ★ | 7 | [8] |
| Fu YY, 2020 | ★ | ★ | ★ | - | ★★ | ★ | ★ | ★ | 8 | [28] |
| Huang FX, 2022 | ★ | ★ | ★ | - | ★★ | ★ | - | ★ | 7 | [21] |
| Chao LV, 2022 | ★ | ★ | ★ | - | ★★ | ★ | ★ | ★ | 8 | [25] |
| Niu Y, 2022 | ★ | ★ | ★ | - | ★★ | ★ | ★ | ★ | 8 | [29] |
| Xu G, 2021 | ★ | ★ | ★ | - | ★★ | - | ★ | ★ | 7 | [20] |
| Nishihara D, 2023 | ★ | ★ | ★ | - | ★★ | ★ | ★ | ★ | 8 | [15] |
| Zhu Z, 2018 | ★ | ★ | ★ | - | ★★ | - | ★ | ★ | 7 | [17] |
| Jing CY, 2019 | ★ | ★ | ★ | - | ★★ | ★ | ★ | ★ | 8 | [16] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kula, A.; Dawidowicz, M.; Mielcarska, S.; Świętochowska, E.; Waniczek, D. Prognostic Value of HHLA2 in Patients with Solid Tumors: A Meta-Analysis. Int. J. Mol. Sci. 2024, 25, 4760. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms25094760
Kula A, Dawidowicz M, Mielcarska S, Świętochowska E, Waniczek D. Prognostic Value of HHLA2 in Patients with Solid Tumors: A Meta-Analysis. International Journal of Molecular Sciences. 2024; 25(9):4760. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms25094760
Chicago/Turabian StyleKula, Agnieszka, Miriam Dawidowicz, Sylwia Mielcarska, Elżbieta Świętochowska, and Dariusz Waniczek. 2024. "Prognostic Value of HHLA2 in Patients with Solid Tumors: A Meta-Analysis" International Journal of Molecular Sciences 25, no. 9: 4760. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms25094760